Anatomiaestiramientos 130305111855 Phpapp02 140129215950 Phpapp02
Upload
maisa-abukhalilCategory
view
74download
0
Physician’s Training Module
Dr. Sarwat JabeenMBBS, MBA Health Management & Pharmaceutical Marketing
Product Manager – Fertility

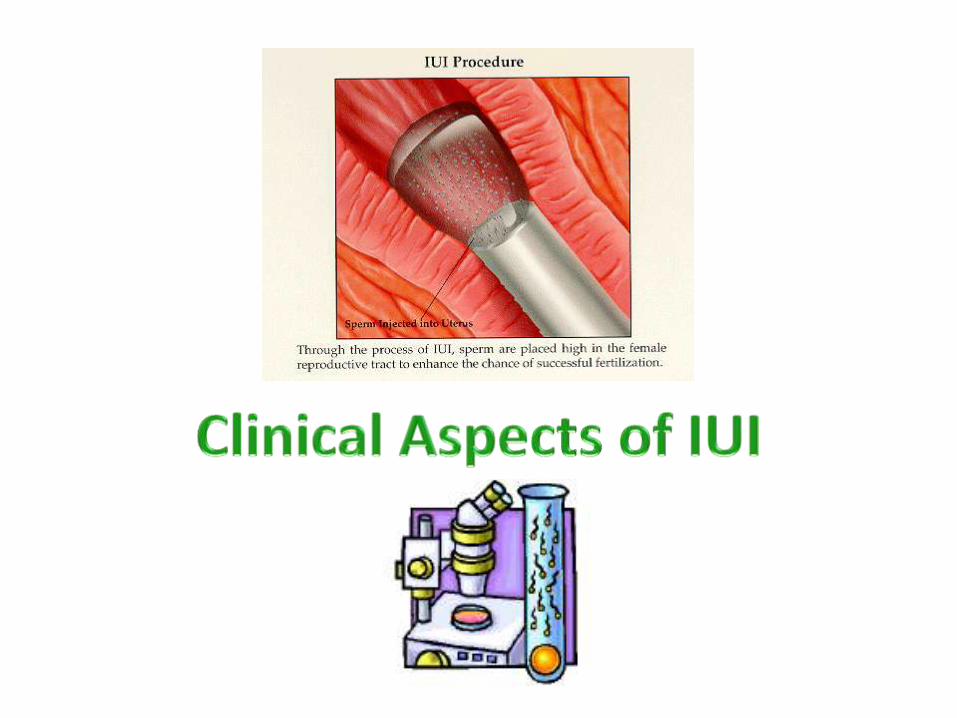
Intrauterine insemination (IUI) is a form of treatment where sperm are inserted into the uterine cavity around the time of
ovulation.
IUI can be carried out in a natural cycle, without the use of drugs, or the 5 ovaries may be stimulated with oral anti-
estrogens or gonadotrophins.
1. NICE Guidelines - 2012
The procedure allows one to bypass the cervix to deposit spermcloser to tubal ostium, thereby facilitating a larger number of motilesperms to reach the fertilization site in the ampulla of fallopiantube.
In addition, the sperm separation procedure would remove WBC,dead and moribund sperms generating free oxygen radicals whichreduce the functional capacity of intact sperms.
Components in the media also induce gentle capacitation of spermwhich is necessary to make them functionally ready for fertilization.
Controlled ovarian stimulation is often used in conjunction with IUItreatment which also enhances the chance of pregnancy byinducing multiple ovulation.

