Jems201209 dl
76
Always En Route At SEPTEMBER 2012
-
Upload
santiago-clei-wandeson-ferreira -
Category
Health & Medicine
-
view
997 -
download
0
Transcript of Jems201209 dl

Choose 11 at www.jems.com/rs
0912-FP_LFT.indd 1 8/14/2012 1:48:58 PM

Choose 13 at www.jems.com/rs
0912-FP_LFT.indd 1 8/14/2012 1:50:54 PM

JOURNAL OF EMERGENCY MEDICAL SERVICES
TheConscience
of EMS
Contents
Premier media Partner of the iafC, the iafC emS SeCtion & fire-reSCue med www.jems.com SePtemBer 2012 JEMS 5
Departments & columns 7 i Load & go i now on JemS.com 12 i EMS in action i Scene of the month 16 i FroM thE Editor i it’s all about the Pump �By a.J. heightman, mPa, emt-P 18 i LEttErS i in Your Words 22 i Priority traFFic i news You Can use 26 i LEadErShiP SEctor i first day �By Gary Ludwig, mS, emt-P 28 i trickS oF thE tradE i Stealth mode �By thom dick 30 i caSE oF thE Month i Life & Limb �By travis Polk, md, & Carrie Sims, md 32 i rESEarch rEViEW i What Current Studies mean to emS �By david Page, mS, nremt-P 68 i EMPLoyMEnt & cLaSSiFiEd adS 71 i ad indEx 72 i handS on i Product reviews from Street Crews 74 i LaSt Word i the ups & downs of emS
About the CoverCrews from Portland (Ore.) Fire Department and American Medical Response work in a systematic, coordi-nated manner at all resuscitations. The “pit crew” approach is proving to be a significant factor in improved resuscitation and return of spontaneous circulation results. For more, read “Attacking Cardiac Arrest, Part II,” pp. 34–39. Photo Kent PowlowsKi
SEPTEMBER 2012 VOl. 37 NO. 9
i attacking cardiac arrESt Part ii i feedback-driven team performance impacts survival By�Jeffrey�M.�Goodloe,�MD,�NREMT-P,�FACEP;�T.J.�Reginald,�
NREMT-P;�David�S.�Howerton,�NREMT-P;�Jim�O.�Winham,�RN,�BSN,�NREMT-P;�&�Tammy�Appleby,�NREMT-B
34
40 i chEck thE rhythM i expert & safe use of adenosine depends on patient’s cardiac status By�Corey�Slovis,�MD,�FACEP;�Jared�McKinney,�MD;�&�Jeremy�Brywczynski,�
MD,�FAAEM
46 i going oUt on a LiMB i emS provider becomes patient By�Steve�Berry
52 i FroM thE SchooL to thE rig i enhance emS preparation using the field training & evaluation
program model By�Skip�Kirkwood,�MS,�JD,�NREMT-P,�EFO,�CEMSO
54 i Mci MagniFiErS i many factors can complicate an incident of any size By�A.J.�Heightman,�MPA,�EMT-P
58 i SUrViVE & thriVE i Current goals & obstacles in cardiac arrest By�Brandon�Oto
60 i dEadLy dozEn i dealing with the 12 types of thoracic injuries By�Mark�Cipolle,�MD,�PhD;�Michael�Rhodes,�MD;�&�Glen�Tinkoff,�MD
i 40
i 30 i 46
005_TOC.indd 5 8/28/2012 9:17:07 AM

Choose 14 at www.jems.com/rs
0912-FP_LFT.indd 1 8/17/2012 2:52:32 PM

www.jems.com sePTemBeR 2012 JEMS 7
What Makes a Good Instructor?National Association of EMS Educators (NAEMSE) session speaker Keith Widmeier, NREMT-P, CCEMT-P, BA, identifies four things that make a good educator. Do you agree?s connect.jems.com/forum/topics/what-makes-a-good-instructor
Is Gun VIolence a socIal dIsease?Public health experts, in the wake of recent mass shoot-ings, are calling for a fresh look at gun violence as a social disease. What do you think?s www.jems.com/article/news/doctors-consider-gun- violence-social-dis
This summer, EMS providers across the nation have responded to several mass casualty incidents ranging from the July 20 Aurora, Colo., theater shooting that killed 12 and injured more than 60 to the Aug. 13 College Station, Texas school shoot-ing that killed three near the Texas A&M University campus. Our hearts go out to the victims. But equally important is the safety of the providers who respond to these types of poten-tially unsafe scenes. Check out JEMS.com’s major incidents page for resources on how to be prepared to respond to mass casualty incidents, such as active-shooter calls.
Hot dIscussIons
lIke usfacebook.com/jemsfans
folloW us twitter.com/jemsconnect
Get connectedlinkedin.com/groups?about=&gid=113182
eMs neWs alertsjems.com/enews
best bloGGersFireEMSBlogs.com
check It outjems.com/ems-products
JEMS.com offers youoriginal content, jobs,products and resources.But we’re much morethan that; we keepyou in touch withyour colleaguesthrough our:
> Facebook fan page;> JEMS Connect site;> Twitter account;> LinkedIn profile;> Product Connect site; and> Fire EMS Blogs site.
folloW us on
load & Go log in for EXClUSiVE ConTEnT
A BETTEr WAy To LEArn
JEMSCE.CoM onLInE ConTInuIng
EduCATIon ProgrAM
free onlIne learnInG opportunItIes!We believe learning is a lifelong commitment. We also think there’s a lot of knowledge to be had in EMS, and we bet most EMS professionals would agree. That’s why we’ve increased the number of free webcasts we’re offering. Make sure to register for one or all of them today.s jems.com/webcasts
Pho
To B
an
kSPh
oTo
S/iS
ToC
kPh
oTo
.Co
m
Sponsored Product Focusflo2MaX 4-In-1 oXyGen MaskThe FLO2MAX 4-in-1 oxygen mask from BLS Systems Limited was designed to deliv-er the maximal amount of oxygen to the patient. This mask was designed to eliminate room air dilution using a patented series of valves. Able to con-vert to a small-volume nebulizer mask, this mask can function as a true “all in one mask” for EMS services. An integrated filter captures all exhaled bac-teria and excess medication, protecting equipment surfaces and staff from airborne contamination. s Check out their Hot Product listing on JEMS.com!
s jems.com/major-incidents
SHow of Support
s www.facebook.com/questions/10150986687569794/
pollInG our fans Check out which MCIs our Facebook fans felt the most prepared for.
Natural disaster
Major vehicle collision
Terrorist attack
Mass shooting
Unknown illness affecting many
Other
15
73
3
4
3
3
TOTAL votes 101
007_Load.indd 7 8/17/2012 12:06:45 PM

Editor-in-ChiEf I A.J. heightman, MPA, EMt-P I [email protected] Editor I Jennifer Berry I [email protected]
AssoCiAtE Editor I Lauren hardcastle I [email protected] Editor I Allison Moen I [email protected]
AssistAnt Editor I Kindra sclar I [email protected] nEws/BLoG MAnAGEr I Bill Carey I [email protected]
MEdiCAL Editor I Edward t. dickinson, Md, nrEMt-P, fACEP tEChniCAL Editors
travis Kusman, MPh, nrEMt-P; fred w. wurster iii, nrEMt-P, AAsContriButinG Editor I Bryan Bledsoe, do, fACEP, fAAEM
EditoriAL dEPArtMEnt I 800/266-5367 I [email protected]
Art dirECtor I Liliana Estep I [email protected] iLLustrAtors
steve Berry, nrEMt-P; Paul Combs, nrEMt-BContriButinG PhotoGrAPhErs
Vu Banh, Glen Ellman, Craig Jackson, Kevin Link, Courtney McCain, tom Page, rick roach,steve silverman, Michael strauss, Chris swabb
dirECtor of eProduCts/ProduCtion I tim francis I [email protected] CoordinAtor I Matt Leatherman I [email protected]
AdVErtisinG dirECtor I Judi Leidiger I 619/795-9040 I [email protected] ACCount rEPrEsEntAtiVE I Cindi richardson I 661-297-4027 I
[email protected] sALEs CoordinAtor I Elizabeth Zook I [email protected]
sALEs & AdMinistrAtiVE CoordinAtor I Liz Coyle I [email protected] eMEdiA CAMPAiGn MAnAGEr I Lisa Bell I [email protected]
AdVErtisinG dEPArtMEnt I 800/266-5367 I fax 619/699-6722
MArKEtinG dirECtor I debbie Murray I [email protected] MAnAGEr I Melanie dowd I [email protected]
MArKEtinG & ConfErEnCE ProGrAM CoordinAtor I Vanessa horne I [email protected]
dirECtor, AudiEnCE dEVELoPMEnt & sALEs suPPort I Mike shear I [email protected] dEVELoPMEnt CoordinAtor I Marisa Collier I [email protected]
suBsCriPtion dEPArtMEnt I 888/456-5367
rEPrints, ePrints & LiCEnsinG I wright’s Media I 877/652-5295 I [email protected]
eMedia Strategy I 410/872-9303 I MAnAGinG dirECtor I dave J. iannone I [email protected]
dirECtor of eMEdiA sALEs I Paul Andrews I [email protected] dirECtor of eMEdiA ContEnt I Chris hebert I [email protected]
elSevier public SafetyViCE PrEsidEnt/PuBLishEr I Jeff Berend I [email protected]
foundinG Editor I Keith Griffiths
foundinG PuBLishErJames o. Page
(1936–2004)
JOURNAL OF EMERGENCY MEDICAL SERVICES
The Conscience
of EMS
JOURNAL OF EMERGENCY MEDICAL SERVICES
TheConscience
of EMS
JOURNAL OF EMERGENCY MEDICAL SERVICES
The Conscience
of EMS
choose 16 at www.jems.com/rschoose 15 at www.jems.com/rs
008_010_STAFFBOXES.indd 8 8/15/2012 9:26:01 AM

Choose 16 at www.jems.com/rs
0912-FP_RT.indd 1 8/14/2012 1:54:20 PM

JOURNAL OF EMERGENCY MEDICAL SERVICES
The Conscience
of EMS
JOURNAL OF EMERGENCY MEDICAL SERVICES
TheConscience
of EMS
JOURNAL OF EMERGENCY MEDICAL SERVICES
The Conscience
of EMS
EDITORIAL bOARDWILLIAm K. ATKInsOn II, PHD, mPH, mPA, EmT-PPresident & Chief Executive Officer
WakeMed Health & Hospitals
JAmEs J. AugusTInE, mD, FACEPMedical Director, Washington Township (Ohio) Fire Department Associate Medical Director, North Naples (Fla.) Fire DepartmentDirector of Clinical Operations, EMP ManagementClinical Associate Professor, Department of
Emergency Medicine, Wright State University
sTEvE bERRy, nREmT-PParamedic & EMS Cartoonist, Woodland Park, Colo.
bRyAn E. bLEDsOE, DO, FACEP, FAAEmProfessor of Emergency Medicine, Director, EMS Fellowship
University of Nevada School of MedicineMedical Director, MedicWest Ambulance
CRIss bRAInARD, EmT-PDeputy Chief of Operations, San Diego Fire-Rescue
CHAD bROCATO, DHs, REmT-PAssistant Chief of Operations, Deerfield Beach Fire-Rescue Adjunct Professor of Anatomy & Physiology, Kaplan University
J. RObERT (ROb) bROWn JR., EFOFire Chief, Stafford County, Va., Fire and Rescue Department Executive Board, EMS Section,
International Association of Fire Chiefs
CAROL A. CunnIngHAm, mD, FACEP, FAAEmState Medical Director
Ohio Department of Public Safety, Division of EMS
THOm DICK, EmT-PQuality Care Coordinator
Platte Valley Ambulance
CHARLIE EIsELE, bs, nREmT-PFlight Paramedic, State Trooper, EMS Instructor
bRuCE EvAns, mPA, EmT-P Deputy Chief, Upper Pine River Bayfield Fire Protection, Colorado District
JAy FITCH, PHDPresident & Founding Partner, Fitch & Associates
RAy FOWLER, mD, FACEPAssociate Professor, University of Texas Southwestern SOMChief of EMS, University of Texas Southwestern Medical Center Chief of Medical Operations,
Dallas Metropolitan Area BioTel (EMS) System
ADAm D. FOx, DPm, DOAssistant Professor of Surgery,
Division of Trauma Surgery & Critical Care, University of Medicine & Dentistry of New Jersey
Former Advanced EMT-3 (AEMT-3)
gREgORy R. FRAILEy, DO, FACOEP, EmT-PMedical Director, Prehospital Services, Susquehanna HealthTactical Physician, Williamsport Bureau of
Police Special Response Team
JEFFREy m. gOODLOE, mD, FACEP, nREmT-PProfessor & EMS Section Chief
Emergency Medicine, University of Oklahoma School of Community Medicine
Medical Director, EMS System for Metropolitan Oklahoma City & Tulsa
KEITH gRIFFITHsPresident, RedFlash GroupFounding Editor, JEMS
DAvE KEsEg, mD, FACEPMedical Director, Columbus Fire Department Clinical Instructor, Ohio State University
W. Ann mAggIORE, JD, nREmT-PAssociate Attorney, Butt, Thornton & Baehr PCClinical Instructor, University of New Mexico,
School of Medicine
COnnIE J. mATTERA, ms, Rn, EmT-PEMS Administrative Director & EMS System Coordinator,
Northwest (Ill.) Community Hospital
RObIn b. mcFEE, DO, mPH, FACPm, FAACTMedical Director, Threat Science Toxicologist & Professional Education Coordinator,
Long Island Regional Poison Information Center
mARK mEREDITH, mDAssistant Professor, Emergency Medicine and Pediatrics,
Vanderbilt Medical Center Assistant EMS Medical Director for Pediatric Care,
Nashville Fire Department
gEOFFREy T. mILLER, EmT-PDirector of Simulation Eastern Virginia Medical School,
Office of Professional Development
bREnT myERs, mD, mPH, FACEPMedical Director, Wake County EMS SystemEmergency Physician, Wake Emergency Physicians PAMedical Director, WakeMed Health & Hospitals
Emergency Services Institute
mARy m. nEWmAnPresident, Sudden Cardiac Arrest Foundation
JOsEPH P. ORnATO, mD, FACP, FACC, FACEPProfessor & Chairman, Department of Emergency Medicine, Virginia
Commonwealth University Medical CenterOperational Medical Director,
Richmond Ambulance Authority
JERRy OvERTOn, mPAChair, International Academies of Emergency Dispatch
DAvID PAgE, ms, nREmT-PParamedic Instructor, Inver Hills (Minn.) Community CollegeParamedic, Allina Medical TransportationMember of the Board of Advisors,
Prehospital Care Research Forum
PAuL E. PEPE, mD, mPH, mACP, FACEP, FCCmProfessor, Surgery, University of Texas
Southwestern Medical CenterHead, Emergency Services, Parkland Health &
Hospital SystemHead, EMS Medical Direction Team,
Dallas Area Biotel (EMS) System
DAvID E. PERssE, mD, FACEPPhysician Director, City of Houston Emergency Medical Services Public Health Authority, City of Houston Department.
of Health & Human ServicesAssociate Professor, Emergency Medicine,
University of Texas Health Science Center—Houston
JOHn J. PERuggIA JR., bsHus, EFO, EmT-P Assistant Chief, Logistics, FDNY Operations
EDWARD m. RACHT, mDChief Medical Officer, American Medical Response
JEFFREy P. sALOmOnE, mD, FACs, nREmT-PAssociate Professor of Surgery,
Emory University School of MedicineDeputy Chief of Surgery, Grady Memorial HospitalAssistant Medical Director, Grady EMS
KATHLEEn s. sCHRAnK, mDProfessor of Medicine and Chief,
Division of Emergency Medicine, University of Miami School of Medicine
Medical Director, City of Miami Fire RescueMedical Director, Village of Key Biscayne Fire Rescue
JOHn sInCLAIR, EmT-PInternational Director, IAFC EMS SectionFire Chief & Emergency Manager,
Kittitas Valley Fire & Rescue
COREy m. sLOvIs, mD, FACP, FACEP, FAAEmProfessor & Chair, Emergency Medicine,
Vanderbilt University Medical CenterProfessor, Medicine, Vanderbilt University Medical CenterMedical Director, Metro Nashville Fire DepartmentMedical Director, Nashville International Airport
WALT A. sTOy, PHD, EmT-P, CCEmTPProfessor & Director, Emergency Medicine,
University of PittsburghDirector, Office of Education,
Center for Emergency Medicine
RICHARD vAnCE, EmT-PCaptain, Carlsbad Fire Department
JOnATHAn D. WAsHKO, bs-EmsA, nREmT-P, AEmDAssistant Vice President, North Shore-LIJ Center for EMSCo-Chairman, Professional Standards Committee,
American Ambulance AssociationAd-Hoc Finance Committee Member, NEMSAC
KEITH WEsLEy, mD, FACEPMedical Director, HealthEast Medical Transportation
KATHERInE H. WEsT, bsn, mED, CICInfection Control Consultant,
Infection Control/Emerging Concepts Inc.
sTEPHEn R. WIRTH, Esq.Attorney, Page, Wolfberg & Wirth LLC.Legal Commissioner & Chair, Panel of Commissioners,
Commission on Accreditation of Ambulance Services (CAAS)
DOugLAs m. WOLFbERg, Esq.Attorney, Page, Wolfberg & Wirth LLC
WAynE m. ZygOWICZ, bA, EFO, EmT-PEMS Division Chief, Littleton Fire Rescue
10 JEMS SEPTEMBER 2012
008_010_STAFFBOXES.indd 10 8/15/2012 9:25:06 AM

Choose 17 at www.jems.com/rs
0912-FP_RT.indd 1 8/20/2012 4:03:55 PM

>> Photo Rick MccluReEMS IN ACTIONScene of the Month
12 JEMS SEPTEMBER 2012
012_013EMSINACTION.indd 12 8/15/2012 9:26:42 AM

www.jems.com sePTemBeR 2012 JEMS 13
EMS providers from Los Angeles County Fire Department, American Medical Response, Bowers Ambulance Service and MedResponse
Ambulance Inc. work together alongside personnel from the Los Angeles County Sheriff’s Department and California Highway Patrol to triage 17 people involved in a major vehicle pileup on the Antelope Valley (14) Freeway. The freeway traverses a mountainous, remote area in northeastern Los Angeles County. The crash happened on June 26 near the town of Agua Dulce. For more details on how providers man-aged, treated and transported patients in this complex mass casualty event, see “MCI Magnifiers: Many factors can complicate an incident of any size,” pp. 54–57, by A.J. Heightman, MPA, EMT-P.
PrEcarious PileuP
012_013EMSINACTION.indd 13 8/15/2012 11:24:37 AM

0912-FP-Spread_0512pu.indd 14 8/14/2012 2:02:29 PM

Choose 18 at www.jems.com/rs
0912-FP-Spread_0512pu.indd 15 8/14/2012 2:02:41 PM

At a conference I participated in recently, Jason McMullan, MD, asso-ciate medical director for the Cin-
cinnati Fire Department, made a statement during a lecture that I want to pass along because it illustrates the critical importance of consistent, uninterrupted compressions and care delivery to cardiac arrest patients.
He pointed out that if his heart were interrupted in its pumping functions for even a few precious seconds, he would experience an interruption in oxygenated blood flow and pass out.
He also noted that the longer the heart was allowed to be dormant, the longer the risk was for bad things to occur and the more difficult it would become to return the heart to its essential pumping efficiency and sustain life. So resuscitation is really all about the pump: timing, efficiency and consistency.
I think back to my early days as a para-medic and the infrequent cardiac arrest “saves” I had. In almost all my successful resuscitations, someone was performing effective CPR early, a shockable rhythm was present, and I was able to rapidly draw the paddles from my defibrillator and shock the rhythm while it was primed, well oxygenated and “ripe.”
In the wild, wild West days, if a gunfighter delayed in getting his gun into action, his chances of winning the battle were less than 50%. The same is true in cardiac arrest resusci-tation. You can chuckle about me using those old-fashioned paddles to shock v fib, but I bet I can still get my paddles on a patient’s chest faster than you can dig out, unpackage and deploy your pre-packaged defibrillator pads. The point: Technology can sometimes present delays in care delivery if not performed rap-idly and in a consistent, systematic manner.
The September issue of JEMS focuses on cardiac issues, from our regular content to the special 32-page EMS State of the Science edi-torial supplement developed and presented to you and attendees at the bi-annual Emer-
gency Cardiac Care Update (ECCU) Con-ference in Orlando, Fla.—where the latest information on cardiac care and resuscitation will be discussed.
In the supplement, developed in coopera-tion with the U.S. Metropolitan Municipali-ties EMS Medical Directors Consortium and multiple sponsors, we feature a host of key articles, backed up by 150 pieces of research, that demonstrate why delivery of resuscita-tion processes in the field needs to be quickly administered and, most importantly, consis-tently delivered.
In addition to the supplement articles, each of the JEMS articles in this issue presents significant messages that are important for you to read, digest and discuss with your medical director, management team, supervi-sors, training staff and field crews. Each also emphasizes important processes or proce-dures that can increase your efficiency and effectiveness in the field, particularly in the resuscitation of cardiac arrest patients and improvements in return of spontaneous cir-culation (ROSC).
In “Attacking Cardiac Arrest,” pp. 34–39, we focus on a systematic approach to resus-citation in the Tulsa and Oklahoma EMS
systems. In “Check the Rhythm,” pp. 40–45, we discuss the correct and effective use of adenosine, the drug of choice for paroxys-mal supraventricular tachycardia (PSVT) and for differentiating PSVT with aberrancy from v tach in patients with monomorphic wide complex tachycardias.
Like many other potent medications designed for a specific effect on the heart, adenosine, if used inappropriately or for the wrong arrhythmia, can prove fatal.
A thought-provoking question-and-answer session by EMS blogger and writer Brandon Oto, “Survive and Thrive,” pp. 58–59, rounds out the issue by presenting multiple important procedures that we cur-rently deploy in the field, or may deploy in the future.
You’ll read several common elements of cardiac resuscitation in both September JEMS and the editorial supplement. But the real take-home message is that the keys to resus-citation are early initiation of each procedure, limited interruption of compressions and a pre-planned, systematic approach to every-thing you do on these critical cardiac resus-citation calls. And remember, success is all about the effective use of the pump. JEMS
from the editorputting issues into perspective
>> by A.J. HeigHtMAn, MpA, eMt-p
16 JEMS SEPTEMBER 2012
It’s All About the PumPMaintaining the basics is key to effective cardiac resuscitation
pHo
to A
.J. H
eig
HtM
An
As with any task, a continuous supply of a fluid and the initial priming of the pump is key to success.
016_EDITOR.indd 16 8/17/2012 12:09:42 PM

