Jordan Health Communication Partnership Johns Hopkins … · Jordan Health Communication...
17
Evaluation of the Arab Women Speak Out TM (AWSO TM ) Initiative - 2 nd Tier (Phase II) - in Irbid Governorate, Jordan, 2012 Jordan Health Communication Partnership Johns Hopkins Bloomberg School of Public Health Center for Communication Programs, JHUCCP July 2012
-
Upload
nguyenkiet -
Category
Documents
-
view
215 -
download
0
Transcript of Jordan Health Communication Partnership Johns Hopkins … · Jordan Health Communication...
Evaluation of the Arab Women Speak OutTM (AWSOTM) Initiative - 2nd
Tier (Phase II) - in Irbid Governorate, Jordan, 2012
Jordan Health Communication Partnership
Johns Hopkins Bloomberg School of Public Health
Center for Communication Programs, JHUCCP
July 2012
1
Table of Contents
Table of Contents ___________________________________________________________________________ 1
Acknowledgements __________________________________________________________________________ 2
Executive Summary __________________________________________________________________________ 3
Introduction ________________________________________________________________________________ 5
Arab Women Speak OutTM
: Background ___________________________________________________ 5
AWSOTM
: 2nd Tier, Phase I ______________________________________________________________ 6
AWSOTM
: 2nd Tier, Phase II _____________________________________________________________ 6
Methodology ________________________________________________________________________ 7
Questionnaire ________________________________________________________________________ 7
Data collection, entry, and analyses ______________________________________________________ 7
Findings 7
Sample Characteristics _________________________________________________________________ 7
Exposure to AWSOTM
__________________________________________________________________ 7
Message 1: Roles of Arab women/Jordanian women and demands of the new life ________________ 9
Message 2: Planning for the future _______________________________________________________ 9
Message 3: Participation of men and women in planning their family and securing its health _______ 10
Message 4: Family planning and the benefits of small families ________________________________ 10
Message 5: How to protect the health of the mother and child/ antenatal care __________________ 10
Message 6: How to protect the health of the mother and child/ postpartum follow-up and immunizations ______________________________________________________________________ 11
Message 7: Breast cancer _____________________________________________________________ 11
Message 8: Healthy lifestyles ___________________________________________________________ 12
Summative Exposure and Effect ________________________________________________________ 12
Summative Message and Story Recall _______________________________________________ 12
Self-reported Benefit from Exposure to Stories/Messages _______________________________ 12
Discussion with Others ________________________________________________________________ 13
Reception and Utilization of the Referral Card _____________________________________________ 14
Limitations ________________________________________________________________________________ 14
Conclusions _______________________________________________________________________________ 14
Recommendations _________________________________________________________________________ 15
2
Acknowledgements Special thanks are due to the Jordan National Forum for Women (JNFW) for their implementation of the AWSOTM training program and the community sessions. The JNFW also worked with community members, mainly women, to encourage positive health behaviors. In particular, thanks are extended to HE May Abu Al-Samen, Samar Al-Shahwan, Ghada Telhab, Yaseen Al Zou’bi and all AWSOTM trainers from Irbid. Appreciation goes to the Irbid Health Project Steering Committee, Chaired by Governor Dr. Raed Adwan, for facilitating the implementation of this program within the different districts in Irbid. Sincere thanks go to Ms. Huda Murad, Behavioral Change Communication for Service Delivery and Community Interventions Senior Specialist, for her commitment and leadership throughout the training, implementation and monitoring of the program. Dr. Carol Underwood, PhD, Senior Research Advisor, and Ms. Sarah Kamhawi, MPH, Monitoring and Evaluation Program Office, wrote this report. Overall, the JHU·CCP provided technical assistance and coordination of the study. Special thanks are due to all JHCP staff who cooperated with and supported the research team throughout the study, including Mr. Edson Whitney, JHCP Chief of Party; Ms. Rula Dajani, JHCP Deputy Chief of Party; Ms. Bushra Jabre, Senior Communication Advisor at JHU·CCP, for reviewing and commenting on the report, and Ms. Lina Qardan, Senior Technical and Advocacy Advisor, for reviewing the questionnaires and study report. Accurate Opinion for Public Opinion Measurements, Co. was subcontracted to provide technical assistance for data entry. Thanks are extended to Mr. Yaser Sa’ad Edin, Executive Manager.
3
Executive Summary
Introduction The Arab Women Speak OutTM (AWSOTM) training program is a key component of the JHCP’s flagship program, “Hayati Ahla.” To expand the reach of AWSOTM, the JHCP developed a set of eight flashcards with the key messages discussed during the AWSOTM sessions. These flashcards were distributed during the AWSO workshops (1st Tier) to the participants, who were asked to use these flashcards to convey core AWSOTM messages to 10-15 neighbors, family and friends (2nd Tier). A total of 17,114 women received messages using the flashcards during Phase II according to the logs kept by 1st Tier participants. This report presents the findings from an evaluation study of AWSOTM 2nd Tier, Phase II outreach in Irbid Governorate. Methodology A random sample was generated from the logs; 408 women were contacted and interviewed by telephone in May 2012. Operational Definitions 1st tier workshop: The community-based discussion groups facilitated by a woman who attended the Train the Trainers workshop. Each workshop comprised approximately 20 women; six modules were covered over a period of three days. 2nd tier: 10-15 neighbors, family and friends who received AWSOTM messages from 1st tier women. Phase I: 2nd tier message dissemination by women who attended 1st tier workshops during December 2011- January 2012. These women were given flashcards. Phase II: 2nd tier message dissemination by women who attended 1st tier workshops during April-June 2012. These women were provided with the flashcards and were given an incentive to disseminate messages. Key Findings
46% of respondents had heard of AWSOTM
40% reported receiving a message related to AWSOTM or Hayati Ahla from a neighbor, relative or friend during the previous month
Eight topics were conveyed on the flashcards through a total of 13 messages or stories.
80% of message recipients recalled the message that women have the right to make family-related decisions; well over 90% of the women said they intend to or already take part in family-related decisions.
76% recalled the message regarding the importance of planning for the future; exposed compared with non-exposed respondents were significantly more likely to have an action plan.
