January 2007 Clinical Cases. BACKGROUND A 57-year-old man presents to a local emergency department...
7
January 2007 Clinical Cases
-
Upload
hortense-flynn -
Category
Documents
-
view
212 -
download
0
Transcript of January 2007 Clinical Cases. BACKGROUND A 57-year-old man presents to a local emergency department...

January 2007
Clinical Cases

BACKGROUND• A 57-year-old man presents to a local emergency
department with severe abdominal pain after being evacuated from a cruise ship. The pain, which is most severe in the right lower portion of his abdomen, started soon after he boarded the ship 2 days ago. Since then, the pain has worsened, and the patient has noticed his abdomen becoming progressively "bloated." The pain is associated with nausea and vomiting. He has not been able to have a bowel movement.
• On further questioning, the patient reports having night sweats, low-grade fevers, intermittent abdominal discomfort with constipation, and a 30-lb weight loss over the last 2-3 months. He has no significant medical history and is not taking any medications.
• He does have a significant family history of colon cancer, soft tissue sarcoma, pancreatic cancer, chronic myeloid leukemia (CML), and prostate cancer.

BACKGROUND
• On physical examination, the patient is alert and oriented. His temperature is 98.8°F, his pulse is 65 beats per minute, his respiratory rate is 18 breaths per minute, and his blood pressure is 104/67 mm Hg.
• Abdominal examination reveals localized tenderness to palpation in the right lower quadrant (RLQ), with a palpable mass. He has generalized abdominal distension but no guarding, rebound, or percussion tenderness.
• Rectal examination reveals guaiac-positive, brown stool. • Findings from the respiratory and neurologic portions of
the physical examination are unremarkable.

BACKGROUND
• Laboratory investigations are ordered and reveal a
Hemoglobin value of 9.4 g/dL, with a corresponding hematocrit of 30.8%.
His WBC count is 6.2 X 109/L, and
his lactate dehydrogenase (LDH) level is elevated at 285 U/L.
Results of an electrolyte panel, liver function tests, and renal function tests are within normal limits.

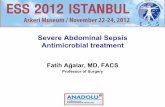
Abdominal CT is performed, which demonstrates a large right lower quadrant mass (see Image).
The mass causes a small-bowel obstruction, and several enlarged retroperitoneal and mesenteric nodes are noted (not pictured).
FNAC CONFIRMS THE DIAGNOSIS

What is the likely etiology of this mass?
• Diffuse, large B-cell lymphoma (DLBCL): Needle biopsy of the RLQ mass revealed a DLBCL involving the intestinal wall.

How would you treat this?• After diagnosis, the patient received a round of CHOP
chemotherapy, which consists of vincristine, doxorubicin, prednisone, and cyclophosphamide (nitrogen mustard), along with dexamethasone (Decadron) and granulocyte colony-stimulating factor (G-CSF).
• Prophylactic surgery to remove the RLQ mass was scheduled because of the relatively high risk of ileocecal bowel perforation during and after chemotherapy because of the lymphoma's extensive infiltration of the entire bowel wall, as seen on CT. The preoperative diagnosis was non-Hodgkin lymphoma (NHL), ie, DLBCL of the small bowel. After surgery, lymphoma to the terminal ileum, right colon, and mesentery of the small bowel were confirmed. The terminal ileum and proximal right colon were resected, and an ileocolic anastomosis was made.