
Jejunal cancer detected after a resection of bilateral ovarian metastasis: Report of a case
4
Surg Today (2010) 40:1084–1087 DOI 10.1007/s00595-009-4174-7 Reprint requests to: H. Maekawa Received: May 31, 2009 / Accepted: August 24, 2009 Case Report Jejunal Cancer Detected After a Resection of Bilateral Ovarian Metastasis: Report of a Case HIROSHI MAEKAWA, KOICHI SATO, YOSHIHIRO KOMATSU, HAJIME ORITA, and MUTSUMI SAKURADA Department of Surgery, Shizuoka Hospital, Juntendo University School of Medicine, 1129 Nagaoka, Izunokuni, Shizuoka 410-2295, Japan Abstract A 50-year-old woman was admitted to our hospital because of abdominal distension and fullness. Com- puted tomography and magnetic resonance imaging showed bilateral ovarian tumors. Although these ovarian tumors were suspected of being metastatic, the primary tumor site could not be detected before the bilateral salpingo-oophorectomy. At the time of laparotomy, there was no apparent peritoneal dissemination or ascites. The pathological findings suggested that the ovarian tumors were metastases from cancer of the digestive tract. Positron emission tomography using 18 F-fluorodeoxyglucose positron emission tomography (FDG-PET) and double-balloon enteroscopy detected jejunal cancer. A second laparotomy for the resection of jejunal cancer was performed. The patient received adjuvant chemotherapy, and there has not been any recurrence for 24 months since the resection was per- formed. In conclusion, FDG-PET was found to play a valuable role in the detection of the primary tumor. Intensive chemotherapy and surgical treatment also contributed to the long-term survival of the patient. Key words Jejunal cancer · Ovarian metastasis · 18 F- Fluorodeoxyglucose positron emission tomography Introduction The rate of metastatic ovarian tumors from the extra- genital organs is 4.4%–6.8%. 1,2 Metastatic ovarian tumors sometimes demonstrate symptoms before the primary sites can be detected. 3 The most common extra- genital primary sites of metastatic ovarian tumor are the colon, stomach, and breast. 1,2 Primary adenocarcinoma of the jejunum is not commonly encountered in clinical practice, and its incidence accounts for approximately 3% of all gastrointestinal tract malignancies. 4 Ovarian metastasis from jejunal cancer is rare. 1,2,5 This report describes a case of ovarian metastasis from primary jejunal cancer, which was detected after the resection of the ovarian metastasis. Case Report A 50-year-old woman was admitted because of a 1-month history of abdominal distension and abdominal fullness. Abdominal and pelvic computed tomography (CT) demonstrated two masses in the pelvic space. These masses were enhanced peripherally and their centers were almost cystic or necrotic (Fig. 1a). Mag- netic resonance imaging of the pelvis also demonstrated two well-circumscribed masses, measuring 12 × 11 × 11 cm and 4 × 3 × 4 cm, respectively (Fig. 1b). The serum tumor markers were examined. The serum level of car- cinoembryonic antigen was 10 ng/ml, that of carbohy- drate antigen 19–9 42 U/ml, and that of CA125 26 U/ml (Table 1). These findings suggested that these tumors were bilateral ovarian metastatic tumors. Gastrointesti- nal fiberscopy, colonoscopy, mammography, and breast ultrasonography did not detect any other lesions. The patient underwent a laparotomy with a diagnosis of a primary ovarian tumor because no apparent primary lesion was detected. At laparotomy, there was no peritoneal dissemination or ascites. No other tumors were found despite careful examination. The patient underwent a total abdominal hysterectomy, bilateral salpingo-oophorectomy, omentectomy, and pelvic lymphadenectomy. The right ovary measured 16 × 12 × 13 cm and weighed 2000 g, and the left ovary measured 5 × 4 × 4 cm and weighed 190 g. The permanent micro- scopic section showed the infiltration of well to moder- ately differentiated adenocarcinoma in both ovaries
