Joshua Medow MD, MS Christopher Nickele MD, Christy Hunter,RN,CCRN, Patricia Chesmore,RN,CCRN, Tammy...
28
Joshua Medow MD, MS Christopher Nickele MD, Christy Hunter,RN,CCRN, Patricia Chesmore,RN,CCRN, Tammy Kundinger,RT, William Tanke,PharmD, Gabriel Norgaard,BS, Tony Frey,BS Doug Miller Symposium April 25, 2013 USING THE ELECTRONIC MEDICAL RECORD TO MAXIMIZE PRACTICE EFFICIENCY IN ORGAN DONATION
-
Upload
frederick-wright -
Category
Documents
-
view
216 -
download
2
Transcript of Joshua Medow MD, MS Christopher Nickele MD, Christy Hunter,RN,CCRN, Patricia Chesmore,RN,CCRN, Tammy...

Joshua Medow MD, MS Christopher Nickele MD, Christy Hunter,RN,CCRN, Patricia Chesmore,RN,CCRN, Tammy Kundinger,RT,
William Tanke,PharmD, Gabriel Norgaard,BS, Tony Frey,BS
Doug Miller Symposium
April 25, 2013
USING THE ELECTRONIC MEDICAL RECORD TO MAXIMIZE PRACTICE EFFICIENCY IN
ORGAN DONATION

DISCLOSURE
• The authors of this presentation have no financial or ethical conflicts to disclose
OUTLINE
• Efficiency
• The use of protocols
• Abilities of the EMR
• Order sets to increase efficiency
• Other avenues to increase efficiency

DEMANDS ON TIME
OR ER
ICU
Documentation
Outpatient Calls
General Care

PROTOCOLS
• Nursing care
• Physician input up front
• Triggers for call to physician
• Requires nursing to implement
• Computerized protocols versus paper1
1. J Burn Care Res. 2011 ; 32(2): 246–255. doi:10.1097/BCR.0b013e31820aaebf
THE TEAM
• Neurocritical Care
• Physician
• Nursing
• Respiratory Care
• Pharmacy
• Hospital IT
BRAIN DEAD DONOR (BDD)
• Optimizing care
• Critical care team efficiency
• Managing parameters / metric driven

DONATION AFTER CARDIAC DEATH (DCD) DONOR
• Donor comfort
• Optimizing care
• Critical care team efficiency
• Managing parameters/metric driven

PROTOCOLS – BDD LUNG PROTECTIVE

PROTOCOLS – DCD LUNG PROTECTIVE

PROTOCOLS – VASOACTIVE ALGORITHM

PROTOCOLS – VASCULAR VOLUME MAINTENANCE1. Obtain weight in kg
2. If weight is > 20 kg skip to step 5
3. If weight is > 10 kg skip to step 7
4. Multiply weight by 4 and skip to step 10
5. Subtract 20 from weight
6. Add 60 to result and skip to step 10
7. Subtract 10 from weight
8. Multiply result by 2
9. Add 40
10. This is the rate to maintenance (.9ns+20k.) IVF at
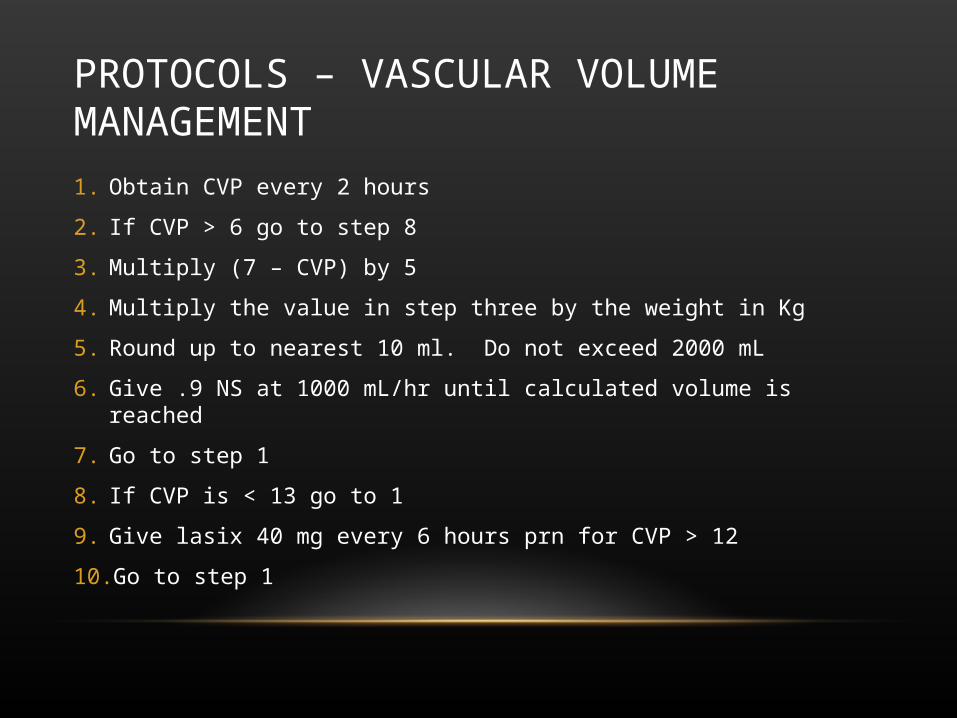
PROTOCOLS – VASCULAR VOLUME MANAGEMENT1. Obtain CVP every 2 hours
2. If CVP > 6 go to step 8
3. Multiply (7 – CVP) by 5
4. Multiply the value in step three by the weight in Kg
5. Round up to nearest 10 ml. Do not exceed 2000 mL
6. Give .9 NS at 1000 mL/hr until calculated volume is reached
7. Go to step 1
8. If CVP is < 13 go to 1
9. Give lasix 40 mg every 6 hours prn for CVP > 12
10. Go to step 1

