Journal
9
Review Saliva: A potential media for disease diagnostics and monitoring Jingyi Liu, Yixiang Duan ⇑ Research Center of Analytical Instrumentation, Analytical & Testing Centre and College of Chemistry, Sichuan University, No. 29 Wangjiang Road, Chengdu 610064, PR China article info Article history: Received 9 September 2011 Received in revised form 28 December 2011 Accepted 26 January 2012 Available online 19 February 2012 Keywords: Saliva Biomarkers Disease diagnosis Oral squamous cell carcinoma Periodontal disease Cancer Sjögren’s syndrome summary Within the past 10 years, the use of saliva as a diagnostic tool has gained considerable attention and become a well-accepted method. As a diagnostic fluid, saliva offers superiority over serum due to both a noninvasive collection method by specially trained persons and a cost-effective approach for screening of large populations. Collection of saliva offers a reduced risk of infection compared to the collection of serum. Moreover, obtaining saliva samples from infant, disabled or anxious patients, is much easier than obtaining other samples. There is a lot of useful components-changing information in saliva when a per- son is in sick. Therefore, we define these changing components as ‘‘biomarkers’’. The utilization of bio- markers as early predictors for clinical disease not only contributes to the effective prevention and treatment of diseases, but also enhances the assessment of potential health risks. In this article, we have reviewed the properties of saliva, the salivary analysis method for biomarker discovery, and the diagnos- tic potentials of salivary biomarkers in monitoring and detecting periodontal disease, Oral and Breast cancers, and Sjögren’s syndrome. We also discussed some barriers of applications of saliva as a diagnostic media as well as recent improvements. We also prospected the future processing directions of using bio- markers in disease diagnosis and draw a conclusion that saliva is indeed an effective media in various disease monitoring and diagnosis. Ó 2012 Elsevier Ltd. All rights reserved. Introduction Early detection of disease plays a significant role in successful clinical treatment. In most cases of various diseases, early detection and diagnosis lead to a greater survival rate with a reduced chance of the disease re-emerging. Successful monitoring of a disease, especially in its early stage, may also reduce any severe impacts on a patient’s health or help to prevent and/or delay succeeding complications. The ability to evaluate physiological conditions, trace disease progression, and monitor post-treatment therapeutic resulting through a noninvasive method is one of the primary objectives in the field of healthcare research. Saliva, a multi-constit- uent oral fluid that can be collected through noninvasive means, has considerable potential for the surveillance of general health and disease. Human saliva contains many kinds of proteins and peptides, each of them carries several significant biological func- tions. With the advancement of novel technological means (such as bioinformatics, metabolomics, genomics and proteomics), saliva, as a clinical tool, has become a more and more attractive option be- cause of its ability to mirror both oral and systemic health condi- tions. 1 But in order for saliva-based diagnostics to be useful, two prerequisites must be fulfilled: (1) discovering biomarkers for various diseases among the complicated composition of saliva, and (2) evaluating the sensitivity and specificity of biomarkers through a series of continuous developments. 2 Saliva profile Water is the most abundant component in saliva, representing 99% of saliva’s total composition. The solid components soluble in the aqueous phase differ from person to person, and can even vary in the same individual at distinct times during a day. The inor- ganic species are mainly composed of weak and strong ions includ- ing Na + ,K + , Cl , Ca 2+ , HPO 2 3 , HCO 3 , Mg 2+ , and NH 3 . The organic species (see Table 1) consist of body secretion products (urea, uric acid and creatinine); putrefaction products (putrescine and cadav- erine); lipids (cholesterol and fatty acids), and more than 400 types of protein. Among those proteins, the most relevant ones are glan- dular in origin (alphaamylase, histatins, cystatins, lactoferrins, lysozymes, mucins, and proline-rich proteins (PRPs)) or are plas- ma-derivatives (albumin, secretory immunoglobulin A (sIgA), and transferrin). 3 Human saliva proteome (HSP) analysis is inherently challenging because human saliva contains an inherently large variety of pro- teins with an equally wide range of concentrations. For example, a-amylase, the most abundant protein in human saliva, is at mg/ ml level, whereas cytokines are typically within the range of pg/ml. 4 1368-8375/$ - see front matter Ó 2012 Elsevier Ltd. All rights reserved. doi:10.1016/j.oraloncology.2012.01.021 ⇑ Corresponding author. Tel.: +86 028 85418180; fax: +86 028 85412316. E-mail address: [email protected] (Y. Duan). Oral Oncology 48 (2012) 569–577 Contents lists available at SciVerse ScienceDirect Oral Oncology journal homepage: www.elsevier.com/locate/oraloncology
-
Upload
sabiran-gibran -
Category
Documents
-
view
41 -
download
0
description
Science
Transcript of Journal

Oral Oncology 48 (2012) 569–577
Contents lists available at SciVerse ScienceDirect
Oral Oncology
journal homepage: www.elsevier .com/locate /ora loncology
Review
Saliva: A potential media for disease diagnostics and monitoring
Jingyi Liu, Yixiang Duan ⇑Research Center of Analytical Instrumentation, Analytical & Testing Centre and College of Chemistry, Sichuan University, No. 29 Wangjiang Road, Chengdu 610064, PR China
a r t i c l e i n f o s u m m a r y
Article history:Received 9 September 2011Received in revised form 28 December 2011Accepted 26 January 2012Available online 19 February 2012
Keywords:SalivaBiomarkersDisease diagnosisOral squamous cell carcinomaPeriodontal diseaseCancerSjögren’s syndrome
1368-8375/$ - see front matter � 2012 Elsevier Ltd. Adoi:10.1016/j.oraloncology.2012.01.021
⇑ Corresponding author. Tel.: +86 028 85418180; faE-mail address: [email protected] (Y. Duan).
Within the past 10 years, the use of saliva as a diagnostic tool has gained considerable attention andbecome a well-accepted method. As a diagnostic fluid, saliva offers superiority over serum due to botha noninvasive collection method by specially trained persons and a cost-effective approach for screeningof large populations. Collection of saliva offers a reduced risk of infection compared to the collection ofserum. Moreover, obtaining saliva samples from infant, disabled or anxious patients, is much easier thanobtaining other samples. There is a lot of useful components-changing information in saliva when a per-son is in sick. Therefore, we define these changing components as ‘‘biomarkers’’. The utilization of bio-markers as early predictors for clinical disease not only contributes to the effective prevention andtreatment of diseases, but also enhances the assessment of potential health risks. In this article, we havereviewed the properties of saliva, the salivary analysis method for biomarker discovery, and the diagnos-tic potentials of salivary biomarkers in monitoring and detecting periodontal disease, Oral and Breastcancers, and Sjögren’s syndrome. We also discussed some barriers of applications of saliva as a diagnosticmedia as well as recent improvements. We also prospected the future processing directions of using bio-markers in disease diagnosis and draw a conclusion that saliva is indeed an effective media in variousdisease monitoring and diagnosis.
� 2012 Elsevier Ltd. All rights reserved.