90% heard the message that women wait until they are at least 18 and men until 22 years of age before marrying for a happy, healthy and stable married life; over 90% of all participants reported that they had already, or intend to, convey this message to young people in their lives regardless of whether they had heard the 2nd Tier messages or not.
91% recalled hearing about the benefits of family planning and of small families. Over 90% of all respondents report positive attitudes about the use of modern contraception as well as the benefits of a small family. 40% of message recipients compared with 35% of non-exposed respondents are current users of modern contraception (difference not significant).
94% reported hearing a message about breast cancer prevention; about 90% of exposed women compared to 76% of non-exposed women reported knowing how to conduct a breast self-exam (BSE), which reached statistical significance. Message recipients were also more likely to report that they had already conducted a BSE; again, a significant difference.
4
80% of 2nd Tier message recipients heard the healthy lifestyles message; 61% of exposed and 49% of non-exposed respondents reported that they already exercise or adhere to a proper diet (statistically significant difference).
Utilization of research findings
These findings will be used to advise other institutions who aim to utilize the AWSOTM training module in Jordan and other settings.
Recommendations
Several of the messages have become normative in Jordanian society, so could be incorporated into the way women are portrayed in future programming, but do not need to be repeated in any specific messages:
o Women’s right to make family-related decisions, o Delay of marriage until at least 18 years of age for women and 22 years of age for
men, and o Importance of prenatal and postnatal care.
Conduct formative research in order to identify new messages that are not normative.
Strengthen the association between AWSOTM and the disseminated messages.
Re-assess the utilization of promotional materials.
5
Introduction
The Jordan Health Communication Partnership (JHCP) Program aims to increase awareness of the importance of family planning (FP) and family health through the campaign “Hayati Ahla” which has been underway at the national level in Jordan since 2007. The Arab Women Speak OutTM (AWSOTM) training program is one component of the “Hayati Ahla” national program.
Arab Women Speak OutTM: Background The AWSOTM training introduces and encourages participants to explore relevant subjects through participatory exercises and presentations of real-life situations to which participants can relate. This setting allows participants to discuss their needs as it helps them by illustrating the importance of health-related decisions in their everyday lives. It is designed to help members of the local community adopt behavioral patterns that can keep them healthy and improve the quality of their lives and those of their families. AWSOTM focuses on issues that are of interest to the individual, the family and the local community in terms of health, economics, social aspects and changing social and gender roles in the Jordanian society. It also covers the acquisition of community development skills by individuals, community organizations and different establishments working in the community itself for the purpose of attaining health efficacy and social wellbeing. AWSOTM has been implemented in a wide range of Arab countries since 1999. An impact evaluation of AWSOTM conducted in 2000 in Egypt, Jordan and Yemen found that participants compared with non-participants were 2.5 times more likely to have taken part in community health activities and 2.3 times more likely to have started their own businesses over the previous 12 months, holding
background characteristics constant, among other findings.1 JHCP capitalized on this success, revising the program to focus more specifically on maternal and child health, family planning and reproductive health while retaining some of the key modules on decision-making and negotiating skills. In 2010, an evaluation of AWSOTM was conducted in Zarqa governorate. That study found that, even a year after participating in AWSOTM, participants expressed significantly higher knowledge regarding important concepts such as gender-related concepts, gender equity, and FP. Although traditionally for women only, AWSOTM was conducted with men in Zarqa as well as with women (though in separate sessions), and was effective with that audience as well. For details, please see JHCP’s report, “Evaluation of the Arab Women Speak OutTM (AWSOTM) Initiative in Zarqa Governorate, Jordan, 2009-2010.” The JHCP also implemented AWSOTM in the governorate of Irbid from April to August 2011 and from January to April 2012. About 3,000 women participated in the workshops during this time period. An evaluation was conducted with the first phase of AWSOTM implementation in Irbid (those who participated from April to August 2011). The evaluation found that participants expressed significantly higher knowledge about the topics discussed during the workshops and they were more likely to adopt the small-family size ideal as compared to the baseline measure. For details, please see JHCP’s report, “Evaluation of the Arab Women Speak OutTM (AWSOTM) Initiative in Irbid Governorate, Jordan, 2011.”
1 Underwood, C. & Jabre, B. 2008. "Enabling Women's Agency: Arab Women Speak Out
TM.” Journal of Communication for
Development and Social Change. 2(2): 13-32.
6
AWSOTM: 2nd Tier, Phase I
To increase the reach of AWSOTM, the JHCP developed a set of flashcards to distribute to the women who attend the workshops (1st Tier). Each of the eight flashcards carries a key message, including a call for action, from the AWSOTM training module. The flashcards also include stories depicted in simple cartoon drawings. These flashcards were distributed to those who attended the 1st Tier step-down workshops. Each woman was trained to use the flashcards and was asked to deliver the messages to 10-15 women from her neighborhood or family. Each set of flashcards included a registration sheet to be completed by the woman disseminating the messages. The woman was instructed to record the names and demographics of those to whom she delivered messages along with a specification of which women were given a referral card to the health centers. This process was first implemented during December of 2011. During December of 2011, 2,378 women participated in 104 1st Tier workshops. Out of these women, 47% (1,129) returned completed message dissemination log sheets with the information of the women who received messages through 2nd Tier message dissemination. According to the logs, 11,591 women received messages through 2nd Tier messages dissemination. A study was conducted in February/ March 2012 to evaluate the reach and effectiveness of 2nd Tier message dissemination. Nearly half (48%) reported receiving a message related to AWSOTM or Hayati Ahla from a neighbor, relative or friend. Of those who received a message:
76% recalled the message regarding the importance of planning for the future; exposed compared with non-exposed respondents were significantly less likely to think that objectives can be achieved without planning.
92% of exposed compared to 74% of non-exposed respondents report positive attitudes about the use of modern contraception as well as the benefits of a small family.
Over 90% of exposed women compared to 59% of non-exposed women indicated that they knew how to conduct a breast self-exam (BSE); 76% of exposed but only 41% of non-exposed respondents reported that they had already conducted a BSE.
The intervention had a “dose effect”: that is, the more messages recalled the greater the number of message-related actions taken, thus attesting to the quality of the message dissemination.