Choose 19 at www.jems.com/rs
0912-FP_RT.indd 1 8/14/2012 2:05:35 PM

LETTERSin your words
18 JEMS SEPTEMBER 2012
I work in a dynamic system. Our response times would be faster, no doubt about it, but only if you have the correct number of units available to respond. Without a high level of responders, response times that should take less than six minutes end up taking 20 minutes.
Also consider the half-life of your employees. Sitting for 12 hours a day, four days a week in a cramped ambu-lance isn’t healthy. I’ve seen EMS providers as young as 25 taking blood thinners. Obesity is becoming a real issue, as well as the ability to pack healthy and efficient meals for lunch and dinner, which doesn’t help the dynamic systems cause.
In my opinion, dynamic systems increase response times by one or two minutes at most. And that system only works if the provider is staffed correctly. On the other hand, stations increase the time an employee can serve his or her community. The question is: Which is more important?
Nathan BrooksVia jems.com
I believe that the trend is to cross-train and diver-sify. I’m a strong supporter of combo units (a mini pumper of sorts) staffed with two firefighters, a police officer and a paramedic personnel. When this has been tried, it has been very successful, but only when the system is designed from scratch. Politics and empires will control change in the tradi-tional departments.
This will allow more units to be used and be capable of multitasking. It will end aerial ladder trucks respond-ing to sick patient calls. It will deliver 250 gallons of water with a reel line that can handle most fires if they’re attacked quickly enough. And it will reduce the stagnant periods that so many paramedics normally experience. This means more pay for more skills, more units for quicker response times and more efficient use of resources.
Tom RichardsVia Jems.com
I was so excited to see the front cover of the July issue of JEMS. I couldn’t wait to read the article. But I was disappointed to see it was more of an opinion piece that didn’t tell us anything new.
As far as response times go, they’re never fast enough. From the information I have, the main response time is initiating CPR within four minutes of arrest. Nobody has enough money or the technology to accomplish this through EMS alone. This is up to the bystander who calls in. As far as dynamic vs. static deployment goes, how many people reach the retire-ment age of 60 with 25–30 years running eight to 12 calls a day in a 12-hour period?
If a patient can be transported to a hospital within the same amount of time it takes to do the paperwork required for a refusal, obtain the two required blood pressures, call their doctor or go through an on-call nurse to set up the appropriate treatment plan, the private ambulance service will choose the transport. Even the public EMS will choose this because it’s quicker to get
the unit out to handle the call volume of a dynamic system. You start taking more than an hour on a call and you don’t transport the patient, and you need more ambulances on the street to make response times, which costs more money. Will communities really invest in their call-takers and call reporting systems?
The catch is that if you don’t dispatch an ambu-lance right away and the call goes from a low-level to a high-level response, then you get dinged for not making the high-level response time because of the time it takes to go through the entire set of ques-tions. If it takes four to six minutes to go through the whole questionnaire, then the ambulance is almost to the scene by the time the call-taker is finished (at least in the cities). You might as well keep sending ambulances.
Bob Farley, EMT-P
Author Jonathan D. Washko, BS-EMSA, NREMT-P, EMD, responds: Sorry for your disappointment. Unfortunately, I’m only given so many words and so much space to express concepts and ideas that quite honestly could fill volumes.
You’re correct in your observation related to the initiation of CPR and the timeliness associated with starting effective chest compressions and survival. You are also correct that few can afford to provide a four-minute response time standard with first response or transport assets.
You may note in my article I discussed the initiation of CPR by a variety of methods, the first being dispatch life-support (DLS). DLS is pre-arrival instructions given by trained emergency medical dispatchers following clinical algorithms that provide lay callers the instruc-tions necessary to get care initiated before EMS arrives. In many communities that embrace this type of system,
‘NEw’ METhodS?The article featured on the July JEMS cover, “Rethinking Delivery Models: EMS Industry May Shift Delivery Methods,” by Jonathan D. Washko, BS-EMSA, NREMT-P, EMD, gar-nered a great deal of interest from readers. What is ‘the new normal’ of EMS, and how do you embrace it? Also, a JEMS Connect discus-sion thread about the use of lights and siren at night generated a conversation among Facebook fans regarding this hot topic. Do they do more damage than help?
illu
stra
tio
n s
tev
e be
rry
Hi Guys. No ambulance needed.I’m a paramedic and have cleared
my C-spine already.
018_020LETTERS.indd 18 8/17/2012 12:13:09 PM

Watch Steve Berry and JEMS Editor-in-Chief AJ Heightman tell you why this book is a must-read!
SteveBerryBook_fp_05-12.indd 1 8/15/2012 4:20:03 PM

20 JEMS SEPTEMBER 2012
pre-arrival instructions save countless lives through the immediate (within a minute or so of 9-1-1 activation) initi-ation of lifesaving treatments. My point is that response times do count in survival and many EMS systems that have improved response times (although they may not have published their findings) have also seen correlated improvements in cardiac arrest return of spontaneous circulation (ROSC) rates.
The mechanism by which the response time improves may vary, for example, the use of dispatch life support or system status management or just adding more resources into the EMS system or a combination of these in order to yield improved clinical results. The point is that systems attempting to achieve this with traditional deployment methodologies are financially unsustainable for a variety of reasons.
To your next concern regarding human sustainability, I agree. Workloads must be balanced in order to provide not just long-term financial stability but also the stability of our teams. Unfortunately, dynamic deployment (like any other tool) can be used for good or bad. It’s how the tool was used that matters. I know many individuals in balanced high-performance EMS systems that have worked their entire careers in the field and love the work they do.
To your third point, regarding whether private entities will embrace the concepts associated with healthcare reform, my answer is that they’ll have no other choice. As I mentioned in the article, once the economic conditions change and population-based pay-ments replace fee-for-service payment methodologies, a shift in how we have to deliver care will take place driven by market force innovation and the dollars avail-able to provide care. As this shift occurs, our mission in EMS will also shift toward keeping patients out of the emergency department and placing them in the proper locus of care.
Next, you’re correct in your concerns related to
the legal risks associated with triage and care referral systems versus treating and transporting everyone. It is evident that the U.S. healthcare system practices risk avoidance in pretty much everything it does; however, if we’re to overcome these obstacles, we must shift from risk avoidance to risk tolerance, and the government will have to help us accomplish this through reform or some other mechanism.
Finally, your point about performance-based con-tracting is spot on. Regulators will have to also evolve and create penalty and reward systems designed around new goals and objectives. We may also see a shift in the regulators moving from government-based ones toward payer-based or provider-based governance models as their bottom lines.
Lastly, this little known excerpt from Jack L. Stout addresses many of my critics and is one of the impetuses that drives me to do what I do every day:
“As EMS providers, we invite the public to literally trust us with their lives. We advise the public that, during a medical emergency, they should rely upon our organization, and not any other. We even suggest that it is safer to count on us than the resources of one’s own family and friends. We had better be right. Regardless of actual performance, EMS organizations do not differ significantly in their claimed goals and values. Public and private, nearly all claim dedication to patient care. Efficient or not, most claim an intent to give the commu-nity its money’s worth. And whether the money comes from user fees or local tax sources, the claim is the same.
Our moral obligation to pursue clinical and response time improvement is widely accepted. But our related obligation to pursue economic efficiency is poorly understood. Many believe these are separate issues. They are not. Economic efficiency is nothing more than the ability to convert dollars into service. If we could do better with the dollars we have available, but we don’t, the responsibility must be ours. In EMS, that respon-
sibility is enormous—it is impossible to waste dollars without also wasting lives.”
Use of Lights & sirenLights for safety on scene ... but if it’s a residence, we will usually turn them off once we arrive and no sirens at night in town .... we live in a small rural community and traffic is generally not an issue.
Leslie LloydVia Facebook
This issue again ... Sigh. Sadly, we as a profession of car-ing, are stuck utilizing all emergency signaling devices to be recognized as an emergency operation. Litigation against our fellow professionals has consistently found us at fault when we try to be ‘reasonable’ to the public and run silent to aid a neighbor. Running silent draws the criticism that we don’t take the response seriously. Using the signaling devices wakes everyone up and gets us tagged as hooligans with no regard for the public. It is with a wince that I flip the switches and roll using the signaling devices as the lesser of the evils is not getting you and your department stuck in a lengthy and costly litigation should the untoward take place.
David M. NeptuneVia Facebook
If the nature of the call merits an emergency response it gets one. An emergency response means lights AND sirens, not lights OR sirens. The time of day has nothing to do with it. JEMS
Bob Upson Via Facebook
Letters>> continued from page 18
Do you have questions, comments or concerns about recent JEMS or JEMS.com articles? We’d love to hear from you. E-mail your letters to editor.jems@
elsevier.com or send to 525 B St. Suite 1800, San Diego, CA 92101, Attn: Allison Moen.
interesting fACt ABoUt A photo thAt rAn in oUr AUgUst 2012 issUe Photographer Kathy Keatley Garvey took this rare photo that won an international award and has drawn international acclaim on the Internet. It was named one of the top images of 2012 on huffington Post and also was select as “Picture of the Day” on numerous websites. Garvey captured this image of a bee stinging Cooperative extension apiculturist eric Mussen of the University of California, Davis, Department of entomology in the apiary of the harry h. laidlaw Jr. honey Bee research Facility, UC Davis. What’s unusual about this photo is that this sting was not a clean break; you can see the abdominal tissue being pulled out as the bee tries to leave.
Kathy Keatley Garvey is a communications specialist with the UC Davis Department of entomology and a former newspaper editor but enjoys taking macro photos of insects in her leisure time. She also writes a daily educational Bug Squad blog on the UC agriculture and Natural resources website; the blog, a volunteer blog, has garnered some 3 million hits in three years.
018_020LETTERS.indd 20 8/15/2012 9:31:16 AM

Choose 20 at www.jems.com/rs
0912-FP_RT.indd 1 8/14/2012 2:07:20 PM

Just after midnight on July 21, moviego-ers and responders in Aurora, Colo., were subjected to real-life horror and chaos
when a heavily armed gunman dressed in full body armor exited and returned via a rigged door during a premiere showing of the latest Batman movie, “The Dark Knight Rises” and fired on the packed audience. The gunman killed 12 people and wounded 58 others.
It was a horrific event, complicated by many factors: the early morning time, a dark environment both inside and outside the theater, and the presence of a chemical agent designed to debilitate the victims and make easier, less resistive targets. Not to mention the incident also involved the panicked and chaotic exodus of hundreds of moviegoers—many with serious injuries—who fled, in all directions not only from the fully packed room, but also into other nearby rooms, hall-ways and concession areas.
Many horribly injured victims who fled from a multitude of exits sought help from the first public safety personnel they could find. In many cases, the first person of contact was a police officer. Although EMS and fire resources were on the scene and still respond-ing, the multitude of factors presented above didn’t allow for a standard mass casualty incident (MCI) set up and action plan.
A gag order by the judge overseeing the legal aspects of this case has limited the release of information about the incident and ability of responders to tell their side of the story. So it’s frustrating to read newspaper accounts and challenges about the way the Aurora Fire Department and their contracted ambulance provider, Rural/Metro Corpo-ration, responded, treated and transported patients. The local media has been critical of the seemingly short supply of ambulances during the first 30 minutes of the incident. And much has also been written about the police transporting victims rapidly from the scene to definitive care.
Any seasoned responder who has arrived on scene at an MCI knows that even under
the best of conditions, a mass exodus of the injured and uninjured from an incident can be difficult to manage. Sorting out the injured in a dark parking lot and at multiple exit points is a complex task. The rapid transpor-tation of victims from that scene with criti-cal penetrating and exsanguinating gunshot wounds in police vehicles may in fact turn
out to be a key lifesaving effort—as it was when President Ronald Reagan was shot in Washington, D.C. and rapidly transported to a trauma center in his limousine.
JEMS will report on this major incident when appropriate clearances are received. Until then, don’t prejudge our colleagues in Aurora. —A.J. Heightman, MPA, EMT-P
PRIORITY TRAFFICNEWS YOU CAN USE
22 JEMS SEPTEMBER 2012
News media prematurely critiques incident Aurora Active shooter
Audio from Aurora shooting: www.jems.com/video/news/audio-colorado-theater-shooting
AP
PhO
tO/E
d A
Nd
riES
ki
Police officers were thrust into a patient transportation role in Aurora.
The media was critical in initial reports of a slow EMS response of resources to the Aurora shooting, but JEMS Facebook fans quickly jumped to their defense:
>> Michael Torchia: We can train for these situations but no two situations are ever the same, and we’re humans not robots. The press never says, “they did two things wrong but 100 things right.”
>> Suzi Pierce-Green: I saw where our agencies were on the news saying they practice and prepare for such an event, and all I could think is NO MATTER how much you prepare it’s a charlie foxtrot and everyone just does their best. My hat is off to them in the great job they did!
>> KimiAnn Corey: People need to understand we have a system/protocols we have to follow for that stuff. There were on scene within minutes, but they had so many patients in the parking lot bombarding [them] that they couldn’t just bypass.
>> Bobby Dorrell: You’re not helping anyone if you as a responder get hurt. In a situation like that, scene safety is the top priority.
Join the conversation at www.facebook.com/jemsfans
Defending THEir own
022_024PT.indd 22 8/17/2012 12:14:28 PM

www.jems.com sePTemBeR 2012 JEMS 23
Robe
Rt K
nes
ch
Ke/D
Rea
mst
ime.
co
m
Federal law addresses Critical Drug Issues
eMS providers are patient advocates and voices for
the sick, injured, and some-times, even the deceased. During such events as the unfortunate mass shoot-ing at the movie theater in Aurora, Colo., providers are often tasked with ensuring family members and relief agencies know about the status of the victims. Thankfully, Health Insurance Portability and Accountabil-ity Act (HIPAA) makes the sharing of critical patient information a little easier during an MCI.
>> disaster relief entities: HIPAA allows EMS providers to share informa-tion about a patient’s location, general condition or death with an agency
that’s authorized to assist in disaster relief efforts. This information can be shared with the disaster relief agency for the purposes of notifying a family member, a personal rep-resentative of the patient or another person responsible for the patient’s care. So EMS providers can release patient information to such entities as the American Red Cross, a state emergency management agency or
another similar type of entity to enable that organization to contact someone who’s responsible for the patient’s care.
>> Family Members and Friends: HIPAA also permits EMS providers to dis-close information about a patient’s location, general condition or death to a patient’s family member, relative, close personal friend or any other person who might be involved in the patient’s care. Bystanders, how-ever, are a different story. Even if a bystander is truly concerned about a patient’s welfare, or may have even assisted the patient before you arrived on the scene, you may not share patient information with them, unless the patient agrees.
There are two rules that you must follow when providing patient informa-tion to relief agencies or family and friends:
1. If the patient is competent and able to make healthcare decisions, you should first obtain the individual’s agreement to share the information, or at least give him/her an opportunity to object. The patient’s verbal agreement is enough. You can also infer from the circumstances that the patient doesn’t object to you sharing the information. For exam-ple, if you ask the patient if there’s anyone you can contact and they say “my spouse,” you can infer that the patient is OK with giving infor-mation to the spouse.
2. If the patient is incapacitated, which is often the case in MCIs, then providers can disclose patient information if they believe that disclosure is in the best interests of the patient. HIPAA permits providers to use their best judgment here in gauging how much information they should share. Just remember to keep the patient’s
Pro Bono is written by attor-neys doug wolfberg, ryan stark and steve wirth of Page, wolfberg & wirth llC, a national EMS-industry law firm. Visit the firm’s website at www.pwwemslaw.com for more EMS law information.
Choose 21 at www.jems.com/rs
022_024PT.indd 23 8/15/2012 11:22:22 AM

best interests in mind and to not disclose more than the patient’s location, general condition or death.
Finally, there’s always the concern about others overhearing discussions between two crew mem-bers or radio transmissions. But these types of inevi-table disclosures are called “incidental disclosures” under HIPAA and generally don’t pose a HIPAA viola-tion. In addition, if it’s necessary to ask a bystander, police officer, news reporter or other non-medical person to assist you in treating, moving or trans-porting a patient in a mass casualty situation, you may do so.
HIPAA always permits you to share patient infor-mation for treatment-related purposes with any party who’s also involved in the treatment of the patient. And it isn’t a HIPAA violation to transport multiple patients in an ambulance or other vehicle. Sometimes, an emergency simply overwhelms the available resources, and HIPAA recognizes that inci-dental disclosures will occur.
All of us at Page, Wolfberg & Wirth would like to express our deepest sympathy for the victims and everyone affected by the tragedy in Aurora.
We also express utmost gratitude to all of the responders who answered the call on that fateful morning, and those across the U.S. who continue to answer that call every day. We’re honored to rep-resent an industry that’s solely committed to the
care of others in need. The authors are all attorneys with Page, Wolf-
berg & Wirth, a national EMS law firm. Visit the firm’s website at www.pwwemslaw.com for more informa-tion on a variety of EMS law issues.
24 JEMS SEPTEMBER 2012
>> continued from page 23
For more of the latest EMS news, visit JEMS.com/news
QUICK taKeAs emergency medicine evolves, the National Institutes of Health (NIH) recently opened an Office of Emergency Care Research (OECR) to bridge research from institute to institute and from academia to institute. At this time it’s composed of an office of two to three people, a working group of 23 and a steering group of five. Walter Koroshetz, MD, is its acting director.
“This was the recommendation of a steering committee’s strategic plan to create this office. We want to be sensitive to all of our institutes,” he says.
After five years of discussion with the NIH and the emergency medicine community, the creation of the office was announced late in July.
The NIH is composed of 27 institutes, such as nursing, neurology and child health. With the new office, the many disciplines of research that fall under the huge tent of emergency medicine have the potential to work together better and become greater than the sum of their parts.
“We all do emergency research. The OECR is a convergence point between those institutes,” Koro-shetz says.
Although still in its infancy, Koroshetz is excited about the prospects and will recruit a permanent direc-tor. “The time is right. Research in an emergency setting is more feasible now working with a good set of investigators. —Devin Greaney
Choose 22 at www.jems.com/rs
022_024PT.indd 24 8/17/2012 12:14:45 PM

