January 25, 2012 Implementing Recovery-Oriented Practices Kevin Ann Huckshorn RN, MSN, CADC Paula G....
89
January 25, 2012 Implementing Recovery-Oriented Practices Kevin Ann Huckshorn RN, MSN, CADC Paula G. Panzer, M.D. Eric Arauz, MLER
-
Upload
lorin-powers -
Category
Documents
-
view
214 -
download
2
Transcript of January 25, 2012 Implementing Recovery-Oriented Practices Kevin Ann Huckshorn RN, MSN, CADC Paula G....

January 25, 2012
Implementing Recovery-Oriented Practices
Kevin Ann HuckshornRN, MSN, CADC
Paula G. Panzer, M.D. Eric Arauz, MLER

January 25, 2012
Kevin Ann Huckshorn, RN, MSN, CADCDelaware Director for the Division of Substance Abuse and Mental Health
Paula Panzer, M.D.Director of Training and Professional Development Jewish Board of Family and Children's Services
Eric Arauz, MLERArauz Inspirational Enterprises Adjunct Instructor, Department of Psychiatry, Robert Wood Johnson Medical School New Jersey Governor’s Council on Alcoholism and Drug Abuse APNA RTP Steering and Curriculum Committees
Moderated byLarry Davidson, Ph.D.Project Director, Recovery to Practice (RTP)Development Services Group (DSG), Inc.
If you are not hearing the audio…
To access the audio portion of this Webinar, please dial the conference service directly and enter the participant access code:
Audio Conferencing (toll-free):1.888.790.1893
Participant Access Code:6730907
3–3:05 p.m.
3:05–3:10 p.m.
3:10–3:25 p.m.
3:25–3:40 p.m.
3:40–3:55 p.m.
3:55–4:30 p.m.
Welcome
Introductions & Overview
Trauma-Informed Care: A Shift in Thinking for Service Providers
Understanding and Addressing the Impact of Trauma in a Recovery-Oriented Practice
The Trauma of Delusions
Discussion
Wilma TownsendSAMHSA/CMHS
Larry Davidson, Ph.D.DSG, Inc.
Kevin Ann HuckshornRN, MSN, CADC
Paula Panzer, M.D.
Eric Arauz, MLER
Participants & Presenters

Process for Questions, Answers, and Downloading Slides
Our speakers will present their slides, which will be followed by moderated questions and answers. We encourage you to ask questions or make comments! To ask a question, click on the Q/A tab and type your question in the window that opens, or press *1 for the operator, who will take your question in the order in which it is received.
This Webinar will be recorded and archived for future use. Please visit www.dsgonline.com/rtp/resources.html for more information.
Kevin Ann Huckshorn, RN, MSN, CADCDSAMH State Division DirectorSubstance Abuse and Mental Health
Kevin Ann Huckshorn

7
Outline
What is trauma?
What is Trauma-Informed Care (TIC)?
What are the differences between a trauma-informed and uninformed service system?
Trauma assessment

8
What Makes an Event Traumatic?
Traumatic Events Are
Sudden, unexpected, and extreme.
Usually involve physical harm or perceived life threat. (Research has shown perception of “life threats” is a powerful predictor of the impact of trauma.)
People experience these events as out of their control.
Certain stages of life make people more vulnerable to the effects of trauma, including childhood, teenage years, and early 20s. All presuppose a greater impact on life in adulthood.
(Tedeschi, 2011)

9
Traumatic Life EventsThat Can Result in Mental Health Problems
Are interpersonal in nature: intentional, prolonged, repeated
Includes sexual abuse, physical abuse, severe neglect, emotional abuse
Includes witnessing violence, repeated abandonment, sudden and traumatic loss
Can occur in childhood, adolescence, or at any point in an adult’s lifetime depending on extent (Terr, 1991; Giller, 1999; Felitti, 1998)
The process of “becoming homeless” is widely believed to have exposed all involved to trauma; homelessness itself is traumatic
(Hopper, Bassuk, & Olivet, 2010)

10
The Definition of Trauma-Informed Care
“Trauma-Informed Care is a strengths-based framework that
Is grounded in an understanding of (and on) responsiveness to the impact of trauma
Emphasizes physical, psychological, and emotional safety for both providers and survivors
Creates opportunities for survivors to rebuild a sense of control and empowerment.”
(Hopper, Bassuk, & Olivet, 2010)

