Jennifer Carlquist PA-C, ER CAQ Community Hospital Of ...
80
Jennifer Carlquist PA-C, ER CAQ Community Hospital Of Monterey Peninsula, Central Coast Cardiology
Transcript of Jennifer Carlquist PA-C, ER CAQ Community Hospital Of ...

Jennifer Carlquist PA-C, ER CAQ
Community Hospital Of Monterey Peninsula, Central Coast Cardiology

CHF Margarita
Cointreau(Spironolactone)
TEQUILA(Furosemide)
Margarita mix(BB)
LIME(ACEI)
Adjust to taste

“I am worried about her 16o systolic”

Objectives
AF treatment strategies
CHF tips and tricks
Common medication side effects
Cocktails the Kill!



They are buying what you are selling.



“Broccoli not beta blockers.”
No stress
Exercise
Meditate
Eat better
Say no

“Free lunch” - Lifestyle wins
As compared with the control diet with a high sodium level, the DASH diet with a low sodium level led to a mean systolic blood pressure that was 7.1 mm Hg lower in participants without hypertension, and 11.5 mm Hg lower in participants with hypertension.
N Engl J Med 1990;322:569-574


Case #1: 65 year old male attorney

Strategy
Stable? Unstable? Acute? Chronic?
Rate vs Rhythm.
1. Diltiazem is the premier drug for rate control
(NO HF)
2. BB
3. Verapamil

More on him….
He received Diltiazem 120 mg and converted.
He was discharged on Multaq and Eliquis
Labs: TSH, CBC, trop all normal
“This Multaq is too expensive. There HAS GOT TO be something else.”

Things to rule out
Post op, coPd, Partying
Infiltrative myxoma
Rheumatic valvular disease
Acute MI
Thyroid
Toxins
Environmental

Get you know your customer
Obese? Sleep apnea
Echo – LAE
Lexiscan – ischemic substrate
Bleeding issues?
HRTF?
Beer

How do you choose a drug?
How symptomatic?
How long to stay in it – perioperative?
Bleeder?
How likely to stroke?
How much are they in it?
WHAT DO THEY WANT TO DO

Simple?

Insert chart about this

“The second time you want to be a zero…”
1 - strong consideration for AC
2 and up- “No brainer”
BUT - 1 from female (< 65 years old without other risk factors) NO AC

Pick your poison
Warfarin – (target 2-3)
Rivaroxaban, Apixiban, Dabigitran, Edoxaban(non-valvular)
ASA

To bleed or not to bleed…
Factor 10 Coumadin
No monitoring
No reversal agents
No medication interactions
No food interactions
Expensive up to $12/day
Needs monitoring
Reversal possible
Medication interactions
Food interactions
Renal insufficiency
Inexpensive
AC

AC Rate RhythmSotolol
Flecainide
Propafenone
Dronedarone
Amiodarone

Calls back: “I read the side effects on amiodarone…”
“What else can I be on?”
Sometimes the choice is between bad and worse

Final answer?
Ablate him!

Omeprazole. The new villain?
Can make Plavix less potent
Can lead to bone loss
Probably not that bad but……lawyers
What ever happened to 14 days?
Caviat: Should be on PPI if on coumadin


“My doctor said to ask you about my labs…”
CR 2.2 - _____________, ________________
TSH 10.1 - ________________
HA1c 7 - ___________

What’s wrong with this patient?
Lisinopril Atorvastatin
CarvedilolFurosemide
Metformin
DM, HTN, CHF, Hyperlipidemia

What is missing? What is the dx?
NTG
LisinoprilFurosemide
Dronededarone
Carvedilol
AC/AF

What’s wrong with this picture?
ApixibanK ASA
Metoprolol
Carvedilol
Forgot to take off ASA!
What are they at risk for?
FurosemideCelecoxib
ASA
Ginko
Apixiban
Too Many Blood Thinners

What labs do they need?
Spironolactone Lisinopril K
Warfarin
Digoxin
Digoxin, INR, BMP

What is wrong here?
NTGAsa
Sildenafil Lisinopril
Carvedilol
Nitrate + Viagra =


What medication should we take him off of?