Yet, given the newness of this approach and the fact that less than 50% of the women who had been identified as message recipients by 1st Tier AWSOTM participants actually reported that they had heard an AWSOTM–related message prompted JHCP staff to revisit the training protocol. To that end, JHCP communication between supervisors and trainees was enhanced and promotional materials were given to AWSOTM participants for Phase II of the 2nd tier outreach. The current study was designed to capture the effects of the enhanced approach.
AWSOTM: 2nd Tier, Phase II
During March and April, of 2012, 2156 women participated in 96, 1st Tier workshops. Of these women, 56% (1199) returned completed message dissemination log sheets with contact information for the women with whom they had communicated AWSOTM–related messages. This is referred to as “2nd Tier message dissemination.” Based on the logs, 17,114 women received messages through Phase II of the 2nd Tier message dissemination outreach.
Given that this was a new approach that had been tested only once, the key questions for Phase II were to ascertain (1) if differences between participants and non-participants on key outcomes that
7
were found with Phase I respondents would be confirmed with phase II respondents and (2) to gain a better sense through this second study of what proportion of trainees (1st Tier participants) could be expected to disseminate messages to family and friends.
Methodology
The findings reported herein rely on a post-test only sample design. A sample was generated using the data collected in 2nd Tier message dissemination logs; 86% of the 17,114 logged names included telephone numbers. A probabilistic sample was generated whereby the distribution of message recipients was proportionate to the distribution by district. The sample was generated from those with listed telephone numbers (86% of the 17,114). Potential respondents were contacted and interviewed by telephone from May 13 to May 19, 2012. Interviews were successfully completed with 408 women. None of the women reached by phone refused to participate.
Questionnaire
The interviewer-administered questionnaire included questions about the eight key messages. The questionnaire also included questions about knowledge, attitudes and actions related to the key messages. Questions also allowed for self-reported benefits from being exposed to the messages along with self-reported use of received referral cards.
Data collection, entry, and analyses
Accurate Opinion for Public Opinion Measurements, Co. completed data collection and entry. The data set was entered, cleaned and edited for inconsistencies using CSPro 4.0. Missing data were not statistically imputed. Data analysis was completed using STATA version 11 statistical software.
Findings
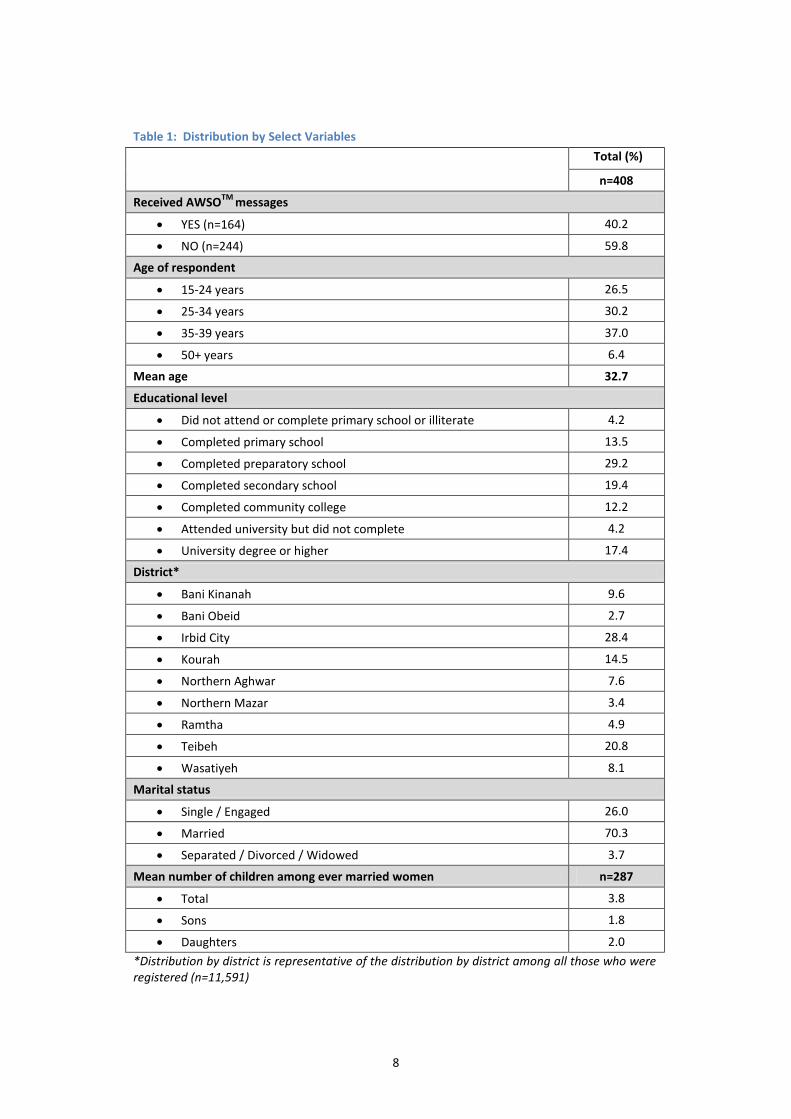
Sample Characteristics As shown in Table 1, most of the women were of reproductive age, with only 6% aged 50 or older. There was a good distribution of educational attainment: 18% had not gone beyond primary school and 17% had completed a university degree or greater. Seven out of ten were married with an average of 3.8 children. There were no differences in age, educational attainment or marital status between those exposed to AWSOTM messages and those not exposed (data not shown).