11
How Many People Have Experienced Trauma?
What about the people we serve?
What about people in other care settings?
12
Prevalence of TraumaMental Health Population: Adults
97% of homeless women with serious mental illness (SMI) experienced severe physical and sexual abuse 87% experienced abuse in both childhood and adulthood
(Goodman et al., 1997)
90% of public mental health clients have been exposed to trauma had multiple experiences of trauma (Mueser et al., in press;
Mueser et al., 1998)
81% of adults diagnosed with bipolar disorder or Dissociative Identity Disorder (90%) were sexually or physically abused as children (Herman et al., 1989; Ross et al., 1990)
29–43% of people with SMI have posttraumatic stress disorder (PTSD) (CMHS/HRANE, 1995; Jennings & Ralph, 1997)
Image: Photo of homeless woman

13
Prevalence of TraumaMental Health Population: Children & Adolescents
Canadian study of 187 adolescentsreported 42% had PTSD.
(Kotlek, Wilkes, & Atkinson, 1998)
In a U.S. study of 100 adolescent inpatients, 93% had histories of trauma and 32% had PTSD. (Lipschitz et al., 1999)
A study of one State system’s child/adolescent long-term care service users (162) found 100% had documented histories of trauma. (Massachusetts DMH, 2007)
Image: Photo of young girl
14
Prevalence of Trauma: Substance Abuse Population
Up to 2/3 of men and women in SA treatment report childhood abuse and neglect. (CSAT, SAMHSA, 2000)
Study of male veterans in SA inpatient unit
77% exposed to severe childhood trauma.
58% history of lifetime PTSD. (Triffleman et al., 1995)
50% of women in SA treatment have history of rape or incest. (Gov. Comm. on Sexual and Domestic Violence, Comm. of Mass., 2006)
Image: Photo of drug-injecting man
15
Prevalence of Trauma: Incarcerated Women
Framingham Women’s Prison, Mass. 90% receiving mental health services or SA services have trauma
histories. (Governor’s Task Force, Comm. of Mass., 2005)
Correctional Institute for Women, R.I. 40% – Childhood sexual abuse 55% – Childhood physical abuse 53% – Adult rape 63% – Adult physical assault 34% – Lifetime PTSD
(Zlotnick, 1997; Zlotnick, Najavits et al., 2003)
Image: Photo of imprisoned women

16
Prevalence of Trauma: Incarcerated Youth
93% of males in a juvenile justice (JJ) facility reported trauma history (compared to 84% females), but more females met criteria for PTSD (18% female, 11% male). (Abram et al., 2004)
70–92% of incarcerated girls reported sexual, physical, or severe emotional abuse in childhood. (DOC, 1998; Chesney & Sheldon, 1997)
PTSD prevalence data varies widely:
3–50% in JJ settings and up to eight times higher than community samples of same-age peers. (Arroyo, 2001; Garland et al., 2001; Teplin et al., 2002; Saigh et al., 1999; Saltzman et al., 2001)
Image: Photo of imprisoned man

17
Trauma Prevalence
The prevalence of trauma appears to be a link or “cross cutting principle” that affects people receiving services in all human service and health care settings.
These individuals often experience depression, SA, serious mental conditions, vulnerability to re-victimization, difficulty working, and/or impaired social networks.
(Hopper, Bassuk, & Olivet, 2010)

18
Pervasiveness of Trauma
“In my own case, growing up in an alcoholic home, I came to accept chaos as a normal state of affairs rather than the exception. I wound up sabotaging my first marriage simply because the calm left me unsettled and nervous; I had to create chaos where none existed because that's all I was familiar with.”
—Suzanne Somers, actress and author
Image: Photo of Suzanne Somers

19
Well Known and Not-So-Well-KnownPeople Aren’t Immune from Trauma
Desperate Housewives star Teri Hatcher revealed she was sexually abused by her uncle after he was arrested for molesting another girl.
Many well known and not-so-well-known people have experienced trauma.
Image: Celebrity photos