-
Upload
hiroshi-maekawa -
Category
Documents
-
view
212 -
download
0
Transcript of Jejunal cancer detected after a resection of bilateral ovarian metastasis: Report of a case

Surg Today (2010) 40:1084–1087DOI 10.1007/s00595-009-4174-7
Reprint requests to: H. MaekawaReceived: May 31, 2009 / Accepted: August 24, 2009
Case Report
Jejunal Cancer Detected After a Resection of Bilateral Ovarian Metastasis: Report of a Case
HIROSHI MAEKAWA, KOICHI SATO, YOSHIHIRO KOMATSU, HAJIME ORITA, and MUTSUMI SAKURADA
Department of Surgery, Shizuoka Hospital, Juntendo University School of Medicine, 1129 Nagaoka, Izunokuni, Shizuoka 410-2295, Japan
AbstractA 50-year-old woman was admitted to our hospital because of abdominal distension and fullness. Com-puted tomography and magnetic resonance imaging showed bilateral ovarian tumors. Although these ovarian tumors were suspected of being metastatic, the primary tumor site could not be detected before the bilateral salpingo-oophorectomy. At the time of laparotomy, there was no apparent peritoneal dissemination or ascites. The pathological fi ndings suggested that the ovarian tumors were metastases from cancer of the digestive tract. Positron emission tomography using 18F-fl uorodeoxyglucose positron emission tomography (FDG-PET) and double-balloon enteroscopy detected jejunal cancer. A second laparotomy for the resection of jejunal cancer was performed. The patient received adjuvant chemotherapy, and there has not been any recurrence for 24 months since the resection was per-formed. In conclusion, FDG-PET was found to play a valuable role in the detection of the primary tumor. Intensive chemotherapy and surgical treatment also contributed to the long-term survival of the patient.
Key words Jejunal cancer · Ovarian metastasis · 18F-Fluorodeoxyglucose positron emission tomography
Introduction
The rate of metastatic ovarian tumors from the extra-genital organs is 4.4%–6.8%.1,2 Metastatic ovarian tumors sometimes demonstrate symptoms before the primary sites can be detected.3 The most common extra-genital primary sites of metastatic ovarian tumor are the colon, stomach, and breast.1,2 Primary adenocarcinoma
of the jejunum is not commonly encountered in clinical practice, and its incidence accounts for approximately 3% of all gastrointestinal tract malignancies.4 Ovarian metastasis from jejunal cancer is rare.1,2,5 This report describes a case of ovarian metastasis from primary jejunal cancer, which was detected after the resection of the ovarian metastasis.
Case Report
A 50-year-old woman was admitted because of a 1-month history of abdominal distension and abdominal fullness. Abdominal and pelvic computed tomography (CT) demonstrated two masses in the pelvic space. These masses were enhanced peripherally and their centers were almost cystic or necrotic (Fig. 1a). Mag-netic resonance imaging of the pelvis also demonstrated two well-circumscribed masses, measuring 12 × 11 × 11 cm and 4 × 3 × 4 cm, respectively (Fig. 1b). The serum tumor markers were examined. The serum level of car-cinoembryonic antigen was 10 ng/ml, that of carbohy-drate antigen 19–9 42 U/ml, and that of CA125 26 U/ml (Table 1). These fi ndings suggested that these tumors were bilateral ovarian metastatic tumors. Gastrointesti-nal fi berscopy, colonoscopy, mammography, and breast ultrasonography did not detect any other lesions.