Where drugs are used to stimulate a cycle, in the case of oral anti-estrogens a woman will take a course of tablets for 5 days.
With gonadotrophins (E.g. rFSH-Puregon) the woman usuallyreceives a course of daily fertility injections for 7 to 10 days.
However, the exact duration of stimulation will depend on whichday of the cycle it is started.
In both circumstances the treatment should be monitored byultrasound scan to assess the ovarian response.
1. NICE Guidelines - 2012

When one to three follicles are seen to have developed to asuitable size, usually with one dominate follicle, then an injection ofhCG is given which triggers ovulation.
Insemination of prepared sperm will be undertaken 24 to 36 hourslater. However, in order to reduce the risk of multiple pregnancies ifmore than three follicles have developed or two or more maturefollicles are seen then insemination may not be undertaken.
1. NICE Guidelines - 2012

Go to following Youtube link for 3D animation on how IUI works:http://www.youtube.com/watch?v=qCdIiLLF0vw

Unexplained infertility
Mild endometriosis
Mild male factor infertility
Disability (physical or psychological) preventing vaginal sexualintercourse
Conditions that require specific consideration in relation tomethods of conception (such as after sperm washing in a couplewhere the male is HIV positive)
Fertility preservation
As part of donor insemination
IUI in stimulated cycles may be considered while waiting for IVF, orwhen in women with patent tubes IVF is not affordable.
1. NICE Guidelines – 2012. 2. Human Reproduction Update, Vol.15, No.3 pp. 265–277, 2009. IUI – The ESHRE Capri Workshop Group
IUI is contraindicated in women with:
Cervical atresia
Cervicitis
Endometritis
Bilateral tubal obstruction
In most cases of amenorrhea or severe oligospermia
1. Human Reproduction Update, Vol.15, No.3 pp. 265–277, 2009. IUI – The ESHRE Capri Workshop Group

Female age <40 years
Minimum of 1.5 years of infertility
Patent fallopian tubes confirmed by laparoscopy /hysterosalpingogram
Presumptive proof of ovulatory cycle
Ultrasound evidence of mature follicles & ovulation
Luteal phase progesterone (P) cutoff >35 nmol/L
Male partner:
Two semen analysis revealing at least 10 million recovered motilesperm / whole sample
Patient with any of the following diagnosis could beconsidered for IUI treatment:
Unexplained infertility
Male factor
Immunological factors
Cervical factors

Proper indication
Satisfactory semen analysis
Patent, healthy fallopian tubes
Need to increase FSH threshold in early follicular phase with eitheroral ovulation inducing agent and / or injections of exogenousgonadotropin preparations (E.g. Puregon)
Identify or preempt the spontaneous LH surge
Detailed clinical history of both partners
Counseling for IUI procedure
Detail explanation of the technique, risk, complications and expectedoutcome.
Examination of the Female Patient
Physical examination and local
Transvaginal Sonography
Day-21 serum progesterone
Tubal assessment by laparoscopy / hysterosalpingogram
If the patient has got irregular menstruation – baseline hormonesshould be done

Poor results have been described when IUI was performed in natural cycles forunexplained and cervical factor.
The rationale behind the use of ovarian hyperstimulation in artificialinsemination is the increase of the number of oocytes available for fertilizationand to correct subtle unpredictable ovulatory dysfunction.
Drugs for OI in IUI:
Oral
Anti-estrogens (Clomiphene Citrate – Ovafin®) 50 – 100 mg for five days
Aromatase Inhibitors (Letrozole) 2.5 – 7.5 mg for five days
Injectables
hMG 75 – 150 mg / day from day 3 – 7 of cycle
FSH – uFSH or rFSH (E.g. Puregon®) 75 – 150 mg / day from day 3 – 7 of cycle
hCG (E.g. Pregnyl®) 5000 – 10,000 IU for follicle puncture and to timeinsemination
1. Human Reproduction 2008. Intrauterine insemination (IUI) as a first-line treatment in developing countries and methodological aspects that might influence IUI success. 2. Ovarian stimulation protocols (anti-oestrogens, gonadotrophins with and without GnRH agonists/antagonists) for intrauterine insemination (IUI) in women with subfertility (Review). Copyright © 2011 The Cochrane Collaboration.