20
What Does All of This Mean?
Great question. A lot of really smart people are working on this answer. What we do know …
Most of the people served in …
MH/SA treatment settings
DOC or JJ systems
Homeless systems
… have trauma histories.
Many people served in other care systems have experienced trauma (ID, TBI, elderly).
People who are not in care settings may also experience trauma—that means our staff, too.
(Hodas, 2004; Frueh et al., 2005; Mueser et al., 1998; Lipschitz et al., 1999; NASMHPD, 1998)
21
Trauma: The interface Between Exposure, Choices, and Health Status
Research has focused on the effects of childhood trauma on adult health outcomes:
Adverse Childhood Experiences (the ACE study) demonstrated the serious health consequences of trauma.
Increasing ACE scores correlated with increasing numbers of risky health behaviors as coping mechanisms in adulthood, including
eating disorders, smoking, substance abuse, self-harm, sexual promiscuity.
These behaviors resulted in
severe medical conditions such as heart disease, pulmonary disease, liver disease, STDs, GYN cancer, and early death.
(Felitti, Anda et al., 1998)
22
OK. So People Who Get Services in Public Health Care Settings Are Most Likely Trauma Survivors. So What?
Calls for implementation of a TIC framework within our service settings
Just like in change theory, this is a multistep, staggered process that highlights three key focus areas:
Attitudes (of staff and clients)
Implementation (how do we make changes?)
Outcomes (How do we measure changes? May include quantitative or qualitative measures.)
(Hopper, Bassuk & Olivet, 2010)

23
Implementing TIC: Outcomes
TIC service settings have better outcomes than “services as usual” for many symptoms and social issues and show a decrease in MH and SA symptoms/ improvement in engagement.
Trauma-informed services may have an improved and positive effect on housing stability (early research).
Trauma-informed services may lead to a decrease in crisis services use and a loss of housing and inpatient care.
Trauma-informed services are cost effective.
Clients respond better to trauma-informed services.
(Hopper et al., 2010)
24
Implementing TIC: Starting Points
Do an organizational “self-assessment” if you feel the need to explore your agency’s readiness. Or “just do it.”
Identify and use a theory-based model as a guide. Document your organization’s beliefs/vision in writing and train staff accordingly.
Strive to avoid any practices that may be re-traumatizing in your system.
Implement universal trauma screening on admission, using standardized measures.
(Hopper et al., 2010)

25
What if You Don’t Know if Someone Has a Trauma History? What Do You Do?
Staff in human service settings need to take a “universal precautions approach.”
Assume that everyone you serve has a history of trauma.
(Hodas, 2004)

26
Universal Precautions
These kinds of “precautions” are aimed at preventing illness or injury before it happens.
Like hand-washing techniques to avoid transmitting germs or using condoms for “safe sex.”
In a trauma-informed setting, this means using strategies to ensure comfort: always be welcoming, avoid conflict/violence, meet needs assertively, and minimize any traumatic event that could hurt clients or staff.
(NETI, 2010)

27
What Does All This Mean?
For the people we serve, the outcomes of traumatic life experiences primarily mean this:
“The loss of ability to regulate the intensity and duration of affect …” (Schore, 2003)
“A breakdown in the capacity to regulate internal states including fear, anger, and sexual impulses.” (van der Kolk, 2005)

28
The Three Contexts of HealingWhen Systems Are Trauma Informed
Safety:
A core developmental need for human beings
o The defining experience of children or adults who have been traumatized is a pervasive mistrust of those “in power,” whether these are parents, caretakers, providers, police, or other officials. These people have suffered core damage to an early developmental stage called “trust vs. mistrust.” To bridge this gap, TIC systems have to first build trust.
(Bath, 2008)
29
Connections:
The second pillar of TIC expects the healthy development of relationships between service recipients and their care providers.
o These are life-giving relationships that are required to bridge the distrust these victims bring to our systems of care. People who have experienced trauma bring suspicion, avoidance, and hostility to their relationships. It is what they expect. It is our role to change this.
The Three Contexts of HealingWhen Systems Are Trauma Informed
(Bath, 2008)

30
The Three Contexts of HealingWhen Systems Are Trauma Informed
Emotion and Impulse Management:
The most pervasive impact of trauma is the dysregulation of emotions and impulses. The ability to regulate these is also one of the most “fundamental protective factors” for healthy adults.
o As such, all providers of human services should understand the need to teach self-regulation skills, e.g., how to learn to “self-soothe.” Active listening can help; labeling problem behaviors and their consequences is another step in this process. Practicing new strategies—with supervision—is key.
(Bath, 2008)