Choose 23 at www.jems.com/rs
0912-FP1_RT.indd 1 8/14/2012 2:17:46 PM

LEADERSHIP SECTORpresented by the iafc ems section
>> by gary ludwig, ms, emt-p
26 JEMS SEPTEMBER 2012
Bob is a newly promoted EMS manager who has been hired from another state to lead an EMS agency. On his
first day, things didn’t go well. He came into the office and greeted only his secretary and next in command. People who wanted to meet him never got the chance because the second-in-command monopolized his time. The second and subsequent days went the same way. Bob never got out of the office. Soon, word trickled to those working in the field that the new boss was an unfriendly, aloof jerk. As could be predicted, everything went downhill from there.
EMTs, paramedics, and people who worked in the EMS administrative offices really didn’t like Bob. He could never get everybody on board with the changes he wanted to implement. People within the EMS organization became resistant to him, didn’t like his approach and grumbled about every policy he issued.
Within six months, Bob was looking for a new job because he wasn’t happy either. Within a year, the Board of Directors let Bob go. What did Bob do wrong? He had a wonderful track record in his other EMS organization, and he had a fantastic resume.
What Bob failed to recognize is that if you’re the new leader of an EMS organiza-tion, it isn’t business as usual on the first day you walk through the door.
YOuR FIRST DAYI’ve always seen this as a make-or-break point. I’ve seen some good people get run out the door because of the way they came in the door. Everybody’s going to be watching what a new manager does and says, as well as observing how they react to different situa-tions. If you’re a new EMS manager and have come in from the outside, your employees will really be watching you.
My first suggestion is to say “hello,” and meet everyone. People want to feel important, and they certainly want to be
recognized by the boss on the first day. Make sure you meet every employee, acknowledge them and give them a personal greeting—from the janitor all the way up to your secre-tary or the next in command.
When you first enter a new organization as the new boss, you should remain positive. If you’re critical of the organization’s cur-rent operation—especially if you’re coming in from the outside—it might not go over well. People will see it as an attack on their organization. Even though you’re a part of the organization, you haven’t been accepted yet. Such statements as, “We did it this way where I just came from” may polarize you and your employees.
Next, I recommend not changing any-
thing until you learn the works and the dynamics that make it function. It’s espe-cially important not to change anything that has to do with the culture of the organiza-tion. If your first act is to change the patch or the name of the organization, expect a tre-mendous amount of resistance and trouble.
People who are already within the orga-nization have created their identity with the organization. Although some may grum-ble, they still take pride in the organization they’re associated with. Taking that away from them can only bring you headaches.
MY ExPERIEnCEWhen I came to Memphis seven years ago, I got around and talked to most of the firefighter/paramedics about the organization and how EMS operated in the department. One of the biggest complaints I heard was about a qual-ity improvement (QI) form that was issued to everyone from a QI officer if you missed something on the patient care report.
A QI officer would show up at your station and make you sign the form acknowledging that you missed something. Quite frankly, it really pissed people off when the situation was their 12th trip of the day at 4 a.m. and they failed to check a box on the patient care report. It was one of the major things I heard, and it really seemed to set them off. I failed to see the significance of the form because it seemed to make the QI process punitive with having to sign the form acknowledging you did something wrong.
So looking for the “low-hanging fruit” and looking for the chance to set the right positive attitude being the “new guy” com-ing in from the outside, I immediately got rid of the QI form. The response was over-
whelmingly positive and upbeat. The crews were elated with my decision. They felt I was a good selection for the organization and I was going to move the EMS part of the fire department forward. It
helped me consolidate support for some of the tough decisions I had to make down the road with changes that were necessary, while maintaining high morale.
COnCLuSIOnBeing new to an EMS organization is a chal-lenge. If you’ve moved a great distance, there’s added stress with moving and finding housing. There’s no need to add to that stress by taking the wrong approach with your entry into the organization. Stay focused, observe and start slow. If you’re successful with your entrance, you will have an easier time down the road making the changes you think are necessary. JEMS
First DayNow what?
Make sure you meet everyone, acknowledge them & give them a personal greeting.
Gary Ludwig, MS, EMT-P, has 35 years of
EMS, fire and rescue experience. He currently
serves as a deputy fire chief for the Memphis
Fire Department. He’s also Chair of the EMS
Section for the International Association of
Fire Chiefs. He can be reached through his website at
GaryLudwig.com.
026LEADERSHIP.indd 26 8/15/2012 9:31:52 AM

Choose 24 at www.jems.com/rs
0912-FP2_RT.indd 1 8/14/2012 2:19:04 PM

TRICKS OF THE TRADEcaring for our patients & ourselves
>> by thom Dick, emt-p
28 JEMS september 2012
My state has a law that says if your emergency warning lights are on during a response, your siren
needs to be on as well. Always. Most laws here are pretty sensible. But like so many things that stipulate “always” or “never” in this business, this one’s goofy.
There are times when the last thing you want to do is advertise your arrival or your intentions in advance. That’s true all the time in some neighborhoods. And it’s fun-damental on interstates, where you pretty much have to expect other drivers to do silly things.
Just for a moment, Life-Saver, put your-self in the mind of the motorist I’m about to describe.
It’s close to dusk. You’re cruising home from work at 65 miles per hour, nodding to your favorite loud music. Suddenly and with-out warning, you’re overwhelmed by a pair of siren speakers that somehow got within 20 feet of your rear bumper. (Yep, that’s way too close.) In addition, your rearview mirror reveals a big blue, elliptical Ford sign with a few inches of a shiny grille around it, and its silver details reflecting the rhythmic flashers of—ohmigosh—an ambulance. (How’d that get there?)
What would you do? Seriously, would you have a seizure? Wet yourself? Pull over quickly and switch places with your front-seat passenger? Slam on the brakes? Speed up and pull to the right without so much as a glance for traffic in the adjoining lane? Lower your window and wave for them to pass? Flip them off? Or turn up the music and drown out that awful woop-woop noise?
Even a year of experience should tell you that if those options were actually offered on a driver’s license renewal test as multiple-choice answers, plenty of licensed drivers out there would consider at least a few of them as viable options.
See, I don’t think most drivers are accus-tomed to making emergency decisions. And when they try, they sometimes make errors
in judgment. (At 65 miles per hour even the smallest errors can have big consequences, can’t they?)
I think of emergency warning equipment as a tool. And I think its applications are generally different on city streets than on interstates. On city streets (at lower speeds), a siren keeps pedestrians on the sidewalk and helps an ambulance get people’s atten-tion from behind so you can ask for the right of way. (Remember it’s ask, not demand.) On interstates, you use it instead to mitigate traffic flow once you’ve gotten past other motorists. But either way, you need the flex-ibility to choose which kinds of warning equipment to use in any given situa-tion. (That might include no warning equipment at all, even during high-priority calls.)
On interstates, the California Highway Patrol (CHP) routinely employs the use of no forward-facing lights and no sirens while they’re en route
to interstate calls. The CHP has known for years that most drivers can’t hear a siren at higher speeds until you’re right on top of them. Most drivers also don’t monitor their rearview mirrors, so they tend to not notice those forward-facing lights anyway. Offi-cers concentrate on sneaking through traffic without startling or scaring anybody. They try to use their rear-facing lights to advise drivers in their wake that they’re respond-ing to an incident. That helps them explain their use of the shoulders, lane changes and sometimes speed.
As emergency vehicle operators, it’s incumbent on us to think for other drivers. We should be doing no harm, not only medi-cally but also in regard to our emergency driving. And as you know, we can do a lot of harm by causing just one other driver to panic.
It’s time to abandon our outdated practice of flooding our cities and interstates with noise every time we respond to an emer-gency. It’s time for all emergency vehicle operators to consider some sort of stealth-mode option as a matter of routine, espe-cially on busy interstates. I also advocate one other thing, and I realize not everyone will agree with it.
You can usually tell when your warning equipment is confusing people. When that happens, your safest option is to shut it down and advise your communications cen-ter that you’re cutting your “code” response due to traffic. That gives dispatchers the option of selecting a more appropriate unit for your call, or at least it tells them you’re going to be delayed. Delay is an acceptable option to hurting innocent people.
Especially our own. JEMS
Thom Dick has been involved in EMS for
41 years, 23 of them as a full-time EMT and
paramedic in San Diego County. He’s currently
the quality care coordinator for Platte Valley
Ambulance, a hospital-based 9-1-1 system in
Brighton, Colo. Contact him at [email protected].
STealTh MoDeIs all this noise really necessary?
ambulances should go into stealth mode during the night instead of flooding cities with unnecessary noise.
pho
to c
hri
s sw
abb
028TRICKS.indd 28 8/15/2012 9:32:35 AM

Choose 25 at www.jems.com/rs
0912-FP_RT.indd 1 8/14/2012 2:20:11 PM

CASE OF THE MONTHDILEMMAS IN DAY-TO-DAY CARE
>> BY TRAvIS POLk, MD, & CARRIE SIMS, MD
30 JEMS SEPTEMBER 2012
It’s easy for a current and former military physician working in a busy urban trauma center to look around and see the count-
less advances in trauma care that have been translated from the military to civilian expe-rience. This month’s case highlights just one of the many lessons learned from caring for injured service members.
PrEHOSPiTAl COurSEWhen a 72-year-old male who was driving unrestrained in his sedan along the highway was suddenly struck from behind, he lost control of his vehicle and it rolled. His left arm, which was resting in the open window, was crushed.
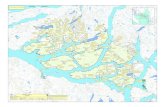
Philadelphia Fire Rescue medics arrived at the scene and found the patient in a large pool of blood with a severely deformed left arm dangling by what seemed to be a thin connec-tion of soft tissue. There was profound, pul-satile bleeding. Medics applied a tourniquet to the arm above the injury and tightened it until the bleeding stopped. They then immo-bilized the patient on a spine board, obtained IV access and administered morphine for pain control, splinted his arm with blankets as best they could and transported him to the trauma center at the Hospital of University of Pennsylvania as a “trauma alert,” the high-est level of activation. The patient remained hemodynamically stable during the transport.
HOSPiTAl COurSEOn arrival, the trauma team quickly com-pleted a primary survey, attached the patient to monitors, exposed and rolled the patient, and obtained additional IV access. Initial vital signs were heart rate=126, blood pres-sure=162/100, respiratory rate=20, tem-perature of 96.9° F and pulse oximetry of 100%. His Glasgow Coma Scale score was 15. Secondary survey was notable for some spi-nal tenderness, abrasions on the back and the obvious near amputation/de-gloving defor-mity of the left forearm. The tourniquet was in place above the elbow, and the bleeding was
stopped. A focused assessment with sonog-raphy in trauma (FAST) ultrasound exam showed no blood in the abdomen, and a chest X-ray was unremarkable.
The tourniquet was carefully released to better examine the arm. This resulted in severe pain for the patient in the area above and surrounding the wound. Pulsatile bleeding appeared to emanate from the vicinity of the radial artery. A limited neurologic exam of the hand with the tourniquet released revealed no evidence of motor or sensory function during this brief interval. Because of the persistent bleeding, the tourniquet was reapplied.
The patient remained in extreme pain and became agitated. At this point, since a neurologic exam had been performed and the patient would be going to the operating room (OR), the medical team proceeded with elective endotracheal intubation to provide adequate sedation and analgesia. Following intubation, the patient was brought to the computed tomography (CT) scanner for imaging of his head, C-spine, chest, abdomen and pelvis. No other injuries were identified.
THE OPErATiNg rOOMThe patient was brought to the OR and
underwent repair of the radial artery, liga-tion of the ulnar artery, external fixation of the radius and ulna, extensive irrigation and debridement of devitalized tissue, and wound coverage with cadaveric skin. He was extu-bated the following morning, and exami-nation of his hand revealed mostly intact sensation and slight movement in his thumb and fingers.
Of note, the patient’s medical history was significant for coronary artery disease and deep vein thrombosis. On initial evaluation, he reported taking aspirin, clopidogrel and warfarin. He was treated with vitamin K via IV and transfused with fresh frozen plasma and platelets for presumed drug-induced coagu-lopathy. His initial hemoglobin was 10.3 gm/dL with an international normalized ratio of 1.1. Given his history of significant blood loss and ongoing hemorrhage, he was trans-fused three units of packed blood cells in the OR. His tetanus status was unknown, so he received a tetanus vaccine. He was treated with broad spectrum antibiotics for his open, severely contaminated fracture.
At the time of this article, the patient had left the intensive care unit, but he remained in the hospital three weeks. On
Life & LimbTourniquet saves man severely injured in vehicle crash
PhO
TO C
Ou
RTES
Y T
RAv
IS P
OLk
This image shows the patient’s arm with a tourniquet shortly after arrival in the emergency department.
030_31CASE.indd 30 8/15/2012 9:33:06 AM

www.jems.com sePTemBeR 2012 JEMS 31
the road to salvation of his limb, the patient had five surgeries, including placement of antibiotic impregnated beads and free-flap tis-sue transplantation.
DiscussionExsanguinating hemorrhage from isolated extremity trauma in the civilian setting is rare. Unfortunately, due to mixed messages in much of the civilian medical literature and first aid texts, many providers are hesitant to place a tourniquet for fear of causing further injury or committing the patient to an ampu-tation. The military experience during the past several years, however, has demonstrated how this simple technology can be both life- and limb- saving.
Historically, the mortality rate from exsanguination from extremity trauma on the battlefield has been approximately 9%.1
A retrospective study of special operations personnel deaths in the global war on ter-ror found that 13% of the potentially pre-ventable deaths might have been prevented with a tourniquet.2 Likewise, a large prospec-tive study examining the use of prehospital and emergency department tourniquet use in a combat support hospital in Iraq found that early use of tourniquets not only provided hemorrhage control but also improved mortality.
In a series of more than 400 applied tour-niquets, no amputations were associated with inappropriate tourniquet use, and few were associated neurologic complications.3 For these reasons, in 2005, the U.S. Army adopted a new standard Tactical Combat Casualty Care guideline that tourniquets should be first-line treatment for any life-threatening extremity trauma while under fire.
Although extremity trauma in the civilian setting is rare, studies show that it’s deadly. A similar retrospective study of exsanguinating extremity trauma in the civilian population identified 14 patient deaths during a period of five and a half years at two Level 1 trauma cen-ters in Houston. Of these 14 patients, 57% had wounds that would have been amenable to the placement of a tourniquet, and therefore potentially could have been saved.4
conclusionGiven this information, civilian EMS providers should feel confident that placing a tourniquet for severe extremity hemorrhage that isn’t controlled by other means is safe, appropriate
and life-saving. Studies also show they should be applied early and before the patient is in shock.3
A variety of tourniquets are available for EMS use. EMS units should work with their medical directors to select and train with the device that best suits their needs. As this case illustrates, the use of a tourniquet was life-saving for this patient and should always be considered in cases of severe extremity trauma. JEMS
Travis Polk, MD, is a trauma surgeon on active duty in the
U.S. Navy currently stationed at the Naval Medical Center in
Portsmouth, Va. He is board certified in general surgery and
board eligible in surgical critical care. At the time of this case,
he was an instructor in surgery and fellow in traumatology,
surgical critical care and emergency surgery at the University
of Pennsylvania in Philadelphia. He can be contacted at
Carrie Sims, MD, is an assistant professor of surgery at
the University of Pennsylvania in Philadelphia and is a for-
mer U.S. Army Reserve Medical Corps Officer. She is board
certified in surgery and surgical critical care and practices as
a trauma surgeon and surgical intensivist. She can be con-
tacted at [email protected].
Disclaimer: The views expressed in this presentation are those of the author and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the U.S. govern-ment. Dr. Polk is a service member. This work was pre-pared as part of his official duties. Title 17, USC, §105 provides that “Copyright protection under this title is not available for any work of the U.S. government.” Title 17, USC, §101 defines a U.S. government work as a work prepared by a military service member or employee of the U.S. government as part of that per-son’s official duties.
RefeRences1. Bellamy RF. The causes of death in conventional
land warfare: Implications for combat casualty careresearch.MilMed.1984;149(2):55–62.
2. Holcomb JB, McMullin NR, Pearse L, et al. Causes ofdeathinU.S.SpecialOperationsForcesintheglobalwaronterrorism:2001–2004.AnnSurg.2007;245(6):986–991.
3. KraghJF,WalterTJ,BaerDG,etal.Survivalwithemer-gencytourniquetusetostopbleedinginmajorlimbtrauma.AnnSurg.2009;249(1):1–7.
4. DorlacWC,DebakeyME,HolcombJB,etal.Mortalityfrom isolated civilian penetrating extremity injury. JTrauma.2005;59(1):217–222.
When placing the tourniquet, providers should remember the following:>> Tighten until all bleeding stops. If the wound is still bleeding, you likely have a venous tourniquet, and it
may need to be tightened further or repositioned in order to occlude all arterial inflow.>> Place as low on the extremity as possible.>> Note the time that the tourniquet is applied. (Paperwork gets lost and people don’t always listen during the
report, so write it on the patient too!)>> Tourniquets are extremely painful; administer some pain medication.
Rad
iog
Raph
Co
uRt
esy
tRa
vis
po
lk
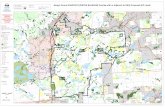
This plain radiograph shows the severely comminuted fracture of the patient’s forearm.
030_31CASE.indd 31 8/15/2012 9:50:16 AM

I CO-OxImetry effeCtIveness IWeaver L, Churchill S, Deru K, et al. False positive rate of carbon monoxide saturation by finger probe oximetry of emergency department patients. Respir Care. 2012 Jul 10. [Epub ahead of print]
Should you trust your pulse CO-oximeter (SpCO) monitor? During the past few
years, there have been conflicting messages about the accuracy of these devices. This Salt Lake City-based emergency department (ED) group attempted to answer that question by comparing Masimo RAD-57 SpCO monitor readings from a finger probe/sensor, to the carboxyhemoglobin (COHb) readings from a simultaneous blood draw.
Three lab technicians collected SpCO and COHb samples on 1,363 ED patients receiv-ing blood draws from April to August 2008. This was a non-randomized sample of conve-nience study conducted at a single hospital.
The authors report that 84% of the study’s population was light-skinned and 45% were male. Fifty-two of the people studied were non-smokers. A variety of patient complaints existed, but the SpCO monitor flagged 122 patients, meeting a false positive criteria. A false positive was considered if the SpCO showed a value greater than a 3% point differ-ence than the actual COHb level.
Only four patients were actually diagnosedwith CO poisoning from the entire sample. In these cases, the SpCO oximetry monitor reading was 4–14% lower than COHb blood levels, which led the authors to conclude that the RAD-57 reports lower numbers than COHb. So far so good, right?
Well, three other patients with COHb greater than 10% received a 0% rating on the SpCO monitor. If the SpCO value of 0% had been used as a field triage tool, then these patients may have not received necessary evaluation and treatment at an ED.
So what should we conclude? First, the good: Previous studies have followed some flawed methodologies and didn’t adequately describe the details of their methodologies.
(See a review by Keith Wesley, MD, FACEP, and Marshall Washick, NREMT-P at www.jems.com/article/patient-care/rad-57-pulse-oximeter-performa.)
The authors of this Salt Lake City hospital study were careful to describe their methods and avoid some of the previous pitfalls of other researchers (e.g., timing of the blood draw). The authors did not report whether the sensors were shielded from excessive ambient light, if patient motion was reduced, or if the various sensor sizes were used, which are each important considerations with the Masimo CO-Oximeter. They did report that the device performed within the margin of the manufac-turer’s specifications.
And, from a purely statistical and research perspective, the sample of patients with detectible CO levels is simply too small to make any meaningful conclusions.
The concern a study like this presents is that, if we are to use this device for prehos-pital triage of potential CO exposures, then it would be preferable that the device would be sensitive enough to detect any potential exposure, and perhaps err on the side of over-triaging. Sending someone home based on a RAD-57’s “0” or low reading if that patient was actually sick, could be disastrous. Regardless of whether this was an operator or machine error, I worry about the patients with 0% readings who had elevated blood COHb readings.
I would feel pretty terrible sending some-one home only to find out they had a treatable condition that caused them harm because of my lack of action. The contro-versy will continue, but this is an important reason never to just base your field triage decisions on any machines. Instead, provid-ers should use these devices in conjunction with other assessment processes and treat-ment tools, particularly when patients have potentially been exposed to CO or have CO symptoms.
I nausea Cure? IFullerton L, Weiss S, Forman P, et al. Ondansetron oral dissolving tablets are superior to normal saline alone for prehospital nausea. Prehosp Emerg Care. 2012. [Epub ahead of print.]
This prehospital cohort study compared the use of normal saline bolus with an
odansetron orally dissolving tablet (ODT) for the treatment of nausea. Researchers enrolled 274 consecutive patients to receive
32 JEMS SEPTEMBER 2012
researCH revIeWWhat current studies mean to ems
>> by david Page, ms, nremt-P
EffEcTivE carEStudies measure CO-detection device & nausea treatment
researchers analyzed the false positive rate of car-bon monoxide saturation on the raD-57 monitor.
Pho
to d
av
id P
ag
e
BOttOm LIneWhat we know: The RAD-57 is being used by many systems across the country. The machine has shown great promise and helped identify many CO exposures. Previous research has raised concerns regarding its accuracy.
What these studies add: This study provides very weak evidence of a possible 9% false positive rate and confusion about the trustworthiness of a low RAD-57 number based on only five patients. More rigorous study is needed before any conclusions can be made. Providers are encouraged to talk to their medical directors and be sure to receive proper orientation and training before using any medical device.
32_33ResearchReview.indd 32 8/17/2012 12:15:36 PM

www.jems.com sePTemBeR 2012 JEMS 33
David Page, MS, NREMT-P, is an educator at Inver Hills Community College and a paramedic at Allina EMS in Minneapolis/St. Paul. He’s a member of the Board of Advisors of the Prehospital Care Research
Forum. Send him feedback at [email protected].
Visit www.pcrfpodcast.org for audio commentary.
I watch box I
Blanchette C, Dalal A, Mapel D, et al. Changes in COPD demographics and costs over 20 years. Journal Med Econ. 2012. [Epub ahead of print.]
This cross-sectional, population-based study should pique the curiosity of community para-medic advocates. They report rapidly rising in-hospital admission costs and more prevalence of chronic obstructive pulmonary disorder (COPD) in women. This survey of 416 respondents shows a 37% increase in the cost of caring for COPD dur-ing the past 20 years. The authors conclude that COPD has become a costly disease, which is now more prevalent in women than men. The authors recommend shifting costs to fund prevention and conducting follow-up efforts to avoid readmission of patients back into the hospital.
Perhaps the community paramedic model will play a role in improving this part of the healthcare system.
normal ODT during a four-month period. As you would have predicted, the ODT group showed significantly decreased nausea symptoms. No amount of normal saline was able to show a significant effect. No adverse events were reported, and the two groups of patients were similar in ages and severity of nausea. This study shows a clear win for odansetron and for ALS care making a difference.
Kudos to this group for doing prehos-pital research. Many of us have seen odan-setron work its magic, but having some science to back up its safe and efficacious use makes for a more scientific and profes-sional care standard. JEMS
I glossary ISample of convenience: A sample of convenience is a grouping of research subjects or values collected because they were easily available. They aren’t randomized or otherwise scientifically selected, and generally they’re not repre-sentative of or able to be generalized to an entire population.
choose 27 at www.jems.com/rs
choose 26 at www.jems.com/rs
32_33ResearchReview.indd 33 8/20/2012 4:26:59 PM