The drugs for OI in IUI – A Comparison:
Intra-uterine insemination combined with OH has been proven effective forcouples with unexplained and mild male factor subfertility.
Compared with IVF, IUI with OH is less invasive and more cost-effective .
Antiestrogens Vs. Gonadotropins
In the 2007 Cochrane review of seven trials, the results demonstrated that in an IUIprogram, ovarian stimulation with gonadotrophins increases pregnancy rates percouple significantly, compared to anti-oestrogens, without effecting adverseoutcomes.
Antiestrogens Vs. Aromatase Inhibitors
In the 2007 Cochrane review of five studies, None of the trials solely or incombination provided convincing evidence of a significant difference.
1. Ovarian stimulation protocols (anti-oestrogens, gonadotrophins with and without GnRH agonists/antagonists) for intrauterine insemination (IUI) in women with subfertility (Review). Copyright © 2011 The Cochrane Collaboration.

1. WHO 2010 laboratory manual for the Examination and processing of human semen
WHO Reference Values Reference Limit
Semen volume (ml) 1.5
Sperm concentration (106/ml) 15
Total sperm number (106/ejaculate) 39
Progressive motility (PR, %) 32
Total motility (PR +NP, %) 40
Vitality (live sperms, %) = / > 58
Sperm morphology (NF, %) = / > 4
pH* = / > 7.2
Leucocyte* (106/ml) <1
MAR/Immunobead test* (%) <50
Screening for anti-sperm antibodies should not be offered because there isno evidence of effective treatment to improve fertility.
If the result of the first semen analysis is abnormal, a repeat confirmatorytest should be offered.
Repeat confirmatory tests should ideally be undertaken 3 months after theinitial analysis to allow time for the cycle of spermatozoa formation to becompleted. However, if a gross spermatozoa deficiency (azoospermia orsevere oligozoospermia) has been detected the repeat test should beundertaken as soon as possible.
Concerning the insemination sample, the recommended lower limit rangesfrom 3 million motile sperm to 5 million to 10 million
The routine use of post-coital testing of cervical mucus in the investigationof fertility problems is not recommended because it has no predictive valueon pregnancy rate.
NICE Guidelines 2013
The semen is a mixture of motile and dead spermatozoa with cells, cellulardebris and sometimes micro-organisms present.
Prior to IUI, it is necessary to remove seminal plasma to avoidprostaglandin-induced uterine contractions.
Insemination with unprocessed semen is also associated with pelvicinfection.A variety of methods have been developed to separate the motile spermsfrom the ejaculate. The most common methods are washing andcentrifugation which has been shown to cause some damage to the sperm.
Simple sperm washSwim upGradient
All preparations should done in a laminar flow for sterility.The clean sperm suspension is used for IUI, IVF and ICSI and certain specialsperm tests.
1. Human Reproduction Update, Vol.15, No.3 pp. 265–277, 2009. IUI – The ESHRE Capri Workshop Group. 2. WHO 2010 laboratory manual for the Examination and processing of human semen

Simple Sperm Wash
This method is used if the semen sample is very poor. It mainly removesseminal plasma from the sperms.
One volume of semen is placed in a 15 ml test tube and diluted with 2volume of culture medium. The tube is gently inverted twice to mix thecomponents.
The tube is then centrifuged at 250-300g for 5-7 min.
The supernatant is removed and the pellet is re-suspended in 2 ml ofculture medium.
The centrifugation is repeated at 250-300g for 5-7 min and the supernatantremoved. About 0.4 ml of media is added to the final sperm pellet for re-suspension.
The sample is suited for intra-cervical insemination
WHO 2010 laboratory manual for the Examination and processing of human semen