31
What Does a Trauma-Informed Care System Look Like?
32
Trauma Informed Non-Trauma Informed
Recognition of high prevalence of trauma
Life history is appreciated/recorded
Recognition of setting/culture and practices that are re-traumatizing
Lack of education on trauma prevalence and “universal” precautions
Person seen without family/social history
“Tradition of Toughness” valued as best care approach
How would trauma be recognized?
33
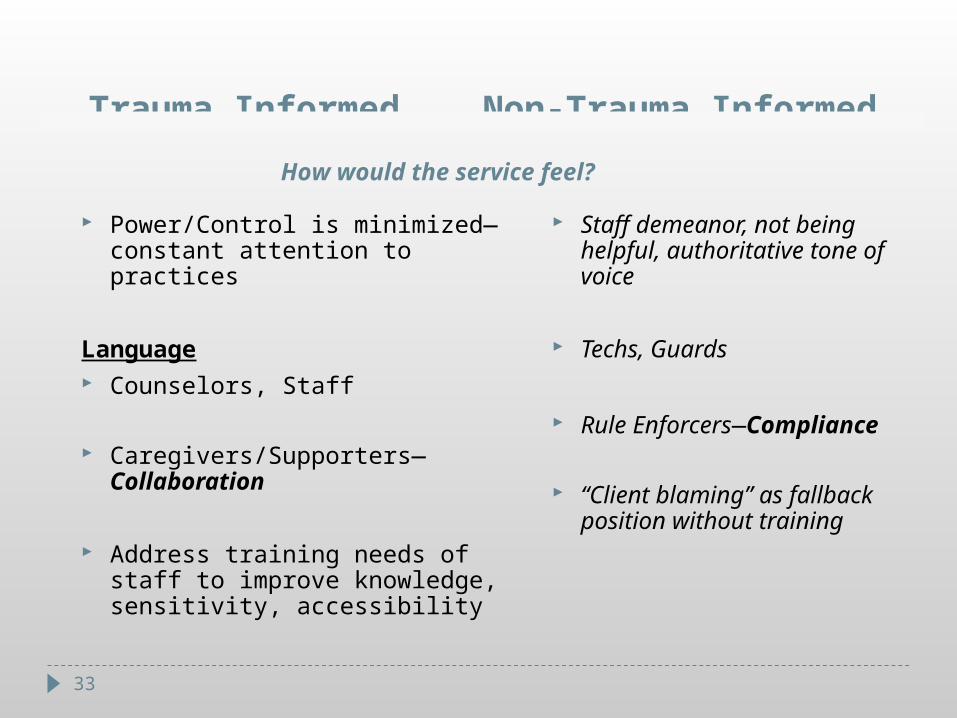
Trauma Informed Non-Trauma Informed
Power/Control is minimized—constant attention to practices
Language Counselors, Staff
Caregivers/Supporters—Collaboration
Address training needs of staff to improve knowledge, sensitivity, accessibility
Staff demeanor, not being helpful, authoritative tone of voice
Techs, Guards
Rule Enforcers—Compliance
“Client blaming” as fallback position without training
How would the service feel?

34
Trauma Informed Non-Trauma Informed
Understand function of behaviors (rage, apathy, irresponsibility, self-injury)
Objective, neutral language
Peer staff employees are present to assist other staff in understanding the person’s perspective
Transparent systems open to outside parties
Behavior seen as intentionally provocative and volitional
Labeling language: manipulative, needy, gamey, “attention seeking”
Lack of Peer Supports
Closed system—advocates discouraged
(Fallot & Harris, 2002; Cook et al., 2002; Ford, 2003; Frueh et al., 2005; Jennings, 1998; Prescott, 2000)
How would people be respected?