Introduction
Early detection of disease plays a significant role in successfulclinical treatment. In most cases of various diseases, early detectionand diagnosis lead to a greater survival rate with a reduced chanceof the disease re-emerging. Successful monitoring of a disease,especially in its early stage, may also reduce any severe impactson a patient’s health or help to prevent and/or delay succeedingcomplications. The ability to evaluate physiological conditions,trace disease progression, and monitor post-treatment therapeuticresulting through a noninvasive method is one of the primaryobjectives in the field of healthcare research. Saliva, a multi-constit-uent oral fluid that can be collected through noninvasive means,has considerable potential for the surveillance of general healthand disease. Human saliva contains many kinds of proteins andpeptides, each of them carries several significant biological func-tions. With the advancement of novel technological means (suchas bioinformatics, metabolomics, genomics and proteomics), saliva,as a clinical tool, has become a more and more attractive option be-cause of its ability to mirror both oral and systemic health condi-tions.1 But in order for saliva-based diagnostics to be useful, twoprerequisites must be fulfilled: (1) discovering biomarkers for
ll rights reserved.
x: +86 028 85412316.
various diseases among the complicated composition of saliva,and (2) evaluating the sensitivity and specificity of biomarkersthrough a series of continuous developments.2
Saliva profile
Water is the most abundant component in saliva, representing99% of saliva’s total composition. The solid components solublein the aqueous phase differ from person to person, and can evenvary in the same individual at distinct times during a day. The inor-ganic species are mainly composed of weak and strong ions includ-ing Na+, K+, Cl�, Ca2+, HPO2�
3 , HCO�3 , Mg2+, and NH3. The organicspecies (see Table 1) consist of body secretion products (urea, uricacid and creatinine); putrefaction products (putrescine and cadav-erine); lipids (cholesterol and fatty acids), and more than 400 typesof protein. Among those proteins, the most relevant ones are glan-dular in origin (alphaamylase, histatins, cystatins, lactoferrins,lysozymes, mucins, and proline-rich proteins (PRPs)) or are plas-ma-derivatives (albumin, secretory immunoglobulin A (sIgA), andtransferrin).3
Human saliva proteome (HSP) analysis is inherently challengingbecause human saliva contains an inherently large variety of pro-teins with an equally wide range of concentrations. For example,a-amylase, the most abundant protein in human saliva, is at mg/ml level, whereas cytokines are typically within the range of pg/ml.4

Table 1Salivary proteins.3
Salivary protein Origin Functions Concentrations
Total proteins 0.47 ± 0.19 mg/ml, 0.9 ± 0.2 mg/ml, 4.3–710.0 mg/dl, 2.67 ± 0.54 mg/mla-Amylase Starch digestion 3257 ± 1682 U/ml, 1080.0 ± 135.6 IU/l, 476 ± 191 lg/mlAlbumin Plasma Mainly from plasma leakage 0.2 ± 0.1 mg/ml, 0.8–192 mg/dlCystatins group SM > SL Antimicrobial(cistein-proteinase inhibitor) 14.3 kDa form 58 ± 25 lg/ml; 14.2 kDa form 91 ± 46 lg/mlHystatin P Antifungal 1190 ± 313 lg/mlSecretory IgA B lymphocytes Antimicrobial 124.3–335.3 lg/mlLactoferrin Mucous > serous Antimicrobial 3.7 ± 2.5 lg/mlLysozyme SL > SM,P Antimicrobial 3.5–92.0 lg/ml, 21.8 ± 2.5 mg/dl, 59.7–1062.3 lg/mlMucins group Mucous glands Lubrication MUC5B: 2.4 ± 1.7 U/mlPRPs P Binding to bacteria and with dietary tannins Acidic PRP: 456 ± 139 lg/ml,
Basic PRP:165 ± 69 lg/mlStatherin Ca++ binding 4.93 ± 0.61 lmol/l, 36 ± 18 lg/mlTransferrin Plasma 0.58 ± 0.2 mg/dl
SM = submandibular; SL = sublingual; P = parotid.
570 J. Liu, Y. Duan / Oral Oncology 48 (2012) 569–577
The reason why saliva can potentially be used as a specimen fordiagnosis is because of its exchange with substances existing in hu-man serum. A thin layer of epithelial cells separating the salivaryducts from the systemic circulation enables the transfer of sub-stances to the saliva by means of active carriage, diffusion throughthe cell membrane, or passive diffusion via a concentrationgradient.
One of the principal advantages of using saliva as a diagnosticmedia is that its sampling is easy and noninvasive, thus eliminat-ing any discomfort and pain associated with blood collection whilealso avoiding privacy issues associated with urine collection. Addi-tionally, compared with blood, saliva contains a smaller quantity ofproteins, therefore decreasing any potential risk of non-specificinterference and hydrostatic interactions. Within blood, the pro-tein concentration can vary over several orders of magnitude, withprotein half-lives ranging from a few seconds to several months orlonger. The composition of saliva, however, is not as complex orvarying as serum, and should more accurately reflect the currentcondition of the body at any given time.
Ultimately, saliva may contain locally expressed proteins andother substances that can be used as indicators of diseases. Thesecomponents, called biomarkers, can be closely related to an indi-vidual’s health condition and can change greatly when diseases af-flict the body.
Biomarker
According to the National Institutes of Health, a biomarker is acharacteristic that is objectively measured and evaluated as anindicator of normal biologic processes, pathogenic processes, orpharmaceutical responses to a therapeutic intervention.5 Generallyspeaking, a biomarker can be any biomolecule or specific charac-teristic, feature, or indicator of an alteration in any biological con-stitution and function that can objectively reflect the state of aliving organism.6
Criterion for biomarker
� A major product of oxidative modification that may be impli-cated directly in the development of a disease;� A stable product, not susceptible to artefactual induction, not
easy to lose, or not changeable during storage;� Representative of the balance between oxidative damage gener-
ation and clearance;� Determined by an analytical assay that is specific, sensitive,
reproducible and robust;� Free of confounding and interference factors from dietary
intake;
� Accessible in a target tissue or a valid surrogate tissue such as aleukocyte;� Detectable and measurable within the limits of detection of a
reliable analytical procedure.7
The discovery–validation–implementation paradigm
A biomarker must be verified and validated before it can haveany impact or application on health risk assessment. The verificat-ing process might be considered as a process that is conceptuallysimilar to therapeutic drug evaluation. There are six prerequisitesbefore a biomarker can be used in a clinical assay: (1) preclinicaltesting: developing in vitro or in animal models; (2) preliminarytesting: developing preliminary assays on patient samples; (3) fea-sibility analysis: testing on a small group of patients to determineits ability to discriminate between healthy or diseased subjects; (4)validation of the accuracy of assays; (5) statistical analysis: deter-mining in large patient populations; (6) post-approval reportingand testing. A general recommendation is that the validation effortshould concentrate on those biomarkers directly involved in thecausal pathway of disease, since the closer to the causal pathwaythe biomarker is, the more precisely it will predict disease.8
Saliva analysis
In the last few years, remarkable efforts have been devoted tothe identification of proteins in human and parotid saliva by usingdiverse proteomic approaches. High-resolution liquid separation isa critical component in both shotgun and random proteome anal-ysis. Pre-fractionation of proteins using liquid-based separationtechniques is often required for a comprehensive analysis. Separa-tions can be performed based on the physiochemical properties ofthe interested protein using capillary isoelectric focusing (IEF),9 gelfiltration liquid chromatography (LC), reversed-phase (RP) LC,strong cation exchange LC or ZOOM IEF. The fractions are collectedand digested using proteolytic enzymes and the resulting peptidesare analyzed with 1D-LC/MS/MS or 2D-LC/MS/MS, either online oroffline. The online 2D-LC separation uses a single capillary columnpacked with two types of LC separation media10 or an automaticcolumn-switching technique. Free-flow electrophoresis can becoupled with RP-LC to greatly enhance the separation of peptidesprior to MS/MS analysis.11
In other cases, investigators have used two-dimensional (2D)gel electrophoresis (GE) to separate protein components, followedby mass spectrometry (MS) to subsequently identify the peptidesproduced from in-gel digestion of the proteins of interest. This ap-proach revealed that more than 300 proteins exist within saliva.When separations were performed using liquid chromatography

Table 2Various salivary biomarkers significantly altered in OSCC patients as compared withhealthy controls.56
Biomarker Biological function
IAP Apoptosis inhibitorSCC Squamous cell carcinoma associated
antigenCEA Carcinogenic embryonic carcinogenCA19-9 Carcino-antigenCA125 Serum tumor markerCyfra 21-1 Intermediate filament proteinTPS Tissue polypeptide specific antigenRNS Reactive nitrogen species8-OHdG DNA damage markerIgG ImmunoglobulinSec IgA Mucosal immunoglobinIGF Growth factorMMP-2, MMP-11 Metalloproteinase
J. Liu, Y. Duan / Oral Oncology 48 (2012) 569–577 571
(LC) instead of GE, the results from 2D-MS identified more than1050 proteins in saliva.12–14
Recently, surface-enhanced laser desorption/ionization time-offlight (SELDI-TOF) has also been utilized. This technique, whichcombines matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF-MS) with surface chroma-tography, enables rapid and high-throughput detection of criticalproteins and peptides requiring only small amounts of non pre-processed sample.15 Finally, additional methodologies, such ashigh performance liquid chromatography/mass spectrometry(HPLC/MS), have proven to be useful in the evaluation of the small-est salivary proteins and peptides.16 Currently, the proteomic anal-ysis of salivary biomarkers holds promise as a non-invasivemethod for identifying various diseases such as cancer, diabetes,and autoimmune diseases. These profiling technologies may beintegrated to achieve a more comprehensive analysis.