34 JEMS SEPTEMBER 2012
Feedback-driven team perFormance impacts survival>> By Jeffrey M. Goodloe, Md, NreMT-P, fACeP; T.J. reGiNAld, NreMT-P; dAvid S. HowerToN, NreMT-P;
JiM o. wiNHAM, rN, BSN, NreMT-P; & TAMMy APPleBy, NreMT-B
034_039EMSALiL.indd 34 8/17/2012 12:16:43 PM

Pho
to D
av
iD h
ow
erto
n
As EMS professionals, we’re routinely challenged to successfully resuscitate victims of sudden cardiac arrest. Fortunately, our
understanding of cardiac arrest pathophysiology continues to grow. More fortunate still, our enthusiasm in translating that understand-ing to effective therapies has never been greater.
In the August 2012 issue of JEMS, we introduced a comprehen-sive restructuring of the EMS System for Metropolitan Oklahoma City and Tulsa’s cardiac arrest program using a three-part approach: chest compression fundamentals, resuscitation team dynamics and accelerated feedback on resuscitation performance. We discussed the benefit of going “back to the basics” of chest compression fun-damentals training, increasing our rate to 120 chest compressions per minute and using metronomes to attain and maintain that rate
throughout resuscitations. Now, we share how those fundamentals were incorporated into a Resuscitation Team Playbook and how we use directed feedback to further refine resuscitation performance.
Step 2: Resuscitation Team Dynamics. Have you ever been a part of an EMS call that was particularly “busy” in activity, yet when the patient was transferred for further care, you started to think, “What did we actually get done?” Us too. In fact, it happens to all of us in
EMS providers go back to the basics in training for cardiac resuscitation.
www.jems.com sePTemBeR 2012 JEMS 35
For Step 1 and the introduction to this team’s approach to resuscita-tion, read “Oklahoma EMS System Strives for Higher Cardiac Arrest
Survival Rates” at www.jems.com /magazines/2012/august.
034_039EMSALiL.indd 35 8/15/2012 9:51:18 AM

36 JEMS SEPTEMBER 2012
cardiac arrest part ii >> continued from page 35
the inherently challenging practice of EMS medicine. We believe what you do with those reflections can make all the difference in the world for future patients. We therefore chose to turn our reflections, and those of our colleagues, into a Resuscitation Team Playbook that channels individual enthusiasms into a care-fully orchestrated team performance, often described favorably as “pit crew resuscitation.”
Figure 1 shows the positions used in our resuscitations, with roles defined for teams of one to six professionals. In our EMS system, we often start with resuscitation teams of two, three, or four, with subsequently arriving responders building that team to five or six actively contributing members. It’s rare in our system that one EMT or paramedic would be tasked with resuscitating a cardiac arrest patient alone, but it could happen for a brief period if a patient were to collapse at a nearly empty fire station or ambulance headquarters. We wanted to ensure we had all the possibilities covered, including the single rescuer scenario. Let’s review the key contributions provided by each position, so that you’ll be certain to include the care most likely to promote neurologically intact survival, regardless of resus-citation team size.
Position 1: Rapidly identifies arrest and initiates continuous chest compressions.
>> Alternates minutes of chest compressions with Position 2 over the course of the resuscitation.
>> When not compressing, assists with bag-valve-mask ventila-tions (squeezing the bag).
>> Minimizes pauses in chest compressions for rhythm deter-mination and/or defibrillation.
Position 2: Applies automated external defibrillator or monitor/manual defibrillator.
>> Mirror image of Position 1. Position 3: Provides airway management; avoids hyperventila-
tion.Position 4: Leads scene management.>> Interface with family/bystanders for events preceding
arrest and medical history.>> Supervises positions 1–3 for continuous compressions,
timely defibrillation, and no hyperventilation.Position 5: Provides ALS support.>> Rhythm determination and manual defibrillation.>> Vascular access.>> Medication administration.Position 6: Provides ALS support.>> Patient management leader.
At first, it looks like a lot of instruction—because it is. How-ever, these directives simply expand in detail on the key contri-butions at each position. You may think this degree of directive is micromanaging hardworking EMS professionals who already know the right things to do in time-sensitive situations. You’re right; it actually is micromanaging, but let’s look at why cardiac
The full playbook can be accessed at www.jems.com/patient-care
choose 28 at www.jems.com/rs
034_039EMSALiL.indd 36 8/17/2012 12:16:47 PM

arrest calls for no less. Try this exercise, literally. Do 20 jumping jacks. What do
you feel? Unless you’re in particularly athletic shape, you likely feel an increase in pulse and in respiratory rate and effort. Why? You’re compensating for an increased activity demand. The human body is amazing in its ability to compensate, even to some degree when severely ill or injured. But spontaneous circulation reflects an unforgiving light switch. When it’s “on,” compensation is at work. When it’s “off,” as in cardiac arrest, there’s complete loss of compensation … except for resuscita-tive efforts.
Thinking back to our understanding of cardiac arrest patho-physiology, we have to be precise in those efforts for our “com-pensation on loan” to work. The only way to make that happen comes when we use a carefully crafted plan (the playbook) and actively micromanage ourselves in each position (running the play). So in sum, it’s not micromanaging by others, it’s self-micro-managing, and it’s for all the right reasons.
We’ve definitely laid out a plan, but how do we know whether it’s the right plan? One quick answer you’ll say is by looking at neu-rologically intact survival rates—before and after adoption of this plan. In fact, that’s a great answer, but we think it comes up short as the lone answer.
In athletics, if a team loses a game, does that mean they played badly? Often, the answer is “not at all;” it may mean the team sim-ply played a better team, or depending on how score is kept, the team may have started with a handicap that’s insurmountable. Ever start a resuscitation feeling that you were working with such a handicap? That’s where Step 3 comes into use in our cardiac arrest program.
Step 3: Feedback on Resuscitation Team Performance. Every high-performance professional values feedback designed to “build up” future abilities. Our feedback program channels that philosophy using proprietary software that captures data from the monitor/
Figure 1: Resuscitation Positions
P4
P3
P1
Scene Management
Airway Management
Set Up AED/Defibrillator
Chest Compressions
Chest Compressions
Patient Management
Defibrillation Vascular Access
Medication Administration
P5P6
P2
Choose 29 at www.jems.com/rs
034_039EMSALiL.indd 37 8/15/2012 9:55:56 AM

38 JEMS SEPTEMBER 2012
cardiac arrest part ii >> continued from page 37
defibrillator throughout the resuscitation. Many EMS systems are using this type of capability, but the real value lies in merging data with a set of skilled clinical eyes, annotating the basic feedback forms. Credit goes to the Redmond, Wash., Medic One program for helping us see the full potential already in our grasp.
Only through annotating a case do specific gaps in compres-
sions, changes in ventilation rates and timings of defibrillation really become clear. No “real world” resuscitation will ever be textbook perfect. Thus, only through analysis by an experienced clinician does variability reliably fall into the “makes sense” or “opportunity to reflect” categories. Without annotation, a “report card” gets generated without showing a valid grade … arguably pointless, right?
Our goal is to have an annotated resuscitation team perfor-mance feedback report available to the resuscitation team on its next shift after working a cardiac arrest. The report is sent with explanation through annotated comments and without discour-aging remarks, even in areas for improvement. Those areas are self-evident, and we believe the best correction can come through team reflection.
So how are we doing in achieving our own goal? Currenrtly, just about 5% of the time. But here’s a key point, and one we’ve had to learn with hard experience: If you wait until everything is perfect to start improving, you never start improving. Like
EMS providers in Oklahoma City and Tulsa maintain a rate of 120 compressions, using metronomes in training.
pho
to d
av
id h
ow
erto
n
choose 30 at www.jems.com/rs
choose 31 at www.jems.com/rs
034_039EMSALiL.indd 38 8/15/2012 10:06:08 AM

most EMS systems, we’re understaffed in comparison with our goals. However, we’re fortunate in being able to hire a new data specialist position that’s dedicated full-time in our Office of the Medical Director. This position will dramatically improve our feedback abilities, both in volume and timeliness.
Even with feedback 5% of the time, the results are encourag-ing. We’re routinely seeing chest compression fractions (CCF) (i.e., time in which chest compressions are actively occurring) above 90%. In fact, many resuscitations are being performed with CCFs above 95%. (To be clear, these cases reflect random analysis, not just review of clear survivors.) These numbers reflect CCF increases 5–15% above our historical baselines. Not surprisingly, return of spontaneous circulation (ROSC) rates have increased since we started resuscitation team dynamics in February. Although we anticipate cardiac arrest survival rates in 2012 to be rewarding, it’s still early, and we don’t want to report on incomplete data.
ConClusion (For now)Our EMS system, just like yours, is committed to attacking car-diac arrest and doing everything we can to help the suddenly dead become alive again. Focusing our energies (with encouragement from friends throughout EMS) on chest compression fundamen-tals, resuscitation team dynamics and better timely feedback on resuscitation team performance—all in support of patients and the EMS professionals caring for them—makes a lasting influence on cardiac arrest. JEMS
Jeffrey M. Goodloe, MD, NREMT-P, FACEP, is professor and chief of the EMS section
of the Department of Emergency Medicine at The University of Oklahoma School
of Community Medicine in Tulsa. He serves as medical director for the Medical
Control Board in the EMS System for Metropolitan Oklahoma City and Tulsa,
working with a multitude of agencies, including the Emergency Medical Services
Authority (EMSA), the Oklahoma City Fire Department and the Tulsa Fire Depart-
ment. He started in EMS in 1988 as an EMT-B and has never quit learning. Contact
him at [email protected]
T.J. Reginald, NREMT-P, is director of research and clinical standards develop-
ment for the Office of the Medical Director in Oklahoma City and Tulsa. He’s a
driving force behind the success and continuing advancement of cardiac arrest
resuscitation in the major metropolitan areas of Oklahoma. His EMS career spans
three decades and includes a multitude of clinical and administrative leadership
roles. Contact him at [email protected].
David S. Howerton, NREMT-P, is director of Clinical Affairs - Western Division for
the Office of the Medical Director in Oklahoma City. He’s the medical oversight liai-
son officer for all metropolitan Oklahoma City agencies working with the Medical
Control Board. His EMS career spans nearly three decades and includes a multitude
of clinical and administrative leadership roles. Contact him at [email protected].
Jim O. Winham, RN, BSN, NREMT-P, is the immediate past director of Clinical
Affairs - Eastern Division for the Office of the Medical Director in Tulsa. He’s enjoying
a new career move as the general manager for Paramedics Plus - Oklahoma. His EMS
career spans more than three decades and includes a multitude of operational, clini-
cal and administrative leadership roles. Contact him at [email protected].
Tammy Appleby, NREMT-B, is executive assistant to the medical director for the
Office of the Medical Director in Oklahoma City and Tulsa. Retired from the U.S.
Air Force, she has an accomplished career in medical operation administration and
leadership. Contact her at [email protected].
Choose 32 at www.jems.com/rs
034_039EMSALiL.indd 39 8/15/2012 10:08:59 AM

40 JEMS SEPTEMBER 2012
Pho
to C
ou
rtes
y P
ort
lan
d F
ire
deP
art
men
t
Once adenosine is administered, its effectiveness lasts between five and 10 seconds.
040_045Adenosine.indd 40 8/15/2012 10:27:03 AM

ExpErt & safE usE of adEnosinE dEpEnds on patiEnt’s cardiac status
Pharmacology & mechanisms of actionAdenosine’s mechanism of action can be thought of as a “temporary paralyzing” of supraventricular tissue. Pharmacologically, adenosine hyperpolarizes the cell by stimulating an inward potassium current and temporarily inhibiting calcium migration.2 In doing so, the pace-maker activity of the sinoatrial (SA) node, spontaneous atrial activity and conduction through the atrioventricular (AV) node are dramati-cally slowed or temporarily stopped.
Adenosine has no effects on accessory pathways, such as those seen in the Wolf-Parkinson White Syndrome (WPW). Mild side effects of adenosine are common. They include a transient sinus pause that usually lasts less than five seconds, chest pressure or tight-ness, dyspnea, facial flushing and the feeling of impending doom (see Table 1, below).2–4
Rare, benign side effects reported include anxiety and dizziness. In one large prehospital trial, 11% of patients had a minor transient complaint, with chest pain being the most common complaint seen in 4% of patients.4 Chest tightness was induced by adenosine admin-istration in 83% of patients in one large in-emergency department (ED) study.5
side effectsSide effects from adenosine administration that are serious are extremely rare when used in healthy patients with PSVT (see Table 1, below). Adenosine may cause mild bronchospasm, which is almost always short lived. However, adenosine can also cause severe bron-
chospasm and should be given carefully to those with a history of asthma or chronic obstructive pulmo-nary disease (COPD).6 It shouldn’t be given to patients who are already wheezing. Adenosine has also been reported
to cause prolonged sinus pauses, syncope, seizures and even asys-tole, although this rare side effect has been described almost solely in older patients with preexisting conduction disease and/or second- or third-degree heart block.7–9 Adenosine is the drug of choice for PSVT in pregnant patients.1
The biggest dangers with adenosine are seen in two groups of patients: 1) those with atrial fibrillation or atrial flutter, and 2) those in sinus tachycardia and not PSVT.
www.jems.com sePTemBeR 2012 JEMS 41
>> By Corey SloviS, MD, FACeP; JAreD MCKinney, MD; & JereMy BrywCzynSKi, MD, FAAeM
Minor Major
Chest tightness Angina
Shortness of breath ventricular tachycardia
warmth Bronchospasm
Diaphoresis respiratory arrest
impending doom Cardiac arrest
Table 1: Toxicology of Adenosine
denosine is the drug of choice for paroxysmal supraventricular tachycardia (PSVT) and is once again Advanced Cardiac Life Support-approved for differentiating PSVT with aberrancy from ventricu-lar tachycardia (v tach) in patients with monomorphic wide complex tachycardias.1 Adenosine is a potent and safe antiarrhythmic when used appropriately. However, its use in the wrong patient or rhythm can prove fatal. This article focuses on how to expertly use adenosine and to know when this “safe” antiarrhythmic can be dangerous and contraindicated.
Figure 1a, 1b & 1c: regular wide-Complex Tachycardia
Figure 1b
Figure 1c
To verify true regularity, make marks on a piece of paper that match the peaks of the QRS then moving the QRS-marked paper a few beats over to compare it to three to four new beats on the rhythm strip. If they line up, the rhythm is regular; if they don’t, the rhythm is irregular, and adenosine shouldn’t be used.
040_045Adenosine.indd 41 8/15/2012 10:27:30 AM

42 JEMS SEPTEMBER 2012
Numerous studies in the literature report serious rhythm degeneration and even death when adenosine has been inadvertently given to patients with either atrial fibrillation or atrial flutter. Adenosine can convert rela-tively stable atrial flutter with 2:1 conduction and a heart rate of 150 to 1:1 conduction with a heart rate of 300 and cause rapid clinical decompensation.10
Adenosine slows or blocks antegrade (atrial to ventricular) conduction through the AV node but doesn’t affect accessory or bypass tracts like those seen in WPW syn-drome. Because of this, adenosine can be dangerous when given to patients with atrial
fibrillation, especially if they have a bypass track. Numerous reports show patients degenerating into rapid atrial fibrillation with rates at 250 or greater and becoming hemodynamically unstable.10–13
Thus, an absolute contraindication to adenosine exists in patients who have either atrial flutter or an irregular rhythm in atrial fibrillation. Because rapid atrial fibrillation may seem regular on ECG monitor, para-medics are urged to run a rhythm strip and verify true regularity.
We find this easiest by making marks on a piece of paper that match the peaks of the QRS then moving the QRS-marked paper a
few beats over to compare it to three to four new beats on the rhythm strip. If they line up, then the rhythm is regular; if they don’t, then the rhythm is irregular (and likely atrial fibrillation), and adenosine shouldn’t be used (see Figures 1a, 1b, 1c, p. 41).
The other absolute contraindication to adenosine is in sinus tachycardia. Dehy-drated patients, especially the elderly with fever, failure to thrive and/or an infection may appear to be in PSVT when in fact they’re barely compensated with a sinus tachycar-dia with a rate that may be greater than 150. These patients are at high risk for morbidity and mortality if adenosine is administered,
CheCk the Rhythm >> continued from page 41
Presentation Reason It Is Not PSVT
Heart rate of 150 or less At 150 atrial flutter 1:1; 150 or less usually is sinus tach
Irregular rhythm Atrial fibrillation or multifocal atrial tachycardia
Transiently slows to vagal stimulation Diagnostic of sinus tachycardia
History of atrial fibrillation, atrial flutter or multifocal atrial tachycardia (MAT) Marked increased likelihood of previous arrhythmia and not PSVT
History of COPD or CHF Atrial fibrillation or MAT much more likely
Table 2: When PSVT is not likely PSVT
Choose 33 at www.jems.com/rs Choose 34 at www.jems.com/rs
040_045Adenosine.indd 42 8/15/2012 10:27:19 AM

and they have a prolonged sinus pause (see Table 2, below).
In cases for which there’s any chance that sinus tachycardia is the etiology of the patient’s elevated heart rate, a rapid fluid bolus of 250 cc should be administered. Any slowing by just a few beats per minute (rather than a dramatic conversion to a normal sinus rhythm) confirms the diagnosis of sinus tachycardia due to volume depletion.
This is also true in heat stroke victims with PSVT at rates approaching 180 beats per minute. EMS providers should rap-idly hydrate and cool these patients before administering adenosine. If the patient’s
pulse begins to fall with therapy, the diagno-sis of sinus tachycardia due to heat illness and dehydration is confirmed, and adenosine is contraindicated. Table 2 lists the rhythms, rates and patient types in which the diagno-sis of PSVT should be considered unlikely.
AdministrAtion & dosAgeOnce adenosine is administered, its effec-tiveness lasts only between five and 10 sec-onds because it’s rapidly metabolized by cellular uptake. Because of the ability of blood vessel endothelium to metabolize adenosine, it’s imperative for EMS providers to give adenosine by rapid bolus followed by
a 10–20 cc rapid flush.2,3
Larger, more proximal IV lines are pre-ferred because small-bore IVs don’t rou-tinely allow fast flow or rapid transit to the heart. The dosage of adenosine should be reduced to 3 mgs if injected into a central line, and it shouldn’t be used in heart trans-plant patients.1,14
The standard initial recommended dos-age of adenosine is 6 mg, followed by a rapid saline flush. If this dose isn’t effective, EMS providers should double the dose to 12 mg, repeat the bolus and rapidly flush the line.1–
15 These recommendations come from the original article that compared adenosine
Figure 2: Prolonged Pause Status Post Adenosine
Choose 35 at www.jems.com/rs
040_045Adenosine.indd 43 8/15/2012 10:26:40 AM