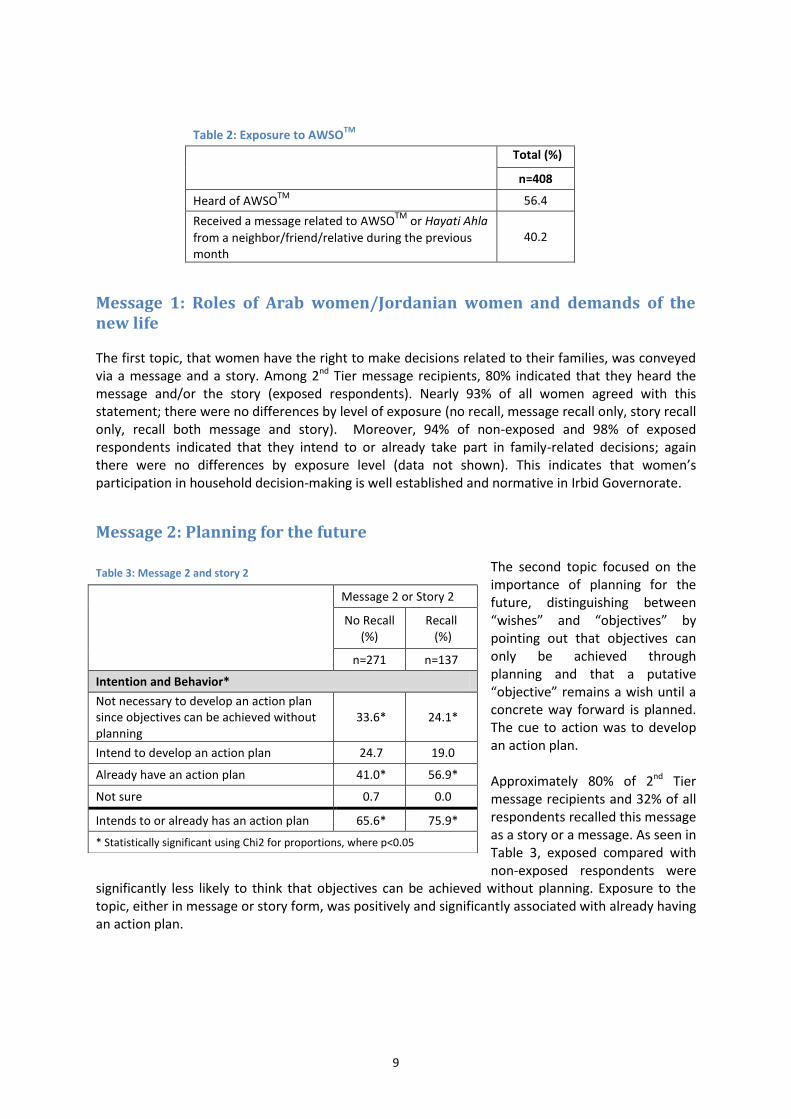
Exposure to AWSOTM Nearly 56% of respondents had heard of AWSOTM and 40% reported receiving a message related to AWSOTM or Hayati Ahla from a neighbor, relative or friend (hereafter, 2nd Tier message recipients) during the previous month as shown in Table 2. It could be that some message recipients did not specifically associate the messages to AWSOTM or Hayati Ahla. Even if the estimated reach is 40% of the 17, 114 women whose names were in the logs, an additional 6,800 women were reached through the 2nd Tier approach with minimal costs.
8
Table 1: Distribution by Select Variables
Total (%)
n=408
Received AWSOTM
messages
YES (n=164) 40.2
NO (n=244) 59.8
Age of respondent
15-24 years 26.5
25-34 years 30.2
35-39 years 37.0
50+ years 6.4
Mean age 32.7
Educational level
Did not attend or complete primary school or illiterate 4.2
Completed primary school 13.5
Completed preparatory school 29.2
Completed secondary school 19.4
Completed community college 12.2
Attended university but did not complete 4.2
University degree or higher 17.4
District*
Bani Kinanah 9.6
Bani Obeid 2.7
Irbid City 28.4
Kourah 14.5
Northern Aghwar 7.6
Northern Mazar 3.4
Ramtha 4.9
Teibeh 20.8
Wasatiyeh 8.1
Marital status
Single / Engaged 26.0
Married 70.3
Separated / Divorced / Widowed 3.7
Mean number of children among ever married women n=287
Total 3.8
Sons 1.8
Daughters 2.0
*Distribution by district is representative of the distribution by district among all those who were registered (n=11,591)
9
Table 2: Exposure to AWSO
TM
Total (%)
n=408
Heard of AWSOTM
56.4
Received a message related to AWSOTM
or Hayati Ahla
from a neighbor/friend/relative during the previous month
40.2
Message 1: Roles of Arab women/Jordanian women and demands of the new life
The first topic, that women have the right to make decisions related to their families, was conveyed via a message and a story. Among 2nd Tier message recipients, 80% indicated that they heard the message and/or the story (exposed respondents). Nearly 93% of all women agreed with this statement; there were no differences by level of exposure (no recall, message recall only, story recall only, recall both message and story). Moreover, 94% of non-exposed and 98% of exposed respondents indicated that they intend to or already take part in family-related decisions; again there were no differences by exposure level (data not shown). This indicates that women’s participation in household decision-making is well established and normative in Irbid Governorate.
Message 2: Planning for the future
The second topic focused on the importance of planning for the future, distinguishing between “wishes” and “objectives” by pointing out that objectives can only be achieved through planning and that a putative “objective” remains a wish until a concrete way forward is planned. The cue to action was to develop an action plan. Approximately 80% of 2nd Tier message recipients and 32% of all respondents recalled this message as a story or a message. As seen in Table 3, exposed compared with non-exposed respondents were
significantly less likely to think that objectives can be achieved without planning. Exposure to the topic, either in message or story form, was positively and significantly associated with already having an action plan.
Table 3: Message 2 and story 2
Message 2 or Story 2
No Recall (%)
Recall (%)
n=271 n=137
Intention and Behavior*
Not necessary to develop an action plan since objectives can be achieved without planning
33.6* 24.1*
Intend to develop an action plan 24.7 19.0
Already have an action plan 41.0* 56.9*
Not sure 0.7 0.0
Intends to or already has an action plan 65.6* 75.9*
* Statistically significant using Chi2 for proportions, where p<0.05
10
Message 3: Participation of men and women in planning their family and securing its health
The third subject AWSOTM trainees were asked to discuss was related to the importance of delaying marriage until the age of 18 or later for women and the age of 22 or later for men as the basis for a happy, healthy and stable married life. The cue to action was to discourage the young people in their lives from early marriage. Nearly 91% of 2nd Tier message recipients and 37% of all respondents recalled hearing about this subject via a message and/or a story. There were no differences in knowledge, attitudes, intentions or self-reported actions in this regard as 85% of all recipients disagree that “early marriage is a good basis for a happy and stable life.” Indeed, over 90% of all participants reported that they intend to discourage or have already discouraged their daughters or nieces from marrying before the age of 18 and their sons or nephews before the age of 22. Again, this appears to be a well-establish social norm in Irbid Governorate.