LOH Loss of heterozygosity-loss of specificchromosomal regions
DNA hypermethylation Gene inactivationIL8, IL 1BDUSP1 Chemokine-mediator of inflammatory
responseHA3 Cell proliferation regulatorOAZ1 OncogeneS100P Polyamine synthesis regulatorSAT Calcium binding protein, cell cycle and
differentiation regulatorPolyamine metabolism
Others (salivary mRNA) B2M,FTH1,G0S2,GADD45B,H3F3A,HSPC016,IER3,MAP2K3,PRG1,RGS257
Biomarker ChangeCarbonyls, lactate
dehydrogenase,metalloproteinase-9 (MMP-9) Ki67, Cyclin D1 (CycD1)58
Increased
8-Oxoguanine DNAglycosylase, Phosphoryl-ated-Src, mammary serineprotease inhibitor (Maspin)
Decreased
Salivary biomarkers as a diagnostic tool for different disease
Oral squamous cell carcinoma (OSCC)
Oral squamous cell carcinoma (OSCC) is a common malignanttumor occurring with increasing frequency among individuals.The prevalence of OCSS has had a 5.3-fold increase for men and a2-fold increase for women within the past two decades. The sur-vival rate of oral cancer is 60–80% when detected during its earlystages; however, this number drops to 30–40% when the canceris diagnosed during the advanced stages.17 One pressing issue isthe lack of a reliable early stage diagnostic marker for OSCC, mean-ing almost all OSCC cases are diagnosed when the cancer hasdeveloped well into the advanced stages. In addition, because OSCChas a very high recurrence rate, early identification and detectionbecome essential for patient survival. Detection of OSCC is cur-rently based on expert clinical examination and histological analy-sis of suspicious areas, but it may be undetectable in hidden sites.Therefore, sensitive and specific biomarkers for OSCC may be help-ful for screening of high-risk patients.18
Several studies have developed methods for using salivary pro-teins as potential diagnostic markers for oral cancer. Increasinglevels of saliva-soluble CD44 were shown in the majority of pa-tients with OSCC and could be used to distinguish cancer fromhealth with high specificity.19 Also, the concentration of three tu-mor markers: cytokeratin 19 fragment (Cyfra 21-1)20, tissue poly-peptide antigen, and cancer antigen 125, were found significantlyelevated in the saliva of OSCC patients. Analysis of the concentra-tions of these three markers in both saliva and plasma yielded sim-ilar diagnostic results among OSCC patients.21 Also, the level of p53autoantibodies measured in saliva was found to correlate withthose levels in serum, potentially offering a specific method fordetecting a subset of OSCC with p53 aberrations.22 However, thesecandidate biomarkers were discovered on an individual basis, lim-iting their potential for predicting OSCC. Table 2 present a selectionof potential biomarkers found in OSCC patients.
By using two-dimensional gel electrophoresis (2D-GE) and ma-trix-assisted laser desorption/ionization time-of-flight mass spec-trometry (MALDI-TOF-MS), Cheng-Wen Lin analyzed the proteinprofile of pooled salivary samples from patients with oral squa-mous cell carcinoma (OSCC) and OSCC-free control subjects, find-ing elevated transferrin levels in the saliva of OSCC patients.Additionally, the magnitude of the salivary transferrin levels inOSCC patients strongly correlated with the size and stage of thetumor.23
Using laser-capture micro dissection, St John MAR4 have identi-fied the expression of cellular gene that are uniquely associated withOSCC: interleukin (IL) 8. IL-8 has proven to be clinically significant in
oral cancer diagnosis. Results showed higher concentrations of IL-8in saliva among patients with OSCC. These cytokines may contributeto the pathogenesis of this disease, and have been linked with in-creased tumor growth and metastasis. As a salivary biomarker forearly stage OSCC, IL-8 can be detected at 1.1 pM level using a surfaceimmobilized sandwich assay technique.24 Therefore, the detectionof IL-8 levels could prove to be a cost-effective tool in the diagnosisand monitoring of patients with OSCC.
S. Shintani25 used surface-enhanced laser desorption/ionizationtime-of-flight mass spectrometry (SELDI-TOF) Protein Chip systemto screen for differentially expressed proteins in the saliva samples.Shintani, suggested that Protein Chip analysis may provide a reli-able screening test for early diagnosis of OSCC, with emphasis onthe importance of truncated cystatin SA-I as an OSCC tumor bio-marker. To confirm that truncated cystatin SA-I is an OSCC-specificprotein, the expression levels in pre-and post-treatment salivafrom OSCC patients were compared. Experiments performed onCM10 arrays showed an increased intensity of truncated cystatinSA-I in pre-treatment saliva samples compared to post-treatmentsamples.
TNF-a has a salivary concentration approximately 30 pg/ml inoral cancer patients and 3 pg/ml in healthy individuals. Such a con-centration discrepancy provides another potential biomarker forOSCC supervision. Most proteins found in saliva exist both in indi-viduals with OSCC and in healthy individuals. However, 52 pro-teins were found to be present in OSCC patients only, and 29proteins were found in healthy subjects only.26 The identity of eachprotein is listed in Table 3. Further validation on a larger patientcohort is required for these putative biomarkers.

Table 3Saliva proteins identified only from healthy control (compared with OSCC) subjects and only from OSCC (compared with healthy persons) by subtractive proteomics.
Saliva proteins identified only from healthy control (compared with OSCC) subjects
Clusterin Uteroglobin Utrophin Cornifin A, B Sparc-like protein 1 Metalloproteinaseinhibitor 1
Serine/arginine repetitive Matrix 1 Cask-interzcting protein 2 Splice isoform 1 OfADAMTS-2
Desmoglein 3 Antileuko-proteinase 1 9,42,43,86,172 kDaprotein
Neurofilament triplet H protein Actin-related protein 5 Similar to Iggamma-3 C region
Metaxin 1 isoform 1 Airway trypsin-likeprotease
Hypothetical protein
Similar to heterogeneous nuclear ribonucleoprotein K Macrophage migration inhibitory factor
Saliva proteins identified only from OSCC patientsCatalase Azurocidin Involucrin Transaldolase Hemopexin CalcyclinBeta-2-glycopr-otein 1 Enolase 1 Enolase 2 Enolase 3 Vitamin D-binging
proteinBrain acid SolubleProtein 1
Similar to Myomegalin Phosphoglyc-eratekinase 1
Cathepsin G S-100P mprotein Thioredoxin Calgizzarin Moesin Histone H1.2Peptidylprolyl isomerase A-like Splice isoform 2 of
myeloperoxidaseSquamous cellcarcinoma antigen2
Haptoglobin-relatedprotein
Tumor-related protein CD59 glycoprotein
Peroxiredoxin 2 Epsilon globin Heat shock 70 KDaprotein 1
Shroom-relatedprotein
Alpha enolase, lungspecific
Mac-2 bindingprotein
Triosephosphat-e isomerase Carbonic anhydrase 1 Myeloblas-tin Peroxisomebiogenesis factor 1
Splice isoform 1 ofmyeloperoxidase
Cytoplasmicantiproteinas-e 2
Alpha-1-acid glycoprotein 1 Calcium-bind-ing protein A12 Similar to SEC14-like protein 2
Ras-related proteinRab-7
Antibacterial proteinFALL-39
Muscarinicacetylcholinereceptor M3
Splice isoform 1 of TranscriptionIntermediary factor 1-gamma
SH3 domain-binding glutamicacid-rich-like protein
Hematopoi-eticlineage cell specific
Putative S100calcium-bindingprotein
11 kDa protein 16 kDaprotein 57 kDa protein
Table 4Possible salivary markers for periodontal diseases.59
Proteins Immunoglobulins Enzymes Others
He lactoferrin IgA Elastase PAFTIMP IgG Amylase 8-OHdGVEGF IgM Dipeptidylpeptidase UrateHGF Alanine aminopeptidase AscorbateFibronectin Arginase CortisolAlbumin b-Glucuronidase NitriteCystatins C, S, A, SN Myeloperoxidase Glycosaminoglycans61
Neopterin Lysozyme Cytokine TNF62
a-2-Macroglobulin MMP-1 Hyaluronic acida-1-Antitrypsin MMP-8(collagenase-2) Chondroitin sulphateKeratin MMP-960 Aspartate aminotransferase (AST)C-reactive protein Chitinase Alkaline phosphatase (ALP)63
Complement C3 Cathepsin G Salivary sCD4464
IL-6 MRP8 and MRP1465
EGF 8-Oxo-7,8-dihydro-2-deoxyguanosine (8-oxodG)66
Defensin-1 Cysteine67
3-Hydroxy fatty acids68
Protein carbonyl (PC)69
572 J. Liu, Y. Duan / Oral Oncology 48 (2012) 569–577
Because oral cancer cells are immersed in the salivary milieu,analysis of the salivary proteomes from OSCC patients is a promis-ing approach to finding biomarkers for the disease. Saliva is an eas-ily accessible fluid compared with tissue obtained from biopsy.Therefore, a large number of saliva samples can be collected andanalyzed, allowing for a robust study with sufficient statisticalpower to reveal true signatures for characteristics of the disease.Because OSCC is a complex disease resulting from an interdepen-dent series of genetic alterations rather than a single decisiveevent, a combination of candidate protein markers can improvethe sensitivity and specificity for OSCC detection.
