Jennifer Hayes, DNP, FNP-BC, CPC, CPCO Manager, Medical ...Coding rules can impact E/M code if not...
44
Jennifer Hayes, DNP, FNP-BC, CPC, CPCO Manager, Medical Coding Healthcare Clinic at Walgreens
Transcript of Jennifer Hayes, DNP, FNP-BC, CPC, CPCO Manager, Medical ...Coding rules can impact E/M code if not...

Jennifer Hayes, DNP, FNP-BC, CPC, CPCOManager, Medical CodingHealthcare Clinic at Walgreens

The presenter has no disclosures or conflict of interest to report.
No off-label prescribing will be discussed.

Review key CMS directives in ICD-10 coding
Identify payer requirements for code submission
Evaluate key strategies for coding success


Additional Coding RulesRequire additional diagnosis codes
Caution with EHR
Payer AnalyticsBetter analysis of diagnosis pairing
Unspecified diagnoses
Stringency versus LeniencyCode families
Specificity

Medicare Fee-for-service Part B Fee Schedule only
Any valid code from correct code family acceptable
www.icd10data.com:
https://www.cms.gov/Medicare/Coding/ICD10/Downloads/ICD-10-guidance.pdf

The medical necessity and appropriateness of the diagnostic and/or therapeutic services provided
Services provided have been accurately reported
If not documented, the rationale for ordering diagnostic and other ancillary services should be easily inferred
The CPT and ICD-10-CM codes reported on the health insurance claim form should be supported by the documentation in the medical record
CMS 1997 DOCUMENTATION GUIDELINES FOR EVALUATION & MANAGEMENT SERVICES

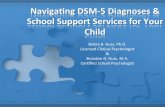
CMS Bell-curve expectations
Family Practice:
https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/MedicareFeeforSvcPartsAB/downloads/EMSpecialty2012.pdf?agree=yes&next=Accept
0
10
20
30
40
50
99201 99202 99203 99204 99205
New Visit %
0
10
20
30
40
50
60
99211 99212 99213 99214 99215
Established Visit %

Coding rules can impact E/M code if not careful
Some diagnoses require 2 codes
Some diagnoses cannot be used together
Better capture of disease severity in diagnosis codes
Combination codes for complications
Coding Tip: Rules Rule!
Being familiar with Excludes1 coding rules
will help avoid mismatch of diagnosis codes


FederalMedicare
StateMedicaid
CommercialPrivate Insurers
Includes Healthcare Marketplace plans
Medicare Advantage

CPT codes
Procedures performed
Additional testing
Screening
(Medicare coverages)
Coding Tip: Less is More!
Know coverages for your payers in order to
perform testing that will support selected treatment plan

Supported by documentation
Provide clinical picture with diagnosis listing
Supports quality of care
Minimizes claim denial

Do not support medical necessity
Many payers rejecting diagnoses containing “unspecified”
Risk Adjustment not correctly captured
Value Based Care Model
Coding Tip: 1-Strike Rule
Avoid diagnosis codes that use the word
“unspecified” more than once in description

Diagnosis that represents the main reason the patient sought medical care
Certain coding rules prevent some diagnoses from being designated as primary
http://medicalnegligence.center/gallery/misdiagnosis-and-medical-negligence/dynamic/misdiagnosis-and-medical-negligence.jpg-nggid0217-ngg0dyn-480x360x100-00f0w010c010r110f110r010t010.jpg

Certain Z-Codes:
BMI
Family history codes
Personal history codes
Z16- (drug resistance)
External Cause Codes
Chapters V00-Y99
Certain Supplemental Codes
(Chapters A00-B99)
http://blog.lionbridge.com/marketing/files/2013/05/Medical.jpg


HTN
Diabetes
Asthma
Etiology
http://media.cmgdigital.com/shared/lt/lt_cache/thumbnail/908/img/photos/2012/05/03/0d/fb/stethoscope_medium.jpg

Provider documentation
Lab and diagnostic test results
Previous medical records
https://pixabay.com/en/medical-record-health-patient-form-781422/

Evidence-based Medically Necessary

HPI
Pertinent positive findings for chief complaint
Individual elements Interval from last follow-up Chronic Condition status PE
Follows EBP guidelines Includes all affected organ
systems from HPI and ROS Examine for all potential
complications
ROS
Inventory of impacted organ systems
Pertinent positive and negative findings
Extension of presenting problem and underlying conditions
https://www.southerncross.co.nz/Portals/0/Group/Health%20Information/SX_Medical_Library_Ad.gif

More Specific
E11.22 Type 2 diabetes mellitus with diabetic chronic kidney disease
N18.2 Chronic kidney disease, stage 2
Z79.4 Long term (current) use of insulin
J45.30 Mild persistent asthma, uncomplicated
Less Specific
E11.9 Type 2 diabetes mellitus without complications
J45.909 Unspecified asthma, uncomplicated

“Site not specified”
Unknown organism
Descriptor for code
UNSPECIFIED
UNSPECIFIED

EBP supports consistencyMeets standard of care requirements
Quality of care provided is consistent
Be cautious of cloningNo 2 patients will present exactly the same way for the same condition

Under-documenting per EBP will result in under-coding
Over-documenting outside of EBP will result in over-coding not supported by medical necessity
Appropriate history is building block for remainder of visit
Not just coding, but also quality of care


Patient presents for checkup with PCP. Has diabetes and HTN and has not been seen in almost 2 years. Has intermittently taken meds if had refills remaining. Recently quit smoking since retiring from work 4 months ago and wants to get back on track with health to enjoy being active in retirement.