Message 4: Family planning and the benefits of small families
Fully 91% of 2nd Tier message recipients (36% of all respondents) recalled hearing about the benefits of family planning and of small families. About 93% of message recipients and 88% of non-exposed reported positive attitudes regarding the use of modern contraception; similar percentages agreed with the benefits of a small family (differences not significant; data not shown). While 40% of message recipients compared with 35% of non-exposed respondents are current users of modern contraception, this difference did not reach significance. About 40% of the women who heard the message indicated that it gave them new information about the utilization of modern FP methods (data not shown).
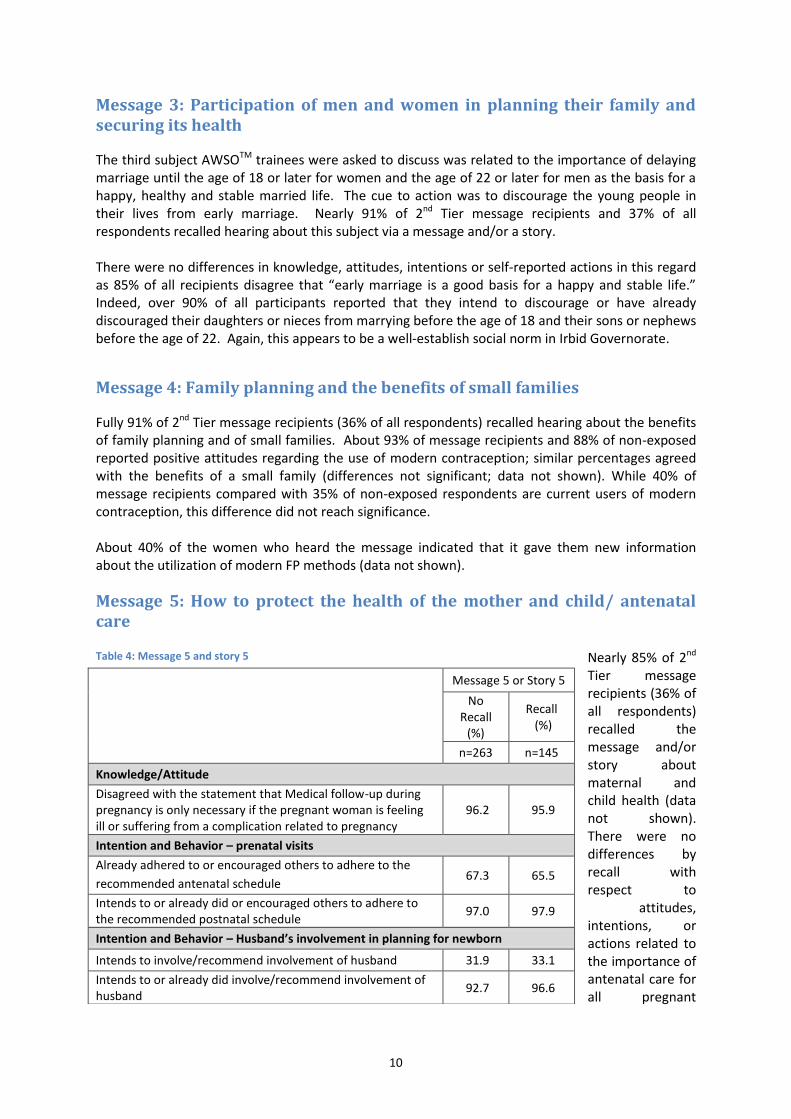
Message 5: How to protect the health of the mother and child/ antenatal care
Nearly 85% of 2nd Tier message recipients (36% of all respondents) recalled the message and/or story about maternal and child health (data not shown). There were no differences by recall with respect to
attitudes, intentions, or actions related to the importance of antenatal care for all pregnant
Table 4: Message 5 and story 5
Message 5 or Story 5
No Recall
(%)
Recall (%)
n=263 n=145
Knowledge/Attitude
Disagreed with the statement that Medical follow-up during pregnancy is only necessary if the pregnant woman is feeling ill or suffering from a complication related to pregnancy
96.2 95.9
Intention and Behavior – prenatal visits
Already adhered to or encouraged others to adhere to the
recommended antenatal schedule 67.3 65.5
Intends to or already did or encouraged others to adhere to the recommended postnatal schedule
97.0 97.9
Intention and Behavior – Husband’s involvement in planning for newborn
Intends to involve/recommend involvement of husband 31.9 33.1
Intends to or already did involve/recommend involvement of husband
92.7 96.6
11
women regardless of how they feel or whether they have experienced complications, encouraging others to adhere to the recommended antenatal schedule, or involving husbands in planning for the newborn. As shown in Table 4, agreement, intentions and actions are already high – they are at or approach 100% when combining intentions with current actions.
Message 6: How to protect the health of the mother and child/ postpartum follow-up and immunizations
Again, message recall was very high with 92% of 2nd Tier message recipients (37% of all respondents) reporting exposure to the message and/or story about how to protect the health of the mother and child. There were no significant differences by level of exposure. Over 90% of all respondents disagreed with the statement that “a woman should only seek postpartum services if she experiences complications.” Over 95% reported that they had already complied or encouraged others to comply with the recommended schedule for postpartum follow-up and immunizations. The rest of the women, with but a few exceptions, indicated that they intend to comply or encourage others to ask the provider about MCH services (data not shown).