Periodontal disease
Periodontitis is a group of inflammatory diseases that is charac-terized by loss of connective tissue attachment and bone around theteeth in conjunction with the formation of periodontal pockets due
to the apical migration of the junctional epithelium.27 If left un-treated, the disease continues with progressive bone destruction,leading to tooth mobility and subsequent tooth loss. Periodontaldisease afflicts over 50% of the adult population in the UnitedStates.28 The detection and utilization of molecular biomarkers cor-relating with periodontal disease would permit rapid and accuratediagnoses, dynamic monitoring of disease activity, and potentiallymore effective treatment. Some components of saliva proposed asdisease markers include enzymes (alkaline phosphatase, esterase,glucuronidase, aminopeptidase), immunoglobulins (IgA, IgG), andsteroid hormones. Many of these salivary components appearedto be useful biochemical markers. Saliva analysis, therefore, canbe a cost-effective approach for monitoring the disease. Table 4 listspossible salivary biomarkers for periodontal diseases.
Matrix metalloproteinase-8 (MMP-8) has been identified as amajor tissue-destructive enzyme in periodontal disease. Conse-quently, MMP-8 is a promising candidate for diagnosing and

J. Liu, Y. Duan / Oral Oncology 48 (2012) 569–577 573
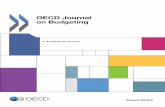
assessing the progression of this episodic disease.29 Research fromHerr et al. discusses the use of clinical point-of-care (POC) diagnos-tic that enables rapid quantitation of an oral disease biomarker inhuman saliva by using a monolithic disposable cartridge designedto operate in a compact analytical instrument. The microfluidicmethod facilitates hands-free saliva analysis by integrating samplepretreatment (filtering, enrichment, mixing) with electrophoreticimmunoassays to quickly measure analyte concentrations in min-imally pretreated saliva samples. Using 20 ll of saliva, they couldrapidly measure (<10 min) the MMP-8 collagen-cleaving enzymeconcentration in saliva from healthy and periodontally diseasedsubjects.30 The microchip electrophoretic immunoassay (lCEI)
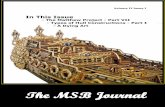
Figure 1A lCEI device layout. Fluid wells are labeled according to contents asfollows: S: sample; B: buffer; SW: sample waste; BW: buffer waste; mAb�:fluorescently labeled monoclonal antibody to MMP-8. Inset shows a 40� bright-field image of the size-exclusion membrane.
Figure 1B On-chip sample enrichment. P1: the detection mixture is loaded againstthe size-exclusion membrane. P2: saliva sample is then loaded, resulting incoenrichment of saliva and aMMP-8� at the size-exclusion membrane. P3: anelectric potential is applied across the membrane, causing the enriched species toelute into the separation channel, thus initiating the electrophoretic immunoassay.Subsequently, the electric potential is switched to omit the membrane from thecurrent path. Current flow is indicated by i.
diagnostic instrument used by Herr et al. relies on photolitho-graphically fabricated molecular sieving gels to enrich samplesand subsequently resolve fluorescent antibodies from MMP-8 com-plex under native electrophoresis conditions. Additional schemat-ics are provided in Fig. 1A and B.
Recently, Lamster et al.31 found a significant correlation be-tween periodontal clinical parameters and salivary b-glucuroni-dase activity. In addition, the total number of white blood cellsand neutrophils in blood was observed to be associated with theconcentration of salivary b-glucuronidase. Conclusively, salivaryb-glucuronidase activity was found to potentially reflect the pres-ence of periodontal disease.
8-Hydroxy-deoxyguanosine (8-OHdG) is a product of oxidativeDNA damage following specific enzymatic cleavage after hydroxyl-ation of the C8 atom in a guanine group. 8-OHdG is one of the mostcommonly used markers for evaluating the damage done bychronic inflammatory diseases. Takane et al.32 collected salivasamples from patients with untreated periodontitis and healthycontrol subjects. Using ELISA, the mean value of 8-OHdG in the sal-iva samples of periodontally diseased subjects was determined tobe higher than that of healthy subjects. Salivary 8-OHdG levels de-creased in response to periodontal therapy and approached themean control values.
Fibronectin is a glycoprotein which mediates adhesion betweencells. Consequently, fibronectin is also involved in the processes ofgrowth, migration and differentiation of the cells. A recent studyclaims that fibronectin in saliva plays a regulatory role in por-phyromonas gingivalis fimbria-mediated pathogenesis in adultperiodontal disease.33 ELISA tests further verified the claim, show-ing that the fibronectin concentrations in saliva of adult periodon-tal patients was significantly lower than that of healthy subjects.
Immunoglobulin A (IgA) is the predominant immunoglobulin insaliva and is categorized into two subclasses: IgA1 and IgA2. IgA1 ispredominantly in serum while IgA2 is found in higher concentra-tions in external secretions such as saliva. Hagewald et al.34 inves-tigated the humoral IgA response in the saliva of aggressiveperiodontitis patients by measuring IgA subclasses and IgA anti-bodies reactive to microorganisms associated with periodontal dis-ease. A significantly lower concentration and secretion rate of totalsalivary IgA2 and IgA1 was found in the aggressive periodontitisgroup.
Several studies have investigated the relationship between gin-gival crevicular fluid (GCF) osteocalcin levels and periodontal dis-ease. Kunimatsu et al.35 reported a positive correlation betweenGCF osteocalcin aminoterminal peptide levels and clinical parame-ters in a crosssectional study of periodontitis and gingivitis pa-tients. Results from another study also revealed a significantlyhigher level of total protein in the GCF of diseased teeth, suggestingthe possibility of using total protein concentration as an indicatorfor periapical disease.36
All of the previously mentioned biomarkers are found in pa-tients with periodontal disease. However, the validity of such spe-cies still needs to be examined with greater detail. Additionally, thediscovery of more biomarkers of disease would always bewelcome.
