Johns Hopkins Health and Education in South Africa.
20
Johns Hopkins Health and Education in South Africa
-
Upload
evan-jonas-knight -
Category
Documents
-
view
215 -
download
0
Transcript of Johns Hopkins Health and Education in South Africa.

Johns Hopkins Health and Education in South Africa

JHHESA: Our Vision
To improve the health and wellbeing of all South Africans through using a strategic communication approach.

JHHESA Our Mission
• Designing and implementing strategic communication programmes.
• Enchancing access to information and the exchange of knowledge.
• Developing programming that is evidence informed through research.
• Providing technical support to South African Partners

JHHESA: Our Approach
INDIVIDUALSOCIAL NETWORKS COMMUNITY SOCIETAL
Behavior and intention; knowledge & skills; beliefs & Values; emotion; perceivedrisk; self-efficacy; self-
image; subjective norms
Partner and family relationships
(communication, trust, understanding, agree-
ment, & power), peerinfluence, gender
equity, bounded normative influence
Leadership; level of participation; information equity;
access to resources;shared ownership;
collective efficacy;social capital; value
for continual improvement
National leadership;per capita income;
income inequality;health policy and
infrastructure;mass media;
religious andcultural values;
gender norms
Physical Environment and InfrastructureBurden of disease; climate and seasonality; transportation and communication networks, access to health care facilities, access to water, sanitation, and household technologies; etc.
Types of CommunicationCommunication for
Participatory Development Dialogue Community MobilisationPeer education
Advocacy To strengthen policy and systems
EngagementMass Media
DialogueCounseling
Peer Education
SOCIAL ECOLOGY MODEL & COMMUNICATION FOR SOCIAL AND BEHAVIORAL CHANGE

The P Process – Developing Evidence Informed Strategies
Key SAG Partners
• SANAC – Men’s Sector – Women’s Sector – Youth Sector – Religious Sector
• Department of Health – National, Provincial and District level.
• South African Broadcasting Corporation • Provincial Departments of Health

Target Audiences
• Primary Audiences: – Youth 15 – 24 – Women of a sexual and reproductive age – Men aged 25+
• Secondary Audiences – Policy and decision makers – Traditional leaders and structures – Government Departments

Objectives: Behavioural Prevention
•Increase the age of sexual debut amongst young people•Increase people’s perception of risk to HIV infection in
relation to their behaviours (Alcohol, transactional sex etc) and sexual partnerships and encouraging the development of risk reduction strategies.
•Reduce the number of men who report having multiple and concurrent partners
•Increase correct and consistent condom usage with all partners.

Objectives Biomedical Prevention
• Promote early antenatal booking amongst pregnant women• Increase the knowledge benefits of exclusive breast feeding
for PMTCT • Reduce the number of children born with HIV• Increase the levels of knowledge of the HIV benefits of
Medical Male circumcision • Increase the number of men who are circumcised.

Objectives: C&T and C&S
• Counseling and Testing • Increase the number of people who undergo VCT for HIV
and who receive their test results• Increase the number of people who test for HIV on a
regular basis
• Care and Support • Increase awareness of the linkages between HIV/TB • Increase knowledge and awareness of the signs and
symptoms of TB • Increase awareness of opportunistic infections and the
need for early treatment
Objectives: Treatment and Strategic Information
•Treatment •Increase the number of people who are treatment
literate.

Mass MediaTelevision PSA’s
Radio PSA’sTelevision and Radio Drama
SeriesRadio Drama and
Talk shows Print Media Feature
WEB and Social Networks
Social Mobilization - Community Outreach - Community Dialogues
- Capacity Building in use of tools
Advocacy Activities Media Advocacy using Television ,
Radio and Print Media Promoting uptake of services
Partnerships and ReferralsMass Media
Partnerships – SABC, e.tv
National and Provincial level Partnerships –
DOH, SANACCommunity Formations
CBO’s, FBO’s Aids and GBV Help
lines Community Based services- FAMSA,
SAPS

JHHESA is a Strategic Communication Partnership for Prevention, Care and Support and Treatment
Strategic Partners: 1. SANAC 2. Department of Health3. Provincial Governments 4. JHU-CCP Broadcast Partners 5. ABC Ulwazi (Radio) – Community Radio 6. SABC Education (TV and Radio) 7. E-TV (Television) 8. Mediology (Media Planning) 9. Mindset Health (Public Health Channel) Research Partners 5. Health and Development Africa 6. Centre for AIDS, Development and Research
(CADRE) Media Advocacy Partners 7. Marcus Brewster Publicity (Media Advocacy)8. Health-E (Media Advocacy) Creative Partners 9. Joe Public (Creative Agency) 10. Matchboxology (Creative Agency)
Capacity building Partners 11. Community Media Trust (Siyayinqoba –
Beat It – Training of Community Health Care Workers)
12. Sonke Gender Justice - Training for Men’s Sector on Brothers for Life
13. Wits HIV and the Media Project 14. UKZN – Centre for Cultural and Media
Studies Community Outreach Partners working with youth, women, men , traditional structures 15. Footballers for Life - Working in
Correctional services16. Lesedi Lechabile - Free State,
Lejwelephutswa17. Mothusimpilo, Gauteng – West18. Turntable Trust, KZN, Sisonke19. The Valley Trust (KZN, Ethekwini)