44 JEMS SEPTEMBER 2012
CheCk the Rhythm >> continued from page 43
with verapamil in PSVT and used a vari-ety of adenosine doses. In this article, the investigators found that 6 mg of adenosine converted 62.3% of patients and that 12 mg converted 91.4% of patients without increase in toxicity.15,16
Because there doesn’t appear to be any increased toxicity in a 12 mg initial dose and it’s more effective, others have recom-mended starting at 12 mg.4,17 Some have rec-ommended doses as high as 18 mg, which can convert 95% of PSVT patients vs. 65% with 6 mg and 90% with 12 mg.18
Thus, paramedics and their medical directors should have pre-established pro-tocols beginning with 6–12 mg. These pro-tocol should conclude that a second 12 mg dose should be attempted if 12 mg is inef-fective,. This is because reports show a sec-ond repeat dose of 12 mg may convert up to 10–31% of patients.4,5
tReating Wide Complex taChyCaRdiaAdenosine was initially considered useful in helping distinguish wide complex tachy-cardias due to aberrantly conducted PSVT vs. true v tach. However, based on cases of patients deteriorating, many cautioned against trying this drug in any patient with wide complex tachycardia.14,16
We now know that adenosine is safe and can help distinguish supraventricular arrhythmias from those originating in the ventricle for monomorphic wide complex tachycardias that are regular in rate (and by definition, have the same QRS size and shape).1
In the largest recent study of adenosine in wide complex tachycardias, 197 patients were studied.16 Of these, 116 had SVT and 81 had v tach. Ninety percent of the SVTs responded to escalating doses of adenosine (i.e., administering 6 mg, then 12 mg, then repeating 12 mg if no response, and even administering 18 mgs to one patient). Only
one patient with proven v tach responded to adenosine, and a second patient may have transiently slowed.
The authors concluded that adenos-ine was safe as long as patients had regu-lar monomorphic wide complexes and that adenosine was useful in helping distinguish between PSVT and v tach. In fact, they noted a 36-fold increase in the likelihood of a
supraventricular origin if the wide complex tachycardia converted to sinus with adenos-ine and a nine-fold increased likelihood of v tach if it didn’t respond to escalating doses of adenosine.
Another thing is absolutely clear: Never give adenosine to a wide irregular tachycar-dia or a polymorphic (multiple different QRS configurations) tachycardia, such as Tors-ades de Pointes. It’s in these patients that ade-nosine might be lethal.1,16
Read about a real case of a patient who presented with Torsades de Pointes at www.jems.com/
torsades-de-pointes.
SummaRy, ConCluSion & ReCommendationSAdenosine is a safe and effective agent in PSVT. It’s currently the EMS drug of choice for regular tachycardias about 150–160 beats per minute, believed to be PSVT—whether wide or narrow. The side effects of
adenosine are usually mild and transient, lasting just a few seconds. They include chest tightness, shortness of breath and a short sinus pause. Although more serious side effects can occur, such as hypotension, bradycardias and seizures, these side effects are rare in healthy patients with no underly-ing heart disease.
Adenosine is contraindicated in patients who are likely to be harmed by its inappro-priate use. Patients with irregular heart rates, especially atrial fibrillation, patients with PSVT mimics such as atrial flutter with 2:1 conduction or sinus tachycardia in a dehy-drated or stressed patient should never receive adenosine.
Adenosine should never be used in wide irregular tachycardias. Providers who are going to use adenosine must be experts in
cardiac rhythm interpretation. They also must carefully review a rhythm strip prior to drug administration.
Our recommended starting dosage is 12 mgs via IV push followed by a 10–20 cc rapid flush of saline. If the first 12 mg dose isn’t effective after one minute, we recom-mend repeating 12 mgs a second time. EMS services and their medical directors should decide whether 6 or 12 mgs should be ini-tially used because there’s no national con-sensus on which is optimal. JEMS
Corey Slovis, MD, FACEP, is professor and chair of emer-
gency medicine at Vanderbilt and serves as the medical
director for Nashville (Tenn.) Fire Department and Nash-
ville International Airport. Slovis is also a member of the
JEMS Editorial Board.
Jared McKinney, MD, is director of event medicine for
Vanderbilt Medical Center, an assistant professor of emer-
gency medicine at Vanderbilt University Medical Center in
Nashville and is an assistant medical director for the Nash-
ville Fire Department.
Jeremy Brywczynski, MD, FAAEM, is medical direc-
tor of Vanderbilt’s aeromedical LifeFlight Program and an
assistant professor of emergency medicine at Vanderbilt
Table 3: Dosages & Protocol for Adenosine Administration
Adenosine Dosing
6–12 mg IV push in large-bore IV
Immediately flush with 10–20 cc normal saline solution
12 mgs IV push if not effective in 60 seconds
If protocol began with 6 mg IV, consider second dose of 12 mgs IV; push and re-flush line.
Contact medical control in the event of refractory cases
An absolute contraindication to adenosine is in patients who have either atrial flutter or an irregular rhythm as is seen in atrial fibrillation.
040_045Adenosine.indd 44 8/15/2012 10:27:26 AM

www.jems.com sePTemBeR 2012 JEMS 45
University Medical Center in Nashville and is an assistant medical director the Nash-
ville Fire Department.
RefeRences1. NeumarRW,OttoCW,LinkMS,etal.Part8:Adultadvancedcardiovascular
lifesupport:2010AmericanHeartAssociationGuidelinesforCardiopulmonaryResuscitationandEmergencyCardiovascularCare.Circulation.2010;122(18Suppl3):S729–S767.
2. SampsonK&KassR.Anti-ArrhytmicDrugs:Introduction.12th.ed.Goodman&Gilman’sthePharmacologicalBasisofTherapeutics2011.McGraw-Hill:NewYork.
3. KoweyP&YanG.AntiarrhythmicDrugs.13th.ed.Hurst’stheHeart2011.McGraw-Hill:NewYork.
4. GauscheM,PersseDE,SugarmanT,etal.,Adenosinefortheprehospi-taltreatmentofparoxysmalsupraventriculartachycardia.AnnEmergMed.1994;24(2):183–189.
5. RiccardiA,ArboscelloE,GhinattiM,etal.Adenosineinthetreatmentofsupra-ventriculartachycardia:5yearsofexperience(2002-2006).AmJEmergMed.2008;26(8):879–882.
6. BurkhartKK.Respiratoryfailurefollowingadenosineadministration.AmJEmergMed.1993;11(3):249–250.
7. ChristopherM,KeyCB,PersseDE.Refractoryasystoleanddeathfollowingtheprehospitaladministrationofadenosine.PrehospEmergCare.2000;4(2):196–198.
8. ReedR,FalkJL&O’BrienJ.Untowardreactiontoadenosinetherapyforsupra-ventriculartachycardia.AmJEmergMed.1991;9(6):566–570.
9. WebsterDP&DaarAA.ProlongedbradyasystoleandseizuresfollowingIVade-nosineforsupraventriculartachycardia.AmJEmergMed.1993;11(2):192–4.
10. MalletML.Proarrhythmiceffectsofadenosine:Areviewoftheliterature.EmergMedJ.2004;21(4):408–410.
11. ExnerDV,MuzykaT,&GillisAM.ProarrhythmiainpatientswiththeWolff-Par-kinson-Whitesyndromeafterstandarddosesofintravenousadenosine.AnnIntMed.1995;122(5):351–352.
12. HaynesBE.Twodeathsafterprehospitaluseofadenosine.JEmergMed.2001;21(2):151–154.
13. ShahCP,GuptaAK,ThakurRK,etal.Adenosine-inducedventricularfibrillation.IndianHeartJournal,2001;53(2):208–210.
14. DelacretazE.Clinicalpractice.Supraventriculartachycardia.NewEngJMed.2006;354(10):1039–1051.
15. DiMarcoJP,MilesW,AkhtarM,etal.Adenosineforparoxysmalsupraventriculartachycardia:doserangingandcomparisonwithverapamil.Assessmentinpla-cebo-controlled,multicentertrials.TheAdenosineforPSVTStudyGroup.AnnIntMed.1990;113(2):104–110.
16. MarillKA,WolframS,DesouzaIS,etal.,Adenosineforwide-complextachycar-dia:Efficacyandsafety.CritCareMed.2009;37(9):2512–2518.
17. SlovisCM,KundencheckPJ,WayneMA,etal.,Prehospitalmanagementofacutetachyarrhythmias.PrehospEmergCare.2003;7(1):2–12.
18. WeismullerP,KattenbeckK,HeinrothKM,etal.[Terminatingsupraventriculartachycardiawithadenosine--comparingtheeffectivenessof12mgand18mg].DtschMedWochenschr.2000;125(33):961–969.
Read a clinical education article about heart rhythms at www.jems.com/article/monitors-
recorders-vital-signs/rhythm-clues
choose 36 at www.jems.com/rs
040_045Adenosine.indd 45 8/15/2012 10:29:13 AM

46 JEMS SEPTEMBER 2012
The smoky plume had relentlessly grown with vehemence during the previous five days—culminating in
a 65 mile-per-hour-wind-driven fire storm that had consumed 346 homes and taken two lives in less than just an hour one day earlier. My mountain community lies just 10 miles west of the Colorado Springs dev-astation, and although we shared with our front-range neighbors the collective loss of property, life and scenic beauty, I admit I felt a sense of selfish relief and guilt that the winds had chosen an easterly path away from my domesticated habitat.
Still, the fire was 0% contained while
being sporadically fanned by wind patterns the likes no one had ever seen before. And there was still a psychopathic pyromaniac on the loose in our county. Add to that an unprecedented 100-plus degree tempera-ture, single-digit humidity and no precipi-tation in the foreseeable future. Many of us believed, in spite of the awe-inspiring quan-tity of firefighting resources being brought to bear, these merciless flames might very well circumvent their way back up the can-yon and valley to consume the foundation of Pikes Peak’s purple mountain majesties. I believed our pre-evacuation orders would no longer include the prefix “pre.”
Now I’m not one to say, “I told you so” (ha!), but for years our highland region had been suffering from a brutal drought. “It’s just a matter of time,” I would inces-santly preach to any ears that were open to my dire warning (of which receptive auricles belonged only to my dog).
Seeing what medics see in EMS affords us the opportunity to integrate the belief system of, “Of course things can always get worse, and, by God, I want to be there when it happens!” The advantage of this seemingly moronic perspective is that it forces EMS providers to believe there’s a solution to any problem regardless of the
EMS providEr bEcoMES patiEnt>> by steve berry
046_050LighterSideredo.indd 46 8/15/2012 10:31:18 AM

www.jems.com sePTemBeR 2012 JEMS 47
probability of a successful outcome. Why else would we want to be there? Simply put, we believe in being hopelessly hopeful.
It is this form of logic that enabled me to endure my neighbor’s ridicule (during the past 20 years) of my efforts to create a fire-free zone around my property. He would watch me diligently work my land as I cleared the forest floor of its dead wood and needles while thinning the pine trees, thus allowing them more personal space to branch out. “What’s the point?” my neighbor would stoically ask. “If a fire rages through here, all will be lost, you silly lumberjack-wanna-be.”
Obviously my neighbor never heard of fire TRIAGE (Trees Readily Ignite Archi-tecturally Grown Entanglements). Just as in EMS, wildland firefighters have triage tags. The black tag for them symbolizes death of a structure by blackened charred embers, and without adequate fire mitigation around one’s home, an owner might as well TRIAGE (Try Running Imme-diately Away Grudgingly East). Firefighters will not take a stand to save such acreage, especially if there’s fuel lying near or above the residence.
This is why just one day after so many homes were lost in Colorado Springs, I was determined to eliminate the last remaining low-lying branch menacingly clawing its way toward my house. But when I say low-lying branch, this particular abominable limb hovered well over 20 feet above the ground. Her ten-tacle branchioles (capillary branches) spread ominously toward the gutters of my second story. She had to come down, and it was to be my last act of fire mitigation should the final order to evacuate come down.
For the record, I will arrogantly admit that I wasn’t too concerned about the task at hand. I considered myself quite handy with a chain saw and axe after having
resided in these thar woods all these years. When December clouds annually shroud our home’s passive solar heating system—no problem. We had wood. The fragrant smoke from the chimney billowed in car-cinogenic testimony to my ability to cut, haul and split wood. “I am a lumberjack! Arrrrgh!” (OK, so I’m a pirate lumberjack.)
With the surface area now secured, the metal clips began to clatter their way up past each step with each pull of the rope. Each subsequent clank would represent an addi-tional foot of separation of me from the earth’s surface. By the sixth clank, I realized I would be lucky if the extension ladder could even reach the base of the tree limb. No matter. My fully extended body and 20" chain saw guide bar would more than
make up for the gap in distance. Cumber-some? Yes. But I’d done it thousand times before without incident. No harm, no foul, right? Riiiiiight.
Copious amounts of sawdust rained down on my head as the guide bar sliced easily through the tree limb like a hot knife through butter. I applauded myself for my foresight in replacing the dull chain with a new one to reduce arm fatigue from hav-ing to hold a 35-pound chain saw above
my head. Take a back seat Paul Bunyan, for I am the master. Blinded by the showering confetti of wood particles, I suddenly heard a crack. Not a little crack, mind you, but a loud, whopping pre-emptive, oh-crap crack!
It’s wise to constantly monitor one’s progress while cutting down timber. The tree will talk to you as the grain is objec-tively being weakened. It’s considered stan-dard practice to give pause and reassess the act of cutting before the wood is completely severed from its rooted ties to itself. But I had cut too deep, too rapidly, and the goggles I had negligently left on the ground wouldn’t provide me the visual acuity neces-sary to foresee the misdirection this gigan-tic sap-laden pendulum was about to take
toward my delicate frame. It’s kind of funny what goes
through one’s mind when some-thing irrevocably bad is about to unhinge your gravitational homeo-stasis. For me, I was thinking of Looney Toons, the Road Runner’s nemesis—Wile E. Coyote. He was, after all, the master of the whistling astrophysical plummet routine, and I’m pretty sure I had his exact same resigned, deadpan expression as the reality of the situation sank into me … literally.
But unlike Wile E., whose scripted character is supposed to be more humiliated than harmed by his failures, I began to contemplate all the potential prospects in store for my fragile anatomical parts as the partially avulsed limb venge-
fully eradicated me like an annoying tick from its main body. For I knew it wasn’t the falling that was going to hurt, but the land-ing that was going to be a bitch.
It’s true what they say: Time stands still at moments like these (sans bladder). Here are just a few of my thoughts as I began my reentry into the atmosphere:
1. This is going to hurt. 2. When was my last BM (breath mint)? 3. Is that squirrel laughing at me?
046_050LighterSideredo.indd 47 8/15/2012 10:31:31 AM

48 JEMS SEPTEMBER 2012
GOING OUT ON A LIMB >> continued from page 47
4. This is going to hurt. 5. What EMS shift is on today, and did
I piss off any of the crew members responding recently?
6. This is embarrassing. I hope no one is watching this. No. Wait. I’m unaided. I hope somebody is watching this.
7. Where is the chain saw? 8. This is going to hurt. 9. Think like a cat. Land like a cat. Think
like a cat. Land like a cat.10. Look! A butterfly! (ADD still intact).11. This is going to … Arrrrrrrrrrrrgh!Hmmmmmm. Interesting. No loss of
consciousness, I think, but (gasp) I can’t catch my breath. Take in a lungful. Yah, nope! That ain’t happening. How am I lying? Left lateral recumbent, which explains the left-sided thoracic pain. I note lateral neck tightness as I attempt to survey myself for external bleed-ing. Sweet! No blood anywhere. What did I land on? Phew! Just missed that severed aspen tree spike. No ground, roots-only, soft needle-laden soil. The chain saw is still running, but where is it? Still no signs of mid-line C-spine point tenderness to palp. Feeling for a strong radial pulse. Ouch! Left wrist slightly deformed. At least I’m right handed. Where did that butter-fly go? Why am I tachycardic? Am I hemorrhaging internally? Could be a spleen from landing on my left side. No, wait. Of course you’re tachycardic you epi-rush-dumb-ass. Why else would your hands be trembling? Besides, the peripheral skin is pink, warm and dry with good capil-lary refill. No abdominal pain. How are the legs? WTF? That doesn’t feel right. Hip frac-ture possibly, but on the right side? Coup contrecoup maybe? Please don’t let it be the pelvis. Cell phone! Where’s my cell phone?
“9-1-1. What is your emergency?” “I fell out of a tree.”“Who fell out of a tree?” “I fell out of a tree.” “What tree?” “My tree.” “You fell out of your tree?” “Yes, my tree!” “Which tree is it?” “The tree I am under!”
I’m sure there was a lot more pertinent dialogue to the conversation with the 9-1-1 operator, but I don’t recall a lot of the details, except for a few shining moments—espe-cially when the dispatcher asked me to please hold. Please hold? Seriously?
Time may have stood still for me during my nosedive into the abyss, but for the Ute Pass Regional Ambulance District (UPRAD) EMS providers who would respond to me on this day, my timing couldn’t have been worse. During the exact moment of my reckless act, an already taxed UPRAD was preparing for the immediate fire evacuation of the town’s chronically sick and immobile citizens by either recruited buses or ambu-lances. On top of that, a rollover accident with multiple patients being ejected was
concurrently being dispatched, along with my call. Thus, through no fault of her own, the 9-1-1 dispatcher had to put me on hold while she valiantly attempted to bring all the available resources to bear amid the chaos.
Still on hold, and having already com-pleted my initial primary survey, I began to contemplate a more thorough self-exam, upon which I discovered not only my health insurance card, but also a Subway sandwich gift card that still had five dollars worth of credit on it. Suddenly, I saw my loyal dog Koosko sitting just above me on the slope. “Lassie,” I bemoaned through my aching thorax. “Go get help girl! Find help.” I was delighted and surprised to see Koosko, sens-ing my situation, take off like a bolt of light-ning toward the road. I closed my eyes in
quiet satisfaction, knowing help was on the way. Minutes later, I felt a light, hollow thud hit my chest, followed by heavy panting. My dog had returned to his master. Not with help mind you, but with his saliva-soaked tennis ball.
Resigned to the fact that it is what it is and that it may take a while before 9-1-1 gets back with me, I feebly lobbed the ball maybe five feet down the hill. Like a good dog, he fetched and returned the ball each time I threw it, despite his obvious air of discontent with my less-than-stellar effort.
As I lay quietly under the tree, despite the continuous, soothing idling rumble of the chain saw’s engine, my mind was far from quiet. I was now scared. Any thread of arrogance that embodied my earlier inter-
pretation of myself was now gone. I knew my body was not that of a young man anymore and that my brain could only mobilize just so many neurons when it came to interpreting any damage. I knew there could possibly be more under-lying issues my endorphins were masking at the moment, despite my stable vital signs. Still, I was hopeful my injuries were limited to muscu-loskeletal in nature as my faithful dog continued to drop his slimy orb on my contused chest.
I didn’t hear the sirens while I continued to reassess my C-spine in a half sit-up position, but I did hear a voice yelling, “EMS.” Moments later, the feel of gloved latex firmly fixating itself bi-laterally along my
temporal lobes was simultaneously met by an upside down, sun-blinded view of para-medic Chris Erickson saying, “Don’t move, Steve!” His voice was both commanding and compassionate; his facial expression read “What the hell were you thinking?”
“I’ve cleared my C-spine,” I began but was quickly cut off.
“You know the drill,” Chris said.“But I …” I heard, “Shut up, Berry!” as the non-
rebreather mask was instantaneously placed over my nose and mouth as if to emphasize the point. And with that, I can honestly say I let go. I let go of the control and put all my trust into my prehospital care providers—my comrades, my brothers, my stupid dog. Chris is one of the best paramedics I’ve ever
046_050LighterSideredo.indd 48 8/15/2012 10:31:33 AM

www.jems.com sePTemBeR 2012 JEMS 49
had the pleasure of knowing, and his EMT partner Travis Daniels, although new to the field of EMS, has more street sense than most medics I’ve known.
“Launch the bird,” Chris tersely ordered. “Damn! Really?” I contested. Again, I was cut off, not by his voice, but
by his charismatic furrowed eyebrows. “He’s one of ours,” Chris emphatically
told the Northeast Teller County firefighters arriving on scene. He wanted a helicopter, and he wanted it now.
Once the C-collar was applied, my view of the world became stiflingly one dimensional ,with occasional faces, arms, hands, splints, stethoscopes, a blood pressure cuff, straps and tennis ball making brief and sporadic appearances across my 20" by 20" transversal viewing plane.
I knew the pinch (ouch!) on my forearm indicated pain management was forthcom-ing, but instead a second pinch in the same general vicinity soon followed.
“Chris? Oh, Chriiiis? Did you just hap-pen to miss the line on your first attempt?” I
satirically inquired in a falsetto voice. “You moved,” he voiced meekly. I couldn’t
help but laugh, despite my unsolicited situa-tion, for three reasons. One: I had ropes for veins without a tourniquet. Two: Chris is a master at venous access. Three: He used the ole pathetic, “You moved” line.
“This was almost all worth it just to wit-ness this implausible moment,” I continued in my attempt to rib him just as my ribs were ribbing me.
“No matter,” he grinned. “You won’t remember this short-term memory moment anyway.” And with that, I was given a fluid challenge of 100 mcg of fentanyl, soon fol-lowed by 2 mg of Versed.
Chris was right about my inability to recall much of what transpired following my IV inoculation of happy meds. Brief moments of EMS procedural applications, well wishes, sounds of sirens and rotor blades, along with loading and unloading from ground to ambulance, ambulance to helicopter and helicopter to hospital helipad felt like only minutes rather than the hour it probably
required to transport me from scene to ED. Nonetheless, there were some moments of clarity that I know can only enhance my patient care and compassion in the future:
Pay attention to the mechanics of trauma tri-age. Chris quickly understood the risk for injury from such a vertical deceleration sce-nario, including the assessment of height, impact surface area, body orientation, age of patient, circumstances of fall, secondary collisions and anticipated weight distribu-tion. I was very lucky to still be among the living, and Chris stayed the course despite my paramedic-induced martyred invincibility.
Introduce your face often to spinal immobilized patients and explain all procedures that are about to or are being performed outside their visual periph-ery. And keep patients posted often as to their current geographic locality during transport.
Provide your patient updates often as to what you suspect isn’t anatomically correct, but also tell them what’s functioning correctly.
A reassuring touch speaks volumes. Although my EMS peers joked with me often during my ordeal, Chris and Travis made it clear they
2013 CALL FOR NOMINATIONSThe James O. Page/ JEMS Leadership Award, sponsored by Elsevier Public Safety, encourages EMS personnel and EMS agencies to deliver quality service, gain the respect of their colleagues in the fi eld of EMS, and fi ght to do what’s in the best interest of patient care and EMS in their community. It recognizes an individual (or organization) who exhibits the drive and tenacious effort to resolve important EMS issues or bring about positive change in an EMS system, often at great personal or professional sacrifi ce.
Eligibility: This award is open to an individual OR an agency who has championed a cause or righted an EMS wrong. Past winners are not eligible to participate.
DEADLINE FOR SUBMISSION: DEC. 30, 2012
For detailed award & submission information, go to: www.jems.com/JOP2013
046_050LighterSideredo.indd 49 8/15/2012 10:33:33 AM