Cancer
Cancer is a major public health problem in many countries. Cur-rently, one in four deaths in the United States is due to cancer.37 Inaddition, pancreatic cancer prognosis tends to be extremely poor,with one of the lowest survival rates among all cancers. Due to alack of any visible symptoms during the early stages, detectioncapabilities are limited. New strategies and biomarkers for earlydetection are, therefore, desperately needed. Salivary biomarkersfor a variety of cancers have been identified and may provide

Table 5Potential biomarkers for breast cancer detection.70
Blood biomarkers in saliva Biomarkers for breast cancer
c-erbB-2 CSTAVEGF TPT1EGF IGF2BP1CEA GRM1
GRIK1H6PDMDM4S100A8CA6(carbonic anhydrase VI)PsoriasinCortisol and dehydro-epiandrosteronesulphate71
Cancer antigen 15-3 (CA15-3)
574 J. Liu, Y. Duan / Oral Oncology 48 (2012) 569–577
valuable diagnostic information. Zhang et al.38 have conducted aprospective sample collection and retrospective, double-blindedvalidation to evaluate the performance and translational utilitiesof salivary transcriptomic biomarkers for noninvasive detectionof resectable pancreatic cancer. It was found that a combinationof four messenger RNA biomarkers (KRAS, MBD3L2, ACRV1, andDPM1) in saliva supernant could differentiate pancreatic cancerpatients from noncancer subjects.
Recently, prostate cancer has become a major health issue inwestern countries. Excluding cutaneous malignancies, it standsas the most frequent malignant illness in men and the second lead-ing cause of cancer-related mortality.39 Using microparticle en-zyme immunoassay,40 free and total prostate-specific antigen(PSA) levels and the free/total (f/t) ratio in the saliva could be com-pared to those in the serum of normal individuals, patients withbenign prostatic hyperplasia (BPH), and prostate cancer. Whilethere was a significant difference between mean serum and sali-vary levels of free and total PSA, the f/t ratio in both saliva and ser-um were very close among normal subjects. Additionally,glycoprotein biomarkers for human cancers, such as prostate-spe-cific antigen, protein c-erbB-2, cancer antigen (CA) 125, 19-9 and15-3, and carcinoembryonic antigen (CEA), have also been detectedin human saliva. Saliva testing of glycoprotein biomarkers may beanother promising approach to human cancer detection.41
Breast cancer is the most commonly diagnosed form of cancerand the leading cause of cancer death in women today. Clinicallyuseful biomarkers for early detection of breast cancer could leadto a significant reduction in mortality rates. The biomarkers forbreast cancer are listed in Table 5.
The protein c-erbB-2, also known as Her2/neu, is a prognosticbreast cancer marker assayed in tissue biopsies from women diag-nosed with malignant tumors. Present studies suggest that solublefragments of the c-erbB-2 oncogene may be released from the cellsurface and become detectable in patients with carcinoma of thebreast. To determine the diagnostic utility of this oncogene, thesoluble form of the c-erbB-2 protein was assayed in the salivaand serum using ELISA in three different groups of women. Find-ings showed the presence of the c-erbB-2 protein in both the salivaand serum of all three groups of women. Moreover, salivary andserum levels of c-erbB-2 in the cancer patients were significantlyhigher than the salivary and serum levels of healthy control sub-jects and benign tumor patients. These results suggest that the c-erbB-2 protein may have potential use in the initial detectionand/or follow-up screening of breast cancer in women.42
Total protein concentration, lipid peroxidation (LPO) levels andpH values in the saliva of breast cancer patients were also foundlower than those in the saliva of healthy individuals. Tissue factor(TF), known as thromboplastin or Factor III, is considered to be amajor regulator of normal hemostasis and thrombosis. Studieshave shown that TF activity is higher in breast cancer patients than
that in the control group, but the difference may not be statisticallysignificant.43 Another study also showed that the levels of vascularendothelial growth factor (VEGF), epidermal growth factor (EGF)and carcinoembryonic antigen (CEA) in the saliva were signifi-cantly elevated in cancer patients. Conclusively, saliva is believedto be a novel avenue for tumor marker research; and with addi-tional efforts and developments, saliva analysis may be a usefulsupplement to current methods of breast cancer detection.44
Tongue cancer is amongst the most common and fatal types ofcancers in the world. Despite advances in cancer detection andtreatment, the prognosis of squamous cell carcinoma of the tongue(TSCC) has not greatly improved within the last few decades andremains one of the most common and fatal head and neck cancersworldwide. Studies from Masood et al.45 examined the levels of IL-1a, IL-6, IL-8, VEGF-a and TNF-a in saliva using quantitative ELISAin three different groups of individuals (endophytic TSCC patients,exophytic TSCC patients and healthy subjects). Research showsthat all five cytokines were elevated in the endophytic TSCC groupcompared to the other groups. IL-1a, IL-6, TNF-a and VEGF werealso elevated in the exophytic TSCC group compared to the controlgroup. Salivary levels of IL-1a, IL-6, IL-8, VEGF-a and TNF-a, couldserve as potential biomarkers for cancer screening and early detec-tion and can also be used to identify the progression of TSCC. An-other relevant work has demonstrated that salivary adenosinedeaminase (ADA) might be used as a diagnostic tool for earlydetection of squamous cell carcinoma of the tongue.46
Sjögren’s syndrome
Sjögren’s syndrome (SS) is a chronic autoimmune disease, beingcharacterized by epithelial cell destruction due to peri-epithelial Band T lymphocytes infiltrating and targeting multiple organs, par-ticularly the moisture producing exocrine glands. Because salivaryand lachrymal glands are involved, dry mouth (xerostomia) anddry eyes (xerophtalmia) represent the typical clinical symptomsof the disease. Sjögren’s syndrome is one of the three most com-mon autoimmune disorders.
Many changes in SS salivary constituents have been describedpreviously (see Table 6), suggesting that saliva could be used todiagnose the syndrome. Saliva samples gathered from individualswith SS show increased concentrations of Na+, Cl�, IgG, lysozyme,matrix metalloproteinase (MMP)-2 and MMP-9 in parotid saliva,as well as increased concentrations of lactoferrin, IgA, b2-micro-globulin, albumin in both parotid and whole saliva, and increasedconcentrations of kallikrein and cystatins C and S in whole saliva.It has also been indicated that the SS salivary protein profile, con-tains an increased number of inflammatory proteins and decreasednumber of acinar proteins.
MMP-2, MMP-9, TIMP-1, and TIMP-2 levels were measuredusing enzyme-linked immunosorbent assay (ELISA) and sandwichenzyme immunoassay (sandwich EIA). The study found that the ra-tio of MMP-9/TIMP-1 and MMP-9 levels in the saliva were signifi-cantly higher in primary SS (pSS) patients than those in healthysubjects. The results suggest that an increase in the overall MMP-9/TIMP-1 ratio, as opposed to simply an increase in MMP-9, inpSS patients’ saliva strongly correlates with the destruction ofglandular and salivary duct tissues.47
Analyses of parotid and whole saliva using ELISA show the sig-nificant increase in lactoferrin and b2-microglobulin levels amongSS patients. b2-Microglobulin, a light-chain molecule categorizedas a major histocompatibility complex class I antigen, is presenton the membrane surface of many nucleated cells, including infil-trating lymphocytes and salivary gland epithelium. Increased lev-els of this protein in SS saliva may, therefore, relate to salivarygland inflammatory activity rather than lymphocyte numbers.48
Lactoferrin is a product of intercalated ductal cells and scattered

Table 6Alterations of salivary proteins in primary SS.72
Salivarycomponent
a-Amylase Carbonic anhydrase VI Proline-rich Proteins (PRPs) Prolactin-InducibleProtein Precursor (PIP)
Lactoferrin b-2-microglobulin
lg k light chain Polymeric Igreceptor
Change Decreased Decreased Increased IncreasedSalivary
component(1) Lipocalin 1precursor(2) Calgranulin B(3) Phosphatidyl ethanolamine
binding protein
Cystatins (S,SN) Lysozyme CCystatin C
MMP-9/TIMP-1Immunoglobulin A,G
Change Increased Decreased Increased IncreasedSalivary
markerProstaglandin E2ThromboxaneB2 [TxB2]
Interleukin-6 (IL-6)Hyaluronic acid (HA)
Soluble interleukin-2 receptor (sIL-2R)73
Protein-conjugated acrolein74
Change Increased Increased IncreasedSalivarymarker Neopterin75
IFN-a76Gamma-glutamyl-tra-nsferase (GGT)77
Change Increased IncreasedChange Increased Increased
J. Liu, Y. Duan / Oral Oncology 48 (2012) 569–577 575
acinar cells in the parotid gland. Previous studies of SS saliva havereported increases in lactoferrin levels without a clear associationto the amount of lymphocytic infiltration.49 Since lactoferrin levelsincrease in other diseases pertaining to the salivary glands, such asparotitis50 and diabetes,51 it cannot be used independently to diag-nose SS.