Programme Priorities for FY12
• Strategic Planning with Provinces and Districts for ACSM– 9 Provincial Reports – 7 local response activities
• Adult Men - Brothers for Life – Sexual prevention and Demand creation for HIV prevention
• Women and Girls – Developing a new programme that addresses maternal and child Health
• Youth – focussed on tertiary institutions and in school and out of school populations using entertainment education programmes.
• Building the capacity of community health care workers in support of the governments PHC
• Building capacity of organisations in social mobilisation for prevention, HCT and
Accomplishments• 1st ever national communication
survey • Planning to local needs using
the local level studies and tracking progress at the local level
• Able to expand on initial PEPFAR investment through public/private partnerships
• Supporting MMC partners with materials to support outreach programmes.
• Supporting the SANAC Men’s Sector and the Communications Technical Task Team
• Developed tools and resources that work in supporting community mobilisation.
• Community dialogues – building community cohesion and response to key issues.
• Scrutinize – demonstrated impact on a number of key outcomes – Multiple partners, condom usage and HCT.
• Intersexions – 2nd most popular drama series and over 23 000 people engaging through social media (Facebook).
.
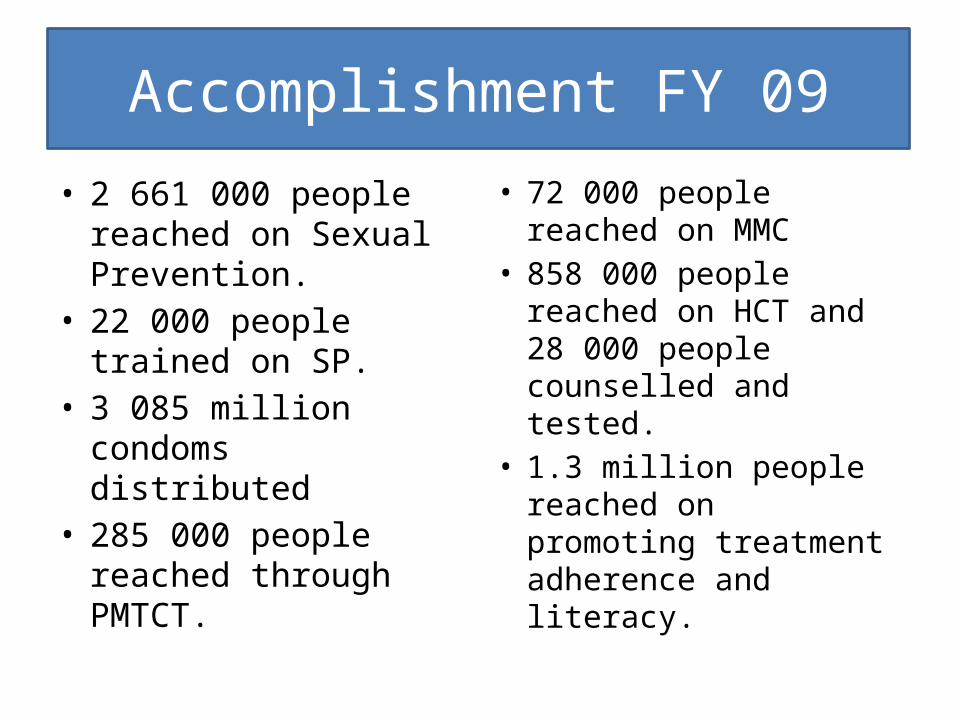
Accomplishment FY 09
• 2 661 000 people reached on Sexual Prevention.
• 22 000 people trained on SP.
• 3 085 million condoms distributed
• 285 000 people reached through PMTCT.
• 72 000 people reached on MMC
• 858 000 people reached on HCT and 28 000 people counselled and tested.
• 1.3 million people reached on promoting treatment adherence and literacy.

How do we know if we are having an impact
• Monitoring system – electronic monitoring system that tracks partner data through monthly reporting
• Monthly and quarterly reporting and Feedback
• Baseline studies undertaken in 2008 will be repeated in 2012
• NCS measures the impact of communication interventions in South Africa includes provincial data.
• Qualitative evaluations – Focus group discuss and individual indepth interviews.
• Evaluating the training programmes what impact is this having?