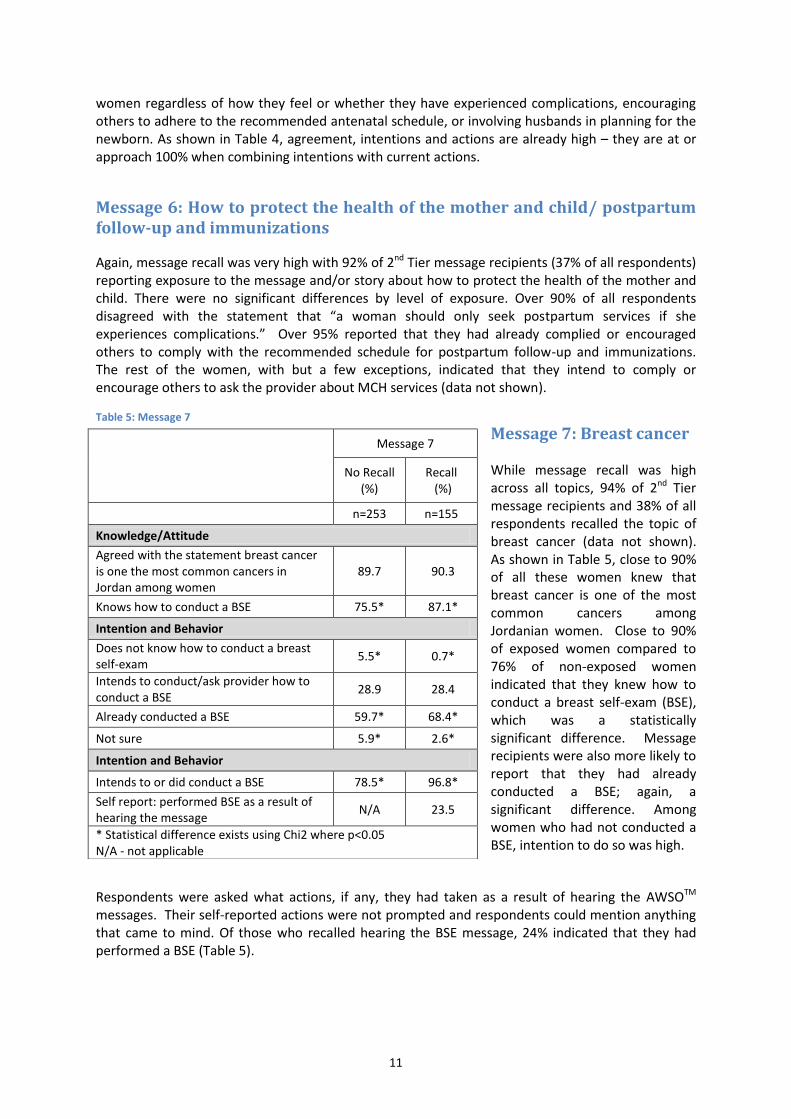
Message 7: Breast cancer While message recall was high across all topics, 94% of 2nd Tier message recipients and 38% of all respondents recalled the topic of breast cancer (data not shown). As shown in Table 5, close to 90% of all these women knew that breast cancer is one of the most common cancers among Jordanian women. Close to 90% of exposed women compared to 76% of non-exposed women indicated that they knew how to conduct a breast self-exam (BSE), which was a statistically significant difference. Message recipients were also more likely to report that they had already conducted a BSE; again, a significant difference. Among women who had not conducted a BSE, intention to do so was high.
Respondents were asked what actions, if any, they had taken as a result of hearing the AWSOTM messages. Their self-reported actions were not prompted and respondents could mention anything that came to mind. Of those who recalled hearing the BSE message, 24% indicated that they had performed a BSE (Table 5).
Table 5: Message 7
Message 7
No Recall (%)
Recall (%)
n=253 n=155
Knowledge/Attitude
Agreed with the statement breast cancer is one the most common cancers in Jordan among women
89.7 90.3
Knows how to conduct a BSE 75.5* 87.1*
Intention and Behavior
Does not know how to conduct a breast self-exam
5.5* 0.7*
Intends to conduct/ask provider how to conduct a BSE
28.9 28.4
Already conducted a BSE 59.7* 68.4*
Not sure 5.9* 2.6*
Intention and Behavior
Intends to or did conduct a BSE 78.5* 96.8*
Self report: performed BSE as a result of hearing the message
N/A 23.5
* Statistical difference exists using Chi2 where p<0.05 N/A - not applicable
12
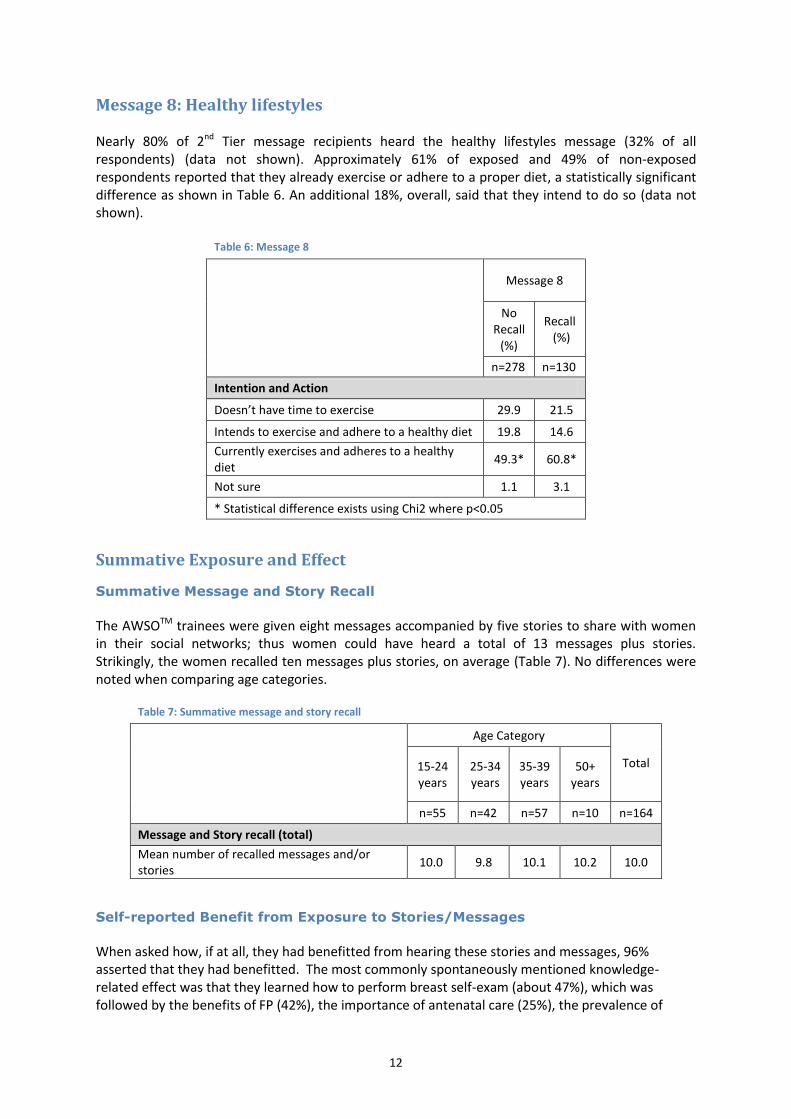
Message 8: Healthy lifestyles Nearly 80% of 2nd Tier message recipients heard the healthy lifestyles message (32% of all respondents) (data not shown). Approximately 61% of exposed and 49% of non-exposed respondents reported that they already exercise or adhere to a proper diet, a statistically significant difference as shown in Table 6. An additional 18%, overall, said that they intend to do so (data not shown).