T.J. Kramer52 quantified C-X-C motif chemokine 13 (CXCL13)with real-time polymerase chain reaction and enzyme-linkedimmunosorbent assay at various stages of SS disease using primarySS (pSS) and secondary SS (sSS) models. The results show thatCXCL13 transcription and protein levels increase with diseaseseverity in salivary tissue and serum, respectively. Moreover,CXCL13 colocalizes with lymphocytes in salivary tissue. At the latestages of SS, increasing levels of CXCL13 in saliva correlate withthat of blood. Therefore, the therapeutic targeting of CXCL13 mayprovide an innovative approach for managing SS disease.
In SS patients, the salivary concentrations of immunoglobulinIgA and IgG, lactoferrin, b2-microglobulin, eicosanoids (prostaglan-din E2 and Thromboxane B2 [TxB2]), interleukin-6 (IL-6), and hyal-uronic acid (HA) were all elevated compared with control groups.Other studies have even suggested using an increase in salivaryIgA as a criterion for the diagnosis of SS. Furthermore, saliva prote-ome analysis of pSS patients broadly links pSS disease to an in-crease in inflammatory proteins and a decrease in acinar proteincompared to non-SS subjects.53,54 Current diagnosis of pSS requiresa salivary gland biopsy. However, validation of newly discoveredbiomarkers could result in a noninvasive method of pSS diagnosisin the near future.
Although a wide range of potential biomarkers for SS detectionexists, there are still many obstacles to overcome. Several constit-uents of saliva have been evaluated within the last 20 years, butnone have been specific or sensitive enough for the diagnosis ofSS. Saliva, which is produced by three major and numerous minorglands, has great variations in both flow and control among indi-viduals, and, at times, even in the same individual under diverseconditions. Another problem that arises is the use of different typesof saliva in various studies. The way in which saliva is collected,either stimulated or unstimulated, can significantly affect salivacomposition. Furthermore, because the rate of salivary flow fromthe submandibular/sublingual glands in SS patients is slower thanthat of healthy individuals, collecting whole saliva versus salivafrom the parotid/submandibular glands can affect the outcome ofthe study. Lastly, the criteria for selecting SS patients have changedwithin the past few decades. While earlier works have used variouscriteria for enrolling SS patients, a publication from the EuropeanCommunity in 1993 has tightened the standards for SS diagnosis.These guidelines, which have been accepted by most rheumatolo-gists, should be used systematically for future studies.
Prospect
Saliva has great potential for the surveillance of general bodyhealth and disease. To reach the above goal through saliva-baseddiagnostics, a new form of miniaturization technology known as‘‘lab-on-a-chip’’ may help through detecting multiple compoundsin parallel and allows for simultaneous assessment of multiple dis-ease conditions. This technology also provides possibility for point-of-care diagnostics. Moreover, because ‘‘lab-on-a-chip’’ technologyallows for a personal and private diagnosis outside of the labora-tory, such as at home, it may further enhance healthcare delivery,reduce health disparities, and improve access to care. This newtechnology in association with the saliva-based approach, whichis non-invasive, inexpensive, easier, and safer than approachesbased on serum or urine, can significantly impact diseasediagnostics.2
Identifying disease diagnostic markers and successfully trans-lating research efforts from the laboratory into clinic is the greatestchallenge for salivary diagnostics. Candidate biomarkers need to beextensively tested and studied, as much more validation is re-quired. Proteome analysis has provided significant insight, butfaces many obstacles as well. For instance, the sampling efficiencyof LC-MS/MS varies from one experiment to another, with some ofthe target biomarkers identified based on single-peptide assign-ment. Furthermore, due to a dramatic abundance of amylase in hu-man saliva, effective removal of salivary amylases prior toproteome analysis is both necessary and challenging. Clearly, it ischallenging to translate candidate biomarkers from proteomicinvestigations into real-world diagnostic or prognostic applica-tions. However, new diagnostic tools such as nucleic acid and pro-tein microarrays and microfluidics are under development forassessment and comprehensive screening of biomarkers. If appro-priately validated on larger patient cohorts, testing of candidatebiomarkers coupled with microfluidic devices may become a pow-erful tool for oral cancer diagnosis in the future. Device cartridges,which can simplify assay operation and improve assay sensitivityby integrating saliva pretreatment (mixing, incubation, and enrich-ment) with subsequent quantitative analysis, may also be anattractive option.
Solid-phase microextraction (SPME) has gained widespreadacceptance as a means of analyte-matrix separation and samplepreconcentration. Furthermore, it is compatible with other sepa-ration/detection techniques such as gas chromatography and/orhigh performance liquid chromatography, while providing linearresults for a wide range of concentration.55 By taking into con-sideration the proper stationary-phase coating layer, it is possi-ble to reach a low detection limit with minimized matrixinterference.

576 J. Liu, Y. Duan / Oral Oncology 48 (2012) 569–577
Conclusion
Since the collection of saliva is less invasive than that of bloodfor clinical analysis, it has become an attractive diagnostic fluidfor disease. A noninvasive collection method not only simplifies apatient’s ability to take repeated samples for long-term diseasemonitoring, but significantly reduces the pain and anxiety that istypically associated with blood tests. Unlike blood sample, whichis prone to clotting, saliva is much easier to handle and requiresless pre-analysis manipulation. Moreover, secretions from glandswithin the oral cavity contain proteins are uniquely associatedwith saliva. Therefore, compared with serum based biomarkers,salivary proteins may be a more sensitive and specific indicatorfor certain oral diseases.
However, some relevant problems can not be ignored. Manyputative biomarkers in saliva were independently discovered andmust be further validated before clinical availability for becauseall the current individual markers are not sensitive and specific en-ough to meet strict diagnostic criteria. Also, most current pub-lished results are still preliminary and most of these studies wereconducted in a very small number of samples with no specific mar-ker being carefully validated. One possible way to overcome thelimitations of single disease biomarkers is to set up a biomarkerarray to enhance the reproducibility and specificity for diseasemonitoring through simultaneous measurements of multiplebiomarkers. Although large-scale, quantitative, high-throughputproteomics technologies are still in its very early stages, there isa likelihood that new breakthroughs will be made in the future.We highly expect that salivary diagnostics will become a comple-mentary tool in routine health monitoring and early detection ofdiseases in the near future.
Conflict of interest statement
None declared.
References
1. Streckfus CF, Dubinsky WP. Proteomic analysis of saliva for cancer diagnosis.Expert Rev Proteomics 2007;4(3):329–32.
2. Lee YH, Wong DT. Saliva: an emerging biofluid for early detection of diseases.Am J Dent 2009;22(4):241–8.
3. Chiappin S, Antonelli G, Gatti R, De Palo EF. Saliva specimen: a new laboratorytool for diagnostic and basic investigation. Clin Chim Acta 2007;383(1–):30–40.
4. St John MAR, Li Y, Zhou XF, Denny P, Ho CM, Montemagno C, et al. Interleukin 6and interleukin 8 as potential biomarkers for oral cavity and oropharyngealsquamous cell carcinoma. Arch Otolaryngol Head Neck Surg2004;130(8):929–35.
5. Ilyin SE, Belkowski SM, Plata-Salamán CR. Biomarker discovery and validation:technologies and integrative approaches. Trends Biotechnol 2004;22(8):411–6.
6. Silberring J, Ciborowski P. Biomarker discovery and clinical proteomics. Trac-Trend Anal Chem 2010;29(2):128–40.
7. Griffiths HR, Moller L, Bartosz G, Bast A, Bertoni-Freddari C, Collins A, et al.Biomarkers. Mol Aspects Med 2002;23(1–3):101–208.