ENVIRONMENTAL CONTEXT: SUPPORTS & CONSTRAINTSBurden of disease; level of toxic chemicals in air, water, & food; population density; technology; policy; access to food, safe water & sanitation; access to health care, socio-economic conditions
enabling
SKILLS & KNOWLEDGE reinforcement
Attitudes BEHAVIOR
confirmation
IDEATIONAL FACTORSCOGNITIVE Attitudes (Beliefs & Values) Subjective Norms Self-Efficacy Perceived Risk Self-ImageEMOTIONAL Fear, Sadness, Affection, Happy, Trust, Empathy SOCIAL Mutual Understanding Cohesion & Reciprocity Collective Efficacy
COMMUNICATION
INSTRUCTION
DIRECTIVE Dissemination Promotion Prescription
NONDIRECTIVE Entertainment Counseling Dialogue Social Networks
PUBLIC Advocacy Coalition Formation Regulation
HEALTHPHYSICAL & MENTAL STATUSREDUCED MORBIDITY & MORTALITY from INFECTIOUS & CHRONICDISEASES
INDIVIDUAL Intention & Behavior
COLLECTIVE Leadership Participation Goal Setting Action
META-THEORY OF HEALTH COMMUNICATION
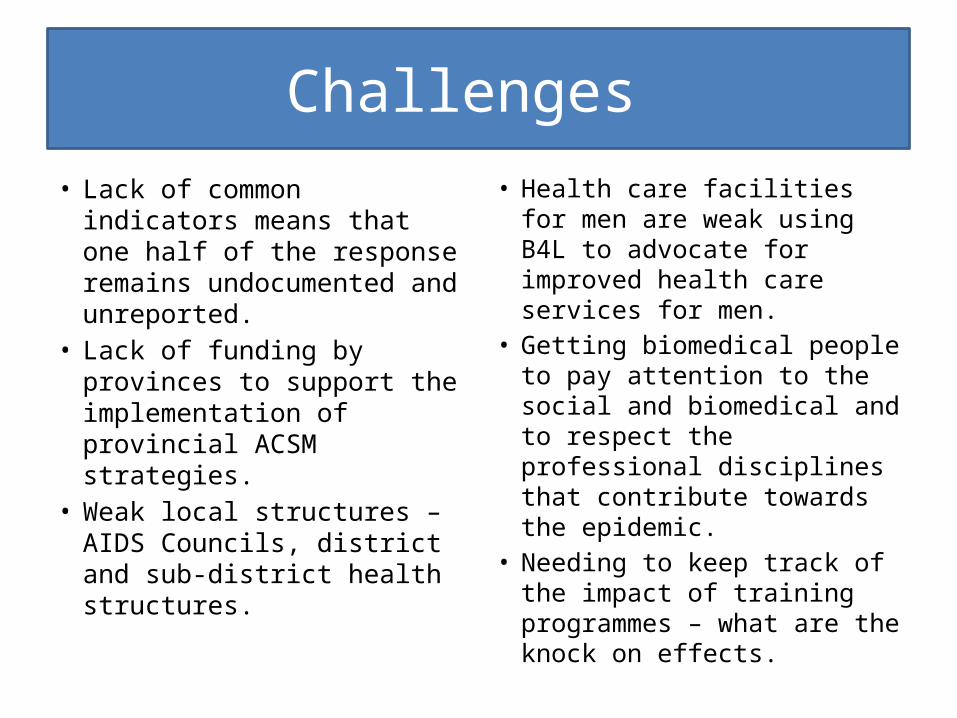
Challenges
• Lack of common indicators means that one half of the response remains undocumented and unreported.
• Lack of funding by provinces to support the implementation of provincial ACSM strategies.
• Weak local structures – AIDS Councils, district and sub-district health structures.
• Health care facilities for men are weak using B4L to advocate for improved health care services for men.
• Getting biomedical people to pay attention to the social and biomedical and to respect the professional disciplines that contribute towards the epidemic.
• Needing to keep track of the impact of training programmes – what are the knock on effects.

Looking beyond USAID/PEPFAR
• Advocating with government to incorporate ACSM into annual planning process – have been some success with ACSM units established but need to be capacitated.
• Encouraging greater linkages between community partners and local and district governments.
• Need to advocate for provinces to budget for ACSM – beyond producing just posters and brochures.
• Looking at additional SAG and other funding sources.







![THE The JOHNS HOPKINS CLUB Events JOHNS HOPKINS … [4].pdf · Club Herald July / August 2015 Events THE The JOHNS HOPKINS CLUB JOHNS HOPKINS UNIVERSITY 3400 North Charles Street,](https://static.fdocuments.in/doc/165x107/5fae1ad08ad8816d2e1aaabe/the-the-johns-hopkins-club-events-johns-hopkins-4pdf-club-herald-july-august.jpg)