CC: Annual check-up
HPI: Patient with uncontrolled hypertension and uncontrolled Type II diabetes. Recently on Medicare due to retirement and wishing to get control of chronic conditions. Had been treated in the past with insulin for diabetes but has only been sporadically taking Metformin and has not used insulin in over a year. A1C 2 years ago was 9.4
PMH: Diabetes, hypertension
FMH: Thyroid cancer – mother; Diabetes – mother; COPD -
sister
Social history: Quit smoking 7 months ago

Constitutional: Denies significant changes in weight
Eyes: No change in vision other than cataracts
Respiratory: Denies cough or SOB
CV: Denies chest pain, palpitations; denies swelling in feet
Neuro: Reports has had some increased foot pain bilaterally; denies any headache; denies any weakness
GU: Reports more frequent urination over past 6 months, waking up more at night
GI: Denies any change in appetite; denies abdominal pain
M/S: Denies any M/S issues
Skin: Denies any sores, dry skin or ulcers

Vitals and General Appearance:
Temp: 99.0; Resp: 21; BP 152/88 (Lt. Arm); 158/90 (Rt. Arm) Pulse: 70; Ht. 6’1”; Wt. 260; BMI 34.3
Appears to be in NAD
HEENT:
Eyes: EOM’s intact; funduscopic exam WNL
Mouth/Throat/Dentition: Lips, teeth, gums WNL
Neck: No thyroid enlargement seen; no carotid bruit
Abdomen:
No organomegaly; no abdominal bruit

Respiratory:Lungs clear to auscultation; respirations unlabored
Cardiovascular:Regular heart rate and rhythm, without murmur, no abnormal or extra heart sounds; 2+ pedal edema; pedal pulses WNL
Neuro:Monofilament reveals diminished sensation on foot exam; DTR’s intact
Skin:No ulcers or skin lesions identified; hammer toe on second digit of left foot

Random glucose: 348
EKG: Normal
Urinalysis: + Glucose; + Ketones
Medical Necessity?
https://pixabay.com/en/test-tube-lab-medical-research-214185/

Additional labs
Screening tests
Key Considerations:Plan exclusions?
ABN or not?
https://static.pexels.com/photos/34846/pexels-photo.jpg

E11.21 Type 2 diabetes mellitus with diabetic nephropathy
E11.36 Type 2 diabetes mellitus with diabetic cataract
E11.41 Type 2 diabetes mellitus with diabetic mononeuropathy
E11.621 Type 2 diabetes mellitus with foot ulcer
E11.65 Type 2 diabetes mellitus with hyperglycemia
E11.41 Type 2 diabetes mellitus with diabetic mononeuropathy

E11.21 Type 2 diabetes mellitus with diabetic nephropathy
E11.36 Type 2 diabetes mellitus with diabetic cataract
E11.41 Type 2 diabetes mellitus with diabetic mononeuropathy
E11.621 Type 2 diabetes mellitus with foot ulcer
E11.65 Type 2 diabetes mellitus with hyperglycemia
E11.36 Type 2 diabetes mellitus with diabetic cataract

I11.0 Hypertensive heart disease with heart failure
I11.9 Hypertensive heart disease without heart failure
I15.0 Renovascular hypertension
I10 Essential (primary) hypertension
I15.8 Other secondary hypertension
I10 Essential (primary) hypertension

Z68.34 Body mass index (BMI) 34.0-34.9, adult
E66.01 Morbid (severe) obesity due to excess calories
E66.9 Obesity, unspecified
E66.3 Overweight
E66.9 Obesity, unspecified
Z68.34 Body mass index (BMI) 34.0-34.9, adult

F17.200 Nicotine dependence, unspecified uncomplicated
F17.210 Nicotine dependence, cigarettes, uncomplicated
F17.290 Nicotine dependence, other tobacco product, uncomplicated
Z72.0 Tobacco use
Z87.891 Personal history of nicotine dependenceZ87.891 Personal history of nicotine dependence

New category in ICD-10
Gives payers view of gaps in care
Identification of population health issues
For this patient, category:
T38.3X6- Underdosing of insulin and oral hypoglycemic [antidiabetic] drugs

Diagnosis CodesE11.41 (Diabetes w/mononeuropathy)
E11.36 (Diabetes w/cataract)
I10 (HTN)
E66.9 (Obesity)
Z68.34 (BMI)
Z87.892 (History of nicotine)
T38.3X6A (Underdosing of insulin)
CPT Codes99214
93000 (EKG)
81000 (Urinalysis)
82962 (Glucose)

Labs reveal:
GFR: 88
Hgb A1C: 10.2
How does this change the diagnosis codes?
http://www.freestockphotos.biz/stockphoto/17099

E11.41 Type 2 diabetes mellitus with diabetic mononeuropathy
E11.36 Type 2 diabetes mellitus with diabetic cataract
E11.22 Type 2 diabetes mellitus with diabetic chronic kidney disease
N18.2 Chronic kidney disease, stage 2 (mild)
Z79.4 Long term (current) use of insulin

I13.10 Hypertensive heart and chronic kidney disease without heart failure, with stage 1 through stage 4 chronic kidney disease, or unspecified chronic kidney disease
N18.2 Chronic kidney disease, stage 2 (mild)

https://www.flickr.com/photos/walterpro/21180411445