50 JEMS SEPTEMBER 2012
GOING OUT ON A LIMB >> continued from page 49
cared deeply about my well-being by simply gripping my hand occasionally.
Be polite. Repeatedly incorporate the words please, thank you and I’m sorry as part of your patient dialogue.
Never throw the tennis ball farther than that of the disabled pet’s owner current ability, lest the dog turn traitor to a different master.
I also took a lesson on humility that I hope to incorporate into my line of work. I broke many safety rules the day of my fall from sapling grace. I knew better, and yet I cut cor-ners and made a conscious decision to take on a substantial and unjustifiable risk. Did my years of experience carving up wooded landscapes allow me more latitude to drift, simply because nothing bad had happened years earlier? Maybe there’s a tendency to ignore or miss the warnings that don’t con-form to what’s actually familiar. It’s easy to draw the line after the accident, but you don’t have to be in one to become a victim.
There’s a reason airline pilots follow a detailed, by-the-numbers transcript of pre-flight safety procedures that they check off
each time they climb into the cockpit, regard-less of their years of winged experience. I plan on being more diligent in regard to the check-off list of EMS preventable foresee-ables. Events will line up a certain way despite the best intentions to prevent a problem, but eventually something will go wrong. Let’s not add to that probability by drifting simply because we’re currently in a safe place.
Shortly after my (insistent) discharge from the hospital (sorry floor nurses, but your venous access technique really sucked), I had the opportunity to attend the Woodland Park community post-Fourth of July Symphony in the Park celebration—an annual event our family has never missed since the birth of our children. The com-munity had a special reason to celebrate this year as our town was just days ear-lier spared the ravages of the Waldo Can-yon fire. Although the annual fireworks were obviously prohibited, the symphonic orchestra instead introduced our local fire-fighters to the stage. A well-deserved, five-minute standing ovation ensued.
As I struggled to stand with my acutely recuperating fractured forearm, wrist, ribs, sacrum, pelvis and various other leaking appendages, I noted the UPRAD ambulance and its crew standing by for the event far off stage, just up the ridge. My applause made no sound as I attempted to clap with my casted forearm in their direction—a fitting silent tribute that I suppose EMS has always unfairly had to shoulder since its true begin-nings. Standing in the shadows, these crews provided fire rehabilitation and evacuated the local hospital of its residents along with countless other sick and bedridden patients. Through all this, they still had to be there for the 9-1-1 call I needed on that day. Thank you EMS, from a grateful patient and his golden retriever. Oh, look! A butterfly!
Until next time, be safe … and this time I really do mean it. JEMS
Steve Berry is an active paramedic with Southwest Teller County EMS in Colorado. He’s the author of the cartoon book series I’m Not An Ambulance Driver. Visit his website at www.iamnotanambulancedriver.com to purchase his books or CDs.
046_050LighterSideredo.indd 50 8/15/2012 10:33:34 AM

did you Miss a live webcast? Check out the archives at www.JEMS.com/webcasts. • May the G-Force Be With You
• ‘Posting’ Is Not a Dirty Word
• When You Leave a Patient Behind: Refusals, Non-Transports & Best Practices for Documentation
• Top 5 Ways an In-Vehicle Router Improves EMS Operations & Patient Care
• CPR Quality Improves Survival
• Breathe Deeply: How CPAP and Ventilation Can Help Your Patients
• Simulating Work: How to Effectively Incorporate Simulation into Prehospital Care
• CPAP: Filling The Sails to Respiratory Relief
• Securing the Airway: The expanding role of extraglottic devices
• Maximizing Your Revenue
• The Mobile Transformation
• EMS Strategies for Improving Cardiac Arrest Survival
• Are You Bagging the Life Out of Your Patients?
• Drug Shortage Action Plans for EMS
• Statewide Trauma System Enables Multi-Agency Coordination with Trauma Centers to Improve Patient Outcomes
• CPAP in EMS: The Standard of Care Argument
With content from writers who are EMS professionals in the field, JEMS provides the information you need on clinical issues, products and trends.
Available in print or digital editions!
Giving you the detailed product information you need, when you need it. We collect all the information from manufacturers and put it in one place, so it’s easy for you to find and easy for you to read. Go to www.jems.com/ems-products
Your online connection to the EMS world, jems.com gives you information on:
• Products• Jobs• Patient Care• Training• Technology
Sign up now for the weekly JEMS.com eNewsletter. Get breaking news, articles and product information sent right to your computer. Read it on your time and stay ahead of the latest news!
jems.com eNewsletter Product Connect
jems.com Websitejems, journal of emergency medical services
Go to www.jems.com
Comprehensive, Credible, Educational...
JEMS Products Help You Save Lives.
Go to jems.com/webcasts to register.
FRee WeBCAsTs
JEMSFamilyofProducs Sept2012_FP.indd 1 8/16/2012 9:37:31 AM

52 JEMS SEPTEMBER 2012
In the government sector, there’s a con-cept known as “the plenary police power of the state.” This means that the state has the
authority to do things to generally protect the well-being, and health and safety, of its citizens.
One of the ways states use this is through the enactment of laws and regulations. The “police power standard,” as seen in licensing statutes and rules, is “the minimum level of knowledge and skill needed so that the regulated profession doesn’t constitute a threat to public health and safety.” It’s a floor. It’s a minimum standard. In the academic sense, it’s a grade C- (or 1.7 on a 4.0 scale).
Unfortunately, in the world of EMS, these minimum standards often turn into a maximum, or a ceiling, once they leave the state capitol. If the minimum number of hours for a paramedic course is set at 1,000 hours, then paramedic programs at educational institutions often get a budget for 1,000 hours and not a minute more.* Therefore, the floor becomes the ceiling. So take a 1.7 standard, graduate a 1.7 student, you’ve got a 1.0 new licensee. Is that person really ready to staff your ambulance? Do you want that person showing up at your house when a loved one is critically sick or injured? Probably not. If you’re a responsible EMS agency leader, you’re aware of this gap and understand that your agency must do something about it.
>> by Skip kirkwood, MS, Jd, NrEMT-p, EFo, CEMSo
EnhancE EMS prEparation uSing thE fiEld training & Evaluation prograM ModEl
pho
To a
lEN
go
/iST
oC
kph
oTo
.Co
M
052_053fieldtraining.indd 52 8/15/2012 10:39:05 AM

www.jems.com sePTemBeR 2012 JEMS 53
*Author’s Note: Throughout this article, we use the term “paramedic” to mean any level of EMS provider who responds to emergency calls and provides medical care and/or ambulance transpor-tation. This use is consistent throughout National EMS Management Association (NEMSMA) publications, with our colleagues in Canada and with the International Paramedic movement.
Filling the gapSo what should we do to fill the gap between the knowledge, skills and effective traits that EMS providers have when they first arrive, and those we’d want them to have when they staff a unit in service on their first shift?
Does your organization approach this question in a manner that will help the new employee? Do you teach the needed (and missing) knowledge, skills and behaviors necessary to protect the provider and your organization, and help to ensure compas-sionate, clinically excellent care for the patients being served?
This problem is not new or unique to EMS. The law enforcement community, which is driven much more by litigation, began to confront this same issue in the mid-1960s, when societal demands on law enforcement began to change, workforce challenges surfaced and community expec-tations increased.
What had been a casual, mostly on-the-job training environment needed to change. The law enforcement community took a close look at their training and operational prac-tices and made the following observations:
1. If you don’t adequately train new employees, bad things happen.
2. If bad things happen, you get sued.3. If you fire people who want their jobs,
you get sued.They adopted a system: the Field Train-
ing and Evaluation Program (FTEP), which originated in 1976 in San Jose, Calif., and spread throughout the U.S. It’s now required for police officer certification in many states and agencies.
The “Bible” of the FTEP program is the book The Field Training Concept in Criminal Justice Agencies, by Glen Kaminsky, which states that an FTEP requires the following:
>> An identified set of competencies that a new police officer must be able to perform before being released for inde-pendent duties;
>> A reliable and valid process by which the new police officer is coached, taught and evaluated;
>> Standardized documentation of per-
formance and progress, using valid and reliable tools; and
>> Formally trained field training officers, supervised by a hierarchy that is prop-erly trained and understands and sup-ports FTEP within the agency.
Is there anything in this list of require-ments that isn’t applicable to an EMS agency?
approaching the ‘gap’EMS agencies have several approaches to training new employees. One way of think-ing, often expounded by EMS managers, is , “They have a state license, so they have been taught what they need to know.” Agencies with this attitude give them the keys to an ambulance, or just a small orientation, and send them out on a rig.
Another line often heard is, “We’re not sure what they know, so we assign them with an experienced medic to teach them the ropes.” The problem with this approach is that most of those folks have not received any formal training in how to teach, evalu-ate or perform employee development.
Finally, the last common way of thinking is, “We need to be sure that they know cer-tain things, so we’ll give them an orientation manual and let their preceptor work through it with them.” This approach assumes that what new employees are lacking is psycho-motor skills, which may be part—but only part—of the problem.
None of these approaches is sufficient. If you use an “on the job training” process for making employment determinations, that is a “test” pursuant to EEOC guidelines. So it must be a valid and reliable test. If not, it has an “adverse impact” on anyone, substantial liability could result.
Some agencies have what they call a field training officer (FTO) program, although many of those programs lack the essential elements of a valid, reliable program. If you ask the medics, “Can you identify the hard FTOs and the easy FTOs?” If even one says “yes”, your system isn’t reliable because it doesn’t have a universal, identifiable stan-dard for passing or failing the process.
introducing eMS-FtepIn the mid-1990s, a number of EMS leaders discovered the law enforcement FTEP pro-gram During the intervening years, several EMS agencies built an EMS version of FTEP.
Discussion among NEMSMA members revealed a perception that “the gap” was not only a real issue, but also an issue that was widening. So in 2009, multiple agencies came
together to take the fledgling EMS-FTEP pro-gram and make it standardized and available throughout the EMS community.
EMS-FTEP consists of two educational programs, the first of which is “Develop-ing and Managing the Emergency Medical Services Field Training and Evaluation Pro-gram.” This program is directed at senior EMS executives and chief officers, training chiefs and other middle managers.
This 24-hour management program requires 2–2.5 days of instruction and edu-cates participants on the need and basis for quality, essential elements (standardized evaluation guidelines, daily observation reports and the recruit training manual) and how to develop them. It outlines how to select, train and supervise EMS FTOs; the legal aspects of EMS-FTEP; and the role of supervisors, managers and executives in ensuring the success of the program.
The second program is the “Basic EMS FTO Course.” This course is designed for EMS personnel who are destined to serve as FTOs in their EMS agencies and for first-line supervisors who will have daily oversight of FTOs and their medics-in-training.
It lasts 3.5 days and includes the essentials of teaching, coaching and remedial train-ing strategies, how to work with employees from different gen-erations, use of EMS-FTEP tools, paramedic/trainee/patient safety, provision of feedback, documentation of performance, and ethical and legal issues involved in field training.
The third FTO component, currently in development, is an FTO program accredita-tion process. EMS agencies that develop and operate field training programs meeting NEMSMA’s EMS-FTEP program standards will be recognized as meeting EMS-FTEP accreditation standards.
Wrapping it upResponsible EMS agencies must identify what’s missing in the gap and take steps to fill in that gap. NEMSMA’s EMS-FTEP program will help agencies develop, imple-ment and evaluate a sound, legally defensi-ble program that will make sure employees are ready when they “hit the street” to pro-vide service to their community. JEMS
Skip Kirkwood, MS, JD, EMT-P, EFO, CMO, is the chief
of the Wake County (N.C.) EMS Division and the current
president of the National EMS Management Association.
Contact him via e-mail at [email protected].
For more information, visit www.nemsma.org.
052_053fieldtraining.indd 53 8/15/2012 10:40:02 AM

When you think of a mass casualty incident (MCI), you often think of a plane crash, bus accident or other incident that
thrusts a large number of victims on responders and tests the resources of an EMS system. However, multiple-patient incidents that have complicating factors occur throughout the world every day. These “MCI multipliers” tax the resources of an EMS system or inhibit the response, access or egress to a scene.
When MCI multipliers exist or occur during an incident, a small MCI can be just as challenging to manage as a large one, so it’s important that incident managers—and EMS, fire and law
enforcement personnel—recognize these factors and take them into account when developing their action plans and managing a scene that involves one or more multipliers (see Table 1, p. 56).
But if you plan ahead and recognize MCI multipliers when you encounter them, you can request any necessary additional or spe-cialized resources. You can also engage in important communi-cations with supervisors, communications centers, hospitals and regional medical resource centers to stay ahead of the chaos.
This article profiles an incident that occurred in the Los Angeles County Fire Department’s (LACoFD) service area. On Tuesday, June
54 JEMS SEPTEMBER 2012
Many factors can coMplicate an
incident of any size>> By A.J. HeigHtmAn, mPA, emt-P
1
054_057MCI.indd 54 8/15/2012 3:58:09 PM

www.jems.com sePTemBeR 2012 JEMS 55
pho
tog
raph
y r
ick
Mc
clu
re
1
2
3
2
3
The scene of a mass casualty incident can be compounded by multiple magnifying factors.
LACoFD USAR team members and firefighters shore and crib an unstable pickup truck involved in a 19-vehicle pile-up.
A patient is extricated in a coordinated operation by LACoFD, AMR and Bowers Ambulance Service personnel.
054_057MCI.indd 55 8/15/2012 3:58:20 PM

56 JEMS SEPTEMBER 2012
26, 2012, this well-drilled, high-call-volume EMS system with numerous resources and personnel was presented with a small MCI that involved several MCI multipliers.
The first multiplier was the location of the incident: a heavily traveled section of the Antelope Valley (14) Freeway that traverses a mountainous, remote area in northeast-ern Los Angeles County near Agua Dulce south of Lancaster. It’s a section of the high-way that’s notorious to responders for fre-quent accidents.
The incident involved just 17 people, two of whom were triaged as critical, but it presented situations and obstacles that made the incident commander’s work just as hard as an MCI involving 100 patients.
The IncIdenT UnfoldsThe incident started around 9:40 a.m. on the southbound side of the “14” freeway, in an area where there’s a steep, down-hill, right-hand bend on the highway. Debris that fell from an unidentified vehi-cle caused traffic to strike it, which led to a sudden backup on the freeway. A tractor trailer rig full of stone and dirt then rounded the bend at normal speed and collided with stopped vehicles.
In an instant, a chain reaction began, causing the tractor trailer and 18 other vehi-cles to pile up in what a Los Angeles Times reporter described as “bizarre roadside sculptures.” Another multiplier was traf-fic halted on the southbound side of the freeway and subsequent lane closures that caused a backup for miles. The LACoFD dispatch center initially dispatched crews
on a “traffic collision, person trapped” assignment.
That assignment sent ALS Squad 131, Engine 107, paramedic assessment Engine 81, Quint 104 and Battalion Chief (BC) 22 and an American Medical Response (AMR) ambulance. But subsequent reports and MCI multipliers soon escalated the incident to a higher-level response.
In a stroke of good luck, a Bowers Ambu-lance Service ambulance, not a normal response unit for the area, was on another assignment and happened on the crash scene within two minutes of the pileup. They reported to LACoFD dispatch that there were at least six vehicles involved and two patients trapped, one underneath a pile of vehicles (another multiplier). Another ambulance from MedResponse Ambu-lance Inc., also traveling on the freeway, also stopped at the scene and was integrated into the operation.
early command decIsIons When BC 22 Greg Hisel arrived on scene, he immediately established formal incident command (IC) from a position in the north-bound lane/center divider, where he could be easily identified and located, and had a maximum view of the incident.
Hisel says that his first observation after assessing the scene was that the big rig wasn’t able to stop in time and “ran through the stopped vehicles like a ping pong ball.”
California Highway Patrol (CHP) officers were already on scene and had shut down the No. 1 northbound lane and all south-bound lanes. The IC confirmed with the
Bowers crew and CHP officers that there were eight patients, two of whom were entrapped in a vehicle under the pile.
Hisel knew he shouldn’t delay request-ing additional resources. So he requested that two additional ambulances be sent to the scene by AMR, the contracted LACoFD ambulance provider.
Because of the tractor trailer involve-ment and the fact that multiple vehicles were mangled on top of each other, with the potential for fuel leaks and other haz-ardous materials involved (more multipli-ers), the IC requested a hazardous materials (hazmat) response. That request resulted in the dispatch of Hazmat Task Force 129 that brought Hazmat Engine 129 and a special-ized hazmat vehicle to the scene.
InITIal search & assessmenT For a more complete search and tally of involved people and patients, the IC assigned Paramedic Assessment Engine 81, commanded by Captain Frank McCar-thy, to perform a search of the scene and all involved vehicles. He also assigned Engine 81 to start triage operations and requested the closet LACoFD air squad be placed on standby.
As a standard procedure, Hisel ordered one engine to position protector hose lines and dry chemical extinguishers on both sides of the incident. Engine 107’s crew, commanded by Captain Steve Bartram, was assigned to establish a medical group.
A duty safety officer, Captain Doug LaCount, ensured that proper safety gear was in use and all safety aspects were con-sidered and managed. LaCount also doubled as the scene public information officer and briefed the media.
IncIdenT escalaTIonWhen advised by Engine 81 that 17 patients were involved, with two of them entrapped, Hisel asked dispatchers to upgrade the call to a “major” incident. This escalated the unit response to three engines, two trucks, two paramedic squads, urban search and rescue (USAR) Task Force 130 (seven per-sonnel who respond in a special tractor trailer) and Squad 130, a two-person USAR Rescue Tender. He also requested the dis-patch of a heavy rescue vehicle equipped with a crane.
As another stroke of luck, LACoFD USAR
mcI magnIfIers >> continued from page 55
Table 1: Multipliers that Affect MCIs 1. Physical location & access/egress complications. 2. Number of access points & distance between exits on a highway. 3. Location, speed & density of traffic. 4. Weather or roadway conditions. 5. Time of day. 6. Staffing levels. 7. Massive debris field. 8. Other simultaneous incidents that drain available resources. 9. Location of specialty teams & resources. 10. Ambulances unfamiliar with a district’s MCI operational procedures. 11. Ambulances from another system arriving on scene, or self-dispatching. 12. Hospital backlogs, closures or lack of resources or capabilities. 13. Communication coverage gaps or inability to communicate with mutual response resources. 14. Failure to establish incident command, divisions or groups early enough. 15. Lack of scene vests or identification of triage, treatment or transportation areas. 16. Late or improper access directions or staging instruction to incoming units. 17. Complicating factors, such as ongoing crashes, gunfire or explosions.
054_057MCI.indd 56 8/15/2012 3:58:35 PM

www.jems.com sePTemBeR 2012 JEMS 57
130, en route to a training exercise, hap-pened to be on the southbound 14 freeway and arrived on the scene rapidly. They went to work immediately, cribbing and shoring vehicles with air shores and other stabili-zation equipment not normally carried on ladder companies, quints or engines. Quint 104, led by Captain Chad Hunter, was desig-nated as the extrication group, and oversaw the extrication of both patients in conjunc-tion with the USAR team.
When AMR supervisor David Ellis arrived on scene, he was assigned the role of transportation coordinator and immedi-ately requested five additional ambulances. With the southbound side of the freeway completely shut down, the IC and CHP com-mand officer approved several northbound units to have access the scene via the south-bound lanes (another multiplier).
Access was difficult because of the road closure, so Ellis requested five additional ambulances from the Santa Clarita area because he knew access from that direction would be more efficient.
Ellis had to have incoming units, approaching from both directions, stage in separate areas, with non-transport LACoFD ALS and USAR squad units positioned in a separate area. The first-arriving ALS squad (131) was assigned to established contact with the LA County Medical Alert Center to provide a scene report, alert local hospitals of the incident and request bed availability.
Triage & TreaTmenTMost of the injured were walking wounded victims who extricated themselves and walked up to the established triage area located along the shade side of the high-way along the face of a cliff. This can be another multiplier: EMT/firefighters were initially confronted with five to seven walk-ing wounded and Priority 3 patients com-plaining of neck and back pain. In the initial stages of triage, the EMTs applied C-collars and positioned patients in a safe patient col-lection area on the shady side of the highway until triage was completed and additional treatment personnel arrived on scene.
Once assessed, the patients deemed to be in need of complete immobilization were fully immobilized and moved in pri-ority order to ambulances by the trans-portation coordinator. The Medical Alert Center assisted the transportation group
supervisor via his assigned radio offi-cer (from ALS Squad 131) in assign-ing patient to the most appropriate hospital and ensuring an even distri-bution of patients. Because the size of the incident was within the scope of normal operations for the crews on the scene, triage tags weren’t used. Instead, the crews used their regular EMS reports, which feature a special section on the back of each report for multiple-patient incidents.
The patients at this incident were all triaged, treated and transported from the scene in less than an hour despite the geographic and physical obstacles presented by the remote area of the highway. They were evenly distrib-uted to four area hospitals: Antelope Valley Hospital in Lancaster, Palmdale Regional Medical Center in Palmdale, Henry Mayo Newhall Memorial Hos-pital in Newhall and Providence Holy Cross Medical Center in Mission Hills.
Lessons LearnedAs with any incident of this nature, crews debriefed and conducted an “after action” review. Some of the key lessons learned include the following:
1. The benefits of joint training with contracted and mutual aid ambulance services and their familiarity of critical MCI operational and command practices;
2. The importance of early search and rescue process and designation/use of a safety officer;
3. The benefits of joint command and use of frequent, concise scene reports;
4. The need to request extra resources and specialized teams early;
5. The importance of knowing the dis-tance to nearby exits/access points;
6. Presentation of vehicle access, approach and staging information to units, particularly when major traffic backups or blocked roadways are involved;
7. The need to use tarps or flags to iden-tify the location of the triage and treat-ment areas for walking wounded and rescuers bringing supplies or patients to them;
8. The potential need to dispatch a
tanker or water tender in the event a significant water supply is needed in a remote area;
9. The benefit of dispatching heavy res-cue and/or USAR resources early into an incident to capitalize on their technical skills, specialized tools and shoring supplies; and
10. The need to deploy scene ID vests whenever a scene escalates or mutual aid resources are involved, so com-mand responsibilities are clearly visible and crews can identify key personnel and their locations. JEMS
A.J. Heightman, MPA, EMT-P, is the JEMS editor-in-chief
and has a background as an EMS director and EMS opera-
tions director. He specializes in MCI management. Contact
him at [email protected].
4The truck driver, initially reported as having experienced a period of uncon-sciousness, was extricated from the cab of his vehicle by LACoFD and AMR personnel.
Providers place C-collars and prevent unnec-essary movement for walking wounded.
5
6
It’s beneficial to have separate staging areas for transport ambulances and non-transport units at the scene of a major incident.
054_057MCI.indd 57 8/15/2012 3:58:43 PM