Swim Up Method
This technique relies on the ability of the sperms to swim. This method issuitable for semen with high to moderate motility.
Semen is diluted with 1:2 ratio of culture medium and centrifuged at 250-300g for 5-7 min.
The supernatant is removed leaving the pellet.
Pipette 0.8-1 ml of media into a new test tube. Carefully layer the semenpellet beneath the media.
Stand at 37o for 45-60 min. Placement of tube at 45oangle creates a largersurface area for sperms to swim-up.
Carefully take up the top 0.5-0.6 ml without disturbing the lower layer andtransfer into a new test tube.
To concentrate the sperms, pooled several tubes and centrifuged at 250-300g for 5-7 min. The supernatant is removed and the resultant pellet re-suspended in 0.4 ml of media.
WHO 2010 laboratory manual for the Examination and processing of human semen
Gradient Systems
Gradient systems use solutions with a higher density than semen toseparate the debris, cells, micro-organisms and non-motile sperms from themotile ones.
Commercially available dense solutions used are colloidal silica (Percoll,Puresperm), poly-sucrose (Ficoll, Ixaprep) and other dense solutions(Optiprep, Nycodenz).
Centrifugal force is applied to enable the motile sperms to swim from a lessdense seminal fluid into a denser solution.
Cellular debris and non-motile microorganisms will be trapped at theinterphase between the two solutions
Select more normal sperms than swim up method.
Recovery may be poor in viscous semen and severe teratozoospermia (smallheads but good swimmers)
WHO 2010 laboratory manual for the Examination and processing of human semen
Quality of the Specimen
• There is no consensus on a lower limit of semen quality at which one would advocate ICSI rather than IUI.
• It has been reported that pregnancy rates are lower if the semen sample contains ,10 million sperm in total.
• Concerning the insemination sample, the recommended lower limit ranges from 3 million motile sperm to 5 million to 10 million.
Human Reproduction Update, Vol.15, No.3 pp. 265–277, 2009. Intrauterine insemination. The ESHRE Capri Workshop Group.

• The sperm suspension can be deposited in the cervix, the uterus, theperitoneum or the Fallopian tube.
• IUI is by far the most common method.
• It is performed by introducing a 0.2–0.5 ml sperm suspension into theuterus with a small catheter, usually without imaging guidance.
• With Fallopian tube sperm perfusion (FSP), the inseminate is 4 ml, so thatwith this large volume of fluid the inseminate may fill not only the uterinecavity and Fallopian tubes, but also some of the volume may even end upinside the peritoneal cavity.
• For frozen semen, IUI is better than intracervical insemination (ICI): thelikelihood of live birth after six insemination cycles is 2-fold higher (OR:1.98; 95% CI: 1.02–3.86) (Besselink et al., 2008).
Human Reproduction Update, Vol.15, No.3 pp. 265–277, 2009. Intrauterine insemination. The ESHRE Capri Workshop Group.

• In two trials among patients with unexplained infertility, results with FSPwere better than with IUI (Kahn et al., 1993; Cantineau et al., 2003).
• For other indications, there is not sufficient data to suggest that FSP is anybetter than IUI.
Human Reproduction Update, Vol.15, No.3 pp. 265–277, 2009. Intrauterine insemination. The ESHRE Capri Workshop Group.
• Insemination can be done at various time points around ovulation and canbe done once or several times.
• In the majority of the published studies, the insemination is done 32–36 hfollowing hCG administration.
• It is assumed that the timing of insemination relative to ovulation is criticalfor an optimal success rate.
• A systematic review found no difference in the pregnancy rate per couplewith two inseminations compared with one (Cantineau et al., 2003).
Human Reproduction Update, Vol.15, No.3 pp. 265–277, 2009. Intrauterine insemination. The ESHRE Capri Workshop Group.