“I am getting all these bruises”
Ticagrelor, ASA, Atorvastatin, Carvedilol, Fish oil, Ginko

“I ache”
Med list: Simvastatin Clopidogril Metoprolol
CoQ 10, qod, Pitavastatin (Livalo)

“My feet can’t fit in my shoes”
Actos (Pioglitazone), ASA, HCTZ, Losartan
Take away Actos, use ted hose, elevate, make sure not unilateral, look for venous stasis, look for HF, dry weight
“Lipidema”
“Not everything that swells is cardiac”

Don’t make it worse
NSAIDS
Glitazones
Diltiazem
Verapamil
Nifedipine
Sotolol
Dronaderone

What medication should we take him off of?
76.1% with spironolactone vs 67.1% with eplerenone

What is the treatment?

“I have this cough…” ACEI vacation
Prilosec (Omeprazole)
Claritin (Loratadine)
Albuterol

“I’m constipated.”
Verapamil, cholestyramine, Ranexa (Ranolazine)

“I have this rash…”
Put on gloves.
Ok, “What?”
Take away all non essentials

Killer Cocktails

“Low Ball Spritz”
Imdur (Isosorbide)
Lasix (Furosemide)
Clonidine
Verapamil

“Long Island Cutie (QT) “
Terfenadine, astemizole
Class I or III antiarrhythmic agent
Macrolide antibiotic
Grapefruit juice

Kill My Kidneys Blast
ACE inhibitor
Diuretic
NSAID
“Kill Your Kidneys Cocktail”

Insulin
Oral hypoglycemic agent
Beta blocker
“Cops Gonna Think You Drunk” Cocktail

Digoxin
Amiodarone
Quinidine
Verapamil
Propafenone
“Mellow Yellow Cocktail”

Aspirin
Clopidogrel
Warfarin
Ginkgo biloba
Vitamin E
“Bloody Mary”

Digoxin
Beta blocker
(Diltiazem, Verapamil)
Amiodarone
“Slow Your Roll”


Case # 3

The Cardiology “Happy Meal”
BB
ACEI
Statin
ASA/Antiplatelet
“FixIt
All”

The Happy Meal: Not so happy?
“I feel dizzy now”
“I don’t want to be on all these medications”
Phase II Cardiac Rehab

Aspirin Tidbits
25% reduction of MI/death
Drinkers and bleeders watch out
No benefit in primary prevention in women under 65

BBA1
HZTZCCBACEI

Nitrates
Induce coronary vasodilation
Dilate peripheral veins – reduce venous return –decreases o2 demand

Refractory Angina
Ranolazine
Isosorbide
Amlodipine

ASAACEIStatin
Car
ved
ilol
Clopidogrel $
Prasugrel $$
Ticagrelor $$
+If stent
BB
Met
op
rolo
l
Ro
uva
stat
in4
0
Ato
rvas
tati
n 8
0Si
mvi
stat
in
81
Ram
ipri
l
Lisi
no
pri
l

“Where’s the bathroom?”

I have to wear this??

2013 – He was sent for echo
“Presented in 2007 with burning in the throat, began several days prior to MI; had BMS to RCA and LAD for acute anteroseptal MI.
Was on Atorvastatin, Ramipril and metoprolol; not taking any longer. Hasn't been feeling well for the past month, with fatigue dyspnea, effort intolerance, and throat/chest discomfort.”

Final read
Severely reduced LV systolic function with anterior, septal and apical akinesis. Severe hypokinesis in remaining segments. EF is 25-30%.
Moderate LV enlargement with mild LA enlargement.


