Jacqueline Claydon February 2014 Clinical Research Associate awarded by CLRN 2013.
17
Rehabilitation after orthopaedic major trauma Jacqueline Claydon February 2014 Clinical Research Associate awarded by CLRN 2013
-
Upload
xavier-castillon -
Category
Documents
-
view
217 -
download
2
Transcript of Jacqueline Claydon February 2014 Clinical Research Associate awarded by CLRN 2013.

Rehabilitation after orthopaedic major trauma
Jacqueline Claydon February 2014Clinical Research Associate awarded by CLRN 2013
Orthopaedic Trauma Rehab Clinic
To use the rehabilitation prescription to improve patient care
Pilot: May – November 2013◦ n=143, mean 5.0 months
Physiotherapy-led consultation◦ Subjective and clinical assessment of all injuries◦ Reassess Rehabilitation Prescription◦ Set Rehabilitation Goals
Refer to clinical and rehabilitation services
Qualitative Research◦ Patient perception of recovery and rehabilitation after orthopaedic major trauma, n=15

Harry’s story
Background
Male, 63, working Fall from a height Major Trauma bypass
0
10
20
30
40
16 to 24 25 to 34 35 to 44 45 to 54 55 to 64 65 to 74 75 to 84 85 +
9 1010
18 20
11 1110
11 9 1117 17
13 13 10Perc
enta
ge, %
Age, years
Non-ortho Ortho
28
18
55RetiredNot work preWorking
Work Status % (Ortho)
Age distribution, %
Want to go back to work, I’ve
worked all my life

Mechanism
Motorbikes: 14%
Fall from height: 22%
Slips, trips and falls: 30% Sports: 6%
Road accident: 15%
Bike: 4%
Assault: 1%
Industrial: 1%
Pedestrian: 8%
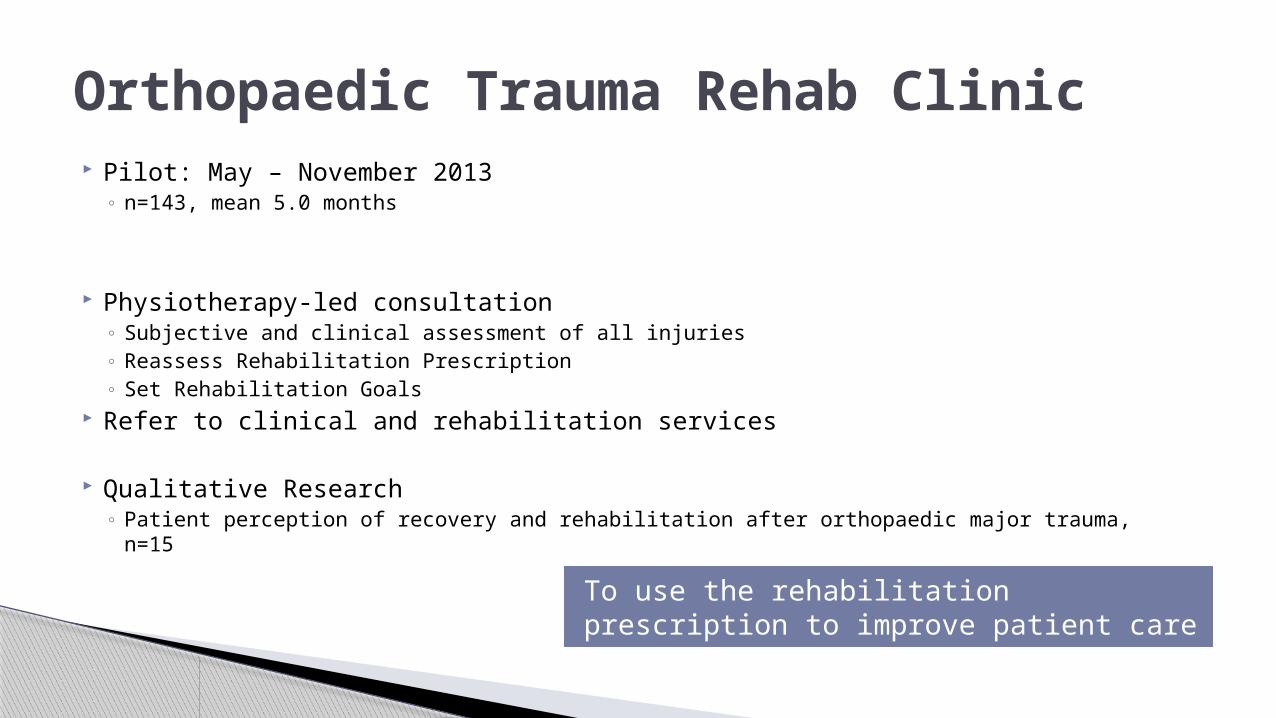
Harry’s injuries
Clinical database, n=692
Orthopaedic: ◦ Pilon fracture ankle
Spanning ex-fix; ORIF Non weight-bearing 3 months
◦ T12 wedge fracture: conservative
ISS 13 ◦ Level 1 All 42% (Ortho 26%)◦ Level 2 All 34% (Ortho 11%)
Ortho48%Neuro
26%
Spines17%
Rehabilitation PrescriptionsOrtho
General
Burns
Neuro
Other
Max Fax
Plastics
Resp
SCI
Spines
ISS does not reflect functional limitations