35
The Importance of Carefully Assessing Trauma

36
Why Is Trauma Assessed?
A more sensitive review of someone’s trauma history should be conducted respectfully and shortly after your first contact in order to
Identify past or current trauma, violence, abuse experiences
Learn how trauma is expressed when the person is under duress
Incorporate this information into an individualized, person-specific care plan
Health care settings need to request this information from referral sources or do a short assessment themselves.
(Cook et al., 2002; Fallot & Harris, 2002; Maine BDS, 2000)

37
Common Trauma Symptoms People Struggle With
Dissociation
Flashbacks
Nightmares
Hypervigilance
Terror
Anxiety
Negative auditory hallucinations
Numbness
Depression
Substance abuse
Self-injury
Eating problems
Sexual promiscuity
Poor judgment and continued cycle of victimization
(DSM IV-TR, 2000)

38
Trauma Assessment Components
Type sexual, physical, emotional, neglect, witnessed domestic violence,
exposure to disaster, combat exposure, other
Age When the abuse occurred is important in terms of the impact on the
person’s development
Who Was abuser a stranger? A family member?
(Carmen et al., 1996)

39
Trauma Assessment: Key Principles
Focus on “what happened to you?” instead of “what is wrong with you?”
Begin to develop a therapeutic relationship (trust, respect, caring) during this process.
(Bloom, 2002)

40
Trauma Assessment: Key Principles
Information from the assessment and “positive responses” should be incorporated into service plans, or the assessment has no value.
Also, if previously disclosed, what happened? Ask if the person has ever told anyone, at all …

41
In Summary…
Most people who access public services have been traumatized.
When stressed, past trauma informs current behaviors.
Troubling behaviors can often be learned survival strategies.
Try to understand the consumer’s history and how to support efforts to teach self-calming and regaining control.
Practices that take away control and choice can be traumatizing.
Watch for trauma “uninformed” practices and try to prevent, avoid, or eliminate these.
Keep asking—Is what I am doing respectful and trauma informed? Is it how I would like to be treated?

42
“If you can, help others;if you cannot do that,
at least do not harm them.”—Dalai Lama

43
Contact Information
Kevin Huckshorn, RN, MSN, CADC
DSAMH
Phone: 302-255-9398
Email: [email protected]
[email protected] NCTSN.org www.homeless.samhsa.gov www.nasmhpd.org

Paula G. Panzer, M.D.Director of Training and Professional DevelopmentJewish Board of Family and Children's ServicesNew York, N.Y.
Paula G. Panzer
45
Understanding trauma is notjust about acquiring
knowledge.
It’s about changing the way youview the world.
—Sandra Bloom, 2007
46
Because coping responses to abuse and neglect are varied and
complex, trauma survivors may carry any psychiatric diagnosis and
frequently trauma survivors carry many diagnoses.
Sidran Institute, 2010
47
We Create Shared Definitions …
… to create a common understanding and language
We start with those involved in the dialogue
Consumers
Clinicians
Community partners
We define to develop policies and practices
We check in to make sure the definition is relevant

48
Trauma
Traumatic Stress
Traumatic Stress Disorders
Trauma-Informed Care
Trauma-Specific Services
Shared Definitions
49
Trauma Traumatization
Trauma—something that threatens
one’s psychic or physical integrity
Traumatization occurs when both internal and external resources are inadequate to cope with external threat. (Bessel van der Kolk, 1989)
50
Traumatic Stress and Traumatic Stress Disorders
Physical and emotional responses
of an individual to trauma
When traumatic events overwhelm
an individual’s ability to cope and
elicit feelings of terror,
powerlessness, rage, and out-of-
control physiological arousal
Disorders related to and/or
specifically a result of trauma
exposure
PTSD
ASD
DID
…DES NOS
And then some less clearly defined

51
Trauma-Specific Services (TSS)
Trauma-Specific Services (TSS) are models designed to treat the
psychological and behavioral consequences of trauma exposure.
Targeted to the period of time relative to trauma exposure (immediate,
short-term, and delayed) and to the type of reactions and symptoms
being addressed (e.g., supporting adaptive coping after a disaster or
treating chronic PTSD).
Based upon evidence for effective interventions.
TSS should be delivered in a TIC system.
TSS are recovery oriented ONLY when offered in a person-centered and
empowering manner.