PROTOCOLS – FREE WATER DEFICIT CORRECTION1. Obtain serum sodium.
2. If serum sodium < 151 skip to step #9.
3. Divide patient admit weight by 2. (VL = patient weight / 2).
4. Number of L of D5W to replace: LD5 = VL – ((150 * VL)/serum sodium).
5. Number of mL of D5W to replace: MLD5 = LD5 * 1000.
6. Round MLD5 to nearest 10 mL.
7. Administer MLD5 at a rate of 500 mL / hour until infusion completed.
8. Wait 2 hours and return to step #1.
9. Obtain serum sodium every 6 hours.
10. If serum sodium > 150 and U.O. > 250 mL/hr give ddAVP 1 mcg every 3 hours and return to step #3.
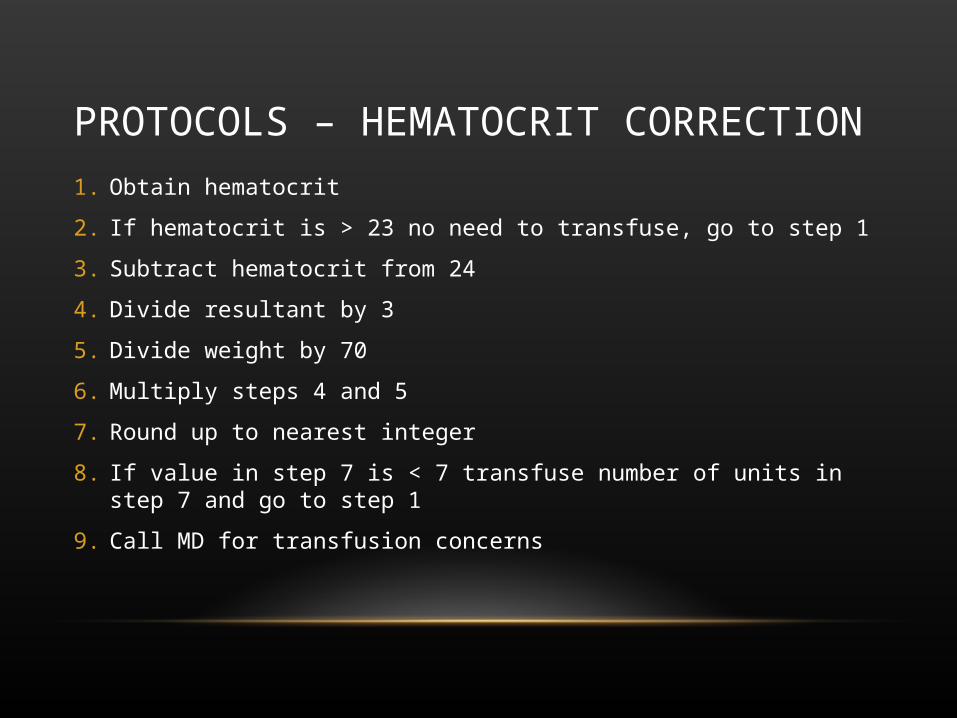
PROTOCOLS – HEMATOCRIT CORRECTION1. Obtain hematocrit
2. If hematocrit is > 23 no need to transfuse, go to step 1
3. Subtract hematocrit from 24
4. Divide resultant by 3
5. Divide weight by 70
6. Multiply steps 4 and 5
7. Round up to nearest integer
8. If value in step 7 is < 7 transfuse number of units in step 7 and go to step 1
9. Call MD for transfusion concerns
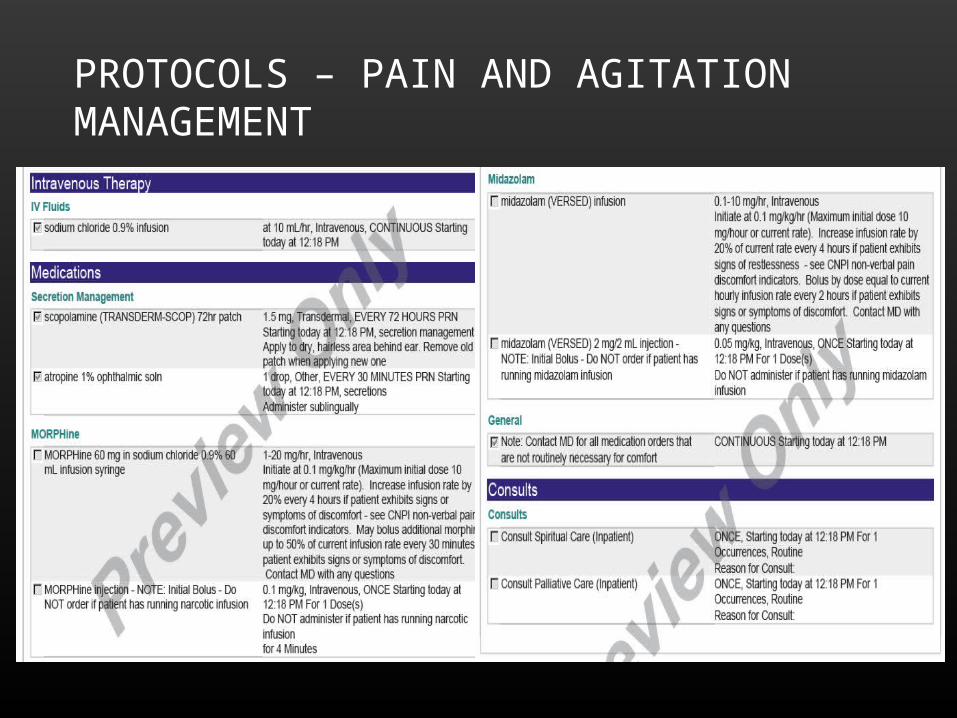
PROTOCOLS – PAIN AND AGITATION MANAGEMENT