8. Bonassi S, Neri M, Puntoni R. Validation of biomarkers as early predictors ofdisease. Mutat Res-Fund Mol M 2001;480–481:349–58.
9. Guo T, Rudnick PA, Wang WJ, Lee CS, Devoe DL, Balgley BM. Characterization ofthe human salivary proteome by capillary isoelectric focusing/nanoreversed-phase liquid chromatography coupled with ESI-tandem MS. J Proteome Res2006;5(6):1469–78.
10. Washburn MP, Wolters D, Yates JR. Large-scale analysis of the yeast proteomeby multidimensional protein identification technology. Nat Biotechnol2001;19(3):242–7.
11. Xie HW, Rhodus NL, Griffin RJ, Carlis JV, Griffin TJ. A catalogue of human salivaproteins identified by free flow electrophoresis-based peptide separation andtandem mass spectrometry. Mol Cell Proteomics 2005;4(11):1826–30.
12. Huang CM. Comparative proteomic analysis of human whole saliva. Arch OralBiol 2004;49(12):951–62.
13. Amado FML, Vitorino RMP, Domingues P, Lobo MJC, Duarte JAR. Analysis of thehuman saliva proteome. Expert Rev Proteomics 2005;2(4):521–39.
14. Ghafouri B, Tagesson C, Lindahl M. Mapping of proteins in human saliva usingtwo-dimensional gel electrophoresis and peptide mass fingerprinting.Proteomics 2003;3(6):1003–15.
15. Schipper R, Loof A, de Groot J, Harthoorn L, Dransfield E, van Heerde W. SELDI-TOF-MS of saliva: methodology and pre-treatment effects. J Chromatogr BAnalyt Technol Biomed Life Sci 2007;847(1):45–53.
16. Hardt M, Thomas LR, Dixon SE, Newport G, Agabian N, Prakobphol A, et al.Toward defining the human parotid gland salivary proteome and peptidome:identification and characterization using 2D SDS-PAGE, ultrafiltration, HPLC,and mass spectrometry. Biochemistry 2005;44(8):2885–99.
17. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA-Cancer JClin 2005;55(2):74–108.
18. Hou XL, Deng DL, Wu X, Lv Y, Zhang JY. Simultaneous stacking of cationic andanionic compounds in single run capillary zone electrophoresis by two-endfield amplified sample injection. J Chromatogr A 2010;1217(35):5622–7.
19. Franzmann EJ, Reategui EP, Pedroso F, Pernas FG, Karakullukcu BM, CarrawayKL, et al. Soluble CD44 is a potential marker for the early detection of head andneck cancer. Cancer Epidemiol Biomarkers Prev 2007;16(7):1348–55.
20. Zhong LP, Zhang CP, Zheng JW, Li J, Chen WT, Zhang ZY. Increased Cyfra 21–1concentration in saliva from primary oral squamous cell carcinoma patients.Arch Oral Biol 2007;52(11):1079–87.
21. Nagler R, Bahar G, Shpitzer T, Feinmesser R. Concomitant analysis of salivarytumor markers – A new diagnostic tool for oral cancer. Clin Cancer Res2006;12(13):3979–84.
22. Tavassoli M, Brunel N, Maher R, Johnson NW, Soussi T. p53 antibodies in thesaliva of patients with squamous cell carcinoma of the oral cavity. Int J Cancer1998;78(3):390–1.
23. Jou Y-J, Lin C-D, Lai C-H, Chen C-H, Kao J-Y, Chen S-Y, et al. Proteomicidentification of salivary transferrin as a biomarker for early detection of oralcancer. Anal Chim Acta 2010;681(1–2):41–8.
24. Tan W, Sabet L, Li Y, Yu T, Klokkevold PR, Wong DT, et al. Optical protein sensorfor detecting cancer markers in saliva. Biosens Bioelectron 2008;24(2):266–71.
25. Shintani S, Hamakawa H, Ueyama Y, Hatori M, Toyoshima T. Identification of atruncated cystatin SA-I as a saliva biomarker for oral squamous cell carcinomausing the SELDI ProteinChip platform. Int J Oral Maxillofac Surg2010;39(1):68–74.
26. Shen Hu, Martha Arellano, Boontheung Pinmanee. Salivary proteomics for oralcancer biomarker discovery. Clin Cancer Res 2008;14:6246–52.
27. Ozmeric N. Advances in periodontal disease markers. Clin Chim Acta2004;343(1–2):1–16.
28. Albandar JM. Periodontal diseases in North America. Periodontol 20002002;29(1):31–69.
29. Kiili M, Cox SW, Chen HW, Wahlgren J, Maisi P, Eley BM, et al. Collagenase-2(MMP-8) and collagenase-3 (MMP-13) in adult periodontitis: molecular formsand levels in gingival crevicular fluid and immunolocalisation in gingival tissue.J Clin Periodontol 2002;29(3):224–32.
30. Herr AE, Hatch AV, Throckmorton DJ, Tran HM, Brennan JS, Giannobile WV,et al. Microfluidic immunoassays as rapid saliva-based clinical diagnostics. ProcNatl Acad Sci U S A 2007;104(13):5268–73.
31. Lamster IB, Kaufman E, Grbic JT, Winston LJ, Singer RE. Beta-glucuronidaseactivity in saliva: relationship to clinical periodontal parameters. J Periodont2003;74(3):353–9.
32. Takane M, Sugano N, Iwasaki H, Iwano Y, Shimizu N, Ito K. New biomarkerevidence of oxidative DNA damage in whole saliva from clinically healthy andperiodontally diseased individuals. J Periodont 2002;73(5):551–4.
33. Murakami Y, Hanazawa S, Tanaka S, Iwahashi H, Kitano S, Fujisawa S.Fibronectin in saliva inhibits Porphyromonas gingivalis fimbria-inducedexpression of inflammatory cytokine gene in mouse macrophages. FEMSImmunol Med Microbiol 1998;22(3):257–62.
34. Hagewald S, Bernimoulin JP, Kottgen E, Kage A. Salivary IgA subclasses andbacteria-reactive IgA in patients with aggressive periodontitis. J Periodontal Res2002;37(5):333–9.
35. Kunimatsu K, Mataki S, Tanaka H, et al. A cross-sectional study on osteocalcinlevels in gingival crevicular fluid from periodontal patients. J Periodont1993;64(9):865–9.
36. Burgener B, Ford AR, Situ H, Fayad MI, Hao JJ, Wenckus CS, et al. Biologicmarkers for odontogenic periradicular periodontitis. J Endodont2010;36(8):1307–10.
37. Jemal A, Siegel R, Ward E, Murray T, Xu JQ, Thun MJ. Cancer statistics, 2007. CA-Cancer J Clin 2007;57(1):43–66.
38. Zhang L, Farrell JJ, Zhou H, Elashoff D, Akin D, Park NH, et al. Salivarytranscriptomic biomarkers for detection of resectable pancreatic cancer.Gastroenterology 2010;138(3):U194–949.
39. Jemal A, Tiwari RC, Murray T, Ghafoor A, Samuels A, Ward E. Cancer statistics.CA-Cancer J Clin 2004;54(1):8–29.
40. Turan T, Demir S, Aybek H, Atahan O, Tuncay OL, Aybek Z. Free and totalprostate-specific antigen levels in saliva and the comparison with serum levelsin men. Eur Urol 2000;38(5):550–4.
41. Hu S, Loo JA, Wong DT. Human saliva proteome analysis and disease biomarkerdiscovery. Expert Rev Proteomics 2007;4(4):531–8.
42. Streckfus C, Bigler L, Dellinger T, Dai XL, Kingman A, Thigpen JT. The presence ofsoluble c-erbB-2 in saliva and serum among women with breast carcinoma: apreliminary study. Clin Cancer Res 2000;6(6):2363–70.
43. Emekli-Alturfan E, Demir G, Kasikci E, Tunali-Akbay T, Pisiriciler R, Caliskan E,et al. Altered biochemical parameters in the saliva of patients with breastcancer. Tohoku J Exp Med 2008;214(2):89–96.