CHF Treatment Tree
3rd Line
Sacubitril/Valsartan Ivabradine
Second Line
Bidil (Isorsorbide/HCTZ) K sparing
First line
BB ACEI/ARB/Diuretics

ACEI pearls
Lisinopril, Ramipril, Enalapril
Check K, CR and BP within one week of initiation or dosage increase in the elderly, and within one to two weeks of initiation or dose
Reduces mortality and morbity

Beta blocker Bits
Hypotension? Stagger or decrease diuretic dose
TAPER
Use Metoprolol Succinate (Toprol XL, Coreg)
No QT

Break it on Dowwwwnn…
Thiazides-HCTZ
Loop diuretics-Lasix, Bumex, Torsemide
K Sparing- Aldactone
Metalazone 30 min before loop shuts down whole tubule

Diuretic Bits
Loops preferred, but thiazides can be considered for patients with hypertension and mild fluid retention.
Furosemide: initial 20 to 40 mg qd/bid
Bumetanide: initial 0.5 to 1 mg qd/bid, max total daily dose 10 mg
Torsemide: initial 10 to 20 mg qd (gut edema)

Potassium Sparing Diuretics
Players: Spironolactone/Eplerenone (aldosterone antagonist)
“Weak diuretics”Help maintain KRarely used alone and are often combined with thiazide or loop diuretics to offset urinary potassium loss.
ACE inhibitor+loop+/- digoxin= improved CHF

“Entresto”, “Corlanor”

“CHF Alcoholics”
Corlanor
(Ivabradine)Entresto(Sacubitril/Valsartan)

Corlanor (Ivabradine))
HCN blocker in SA node (inhibits cardiac pacemaker current to decrease HR)
Lowers HR lowers CHF admissions
Use when maxed out BB, EF less than 35%
Will decrease HR 10-15
Needs to be in sinus to work
No affect on BP
Why do we care about HR in HF?
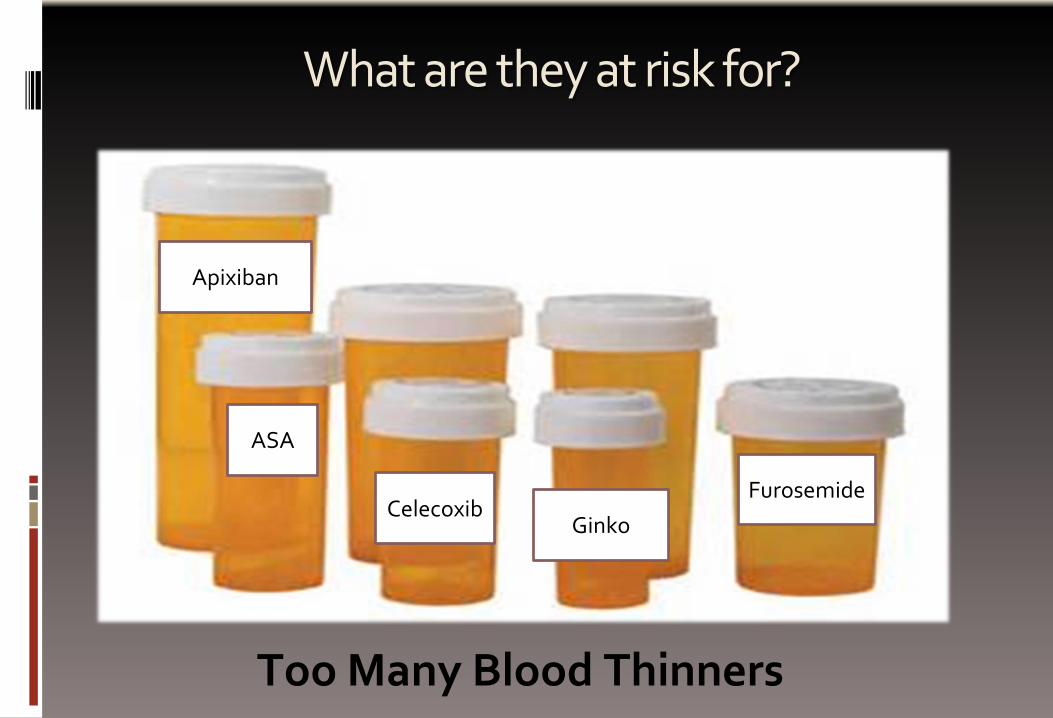
Entresto (Sacubitril/Valsartan)
Class II-IV HF
Breaks down neprilysin decreases BNP degredation -> valsartan antagonizes angiotensin receptors
EF under 40%
Hypotension, hyper K, renal failure, arthralgias can be seen

Jcarlquist.com