The patient underwent a laparotomy with a diagnosis of a primary ovarian tumor because no apparent primary lesion was detected. At laparotomy, there was no peritoneal dissemination or ascites. No other tumors were found despite careful examination. The patient underwent a total abdominal hysterectomy, bilateral salpingo-oophorectomy, omentectomy, and pelvic lymphadenectomy. The right ovary measured 16 × 12 × 13 cm and weighed 2000 g, and the left ovary measured 5 × 4 × 4 cm and weighed 190 g. The permanent micro-scopic section showed the infi ltration of well to moder-ately differentiated adenocarcinoma in both ovaries

H. Maekawa et al.: Jejunal Cancer Detected After Metastasis 1085
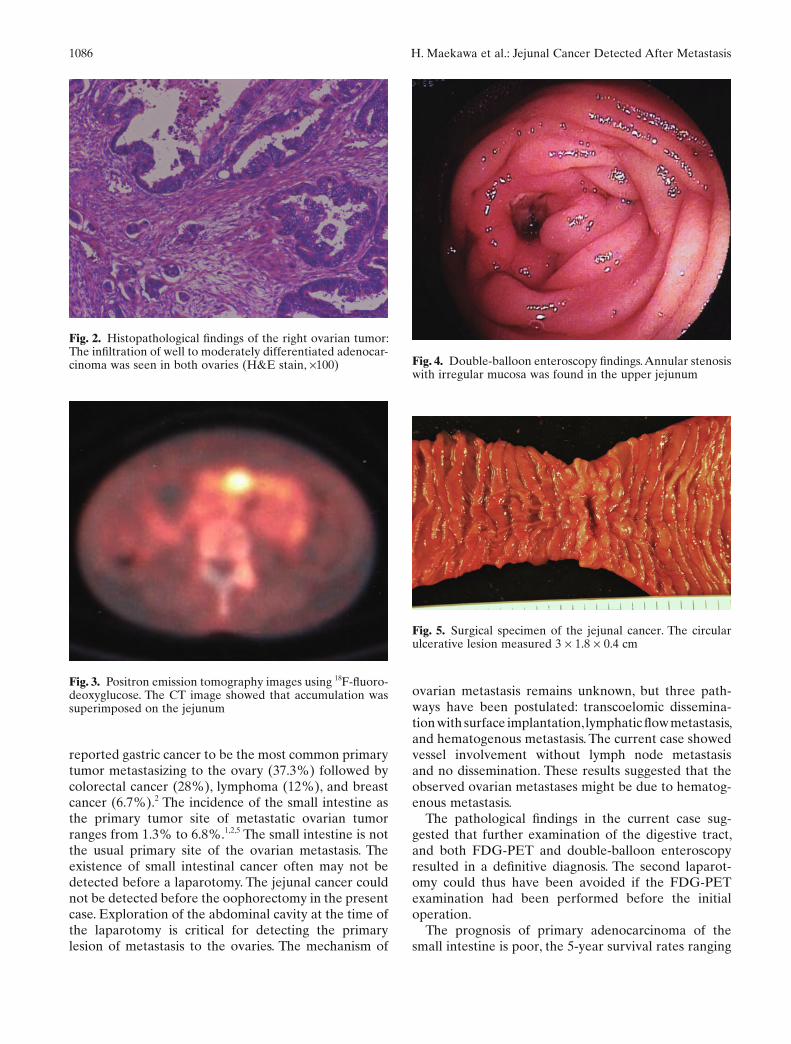
(Fig. 2). There was no metastasis of adenocarcinoma in the dissected lymph nodes. The pathological fi ndings suggested that the ovarian tumors were metastases from cancer of the digestive tract, especially that in the colorectal region. Postoperative endoscopic exami-nations again detected no apparent lesion. Positron emission tomography was performed using 18F-fl uoro-deoxyglucose positron emission tomography (FDG-PET), which showed a single area of uptake in the upper abdomen, superimposed on the jejunum (Fig. 3). Double-balloon enteroscopy was performed, and an annular stenosis with reddish edematous irregular mucosa was found in the upper jejunum (Fig. 4). The pathological result of a biopsy from the jejunal lesion was similar to that of the ovarian tumors. A second lapa-rotomy was performed for resection of the jejunal lesion, because the FDG-PET study did not show any other metastasis. Exploration of the upper abdomen demonstrated an annular constriction of the jejunum 70 cm distal to the ligament of Treitz. There were no disseminated nodules detected during surgery. A partial resection of the jejunum was performed with a biopsy of the mesenteric lymph nodes. The surgical specimen showed a circular ulcerative lesion that measured 3 × 1.8 × 0.4 cm (Fig. 5). Microscopically, the jejunal lesion contained well to moderately differentiated adenocar-cinoma that infi ltrated to serosal, and vessel invasion
was identifi ed. Finally, the patient was diagnosed to have primary jejunal cancer and metastasis to the bilateral ovaries. She was discharged from the hospital 7 days after the second laparotomy. Adjuvant chemotherapy with S-1 (100 mg daily for 4 weeks with 2 weeks off) was administered for 12 months, and no recurrence has been observed for 24 months since the resection.