52
Trauma-Informed Lens and Assessment
Trauma-informed work requires use of
an informed lens.
Trauma histories and trauma
symptoms are not usually
spontaneously offered.
We must ask.
Image: Sunglasses

53
Traumatic Stress Responses and Symptoms
Activation responses
Trigger response
Level of activation
Avoidance responses
Emotional numbing, dissociation, denial, thought suppression
Intrusive and incomplete remembrance
Avoidance of trauma reminders
Re-experiencing
Hyperarousal
Trauma-related, sexualized, aggressive, or oppositional behaviors
Dissociation
Unsafe behaviors
54
AVOIDANCE
Many consumers won’t initiate discussion about trauma exposure because they
may fear talking about the trauma will trigger them and cause an intense and painful reaction
may feel embarrassed, guilty, responsible for, or stigmatized by experiences
trauma memories are typically fragmented and confusing
some have been rejected or further injured with prior attempts to tell
past experiences with telling have been too painful
abusers threatened retaliation if the secret was revealed
Many clinicians are reluctant to initiate discussion about trauma exposure
studies show clinicians underestimate the incidence of consumer trauma exposure and fail to ask
fear it will be too distressing for their consumers
fear the effect it will have on them, or feel they don’t have the skills to help the consumer after disclosure
undervalue the story of the trauma and overvalue their assumptions on the consumer
55
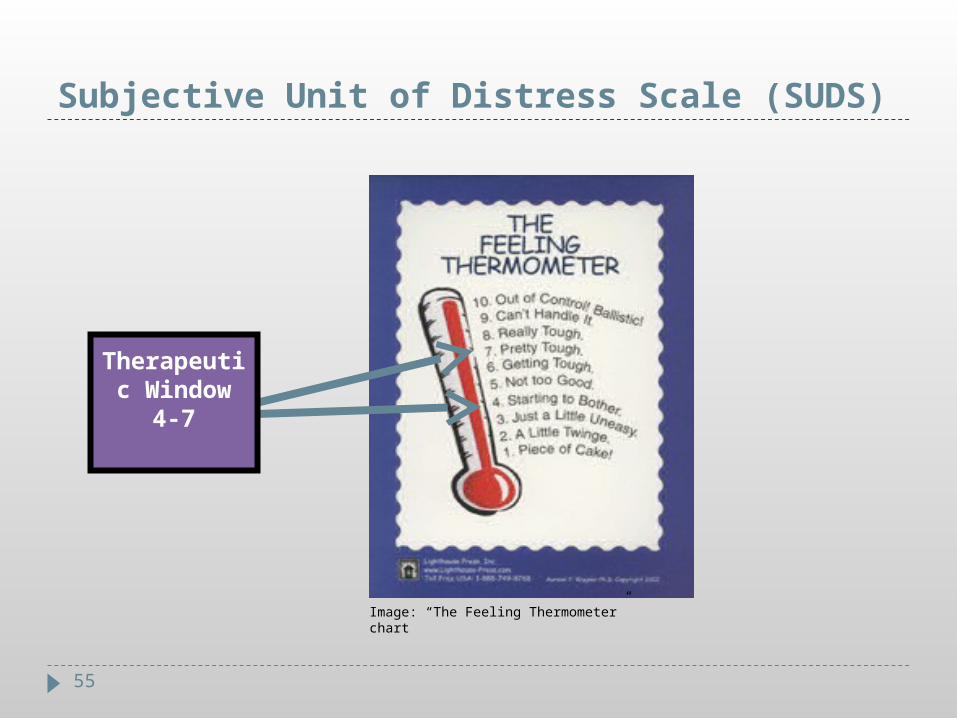
Subjective Unit of Distress Scale (SUDS)
Image: “The Feeling Thermometer” chart
Therapeutic Window
4-7

56
PTSD Protective Factors
PTSD is a failure of natural recovery with both risk factors and protective factors.
Social support is a key mediating factor
Believing and validating the experience
Feeling good about one’s own actions in the face of danger
Cognitive and self-regulation abilities
Positive belief about oneself
Motivation to act effectively in environment
57
Factors to Consider for Treatment Planning
How trauma history is impacting current behavior
How triggers/reminders are impacting behavior
Establish purpose for a trauma-specific intervention
Be mindful of ongoing trauma and environmental risks
Consumer to establish goals
That address symptoms and function
That take into consideration the power of avoidance
That respect meaning making and coping
That start from a strengths perspective
Clear roles for consumer and clinician over the course of the intervention and the value of community supports
Image: Unlatched chest

58
Risks of Not Treating Trauma-Related Disorders
Consumer not heard, valued, understood
Most trauma-specific disorders are treatable
The trauma-specific distress can disrupt functioning and exacerbate co-occurring disorders
Missed opportunity for human connections
Missed chance for meaning making

