Jonathan Feddock, MD Department of Radiation Medicine University of Kentucky.
15
INCORPORATING CESIUM-131 INTERSTITIAL IMPLANTS INTO DAILY CLINICAL PRACTICE: HOW TO MAKE RADIATION APPEAR EXACTLY WHERE YOU WANT. Jonathan Feddock, MD Department of Radiation Medicine University of Kentucky
-
Upload
irma-lucas -
Category
Documents
-
view
219 -
download
0
Transcript of Jonathan Feddock, MD Department of Radiation Medicine University of Kentucky.

INCORPORATING CESIUM-131 INTERSTITIAL IMPLANTS INTO DAILY CLINICAL PRACTICE: HOW TO MAKE RADIATION APPEAR EXACTLY WHERE YOU WANT.
Jonathan Feddock, MDDepartment of Radiation MedicineUniversity of Kentucky

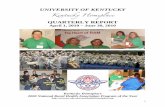
Vaginal cuff recurrence of cervix cancer s/p rad
hysterectomy and adjuvant RT

Okazawa et al. J Rad Res, Open Access, October 15, 2012.

Basic Facts
Radiation Therapy has a well-established role in the curative management of many gynecologic cancers.
Local recurrences following initial treatment including RT are problematic. Options are felt to include radical surgery in very selected patients or palliative care.
Exenterative surgery will be aborted in 25-35% of patients in whom it is attempted. When performed serious acute morbidity, some mortality, and uniform loss of structure and function result.

Basic FactsRe-irradiation is often not considered, in spite of data suggesting its curative potential in well-selected patients. Reasons for not considering re-irradiation include:
Concerns about radiation injury.Patient eligibility for phase I-II trials.Familiarity of the treating physician
If pelvic exenteration is an option (small, central pelvic recurrence), wouldn’t it still be an option if small-volume re-irradiation was either unsuccessful or caused a local complication?

Vaginal cuff recurrence of cervix cancer s/p rad
hysterectomy and adjuvant RT

Orthogonal Radiographs of an Interstitial Au-198 Implant of a Vaginal
Cuff Recurrence

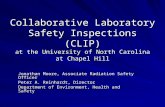
Reconstructed Dose Cloud of 50 Gy

4 days after Au-198 permanent seed implant

8 weeks after Au-198 permanent seed implant (still NED after 10
years)

Interstitial Re-irradiation (IRI)13 pts with recurrent or new primary
gyn cancers underwent IRI between 1986-1990Mean and median age: 63, 70 yrs, respectivelyDiagnosis at time of IRI
Recurrent endometrial ca, n = 6Recurrent cervical ca, n = 4New primary vaginal ca, n = 3
All biopsy-confirmed recurrenceMetastatic work-up negativeRandall ME, Evans L, Greven KM, et al. Interstitial Reirradiation for Recurrent Gynecologic
Malignancies: Results and Analysis of Prognostic Factors. Gyn Oncol (1993) 48: 23-31.

Interstitial Re-irradiation (IRI)
7 permanent seed implants (5 Au-198, 2 Pd-103)6 temporary implants (LDR Ir-192, SNIT)Mean and median implanted volumes: 14.3, 12 cc9/13 (69%) had CR6/14 (46%) NED 24-71 months later Median f/u = 58 monthsOnly 1 possible complication: R-V fistula 22 months following SNIT, in presence of recurrent dz
Randall ME, Evans L, Greven KM, et al. Interstitial Reirradiation for Recurrent Gynecologic Malignancies: Results and Analysis of Prognostic Factors. . Gyn Oncol (1993) 48: 23-31.

IRI Prognostic FactorsCervical and vaginal > endometrialSquamous > adenocarcinomaSmaller tumor volumesHigher RT doses (> 50 Gy)Permanent implants > temporary (SNIT)Vaginal wall/suburethra > vaginal cuffLonger disease-free intervals
Randall ME, Evans L, Greven KM, et al. Interstitial Reirradiation for Recurrent Gynecologic Malignancies: Results and Analysis of Prognostic Factors. Gyn Oncol (1993) 48: 23-31.

RECURRENT DISEASE Advantages for using Surgery
Ability to assess extent of disease and act accordinglyApplicable to larger volume recurrencesAvoids risk of late radiation injury

RECURRENT DISEASEAdvantages for Re-Irradiation
Little peri-operative morbidity or mortalityLittle or no hospitalization required, especially for permanent implantsPreserves structure and function in most patientsMore applicable to patients with medical co-morbidities More acceptable to patientsRelatively inexpensive compared to surgery