44. Brooks MN, Wang JG, Yang L, Zhang R, Elashoff D, Wong DT. Salivaryprotein factors are elevated in breast cancer patients. Mol Med Rep2008;1(3):375–8.

J. Liu, Y. Duan / Oral Oncology 48 (2012) 569–577 577
45. Alexis Korostoff Lindsay Reder, Masood Rizwan, Sinha Uttam K. The role ofsalivary cytokine biomarkers in tongue cancer invasion and mortality. OralOncol 2011;47(4):282–7.
46. Rai B, Kaur J, Jacobs R, Anand SC. Adenosine deaminase in saliva as a diagnosticmarker of squamous cell carcinoma of tongue. Clin Oral Investig2011;15(3):347–9.
47. Asatsuma M, Ito S, Watanabe M, Takeishi H, Nomura S, Wada Y, et al. Increasein the ratio of matrix metalloproteinase-9 to tissue inhibitor ofmetalloproteinase-1 in saliva from patients with primary Sjögren’s syndrome.Clin Chim Acta 2004;345(1–2):99–104.
48. Tishler M, Yaron I, Shirazi I, Yaron M. Saliva: an additional diagnostic tool inSjogren’s syndrome. Semin Arthritis Rheum 1997;27(3):173–9.
49. Konttinen YT, Kulomaa M, Malmström M, Kilpi A, Reitamo S. Lactoferrin inSjögren’s syndrome. Arthritis Rheum 1984;27(4):462–7.
50. Tabak L, Mandel ID, Karlan D, Baurmash H. Alterations in lactoferrin in salivarygland disease. J Dent Res 1978;57(1):43–7.
51. Dodds MWJ, Yeh CK, Johnson DA. Salivary alterations in type 2 (non-insulin-dependent) diabetes mellitus and hypertension. Community Dentist OralEpidemiol 2000;28(5):373–81.
52. Jill M, Kramer DDS, Thomas L. CXCL13 in SJöGren syndrome: a novel biomarkerof disease. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110(6):e15.
53. Ryu OH, Atkinson JC, Hoehn GT, Illei GG, Hart TC. Identification of parotidsalivary biomarkers in Sjogren’s syndrome by surface-enhanced laserdesorption/ionization time-of-flight mass spectrometry and two-dimensionaldifference gel electrophoresis. Rheumatology 2006;45(9):1077–86.
54. Hu S, Wang JH, Meijer J, Leong S, Xie YM, Yu TW, et al. Salivary proteomic andgenomic biomarkers for primary Sjogren’s syndrome. Arthritis Rheum2007;56(11):3588–600.
55. Ashwini Kumar, Ashok Kumar Malik, Matysik FM. Analysis of biologicalsamples using solid-phase microextraction. Bioanal Rev 2009;1:35–55.
56. Nagler RM. Saliva as a tool for oral cancer diagnosis and prognosis. Oral Oncol2009;45(12):1006–10.
57. Li Y, St John MAR, Zhou X, Kim Y, Sinha U, Jordan RCK, et al. Salivarytranscriptome diagnostics for oral cancer detection. Clin Cancer Res2004;10(24):8442–50.
58. Shpitzer T, Hamzany Y, Bahar G, Feinmesser R, Savulescu D, Borovoi I, et al.Salivary analysis of oral cancer biomarkers. Br J Cancer 2009;101(7):1194–8.
59. Ozmeric N. Advances in periodontal disease markers. Clin Chim Acta2004;343(1–2):1–16.
60. Rai B, Kaur J, Jain R, Anand SC. Levels of gingival crevicular metalloproteinases-8 and -9 in periodontitis. Saudi Dent J 2010;22(3):129–31.
61. Last KS, Stanbury JB, Embery G. Glycosaminoglycans in human gingivalcrevicular fluid as indicators of active periodontal disease. Arch Oral Biol1985;30(3):275–81.
62. Rossomando EF, Kennedy JE, Hadjimichael J. Tumour necrosis factor alpha ingingival crevicular fluid as a possible indicator of periodontal disease inhumans. Arch Oral Biol 1990;35(6):431–4.
63. Totan A, Greabu M, Totan C, Spinu T. Salivary aspartate aminotransferase,alanine aminotransferase and alkaline phosphatase: possible markers inperiodontal diseases? Clin Chem Lab Med 2006;44(5):612–5.
64. Ghallab N, Shaker O. Salivary-soluble CD44 levels in smokers and non-smokerswith chronic periodontitis: a pilot study. J Periodont 2010;81(5):710–7.
65. Kojima T, Andersen E, Sanchez JC, Wilkins MR, Hochstrasser DF, Pralong WF,et al. Human gingival crevicular fluid contains MRP8 (S100A8) and MRP14(S100A9), two calcium-binding proteins of the S100 family. J Dent Res2000;79(2):740–7.
66. Cooke MS, Singh R, Hall GK, Mistry V, Duarte TL, Farmer PB, et al. Evaluation ofenzyme-linked immunosorbent assay and liquid chromatography-tandemmass spectrometry methodology for the analysis of 8-oxo-7,8-dihydro-20-deoxyguanosine in saliva and urine. Free Radical Bio Med 2006;41(12):1829–36.
67. Zappacosta B, Manni A, Persichilli S, Boari A, Scribano D, Minucci A, et al.Salivary thiols and enzyme markers of cell damage in periodontal disease. ClinBiochem 2007;40(9–10):661–5.
68. Ferrando R, Szponar B, Sánchez A, Larsson L, Valero-Guillén PL. 3-Hydroxy fattyacids in saliva as diagnostic markers in chronic periodontitis. J Microbiol Meth2005;62(3):285–91.
69. BaltacIoglu E, AkalIn FA, Alver A, Deger O, Karabulut E. Protein carbonyl levelsin serum and gingival crevicular fluid in patients with chronic periodontitis.Arch Oral Biol 2008;53(8):716–22.
70. Zhang L, Xiao H, Karlan S, Zhou H, Gross J, Elashoff D, et al. Discovery andpreclinical validation of salivary transcriptomic and proteomic biomarkers forthe non-invasive detection of breast cancer. PLoS One 2010;5(12):e15573.
71. Read GF, Wilson DW, Campbell FC, Holliday HW, Blamey RW, Griffiths K.Salivary cortisol and dehydroepiandrosterone sulphate levels inpostmenopausal women with primary breast cancer. J Cancer Clin Oncol1983;19(4):477–83.
72. Baldini C, Giusti L, Bazzichi L, Lucacchini A, Bombardieri S. Proteomic analysisof the saliva: a clue for understanding primary from secondary Sjögren’ssyndrome? Autoimmun Rev 2008;7(3):185–91.
73. Tishler M, Yaron I, Shirazi I, Levartovsky D, Yaron M. Salivary and serum solubleinterleukin-2 receptor in primary Sjogren’s syndrome. Arch Oral Biol1999;44(4):305–8.
74. Higashi K, Yoshida M, Igarashi A, Ito K, Wada Y, Murakami S, et al. Intensecorrelation between protein-conjugated acrolein and primary Sjogren’ssyndrome. Clin Chim Acta 2010;411(5–6):359–63.
75. Sfriso P, Ostuni P, Botsios C, Andretta M, Oliviero F, Punzi L, et al. Serum andsalivary neopterin and interferon-gamma in primary Sjogren’s syndrome –Correlation with clinical, laboratory and histopathologic features. Scand JRheumatol 2003;32(2):74–8.
76. Zheng L, Zhang Z, Yu C, Tu L, Zhong L, Yang C. Association between IFN-[alpha]and primary Sjogren’s syndrome. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2009;107(1):e12–8.
77. Jiménez-Alonso J, Sabio JM, Rivera-Cívico F, Martín-Armada M, Rodríguez MÁ,Jáimez L, et al. Salivary and serum [beta]2-microglobulin and gamma-glutamyl-transferase in patients with primary Sjögren syndrome and Sjögrensyndrome secondary to systemic lupus erythematosus. Clin Chim Acta2003;334(1–2):225–31.