59
Trauma-Specific Services
60
Trauma-Specific Servicesin a Recovery-Oriented Practice
Intervention choices in response to experiencing symptoms
To prevent or minimize symptoms
To manage or overcome the disorder
61
Get to Know the Treatments
Evidence-based/supported trauma tx CBT
TF–CBT; CTG–CBT
CPT
CPP
TST
STAIR
EMDR
SPARCS
TREM
Seeking Safety
PE (Prolonged Exposure)
Medication
Others?
Non-trauma-specific EBTs and non-EB treatments often used with traumatized consumersDBT
MST
FFT
STEPPS
PCIT
Somatic treatments (sensorimotor, somatic experiencing, yoga, etc.)
Psychodrama therapy
Narrative Therapy
IPT
Others?
62
Commonalities of Phased Trauma Treatments
1. Safety and stabilization—preparatory phase; purpose is to restore and/or strengthen consumer’s sense of safety and coping skills, and can include the following. Elements of phase will be repeated and reinforced throughout the next two phases.
a) Skills for affect and interpersonal regulation
b) Learning and practice of coping, relaxation, and grounding techniques
c) Psychoeducation
d) Cognitive coping techniques, thought stopping, and attention shifting
e) Provides opportunity for consumer and clinician to build a therapeutic alliance
f) Makes use of spirituality and safe connections

63
Phase One: Safety and Stabilization (cont’d)
Managing Emotions
Affective education and regulation
Grounding techniques
Breathing retraining
Progressive muscle relaxation
Imagery
Self-talk
Containment and distraction
64
Phase One: Safety and Stabilization (cont’d)
Feeling Identification
Identification of affect and intensity
Labeling feelings
Identification of connection between feeling, thoughts, and behaviors
Identification of how consumers experience distress, such as
Body: where the distress is located in their bodies. (Those who dissociate don’t necessarily experience distress this way.) Sense of body in space.
Racing thoughts
Grounding
Necessary first step for affect regulation and active coping
Early, temporary way to manage and contain overwhelming feelings by focusing on a specific sensory pathway for containment

65
Commonalities of Phased Trauma Treatments
2. Remembrance and mourning—provides some form of exposure therapy whereby traumatic events are recalled and cohesively assembled. This phase helps end cycle of PTSD (and is done when it is POST trauma). Exposure can include the following
a) Creation of trauma narrative
b) Processing and integration of traumatic experiences
c) Desensitization through repeated telling of trauma story and/or exposure to fears or aspects avoided
d) Addressing 1 & 2 distorted cognitions
66
Commonalities of Phased Trauma Treatments
3. Reconnection—emotions and cognitions revealed during the exposure phase are examined; treatment moves beyond trauma experience and is connected to consumer’s interpersonal life
a) Identification and modulation of cognitive distortions
b) Meaning making
c) Processing and integration of trauma experience
d) Preparation for returning to daily life
e) Coping with real losses as a result of the trauma(s)

67
Shared Characteristics of EB and Promising Practices
Function as service components within systems of care
Are provided in the community
Utilize natural supports and partner with families, with training and supervision provided by those with formal training
Operate under the auspices of all systems serving children, adults, and families
Integrated with other treatment interventions
Recovery-oriented focus

68
Secondary Traumatic Stress (Overview)

69
Secondary Traumatic Stress
Secondary Traumatic Stress is a natural, normal, potential effect of empathic engagement with a traumatized person.
Doing our job puts us at risk for secondary trauma.

70
Different Levels of Effects
First order Effects—Lower level
Belief systems
Personal control and invulnerability
Personal competence
Live in a just and benevolent world
Goodness of others
Higher level—Effects mimic typical PTSD symptoms
Re-experiencing
Numbing/arousal
Hyperarousal
71
Risk Factors
Degree of Exposure—(thought to be the primary risk factor)
qualitative and quantitative/cumulative
Intensity of work demand/stress overload
Personal history of trauma
Lack of social support/isolation
Punitive work environment
Lack of appropriate and supportive supervision
Exposure to acts of terrorism and violence outside of work

72
Protective Factors: Systemic, Professional, Personal
Self-awareness
Self-nurturance
Escape (not trauma avoidance!)
Humor
Active Coping
Connection—Support
Meaning Making
Transformation

73
Enact Balance
Outlays of Energy
… Balanced by …
Replenishment of Energy
Image: Balance scale
(Mary Jo Barrett, 2009)
74
Personal Self-Care Within the Workplace
Pacing—time management skills
Build in time to talk to colleagues and have a collegial support system in place
Build a personal sense of safety and de-stress: take breaks—even for a few minutes at a time, eat lunch, walk, breathe, don’t answer every call immediately, flowers in office, music you like
Utilize supervision and crisis help
Managing and tolerating the strong effects raised in the course of this work
Review your caseload—how many consumers have trauma histories? Can changes be made moving forward?