Table 6: Message 8
Message 8
No Recall
(%)
Recall (%)
n=278 n=130
Intention and Action
Doesn’t have time to exercise 29.9 21.5
Intends to exercise and adhere to a healthy diet 19.8 14.6
Currently exercises and adheres to a healthy diet
49.3* 60.8*
Not sure 1.1 3.1
* Statistical difference exists using Chi2 where p<0.05
Summative Exposure and Effect
Summative Message and Story Recall
The AWSOTM trainees were given eight messages accompanied by five stories to share with women in their social networks; thus women could have heard a total of 13 messages plus stories. Strikingly, the women recalled ten messages plus stories, on average (Table 7). No differences were noted when comparing age categories.
Table 7: Summative message and story recall
Age Category
Total 15-24 years
25-34 years
35-39 years
50+ years
n=55 n=42 n=57 n=10 n=164
Message and Story recall (total)
Mean number of recalled messages and/or stories
10.0 9.8 10.1 10.2 10.0
Self-reported Benefit from Exposure to Stories/Messages
When asked how, if at all, they had benefitted from hearing these stories and messages, 96% asserted that they had benefitted. The most commonly spontaneously mentioned knowledge-related effect was that they learned how to perform breast self-exam (about 47%), which was followed by the benefits of FP (42%), the importance of antenatal care (25%), the prevalence of
13
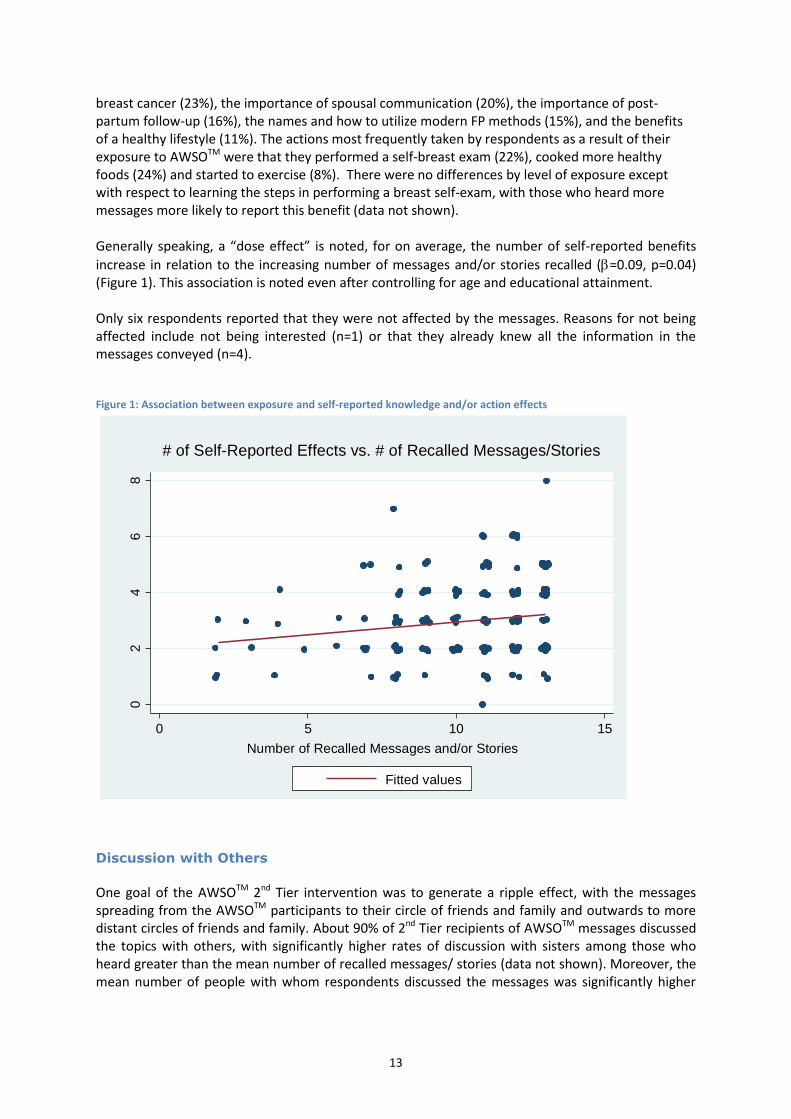
breast cancer (23%), the importance of spousal communication (20%), the importance of post-partum follow-up (16%), the names and how to utilize modern FP methods (15%), and the benefits of a healthy lifestyle (11%). The actions most frequently taken by respondents as a result of their exposure to AWSOTM were that they performed a self-breast exam (22%), cooked more healthy foods (24%) and started to exercise (8%). There were no differences by level of exposure except with respect to learning the steps in performing a breast self-exam, with those who heard more messages more likely to report this benefit (data not shown). Generally speaking, a “dose effect” is noted, for on average, the number of self-reported benefits
increase in relation to the increasing number of messages and/or stories recalled (=0.09, p=0.04) (Figure 1). This association is noted even after controlling for age and educational attainment. Only six respondents reported that they were not affected by the messages. Reasons for not being affected include not being interested (n=1) or that they already knew all the information in the messages conveyed (n=4). Figure 1: Association between exposure and self-reported knowledge and/or action effects
Discussion with Others
One goal of the AWSOTM 2nd Tier intervention was to generate a ripple effect, with the messages spreading from the AWSOTM participants to their circle of friends and family and outwards to more distant circles of friends and family. About 90% of 2nd Tier recipients of AWSOTM messages discussed the topics with others, with significantly higher rates of discussion with sisters among those who heard greater than the mean number of recalled messages/ stories (data not shown). Moreover, the mean number of people with whom respondents discussed the messages was significantly higher
02
46
8
Num
ber
of S
elf-R
epo
rte
d A
ction
and
/or
Kn
ow
ledg
e E
ffects
0 5 10 15
Number of Recalled Messages and/or Stories
Fitted values
# of Self-Reported Effects vs. # of Recalled Messages/Stories

14
among those who recalled more compared with those who heard fewer than the mean number of messages and stories (1.7 v. 1.3, p=0.03).