58 jems SEPTEMBER 2012
Q: Why should We change the Way We do things?A: Sudden cardiac arrest (SCA) continues to needlessly kill too many people. If you col-lapse tomorrow without a pulse in down-town Seattle, you have about a 50/50 chance of walking out of the hospital with a func-tioning brain. But if you were to collapse in Detroit instead, your chances of survival would be less than 1%. That’s a difference of over 40 times, and we’d never accept such a survival disparity for other diseases. In fact, if anything else caused that many prevent-able deaths in our community, there would be an uproar.
Granted, some people simply aren’t going to survive after sudden out-of-hospital car-diac arrest. But when we compare num-bers, we’re usually looking at witnessed arrests with a primarily cardiac etiology and a shockable initial rhythm. In other words, these are patients who could survive if we give them a fighting chance.
It is possible to fix the gap? Consider that Wake County, N.C., which saw around 14% of its shockable arrests survive in 2004, improved its survival to more than 40% after an aggressive initiative to strengthen their resuscitation infrastructure. That could be you.
Q: i Want numbers like that in my community. What’s the secret?A: Unfortunately, if we’ve learned any-thing yet after 60-plus years of resuscitation
research, it’s that there’s no secret. The old model of a “cardiac chain of survival” keeps proving true. Good outcomes depend on an interlocking sequence of events happen-ing rapidly and effectively. If even one link is weak or missing, you can’t make up for it elsewhere. There are no silver bullets or quick fixes; a comprehensive system built on a solid foundation is essential.
Q: this doesn’t sound neW at all. What has changed?A: It’s not new. If anything is new, it’s our understanding of what’s truly necessary and what can be deemphasized. It’s clear that early and high-quality chest compres-sions save lives, as does early defibrillation, and post-arrest hypothermia. Beyond those three interventions, anything else is exper-imental at best and a distraction at worst, so the goal is now to create systems that streamline delivery of the basics.
In most cases, the weakest link in the chain—and hence the lowest-hanging fruit—is layperson intervention. Many arrests still don’t get bystander compres-sions; even fewer get pre-EMS defibrillation. The consequences are grim. Thus, the chal-lenges of resuscitation have shifted from the clinical, such as finding the ideal anti-arrhythmic medication, and toward the psychological: determining how to market CPR so people will learn it, teach it so they’ll remember it, and contextualize it so they’ll be willing to do it.
That’s why the American Heart Associ-ation (AHA) CPR recommendations have been getting simpler every five years. If streamlining the methodology means that more patients get compressions instead of nothing, that’s a definite win.
We’re realizing that when EMS provid-ers walk in and nobody’s doing CPR—even bystanders who have been certified—it’s because they were afraid of doing it wrong and being liable, concerned about catching a disease, or not confident they could cor-rectly recognize the need. We can fix those problems with smart and pointed public education, such as public safety announce-ments and simplified 20-minute CPR Any-time courses. In short, we need to mobilize the population.
On the other hand, we’re also learning that chest compressions and defibrillation aren’t “all or nothing.” You can execute them well or poorly, and the quality of that execu-tion makes a difference.
As a result, today’s ideal resuscitation is much closer to a golf swing than a math test. It’s become a physical rather than a cognitive skill. But it’s still not an easy skill, and practice is needed to succeed. EMS sys-tems that are yielding the best survival are taking the time to drill through the funda-mentals until all responders are perform-ing compressions deep and fast, with full recoil, minimal interruptions, no hyper-ventilation and seamless integration with defibrillation.
That’s the reason for the “pit crew” model many successful services have adopted, where the role of every provider is explicitly assigned and choreographed ahead of time. It’s all just another way to ensure the funda-mentals are done right.
Current goals & obstaCles in CardiaC arrest >> By Brandon oto
Brandon Oto, BA, NREMT-B, is editor of emsbasics.com and a field EMT and clinical educator who works with rescuers in numerous settings to promote best practices for resuscitation and streamline
systems of care. He discussed sudden cardiac arrest (SCA) outcomes with JEMS in advance of September’s biannual Emergency Cardiovascular Care Update Conference. In this question-and-answer session, Brandon offers his perspective on the current challenges of SCA and how folks in the trenches are confronting them.
Pho
to l
inea
rcu
rves
/ist
oc
kPh
oto
.co
m
058_059OtoQA.indd 58 8/15/2012 10:56:26 AM

www.jems.com sePTemBeR 2012 JEMS 59
Q: This sounds like a big under-Taking. Where do i sTarT?A: To address any problem with so many different facets, numerous parties must be involved. This includes government, public safety, EMS and healthcare agencies, as well as the public itself. Rarely will a system be successful without widespread buy-in.
These parties won’t come together with-out an active effort to recruit them. Since most victims of SCA don’t survive, it isn’t a high-visibility problem and public aware-ness is poor. Motivation for change requires champions to advocate for it. EMS is well positioned to shoulder that burden, along with other public safety and healthcare ser-vices. We can also benefit from the testi-mony of successfully resuscitated victims, whose good outcomes and compelling sto-ries help bring the message to life.
Most of all, it’s clear lip service isn’t enough. Everyone believes in these ideas and wants survival. But you need to put in real work and make real changes. And although it’s often difficult to get traction when most people don’t realize the prob-lem exists, things can snowball once they develop momentum.
For example, one of the great achieve-ments in Seattle wasn’t just developing strong tools for resuscitation, it was creating a culture of survival. Now, the community is proud of what they have. They believe in it. And if someone collapses, there’s an expecta-tion that someone else will intervene.
You don’t need to reinvent the wheel. Some great templates already exist, such as Medtronic Foundation’s HeartRescue pro-gram and the AHA’s HEARTSafe Commu-nities. In the HEARTSafe model, a region (usually a state) establishes criteria support-ing the chain of survival. When a commu-nity in that region meets the requirements, they can apply to their home office and receive “HEARTSafe” designation, earning the right to post a sign proclaiming that sta-tus. It’s an odd motivator and a grass-roots approach. Although the AHA supports the concept, nobody owns it, no central admin-istration exists, and it costs nothing to implement. But it’s proven internationally successful, and if your state doesn’t already have a program, many good criteria exist that can be readily adopted.
Q: ThaT covers bysTanders. WhaT should eMs agencies be doing?A: The first step is data collection. You need a reliable scorecard. If you don’t know
how well you’re doing, you can’t do much to improve. (Nor would you even realize if you had.) The more data, the better.
With hospital input, basic figures can be compiled directly from electronic patient care report systems. Or you can use a pur-pose-built, Utstein-type registry, such as the Cardiac Arrest Registry to Enhance Survival (CARES) database.
To drill down further, all major manufac-turers offer software suites allowing review of data, such as compression fraction (i.e., the total time spent on vs. off the chest), depth and ventilatory rate. This is invaluable for pinpointing where you need to focus your efforts, both as a system and as individual providers. As you implement changes, you can track the results and watch your num-bers climb.
Ironically, one of the challenges can come from the veterans in your system. Many paramedics with 10–20 years’ experience have visited so many arrests and seen so few positive outcomes that they’ve come to view working a code as mere ritual, an opportu-nity to go through the motions and perhaps practice some little-used skills, rather than a fight for survival. Highlighting the statis-tics and offering testimonies from survivors can help convince them that out-of-hospital SCA is now a treatable, survivable condition. Once they’re believers, they can become your best advocates.
Work with your fellow rescuers to estab-lish a standard flow of care, if not an actual “pit crew” model, for every arrest. This will not only ensure that everybody understands their role and what the goals are on scene, it also gets all parties on-board so that the police officer who shows up first is just as passionate about compressions and defibril-lation as the paramedics who arrive later.
In addition, remember that your receiv-ing hospitals are a key part of the puzzle. Post-arrest hypothermia is truly lifesaving, yet has still not been consistently adopted in many EDs.
EMS may help move this forward by working directly with hospital administra-tors. However, if financial constraints or general institutional inertia stand in the way, we can also apply friendly but effective pres-sure by instituting field hypothermia proto-cols (most EDs are more likely to continue ongoing cooling measures than to initiate them), or even modifying destination plans to prohibit post-arrest patients from being transported to hospitals that won’t provide therapeutic hypothermia.
Another conversation worth having involves hospital willingness to perform percutaneous coronary intervention (PCI) on post-arrest patients, or even intra-arrest patients (perhaps using a mechanical com-pression device) who have not achieved return of spontaneous circulation (ROSC). Although potentially lifesaving, many centers are reluctant to catheterize these patients due to their risk—treating such a high-mortality cohort can bring down out-come figures. Try to work out indications and contraindications with the interven-tionalists ahead of time.
Q: WhaT’s on The horizon?A: Intriguing possibilities for future inter-ventions include the administration of such IV female sex hormones as estrogen, which has shown promise for mitigating tissue damage. “Ischemic conditioning,” possibly using low-tech devices like blood pressure cuffs, may also prove to be beneficial.
Double defibrillation for refractory ven-tricular fibrillation (v fib), lipid infusions for overdoses and high-dose nitrates all might have a role for specific patient groups. And more studies are needed to refine best prac-tices for hypothermia, including the role of field induction and specific endpoints for duration, temperature and supportive care.
We may even eventually find that effec-tive hypothermia helps “bridge the gap” to neurologically intact discharge for the many therapies, such as epinephrine, that have shown early improvements in ROSC but no long-term benefits.
Better still are innovations that improve our ability to deliver BLS, such as real-time CPR feedback and metronome tools, active decompression devices or smart-phone apps that direct bystanders to avail-able AEDs.
And there’s some evidence that “hands-on CPR,” or defibrillation without taking gloved hands off the chest, may be safe and allow us to remove yet another interrup-tion to continuous compressions. (Some clinicians are already practicing this rou-tinely, with no negative incidents reported thus far.)
In the end, however, the basic picture remains the same. Improving survival from out-of-hospital cardiac arrest requires widespread improvements to the entire chain of survival. And that means making a commitment and doing the work. We can have it everywhere, but it won’t happen on its own. JEMS
058_059OtoQA.indd 59 8/15/2012 10:56:27 AM

60 jems SEPTEMBER 2012
Dealing with the 12 types of thoracic injuries
>> By Mark Cipolle, MD, phD; MiChael rhoDes, MD; & Glen Tinkoff, MD
Case study 1: You’re dispatched to a scene in which a young male has been stabbed. On arrival, you hear him screaming in pain and find him diaphoretic and dyspneic. He tells you he was stabbed with a pocket knife. The wound is in the right chest, slightly lateral and just above the nipple. He has distended neck veins, decreased breath sounds on the right chest, a systolic blood pressure of 60 and a heart rate of 130. You provide supplemental oxygen, and then you would do which of the following?
a. Perform drug-facilitated intubation;b. Place an IV;c. Perform a needle decompression of the right chest; ord. Place a chest seal over the wound.Of course, we know you selected “c” because there are few things more gratifying in trauma care
than saving a life with a needle decompression for a tension pneumothorax! You recognized that the patient was maintaining his own airway and the shock was due to inadequate venous return from the elevated pressure in his right chest. Just like other life-threatening problems after injury, putting more volume in a closed space will soon lead to disastrous consequences (e.g., tension pneumotho-rax, cardiac tamponade, brain hemorrhage and brain edema).
60_65CEthoracic.indd 60 8/15/2012 11:04:49 AM

www.jems.com sePTemBeR 2012 JEMS 61
Hospital staff performs a thoractomy on a patient where the heart is visible through the wound.
Pho
to a
da
m f
ox
60_65CEthoracic.indd 61 8/15/2012 11:04:37 AM

62 JEMS SEPTEMBER 2012
Case study 2: Shortly after complet-ing your paperwork from the stab wound patient, you’re summoned to care for an intoxicated middle-aged man who drove his car off the road, rolled over a few times and smashed into a tree. He was unrestrained. He’s complaining of severe left chest pain, and you observe abrasions, crepitus and poor chest rise with inspiration of the left chest. His BP is 120/80, HR is 110 and oxygen satu-ration (SpO2) is 85%. Which of the following would be your next step?
a. Place an IV;b. Place the patient on high-flow oxygen;c. Perform a needle decompression of the
left chest; ord. Perform rapid sequence intubation.When we answer this question, our
thought process goes something like this: The airway is intact, and circulation appears reasonable. However, there’s a problem with breathing, so the answer is “b.” The patient likely has a flail chest and may very well have a hemothorax and/or pneumothorax on that side, but vital signs are reasonable so needle decompression is not indicated. This patient will be best served by supplemental oxygen, followed by placing an IV line (“b” is before “c”) while rapidly transporting your patient to the trauma center for definitive care.
These cases are examples of two patients with life threatening thoracic trauma who have different mechanisms of injury. The patient in the first case required a rapid assessment and a decision, as well as a maneuver in the field that saved his life. The second patient required BLS intervention only.
About 25% of trauma deaths in the U.S. result from major thoracic injury.
Although most thoracic trauma is ultimately managed without an operation (up to 85%), proper prehospital management is vital in achieving a good outcome. Early recognition of severe or potentially severe thoracic inju-ries followed by rapid treatment in the field may make the difference between life and death for these patients. Several prehospital interventions are currently available—and some on the horizon—that providers may employ with the potential to reduce the mor-tality and morbidity of chest injury.
To properly treat these patients, providers should be able to recognize the “deadly dozen” thoracic injuries, understand the importance of the mechanism and location of injury and
identify the key features of a good assessment of chest injury. In addition, current monitor-ing and therapeutic options, and new moni-toring technologies are also important in the prehospital management of thoracic trauma.
the ‘deadly dozen’With such vital structures as the heart, lungs and major vascular structures residing in the
thoracic cavity, it isn’t surprising that chest injuries can be or become fatal immediately or within hours. The foundation of good trauma care, as taught in Advanced Trauma Life Support and Prehospital Trauma Life Support, is to identify and treat life-threat-ening injuries in the “golden hour.”
Other than provision of a definitive air-way and/or needle decompression of a ten-sion pneumothorax in the field, the vast majority of patients with thoracic injury will be best served by “load and go” with high-flow oxygen and placement of an IV line.
MeChanisM of injuryIt’s important to consider that the thoracic cavity not only contains the heart and lungs but also the origination of major vascular structures (e.g., the aorta, subclavian and carotid arteries). Also, running through the mediastinum along with the heart are the major aerodigestive structures, the esopha-gus, trachea and bronchi. The bottom half of the rib cage protects such major structures of the upper abdomen as the liver, spleen, stom-ach and kidneys.
In fact, the diaphragm may rise as high as the fourth intercostal space, so penetrat-ing injury in this thoracoabdominal area can injure vital organs both above and below the diaphragm. The thoracoabdominal region
learning Objectives>> Recognize the “deadly dozen” thoracic
injuries.>> Understand the importance of the
mechanism and location of injury.>> Be able to identify the key features of a
good assessment of chest injury.
Key TermsMechanisms of injury: The method or force that causes a victim’s injuries.Tension pneumothorax: Positive-pressure air or gas accumulation within the pleural cavity, compressing the lungs and limiting the ability of the heart to function.Thoracotomy: An incision into the chest cavity.Pericardial tamponade: Compression of the heart due to increased pressure within the pericardial sac due to accumulated fluid or blood.
deadly dozen>> cOnTinued frOm page 61
injuries identified in the primary survey often encountered by prehospital personnel
Airway obstruction: The airway originates in the thorax constituting the tracheo-bronchial tree, which may obstruct with blood or secretions that need to be addressed despite the presence of an endotracheal tube or surgical airway.
Flail chest: Two fractures on at least two adjacent ribs, causing instability in part of the chest wall and paradoxical breathing with the lung underlying the injured area contracting on inspiration and bulging on expiration. This results in respiratory insufficiency.
Open pneumothorax: A pneumothorax associated with a chest wall defect greater than 0.75 times the size of the trachea in which air enters preferentially through the thoracic cavity (“sucking” chest wound) and results in inadequate oxygenation and ventilation.
Massive hemothorax: Greater than 1,500 mL of blood within the pleural space of a hemothorax, causing significant compression of the lung and hemorrhagic shock.
Tension pneumothorax: Progressive build-up of air within the pleural space that pushes the mediastinum to the opposite hemithorax and obstructs venous return to the heart, leading to circulatory instability and arrest.
Cardiac tamponade: Compression of the heart that occurs when blood builds up in the pericardial sac impeding heart contractions and leading to circulatory instability and arrest.
injuries identified in the secondary survey or during hospital evaluation
Myocardial contusion Diaphragmatic tears
Traumatic aortic rupture Pulmonary contusion
Tracheal or bronchial tree injury Blast injuries
Table 1: The ‘Deadly Dozen’ Killers of Thoracic Trauma
60_65CEthoracic.indd 62 8/17/2012 12:23:48 PM

www.jems.com sePTemBeR 2012 JEMS 63
is defined as nipples to costal margins in the front and inferior border of scapula to costal margins in the back. The location of pene-trating injury is critical to provision of proper prehospital care and hospital evaluation.
It’s important to separate stab wounds from gunshot wounds. In addition, gun-shot wounds should be categorized by type, velocity, number of wounds and trajectory. For a categorization of gunshot wounds, go to jems.com/deadly-dozen.
Stab wounds should be characterized when possible by number, location, and the width and length of the blade. It’s critical to identify and accurately describe the anatomic location of stab wounds. It’s not only impor-tant to guide the work-up once the patient arrives at the trauma center, but it may deter-mine what you do in the field if a patient sud-denly deteriorates.
For example, a patient who becomes pulseless in your ambulance with a single stab wound to “the box” (a rectangle outlined by the clavicles, nipple line and costal mar-gins) will be treated differently from a patient with a chest stab wound lateral to the box. In the latter case, our working diagnosis would be a tension pneumothorax, which will be treated with a needle decompression. The first patient who has a stab wound in the box is likely dying of pericardial tamponade from a cardiac injury. This patient will be best served by “load and go” and communication of this scenario to the trauma center so they may prepare for direct operating room (OR) transport and sternotomy.
Table 2, below, describes important ana-tomic descriptors for pen-etrating trauma that may assist in facilitating diagnosis and treatment.
An important aspect of penetrating thoracic trauma is that it has the highest sur-vivability after resuscitative thoracotomy. Patients with a single penetrating injury to the chest are more likely to survive a resuscitative tho-racotomy than any other type of patient. Survivabil-ity in this scenario has been reported to be 15–35%. No other type of injury comes anywhere close to this sur-vivability (e.g., multiple
penetrating injuries or blunt injury at 1–2%). Given this, most trauma surgeons will per-form a resuscitative thoracotomy on a patient with penetrating chest trauma that had signs of life in the field and up to 15 minutes of CPR. Therefore, effective CPR and commu-nication with the trauma center would be what’s best in this scenario.
Blunt InjuryIn many ways, blunt injury is more chal-lenging to care for than penetrating injury, because it’s generally less obvious which organs are injured, and it’s often accompa-nied by more tissue injury and inflammatory response. This is especially true in civilian trauma. Other than an open pneumothorax and cardiac tamponade, the remainder of the “deadly dozen” are more common after blunt injury than penetrating injury.
Blunt injury should be described by mech-anism so the trauma team can identify key injuries as quickly as possible. See Table 3, p.
64 for these mechanisms and the potential deadly injuries associated with them.
AssessmentA good history and physical examination is essential. PHTLS recommends a SAM-PLE history (symptoms, age and allergies, medications, past history, last meal and the events surrounding the injury). The physical examination, challenging in the field, should include observation, auscultation, palpation and percussion accompanied by pulse oxim-etry. A great deal can be learned by taking a minute to perform an adequate thoracic exam with special attention to the findings described in Table 4, p. 64.
A good assessment may be challenging in the field. For instance, the classic signs of a tension pneumothorax may be difficult to identify at a chaotic scene. Cyanosis may be difficult to identify in low-light conditions, especially with blood and dirt present. Dis-tended neck veins is a classic sign but a late
Descriptor
Right vs. left
Supraclavicular
Subclavicular
Precordial (or “the box”)
Anterior chest
Lateral chest
Posterior chest
Paravertebral
Above or below nipple
Supra umbilical
Substernal
table 2: Anatomic Descriptors of Penetrating Thoracic Trauma
A patient with a knife wound to the chest that’s partially in “the box.”
Gunshot wound to the “box.”
Pho
to e
dw
ard
dic
kin
son
Pho
to a
da
m f
ox
60_65CEthoracic.indd 63 8/15/2012 11:04:14 AM