Discussion
The incidence of metastatic ovarian tumors from extra-genital tumors is 4.4%–6.8%. The diagnosis of the meta-static ovarian tumors is not always easy. Kim et al. suggested that CT and magnetic resonance fi ndings are sometimes useful for the diagnosis of ovarian metastatic tumors.6 The fi ndings of solid ovarian tumors containing well-demarcated intratumoral cystic lesions suggest a metastatic tumor. However, the CT aspect of the meta-static ovarian tumor is not completely distinguishable from primary ovarian cancer.7 A metastatic ovarian tumor is frequently diagnosed at the time of a laparot-omy or postoperatively. Kim et al. reported that 25% of the primary site tumors are found at the time of lara-rotomy.6 Turan et al. reported that the primary tumor sites were not detected even after an oophorectomy in 12.1% of metastatic ovarian tumors.2 Turan et al. also
Fig. 1. a Pelvic axial computed tomogra-phy (CT) with contrast enhancement. An ovarian mass occupies the pelvis. There is a predominance of the central cystic com-ponent with a surrounding moderate enhancement of the solid component. b Sagittal T2-weighted magnetic resonance image of the pelvis. A large pelvic mass with cystic and solid components was visualized
Table 1. Laboratory fi ndings on admission
Normal range Normal range
Hemoglobin 12.9 g/dl 34–42 Na 139 mEq/l 135–152Hematocrit 38.8% 12–16 K 4.2 mEq/l 3.5–5.3RBC 424 × 104/ml 380–480 × 104 Cl 102 mEq/l 96–107WBC 7300/ml 4000–8000 Ca 8.3 mg/dl 8–11Platelets 25.3 × 104/ml 15–40 × 104
Total protein 6.7 g/dl 6.5–8 BUN 11.9 mg/dl 8–22Albumin 3.9 g/dl 3.0–5.0 Cr 0.5 mg/dl 0.4–1.2GOT 17 IU/l 10–40 Tumor markerGPT 10 IU/l 5–40 CEA 10 ng/ml 0–5LDH 270 IU/l 120–230 CA19-9 42 U/ml 1–38Glucose 89 mg/dl 65–110 CA125 26 U/ml 0–35
1086 H. Maekawa et al.: Jejunal Cancer Detected After Metastasis
reported gastric cancer to be the most common primary tumor metastasizing to the ovary (37.3%) followed by colorectal cancer (28%), lymphoma (12%), and breast cancer (6.7%).2 The incidence of the small intestine as the primary tumor site of metastatic ovarian tumor ranges from 1.3% to 6.8%.1,2,5 The small intestine is not the usual primary site of the ovarian metastasis. The existence of small intestinal cancer often may not be detected before a laparotomy. The jejunal cancer could not be detected before the oophorectomy in the present case. Exploration of the abdominal cavity at the time of the laparotomy is critical for detecting the primary lesion of metastasis to the ovaries. The mechanism of
Fig. 2. Histopathological fi ndings of the right ovarian tumor: The infi ltration of well to moderately differentiated adenocar-cinoma was seen in both ovaries (H&E stain, ×100)
Fig. 3. Positron emission tomography images using 18F-fl uoro-deoxyglucose. The CT image showed that accumulation was superimposed on the jejunum
Fig. 4. Double-balloon enteroscopy fi ndings. Annular stenosis with irregular mucosa was found in the upper jejunum
Fig. 5. Surgical specimen of the jejunal cancer. The circular ulcerative lesion measured 3 × 1.8 × 0.4 cm
ovarian metastasis remains unknown, but three path-ways have been postulated: transcoelomic dissemina-tion with surface implantation, lymphatic fl ow metastasis, and hematogenous metastasis. The current case showed vessel involvement without lymph node metastasis and no dissemination. These results suggested that the observed ovarian metastases might be due to hematog-enous metastasis.