Reception and Utilization of the Referral Card
Finally, the AWSOTM 1st Tier trainees were asked to give referral cards for the local FP clinic to the women with whom they discussed the messages/stories if appropriate. Nearly 70% of the exposed women indicated that they had received referral cards (Table 8). Of these, 28% indicated that they used the cards. Of those who did not use the cards, 90% intend to use them in the future.
Table 8: Reception and utilization of the referral card
Total (%)
n=164
Received a referral card 69.5
n=114
Used the referral card 28.1
Reasons for not using the card n=82
Did not need it/she was not ill 48.8
Did not have time to go to the health center 37.8
Did not see the point of the card 9.8
Other 3.9
Plans to use the card in the future 90.2
Limitations
Upon further examination, it appears that the research instrument may have resulted in an underestimation of recall. It is worth nothing that the identities and contact information of nearly all of the contacted women who were registered as having received 2nd Tier messages were accurate. This indicates that 1st Tier trainees did not fabricate names or telephone numbers for the purpose of delivering their message dissemination logs in order to receive the promotional materials. In measuring recall, the interviewers asked, “Did you receive a message related to Arab Women Speak OutTM or Hayati Ahla from your neighbor/friend/relative during the previous month?” and they were instructed to mention the name of the 1st Tier trainee if the respondent did was unsure. However, it is possible that the 1st Tier trainee may have discussed messages without using the flashcards, without mentioning AWSOTM and Hayati Ahla or without indicating that they were delivering a message from a training they had received.
Conclusions The 2nd Tier approach to AWSOTM dissemination was designed to expand the reach and impact of the AWSOTM initiative to empower women to make health-related decisions. Initially, the only cost associated with the 2nd Tier outreach was the production of the flashcards and the promotional materials (prayer clothing for women), so the monetary investment was minimal. An assessment of the first phase of 2nd Tier outreach revealed that roughly half of the women who were supposed to have received 2nd Tier messages had any recall of receiving such messages, suggesting that not all the trainees from the 1st Tier disseminated messages according to the programmatic design.

15
Therefore, the second phase of 2nd Tier outreach included some promotional material for women who successfully disseminate messages2. As in the first phase, the 1st Tier trainees were asked to reach out to others on their own time and, to the extent they used their phones to arrange meetings or needed transport to meet with some of their family or friends, with their own resources; however, in the second phase, 1st Tier trainees received promotional materials upon handing in the log containing information about those to whom they disseminated AWSOTM messages. According to the logs turned in by the 1st Tier women during the second phase, some 17,000 were reached. Based on a random sample of the women listed in those logs, 40% actually heard AWSOTM-specific messages from the trainees. Therefore, at first sight, it appears that the inclusion of promotional materials did not positively affect the dissemination of messages, but this must be studied further considering the aforementioned limitations. It is important to highlight that the results from this study reaffirm those found from the evaluation of the first phase of 2nd Tier message dissemination. The results maintain that AWSOTM trainees who did contact other women in their social networks were highly committed as they delivered most of the messages to each woman they approached. Furthermore, there were positive and significant effects with respect to planning for the future, knowledge of and performance of a breast self exam and exercising or adhering to a proper diet. As previously mentioned, the objective of this tiered approach of AWSOTM implementation was the creation of discourse among 2nd Tier recipients and their relations, thus creating a 3rd Tier of message dissemination and resulting in a ripple effect. Such an approach yields exponential growth of message dissemination. As hoped, nearly 90% of 2nd Tier message recipients discussed the messages with others. The number of persons with whom 2nd Tier recipients discussed messages was positively associated with the number of messages received.
Recommendations
This study reiterates the recommendation to amend the content of 2nd Tier messages by reducing the number of messages that may have become normative in Irbid society or by depicting these messages as normative in future programming. The findings also reaffirm the support to continue this approach in that it increased the reach of AWSOTM messages, particularly since a “dose effect” was noted once again. It is recommended that formative research be conducted to amend the messages disseminated through the 2nd Tier of AWSOTM in order to apply this successful approach to the promotion of positive attitudes and actions that are not already normative in Jordanian society or other settings. The findings from this study indicate that it might not be cost-effective to utilize promotional materials for augmentation of 2nd Tier message dissemination. However, given the limitations of this study, it is recommended to explore this issue further. Regardless, it is important to strengthen the link between message dissemination at the 2nd Tier and AWSOTM such that all women who receive messages recognize that they come from AWSOTM . Finally, it is important to keep in mind that this method of message dissemination is a work in progress. Any institution that wishes to implement AWSOTM 2nd Tier message dissemination should conduct its own monitoring and evaluation in order to reach its set goals. JHCP has implemented
2 See “Evaluation of the Arab Women Speak Out
TM (AWSO
TM) Initiative - 2nd Tier (Phase I) - in Irbid Governorate, Jordan,
2011”

16
two phases of 2nd Tier AWSOTM message dissemination. Both phases were implemented in conjunction with monitoring and summative evaluation. Lessons learned from both phases indicated that the ripple effect of message dissemination works. It may be, however, that with more intensive monitoring, a larger proportion of the targeted audience will be reached. Or, it may be that it is unrealistic to expect more than 40-50% of program participants to carry out volunteer activities, which is what 1st Tier participants did when they talked with their family and friends about the AWSOTM messages. Indeed, this level of volunteering is very high as the literature indicates a 10% participation rate in volunteer activities is typical. Further research can help establish realistic expectations for future programming.