Inpatient Rehabilitation Needs
n=143
Initial
Mobility 97%
IADL 79%
Wound management 73%
Pain 95%
Environment 50%
Vocation/Education 21%
Urinary incontinence 14%
Nutrition 7%
Ventilator / Pulm rehab 2%
Mood 4%
Other
Upper limb function 6%
Falls/balance 1%
Sports / hobbies 1%
◦ Physiotherapy◦ OT◦ Nurse◦ Orthopaedics◦ Pain team
Rehabilitation Prescription
They were so good
everybody, right through, the
doctors as well
Discharge home with equipment and carer support ◦ 7 days after injury
Minimal mobility◦ Non weightbearing, zimmer frame
Fracture clinic follow up◦ Physio referral when weightbearing status changes
Trauma Rehab clinic
Discharge planning

Rehabilitation Reality
Environmental issues◦ Not able to manage in own home
Partner’s bungalow◦ Stuck in the house
Wheelchair from the red cross
Fracture complications◦ Osteopenia:
Referred for urgent physio to commence weightbearing
Accessing physiotherapy Geographic issues
Not accept referral from MTC Different health authority than usual
residence (although he pays his Council Tax there)
No capacity for urgent referrals
we rang the Red Cross, and uh, they said yes, and that’s the best, it was twenty pound to hire it, and that’s the best twenty pound I
ever, ever spent