PROTOCOL – PAIN / AGITATION SCORES FOR DOSINGValidated Sedation / Agitation Score Table Used for Midazolam Dosing
Validated Nonverbal Pain Score Table Used for Morphine Dosing

CAPABILITIES
• Can follow new labs/vitals instantly
• Notify nurses instantly
• Can generate pages to physician automatically
• When protocol fails
• When issue needs special attention
• Meds, transfusions, etc.

PURPOSE
• Optimize patient care (organs per donor)
• Efficiency (collected data)
• Hours billed
• Pages generated
• Physician and nurse satisfaction with process
METHODS
• Tracked critical care hours billed
• Tracked pages generated
• Tracked organs procured per donor
• Developed order sets
• Brain Dead Donation
• Donation after Cardiac Death
• EpicCare (Epic Systems Corporation, Verona, WI)
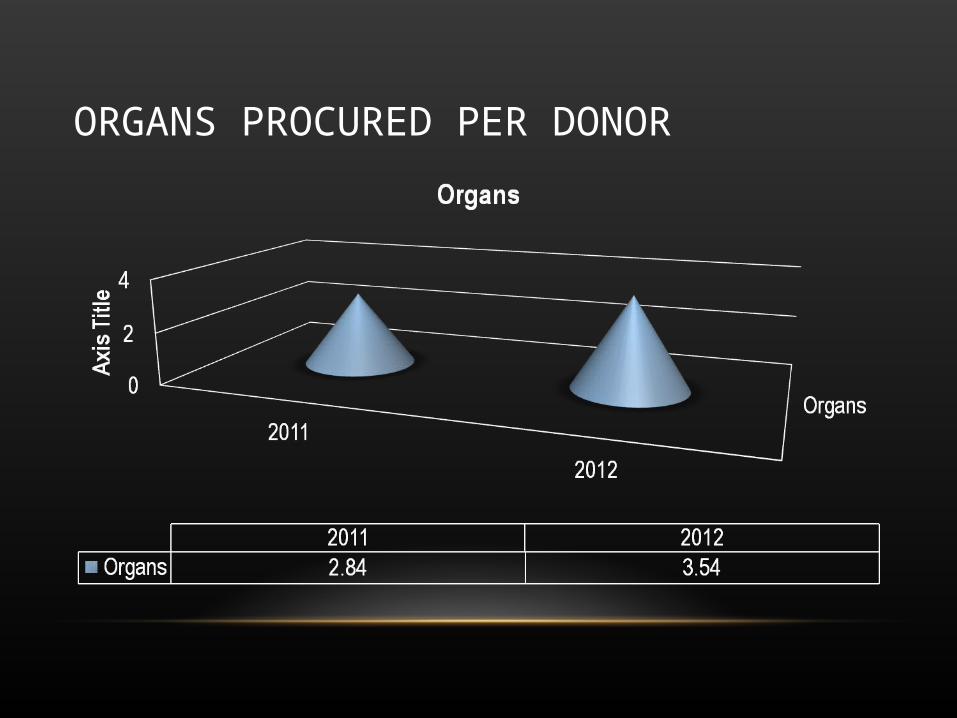
ORGANS PROCURED PER DONOR

CRITICAL CARE CHARGES
• First Hour
• Milwaukee/Chicago 80th percentile 2010 $961
• Madison 80th percentile 2010 $747
• Subsequent Half Hour
• Milwaukee/Chicago $471
• Madison $373

ORDER SET #1
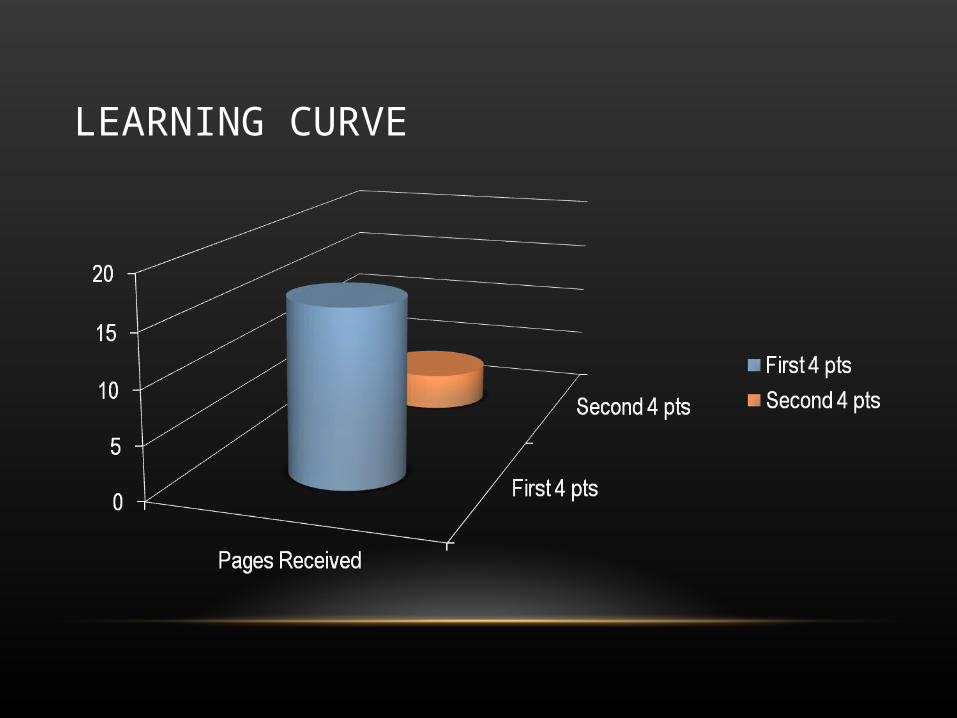
LEARNING CURVE

ORDER SET #2

PROJECT SCOPE
• Single example in the neuro ICU
• Not designed to show patient outcomes
• Donation success rate

CONCLUSIONS
• EMR can change your practice
• Use order sets to their full potential
• Applications to sepsis, ARDS, etc.
• Algorithms must be carefully vetted

THANK YOU