64 JEMS SEPTEMBER 2012
DeaDly Dozen >> continued from page 63
finding and won’t be present in a patient who has had substantial blood loss.
Determining whether breath sounds are diminished on one side may be difficult in a noisy environment. Practicing listening to breath sounds as much as possible will help providers to become more proficient. Percussion of the chest to detect hyperreso-nance may be challenging enough in a quiet environment and nearly impossible at a noisy scene. Tracheal deviation due to a ten-sion pneumothorax is more pronounced in the chest and is usually identified by a chest radiograph, a tool obviously not available in the field. Tracheal deviation in the neck is rarely apparent and is truly a very late sign.
Monitoring optionsAlthough prehospital monitoring is becom-ing more sophisticated all the time, EMS pro-viders shouldn’t lose sight of the basics, which include observation, palpation, auscultation
and percussion. All providers should become adept at these techniques and practice them as much as possible.
The utility of these new monitoring options in the prehospital environment is still under investigation. The focused abdom-inal ultrasound for trauma (FAST) is now an accepted and routine part of the secondary survey during hospital evaluation.
Many reports on the role of ultrasound in the prehospital setting note it can be useful in detecting pneumothoraces, hemo-thoraces, pericardial tamponade, pulmonary embolism, abdominal hemorrhage and cardiac arrest, as well as being helpful in cases of diffi-cult IV access. It has been demonstrated that para-medics can become adept at using this technology
relatively quickly. Considering this and the portability and relatively low cost of ultra-sound, we anticipate it becoming more commonplace in prehospital trauma care. Currently, it’s far more commonly employed in Europe than in the U.S.
Another technology, near-infrared spec-trometry (NIRS), is being used more com-monly in trauma and emergency medicine care to detect tissue oxygen saturation. The currently available monitor, InSpectra StO
2 from Hutchinson Technology, measures the oxygen saturation in the thenar eminence, which is the fleshy part of palm below the thumb. The InSpectra StO2 measures oxy-gen saturation in the capillary beds of these hand muscles giving the provider an esti-mate of overall tissue perfusion. Initial stud-ies in trauma patients demonstrate that levels less than 75% correlate with other measures of hemorrhagic shock, such as acidosis and the development of organ failure. This device is now available as a portable unit about the size of a small shoe.
MechanisM of injury associated injuries
Steering wheel Blunt cardiac injuryRuptured aorta
Seatbelt Blunt cardiac injuryRuptured thoracic aortaHollow viscus & retroperitoneal injuries
Crush injury Flail chestTraumatic asphyxia
Lateral impact Flail chestPneumothorax
Fall (with height when available) Ruptured thoracic aorta
Roll over and/or ejection Airway obstructionTension pneumothoraxHemothoraxMyocardial contusionFlail chestAortic rupturePulmonary contusionTracheal or bronchial injuryDiaphragm injury
Blast injury Primary (i.e., initial overpressure)Pulmonary contusionsPneumothoraxDirect lung injurysecondary (i.e., struck by shrapnel)Flail chestPneumothoraxtertiary (i.e., patient is throw or crushed)Aortic disruptionFlail chestPneumothoraxQuaternary (e.g., thermal or radiation injuries)InhalationDirect lung injury
table 3: Blunt Thoracic Trauma Mechanisms & Associated Injuries
assessMent finding
BP, Pulse, RR, loss of consciousness
Patient complaint
Lip and ear lobe color (hypoxia)
Scleral hemorrhage (crush injury)
Quality of voice
Grunting respirations
Subcutaneous crepitance (rib fracture vs. air)
Tracheal deviation (late finding)
Distended Neck veins (late finding and will not be present with significant hemorrhage) • Tension pneumothorax if decreased breath sounds • Pericardial tamponade if decreased heart sounds
Decreased breath sounds
Air vs. blood vs. abdominal organs in chest
table 4: Important Findings in the Assessment of Thoracic Trauma
seatbelt sign of the chest can be an important indicator of hidden thoracic injuries.
pho
to a
dm
fo
x
60_65CEthoracic.indd 64 8/15/2012 11:04:18 AM

www.jems.com sePTemBeR 2012 JEMS 65
Telemedicine is becoming more common-place worldwide. The ability to transport real-time data and images from the patient’s bedside to a command center manned by physicians and nurses has been available for about 10 years. It’s only a matter of time until this technology will be made routinely avail-able to prehospital providers. EMS providers can transmit not only patient data, such as vital signs, ECG and pulse oximetry, and also images that will be instantly made available to the medical control center. It stands to rea-son that the ability to share this vital informa-tion in real time with medical command will enhance care and decision making.
Although these new technologies may not drastically change care in the field, they may dramatically help the patient by ramping up the response at the hospital. For instance, if medical command is viewing ultrasound images of a pericardium full of blood in a penetrating trauma patient with a NIRS tis-sue perfusion of 50% and a systolic pressure of 90, it’s likely that patient will be directly transported to the OR for sternotomy, rather than spending precious time in the trauma bay only to have the tamponade worsen.
TherapeuTic OpTiOnsAlthough monitoring options have expanded in recent years, our therapeutic options have, for the most part, stayed “tried and true.” These therapeutic options serve a single purpose: to correct problems identi-fied in the primary and secondary survey. Some of the therapeutic options that may be employed in the prehospital care of patients with thoracic injury include:
>> A suction or oral airway device;>> Nasal oxygen;>> Bag-valve mask ventilation;>> Endotracheal intubation;>> A cricothyrotomy;
>> Needle decompression of the chest;>> Positive-end expiratory pressure (PEEP);>> Direct pressure of the hemorrhage;>> Placement of an IV;>> Splinting the chest wall;>> A lidocaine patch over a rib fracture for
prolonged transport; and>> A three-sided occulsive dressing for
“sucking” wounds.
case sTudy 3: A young man shot in the left lateral chest has an open “sucking” chest wound. He appears to be in shock with some respiratory distress with a BP of 100/60, HR 120, 90% oxygen saturation (SpO2) and diminished breath sounds on the left. It’s a long transport time, so you receive medical direction to perform drug-facilitated intuba-tion. Intubation is successful, and you then place a three-sided occlusive dressing over the “sucking” wound and establish an IV. You place a bag-valve mask with 5 cm PEEP, which improves SpO2. However, he loses his pulse while being loaded into the ambulance. What would you do next?
a. Bolus a liter of fluid;b. Increase the frequency of bagging;c. Remove the occlusive dressing; ord. Perform a pericardiocentesis. The correct answer is “c.” Importantly, one
must always remember that PEEP, either via a continuous positive airway pressure mask or via an endotracheal tube, can worsen any kind of pneumothorax, converting it to a tension pneumothorax. Although the posi-tive pressure may be helping the patient’s oxygenation, it may cause more air to enter the pleural space. Also, if a three-sided occlu-sive dressing is used on an open pneumotho-rax and the patient deteriorates, remove the dressing. In this scenario, it would be equiva-lent to a needle decompression.
summaryAlthough most thoracic trauma may be treated non-operatively, major thoracic trauma accounts for 25% of trauma deaths. Except for provision of a definitive air-way and/or relief of a tension pneumotho-rax with a needle decompression, the vast majority of thoracic trauma is best served with “load and go,” high-flow oxygen, place-ment of an IV line and administration of crystalloid solutions as the clinical scenario would indicate.
Understanding the mechanism of injury is helpful in establishing both prehospital and in-hospital management priorities. Patients who sustain a single penetrating wound to the chest have the best survivability after a resuscitative thoracotomy.
Practicing chest assessment skills is vital to being a good prehospital provider. Ultrasound, NIRS tissue oxygenation and telemedicine will likely become more com-monly employed as prehospital monitoring options. PEEP, or “over bagging,” may exac-erbate a simple or open pneumothorax, con-verting it to a tension pneumothorax. JEMS
Mark Cipolle, MD, PhD, is the medical director of the
Trauma Program at Christiana Care Health System in Wilm-
ington, Del.
Michael Rhodes, MD, is the chairman of the Depart-
ment of Surgery at Christiana Care Health System.
Glen Tinkoff, MD, is the vice chairman of the Depart-
ment of Surgery and The Medical Director of the Simulation
Center at Christiana Care Health System.
resOurces1. SalomoneJP,PonsPT,eds.ThoracicTrauma.PreHospi-
talTraumaLifeSupport,SeventhEdition.2010;291–316.2. AsensioJA,MazziniF,VuT.ThoracicInjuries.Trauma
Manual,FourthEdition.2012;Chapter28.3. BowmanJ.VisibleImprovement:Ultrasoundprovides
diagnosticimagesinprehospitalmedicine.JEMS.2010;35(9):36–47.
4. CothrenCC&MooreEE.Emergencydepartmenttho-racotomyforthecriticallyinjuredpatient:Objectives,indicationsandoutcomes.WorldJEmergSurgery.2006;1:1–7.
5. BauzaGM&PeitzmanAB.ThoracicTrauma.Inter-nationalTraumaLifeSupport,SeventhEdition.2012;108–130.
6. CohnS,NathensA,MooreF,etal.TissueOxygen-ationsaturationpredictsthedevelopmentoforgandysfunctionduringtraumaticshockresuscitation.TheJournalofTraumainjury,Infection,andCriticalCare.2007;62(1):44–55.
PRiMaRy SuRvey SeCondaRy SuRvey
Airway obstruction Myocardial contusion (rupture)
Flail chest Thoracic aortic disruption
Open pneumothorax Bronchotracheal disruption
Massive hemothorax Diaphragmatic tears
Tension pneumothorax Pulmonary contusion or hemorrhage
Cardiac tamponade Cardiac tamponade
Table 5 Survey for Thoracic Killers
a CT scan of two rib fractures on the patient’s left (right side of the image).
Ima
ge
ad
am
fo
x
60_65CEthoracic.indd 65 8/15/2012 11:04:22 AM

Get More Information at
March 5 - March 9Washington, D.C.
2013
0912-JEMS_EMST_Spread-new.indd 66 8/16/2012 2:15:42 PM

www.EMSToday.com
Advance Your Career at EMS Today … Where People, Products and Ideas Connect
0912-JEMS_EMST_Spread-new.indd 67 8/16/2012 2:15:44 PM

68 JEMS SEPTEMBER 2012 To Place a Classified ad, please email: [email protected]
HAVE OPEN POSITIONS?Get them filled with a JEMS recruitment classified.
Reach our audience with your message! Email: [email protected]
Employment
Equipment
Equipment
0912-JEMS-classifieds.indd 68 8/15/2012 3:08:18 PM

www.jems.com sePTemBeR 2012 JEMS 69
To Place a Classified ad, please email: [email protected]
HAVE OPEN POSITIONS?Get them filled with a JEMS
recruitment classified.
Reach our audience with your message!
Email: [email protected]
Equipment
LIFE SUPPORT EQUIPMENT
CERTIFICATION AND DEPOT REPAIR
CALL 1.800.383.8962
www.advancedbiomedical.com
Save 25% - All Services
ADVANCED BIO-MEDICAL
0912-JEMS-classifieds.indd 69 8/15/2012 3:08:24 PM

Exclusively for EMS Management
POWERFUL SOLUTIONSFROM SMART THINKERS
EMS Insider provides you with the “inside information” on EMS. It’s a monthly publication
from Elsevier Public Safety and affiliated with JEMS (Journal of Emergency Medical Services)
so it has the best network of sources in EMS. That means you get only the highest quality
reporting . . . insightful, timely, authoritative. . . not available elsewhere. EMS Insider pays for
itself. Every issue contains articles to help you, by bringing you money-saving and revenue-
generating ideas. Don’t miss out, order your subscription today!
*All Newsletter Subscriptions include access to content and archives from the past 15 years at www.JEMS.com.
Subscribe to EMS Insiderwww.JEMS.com or call 1.888.456.5367
avoid pending lawsuits
researchgrant
funding
EMS TrendAnalysis
EMS Research & Technology
revenuegenerating
ideasAVOIDCOSTLY FINES
0912-JEMS-classifieds.indd 70 8/15/2012 4:03:19 PM

ad directYour source for immediate information on advertisers’ products and services
Advertiser RS# Page
FREE advertiser and product informationwww.jems.com/rs
IT’SFAST,IT’SEASYANDJUSTACLICKAWAY!www.jems.com sePTemBeR 2012 JEMS 71
Advertiser RS# Page
5.11 Tactical Series 23,24 25,27
American Heart Association 29 37
BBraun 19 17
Bound Tree Medical 11 2
CentreLearn 73
Columbia Southern University 30 38
Ecolab 22 24
Emergency Medical Products/L.A. Rescue 34 42
Ferno-Washington Inc. 12 3
Hartwell Medical 35 43
JEMS 19,33,49,51,66-67
Junkin Safety Appliance Co. 31 38
Knox Co. 27 33
Laerdal Medical Corporation 38 76
LMA North America 16 9
m2 Inc. 26 33
Mercedes 18 14-15
Michigan Instruments 25 29
Moore Medical LLC 32 39
NAEMT 33 42
Oxygen Generating Systems Intl. 28 36
Philips Healthcare 13 4
Pulmodyne 15 8
Skedco Inc. 21 23
Sprint 17 11
Stryker EMS 37 75
UCLA Prehosp 50
Vidacare Corp. 20 21
Ziamatic Corp. 36 45
Zoll Medical Corporation 14 6
0912-Ad-Index.indd 71 8/15/2012 3:41:23 PM

72 JEMS SEPTEMBER 2012
HANDS ONPRODUCT REVIEWS FROM STREET CREWS
For more product reviews: www.jems.com/journal
The products presented here were featured in June JEMS as Hot Products discovered at this year’s EMS Today Conference and Exposition. These products were listed incorrectly with photos of other products. We regret the error and are presenting them with their correct images and information.
The FlOw-SAFe II CPAP SyStem with built-in manom-eter is now delivering up to 10 cm H2O at 15 LPM while using 50% less oxygen. Flow-Safe II has all of the bene-fits of the original CPAP system with superior safety fea-tures and performance, while consuming less oxygen. It doesn’t require special high-flow equipment. Flow-Safe II also delivers consistent CPAP pressure on inhalation and exhalation. No extra parts—it comes assembled with a deluxe mask, manometer and pressure-relief valve all in one disposable setup package. Clinicians can easily attach a nebulizer in-line for patients requiring aerosol inhalation medication with CPAP therapy.
The ReSCueR emeRgeNCy CPAP SyStem was designed to offer the maximal respiratory support to patients requiring positive pressure therapy. The new-est device available to EMS services, this device offers easy to apply pressure adjustment, separate inspiratory and expiratory filters and a medication port, while having the lowest oxygen consumption of any comparable device. Avail-able in two mask styles, this affordable CPAP system offers more features than any similar disposable CPAP device.
Mercury Medical800/237-6418
BlS SySteMS liMited905/339-1069
The FlO2mAX 4-IN-1 OXygeN mASk was designed to deliver the maximal amount of oxygen to the patient. This mask was designed to eliminate room air dilution using a patented series of valves. Able to convert to a small-volume nebulizer mask, this mask can function as a true “all in one mask” for EMS ser-vices. An integrated filter cap-tures all exhaled bacteria and excess medication, protecting equipment surfaces and staff from airborne contamination.
BlS SySteMS liMited
905/339 [email protected]
www.blssystemsltd.comComing next month, Dominic Silvestro will take over as our new JemS Hands On columnist. Here’s a little bit about him:
Dominic Silvestro, EMT-P, EMS-I, has for the past 19 years served as a career firefighter/paramed-ic for the Richmond Heights (Ohio) Fire Department, where he also served as the department’s public education officer. He has been in the fire/EMS service for more than 24 years. He’s also an EMS coordinator and EMS educator for the University Hospital’s EMS Training and Disaster Preparedness Institute, an Institute of University Hospitals and Rainbow Babies and Children’s Hospital.
New COlumNISt
072HANDSON.indd 72 8/15/2012 11:29:16 AM

No ChargeThree of the five hospitals treating
victims of the July 20 Aurora shooting say they will limit or completely cover the medi-cal expenses incurred. Most of the victims are single and under 35, the cohort most likely without medical insurance. A February 2012 report by the Colorado Health Institute said that one in six Coloradans didn’t have health insurance in 2011.
Children’s Hospital Colorado announced it would use donations and its charity care fund to cover the medical expenses of the unin-sured. The hospital says it will waive all co-pays for those who do have insurance.
HealthOne, which owns the Medical Cen-ter of Aurora and Swedish Medical Center, also says it will limit or eliminate hospital charges based on the individual circumstances of the patients.
The other hospitals, University of Colorado
Hospital and Denver Health Medical Center, are the top “safety net” hospitals in the state, providing $750 million in uncompensated care in 2011.
We applaud their compassionate response to the community.
CoNtiNuiNg a MissioNFreedom House Ambulance Service
served the St. Paul Hill District through 1975, training unemployed or underemployed black residents of the Hill District as EMTs.
In 2009, the St. Paul, Minn., EMS Academy started with the same goal of advancing the EMS profession and including providers of diverse ethnicity, cultures and language abili-ties. About 70 students have graduated from this EMS Academy so far.
Macalester College and Inver Hills Com-munity College partnered with Saint Paul city officials to arrange for three of the
74 JEMS SEPTEMBER 2012
Last WorDThe Ups & downs of eMs
JeMs (Journal of Emergency Medical Services), ISSN 0197-2510, is pub lished monthly by Elsevier Public Safety, 525 B Street, Suite 1800, San Diego, CA 92101-4495; 800/266-5367 (fed. ID #13-1958712). subsCriptioNs: Send $44 for one year (12 issues) or $74 for two years (24 issues) to P.O. Box 17049, North Hollywood, CA 91615-9247, or call 888/456-5367. Canada: Please add $25 per year for postage. All other foreign subscriptions: Please add $35 per year for surface and $75 per year for airmail postage. Send $32 for one year (12 issues) or $62 for two years (24 issues) of digital edition. Single copy: $10.00. postMaster: Send address changes to JEMS (Journal of Emergency Medical Services), P.O. Box 17049, North Hollywood, CA 91615-9248. Claims of nonreceipt or damaged issues must be filed within three months of cover date. Periodicals postage paid at San Diego, Calif., and at additional mailing offices. Canada Post International Publications Mail Product (CanadianDistribution) Sales Agreement No. 1247948. aDvertisiNg iNforMatioN: Rates are available at www.jems.com/jems/advertise/or by request from JEMS Advertising Department at 525 B Street, Suite 1800, San Diego, CA 92101-4495; 800/266-5367. Copyright © 2012 Elsevier Inc. No material may be reproduced or uploaded on computer network services without the expressed permission of the publisher. JEMS is indexed in the Cumulative Index to Nursing & Allied Health Literature and included in the Medline/PubMed database. JEMS is printed in the United States.
illU
sTra
Tio
n p
aU
l C
oM
bs
fiery ChaLLeNgeIt’s unfortunate EMS had to
respond to treat multiple patients for second- & third-degree burns after a moti-vational speaker convinced the patients it was safe to walk on hot coals during an event in San Jose, Calif., in June.
original Freedom House paramedics to attend a renaming and graduation.
Phase II began July 23. EMS Academy grad-uates are providing non-emergency stretcher transport service to those who are medi-cally required to have ambulance transpor-tation from a hospital either back home or to another hospital, or transport for a specialized doctor’s appointment.
We give a thumbs up to the EMS Academy for continuing the Freedom House mission. Check it out at www.ehs.net/emsacademy/ or www.facebook.com/EMSAcademy.
CoMpetiNg seNsesAmerican Medical Response (AMR)
returned to the Community College of Aurora (CCA) for its third annual national competition on July 15.
“Last year they did everything we asked for, pointing out that they could do more. This year we took their suggestions with great results,” says AMR Vice President of Clinical Affairs Scott Bourn, PhD.
The final two-person teams came from New Haven, Conn.; Modesto, Calif.; Lake Havasu, Ariz.; and Olympia, Wash. In the sce-nario, treated a patient who fell from a bal-cony in a bar and an unconscious patient.
All studios are equipped with video and audio, and CCA used wireless patient simula-tors. Pony Anderson, CCA simulation coor-dinator, says that the success of the center is the attention to detail. Scenarios include sight, smell, sound and touch. The Katrina House, where the scenario took place was complete with an “incredible” smell.
We congratulate the Center for Simula-tion staff and AMR for joining forces to pro-vide competitors with a unique, high-fidelity competition. JEMS
074_Lastword.indd 74 8/15/2012 11:07:03 AM

Choose 37 at www.jems.com/rs
0912-FP_RT.indd 1 8/14/2012 2:21:32 PM

Choose 38 at www.jems.com/rs
0912-FP_LFT.indd 1 8/14/2012 2:24:45 PM