The pathological fi ndings in the current case sug-gested that further examination of the digestive tract, and both FDG-PET and double-balloon enteroscopy resulted in a defi nitive diagnosis. The second laparot-omy could thus have been avoided if the FDG-PET examination had been performed before the initial operation.
The prognosis of primary adenocarcinoma of the small intestine is poor, the 5-year survival rates ranging

H. Maekawa et al.: Jejunal Cancer Detected After Metastasis 1087
from 20% to 30%.4 The early and accurate diagnosis of small intestinal cancer is diffi cult because of its rare clinical incidence and lack of specifi c symptoms. Ouriel and Adams suggested that favorable prognostic factors of adenocarcinoma of the small intestine included jejunal location, absence of nodal metastasis, and well-differentiated grade.4 The current patient has remained free from disease after cancer resection for 24 months, with chemotherapy. 5-Fluorouracil-based regimens are often administered in similar cases.4,8 Adjuvant chemo-therapy appears to have a benefi cial effect on survival, although a signifi cant effect after a curative resection has not yet been proven.4,8,9 However, palliative chemo-therapy for patients with metastasis improves the overall survival in comparison to those patients who receive no chemotherapy.8 Sakakura et al. reported the 12-month survival of a patient with jejunal cancer, ovarian metas-tases, and peritoneal dissemination.10 They suggested that intensive chemotherapy and a jejunal resection for carcinoma results in a prolonged survival. Therefore, intensive treatment in addition to the early diagnosis of jejunal cancer is expected to improve its prognosis. A careful and successive workup in order to identify the primary tumor is also important for selecting the optimal treatment for metastatic ovarian tumors.
References
1. Moore RG, Chung M, Granai CO, Gajewski W, Steinhoff MM. Incidence of metastasis to the ovaries from nongenital tract primary tumors. Gynecol Oncol 2004;93:87–91.
2. Turan T, Aykan B, Koc S, Boran N, Tulunay G, Karacay O, et al. Analysis of metastatic ovarian tumors from extragenital primary sites. Tumori 2006;92:491–5.
3. Suzuki J, Kazama S, Kitayama J, Uozaki H, Miyama T, Nagawa H. Signet ring cell carcinoma of the appendix manifesting as colonic obstruction and ovarian tumors: report of a case. Surg Today 2009;39:235–40.
4. Oureil K, Adams JT. Adenocarcinoma of the small intestine. Am J Surg 1984;147:66–71.
5. Gallup DG, Stock RJ, Sammons JJ, Paulk WE. Primary small bowel adenocarcinoma presenting as a malignant ovarian neo-plasm. Mil Med 1985;150:105–6.
6. Kim SH, Kim WH, Park KJ, Lee PJ, Kim JS. CT and MR fi ndings of Krukenberg tumors: comparison with primary ovarian tumors. J Comput Assist Tomgr 1996;20:393–8.
7. Mata JM, Inaraja L, Rams A, Andreu J, Donoso L, Marcuello G. CT fi ndings in metastatic ovarian tumors from gastrointestinal tract neoplasms (Krukenberg tumors). Gatrointest Radiol 1988;13:242–6.
8. Sook HH, Yoon HK, Sang YR, Jae HB, Seung TO, Keun WI, et al. Primary adenocarcinoma of the small intestine: Presentation, prognostic factors and clinical outcome. Jpn J Clin Oncol 2009;39:54–61.
9. Tsuruchi N, Kubota H, Tsukamoto N, Kurano A. Primary jejunal adenocarcinoma masquerading as a primary ovarian malignancy. Gynecol Oncol 1995;58:129–32.
10. Sakakura C, Hagiwara A, Yoshikawa T, Hamada T, Yamagishi H. Huge ovarian metastasis from jejuna cancer occurring immedi-ately after initial operation. Hepatogastroenterology 2005;52:425–8.


