IUI in an Office Setting
IUI is done as an office procedure by gynecologists in private practice.
They use the services of the nearby ultrasound centers for follicular trackingand of specialized IUI laboratory for sperm preparation.
In case of any complication, patients are transferred to a specializedhospital.
Good coordination between gynecologist, sonology lab and IUI lab isrequired to make this setup successful.
IUI within a General Hospital
IUI is done by gynecological consultants.
Laboratory and ultrasound services are available in respective departmentsfor follicular tracking and semen preparation.
Disadvantage is sonologist may not have adequate training in folliculartracking and semen preparation in a general laboratory may result insuboptimal results.
IUI within an IUI Clinic
All IUI services re provided under one roof.
Initially the unit may start only as IUI clinic but may later commence othertreatments of ART.
This should be kept in mind when planning IUI clinic so that space forexpansion to create a future ART center in same premises is available.
IUI within ART Center
This IUI setup is in a specialized ART laboratory.
The appropriate equipments, media, drugs and staff are already in placeand no separate requirements need to be filled.
Room for IUI Laboratory
The room should be as close as possible to procedure room.
The room must have its own air conditioning.
There must not be any free access to any toxic fumes.
Sufficient space to accommodate necessary equipments.
During insemination it is vital that clinician is able to communicatewith lab personnel.
There must be suitable facilities for sperm preparation.

1. Semen Assessment & SpermPreparation
Meckler counting chambers
Microscope phase contrastmicroscope with resolving power4,10,40,100 with eye piece 10x.
Centrifuge machine with swing-outrotor, timer and RPM meter
5% CO2 incubator with 37C withgas cylinder
Laminar flow hood (horizontal /vertical)
Wide mouth sterile semencollecting jar
Integrated Laminar FlowIUI Workstation

2. Semen Assessment & Sperm Preparation
Sterile test tubes
Sterile conical / round bottom tubes
Pipette
Pipette pump
Test tube rack
Media
Good light source
CASA system
CASA System

3. Gynecological Equipment
Cusco’s speculum
IUI catheter
1 ml syringe
Uterine sound
Cervical dilator 5/6 mm
Tenaculum single toothed
OT light
Ultrasound machine with transvaginal probe
4. Media
Flushing media
Culture media
Sperm preparation media
Cryopreservation media
5. Record Keeping and Documentation
6. Maintenance of Equipment
Incubator should be checked daily in the morning for temperature
Internal water reservoir of the incubator should be cleaned regularly
Laminar flow should be cleaned periodically with 70% isopropylalcohol
Gas cylinder should be checked regularly to check for any leakage
7. Quality Control Methods & Laboratory Asepsis should be in place

Physical Structure & Floor Plan

1. Reception Enlistment Area
2. Waiting Area
3. Subfertility Clinic Area
4. Male clinic Area
5. Sperm Collection Room
6. Andrology Laboratory
7. Receiving area
8. Main laboratory

9. IUI Procedure Room
Patient bed
Cusco’s speculum
Disposable rubber sheet
Disposable per vaginal gloves
Swab holding forceps
Volsellum
10. Doctor’s Office
11. Transvaginal Ultrasonography Room