75
Personal Self-Care Outside the Workplace
Consider therapy for unresolved trauma, which the therapeutic work
may be activating
Practice stress management through meditation, prayer, conscious
relaxation, deep breathing, and exercise
Keep in contact with trusted others
Engage in hobbies and enjoyed activities
Get quiet time
Develop a written plan focused on maintaining work–life balance
76
Contact Information
Paula G. Panzer, M.D.
Jewish Board of Family and Children’s Services
New York, N.Y.
Center for Trauma Program Innovation
Martha K. Selig Educational Institute
www.jbfcs.org
Eric Arauz, MLER Arauz Inspirational Enterprises
Eric Arauz, MLER

78
The Trauma of Delusions
Image: Pablo Picasso’s “Guernica”

79
Image: Man being attacked by shark
…this led to a lifelong phobia of sharks.
While in a manic episode, a man had a recurring delusion of a shark attack…
80
The Blasphemy of Mania
Image: “Man of Fire,” Jorge Orozco

81
Religious Feeling Emulates Sickness
Mental illness has stolen God from me …
82
Recovery
“The patient must find the courage to direct his attention to the phenomena of his illness. His illness must no longer seem to him contemptible, but must become enemy worthy of his mettle, a piece of his personality, which has solid ground for its existence, and out of which things value for his future life have to be derived.” —Sigmund Freud (from Trauma and Healing, Dr. Judith Herman)

83
“Art, not psychology, is the language of emotions.”
Critique of Religion and Philosophy (1958), Walter Kaufmann
Image: “The Madhouse,” Francisco de Goya
84
Language of Madness
Language of the heart: addiction
Alternative to clinical language
Feel versus logic
Subjective versus objective

85
Frankenstein (1818), Mary Shelley: Created by doctors; conscious of his otherness to society; stigmatized as monster
Diary of a Madman (1835), Nikolai Gogol: Narrative of delusions; elucidates the progression of madness
Hamlet (1603), William Shakespeare: Duality of mind; aware that thought may not be sound
The Metamorphosis (1915), Franz Kafka: Experience of turning into something your family fears and does not understand; what it can feel like after hospital
“Freak on a Leash” (1998), Korn: “Something takes a part of me, Something lost and never seen, Every time I start to believe, Something’s raped and taken from me, from me”; hyperarousal of biological disease
Resources for Practitioners

86
President, Arauz Inspirational Enterprises LLC
Adjunct Instructor, Psychiatry: Robert Wood Johnson Medical School
Special State Officer, N.J. Governor’s Council on Alcoholism and Drug Abuse
New York Times Contributor
International Trauma Trainer
2009 SAMHSA/U.S. Department of Health and Human Services “Voice Award” recipient for National Advocacy
Lecturer at SAMHSA, NASMHPD, Yale University, Purdue University, Bristol–Myers Squibb, etc.
Featured on ABC’s Good Morning America “Now–Mind and Mood” special
Keynote 2010 American Psychiatric Nurses Convention in Louisville, K.Y.; numerous national keynotes
Disabled American veteran who served in U.S. Navy in Operation Desert Shield
Eric Arauz, MLER

87
Contact Information
Eric Arauz, MLER
www.ericarauz.com

88
Q&A, Discussion, and Summary
To ask a question, click on the Q/A tab and type your question in the window that opens, or press *1 for the operator, who will take your question in the order in which it is received.
Larry Davidson, Ph.D.
Project Director, Recovery to Practice
DSG, Inc.
Thanks for joining our Webinar today!
Image: Photo of Larry Davidson, Ph.D.

89
Downloads & Contact Information
For a copy of today’s presentation, visit the RTP Resources Center:
www.dsgonline.com/rtp/resources.html
To join the RTP ListServ, visit http://www2.dsgonline.com/rtp_listserv
… or contact us at