If you hadn’t rung that day and stepped in, I still mightn’t be
getting physio
“…. It got us really down, you know. Got us really down. I know I need physio, why can’t I have it?
…..and I felt is it because I’ve got a Hospital C consultant and Hospital O won’t look after us ….”
I just thought, why
can’t everybody
get together
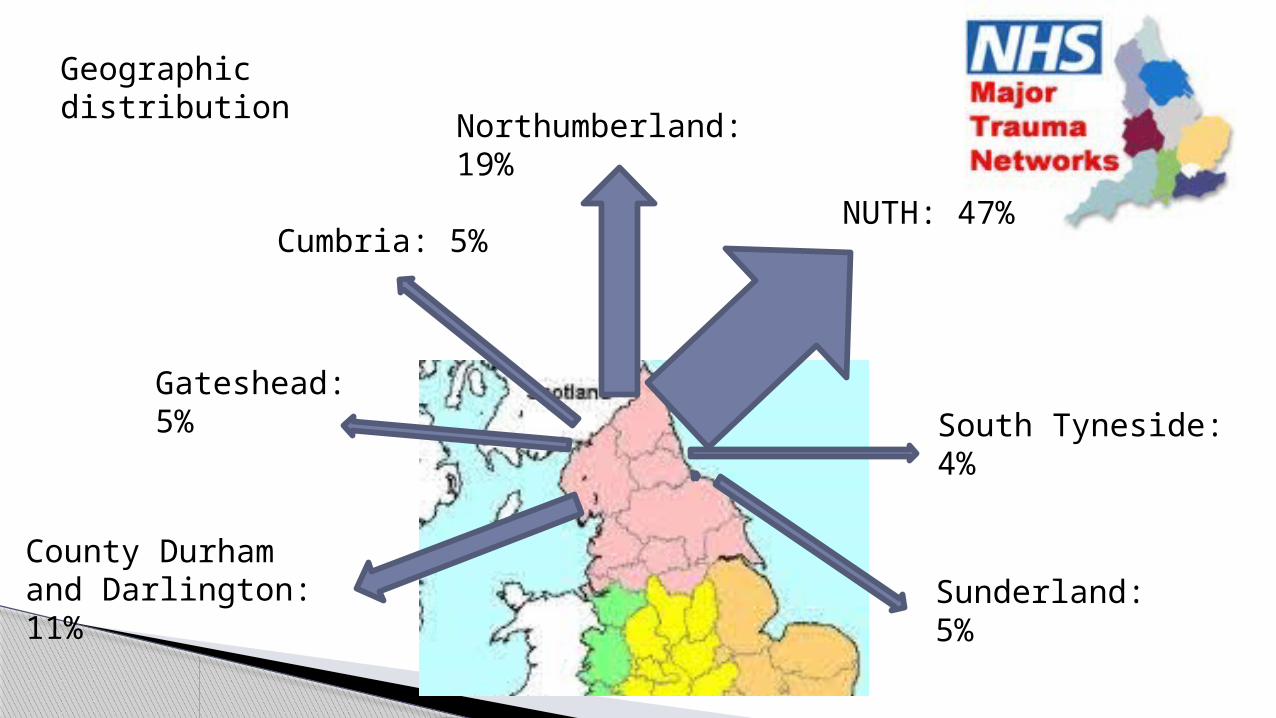
South Tyneside: 4%
Sunderland: 5%
Cumbria: 5%
Gateshead: 5%
Northumberland: 19%
NUTH: 47%
County Durham and Darlington: 11%
Geographic distribution
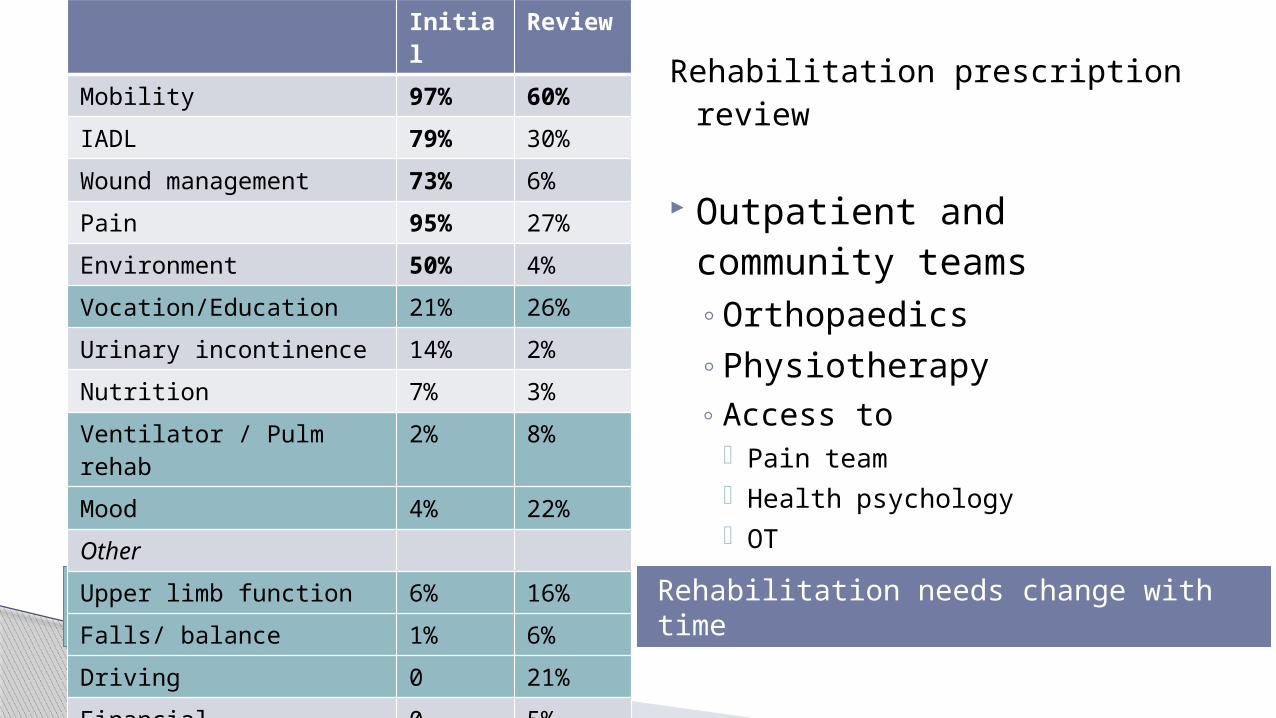
Increase at review Rehabilitation needs change with time
Initial Review
Mobility 97% 60%
IADL 79% 30%
Wound management 73% 6%
Pain 95% 27%
Environment 50% 4%
Vocation/Education 21% 26%
Urinary incontinence 14% 2%
Nutrition 7% 3%
Ventilator / Pulm rehab 2% 8%
Mood 4% 22%
Other
Upper limb function 6% 16%
Falls/ balance 1% 6%
Driving 0 21%
Financial difficulties 0 5%
Sports / hobbies 1% 4%
Rehabilitation prescription review
Outpatient and community teams◦Orthopaedics◦Physiotherapy◦ Access to
Pain team Health psychology OT
Trauma Rehab clinic
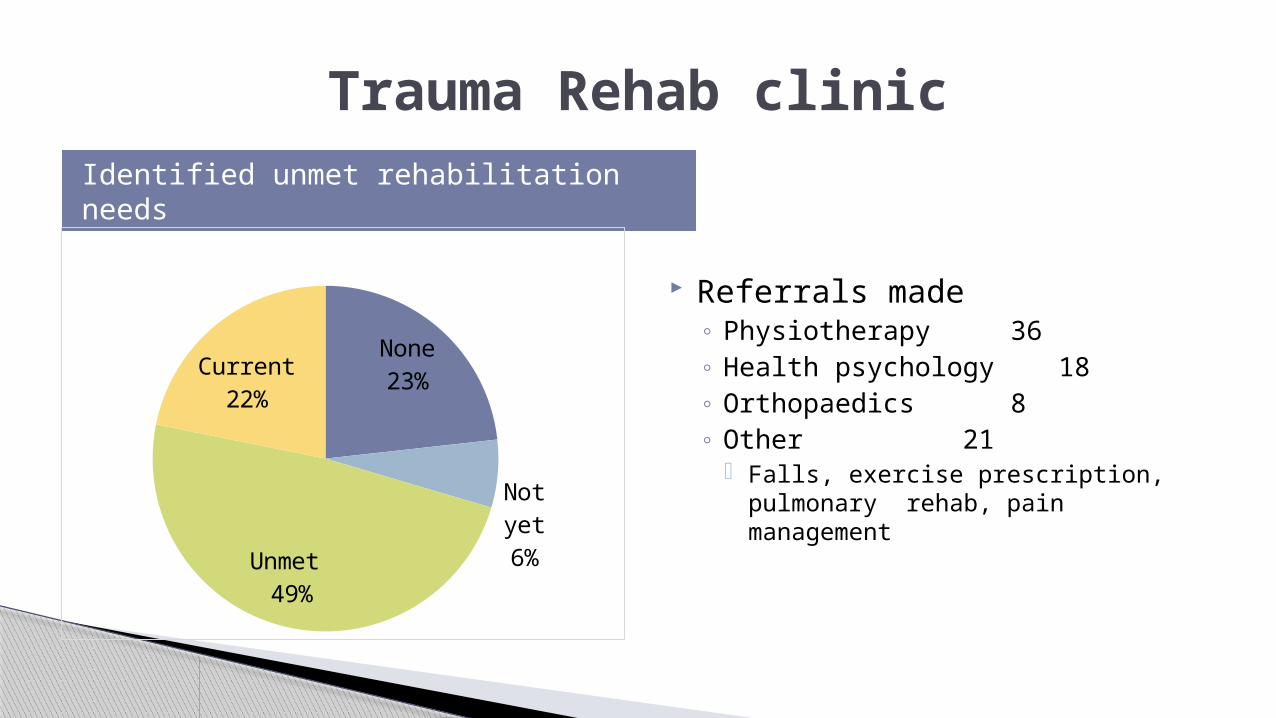
Identified unmet rehabilitation needs
None23%
Not yet6%
Unmet 49%
Current22%
Referrals made ◦ Physiotherapy 36◦ Health psychology 18◦ Orthopaedics 8◦ Other 21
Falls, exercise prescription, pulmonary rehab, pain management
Trauma Rehab Clinic
Rehabilitation needs change with time
Rehabilitation needs change with time ◦ Trauma rehab clinic effectively identifies
current multidisciplinary needs
Improved co-ordination and communication between existing services◦ Virtual team
Raised awareness: inequalities of rehabilitation provision
I felt like I was being treated as a person
No-one had set any goals, think it will help me move forward
I was surprised I’d not been
seen

Newcastle Clinical AHP group◦ Improving co-ordination and communication between local teams
Regional AHP clinical conference◦ Clinical skills◦ Start to build regional network
Research: patient perceptions of recovery and rehabilitation after orthopaedic major trauma◦ Data analysis completion May 2014
What’s next…
I’ve got to be honest. I didn’t think it
would take as long. You think you’re like, I’ll be back in work in
four or five weeks. It’s hard to grasp

“Changed me outlook on life. Live for tomorrow, ‘cause you never know what’s going to happen” Harry, 2013

Major Trauma Rehabilitation
Rehabilitation Prescription