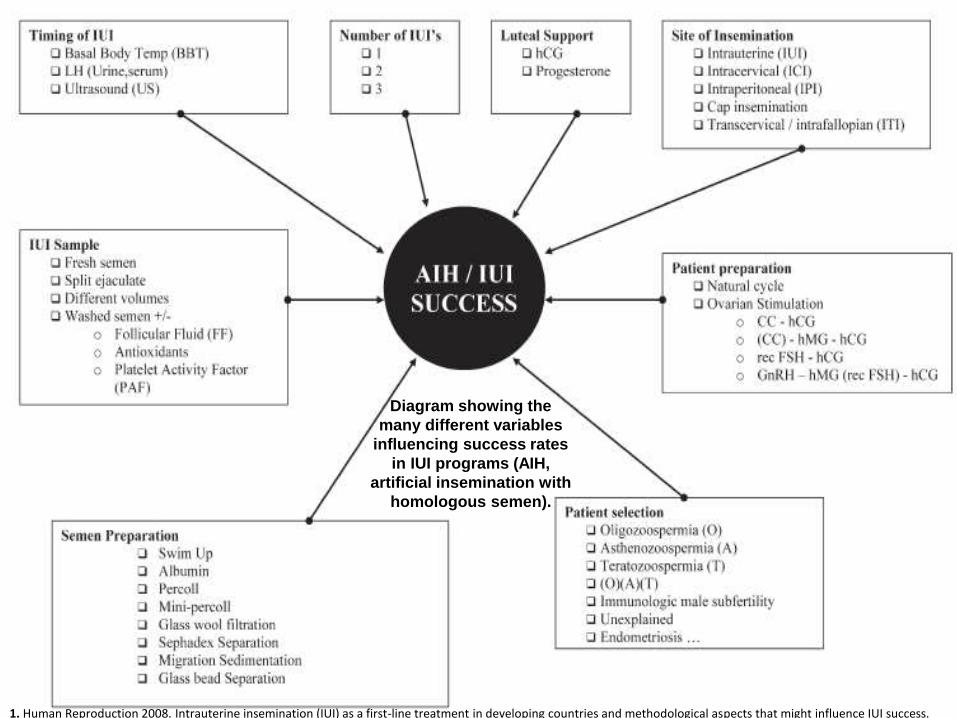
Diagram showing the
many different variables
influencing success rates
in IUI programs (AIH,
artificial insemination with
homologous semen).
1. Human Reproduction 2008. Intrauterine insemination (IUI) as a first-line treatment in developing countries and methodological aspects that might influence IUI success.
Age of the female
Indication for IUI
Use of controlled ovarian stimulation
The processed total motile sperm count in the inseminate
Practical Issues Involved in Enhancing Pregnancy Outcome inIUI
Duration of subfertility
Parity
Pre-IUI semen report
Number of IUI cycles attempted

Practical Issues Involved in Enhancing Pregnancy Outcome inIUI (contd.)
Number and size of dominant follicle
Blood estradiol concentration on hCG day
Endometrial thickness at scan on hCG day
Doppler blood flow studies of follicles / endometrium
Practical issues at IUI:Type of IUI catheter
Fresh or frozen-thawed sperm
Post-processing sperm morphology / motility grade
Timing of IUI in relation to hCG administration
Practical Issues Involved in Enhancing Pregnancy Outcome inIUI (contd.)
Practical issues at IUI (contd.):Number of IUIs
Volume of inseminate used
Time to rest following IUI procedure
1. For people with unexplained infertility, mild endometriosis or mildmale factor infertility, who are having regular unprotected sexualintercourse:
– do not routinely offer intrauterine insemination, either with orwithout ovarian stimulation
– advise them to try to conceive for a total of 2 years (including up to 1year before investigation) before IVF will be considered.
1. NICE Guidelines - 2012
2. Consider unstimulated intrauterine insemination as atreatment option in the following groups as an alternative tovaginal sexual intercourse:– people who are unable to, or would find it very difficult to have vaginal
intercourse because of a clinically diagnosed physical disability orpsychosexual problem who are using partner or donor sperm;
– people with conditions that require specific consideration in relationto methods of conception (for example, after sperm washing wherethe man is HIV positive)
– people in same-sex relationships.
1. NICE Guidelines - 2012

3. For people in recommendation 2 who have not conceivedafter six cycles of donor or partner insemination, despiteevidence of normal ovulation, tubal patency and semenanalysis, offer a further six cycles of unstimulated intrauterineinsemination before IVF is considered.
1. NICE Guidelines - 2012

• In good prognosis couples, the live birth rate is better withouttreatment.
• IUI is widely used with infertility diagnoses other thanbilateral tubal obstruction, severe male infertility and severeovulation defects.
• Differences in sperm preparation and IUI methodology do nothave profound effects on the success rate.
• Prior to using IVF, IUI with clomiphene ovarian stimulation isrelatively cheap and many couples will conceive and notrequire IVF.
Human Reproduction Update, Vol.15, No.3 pp. 265–277, 2009. Intrauterine insemination. The ESHRE Capri Workshop Group.
• IUI in stimulated cycles was effective only in patients withmore than 3 years duration of infertility but is associated witha significant rate of higher-order multiple births.
• Prevention of premature LH surges and luteal phase supportdo not appear major requirements in IUI cycles.
• Although IUI treatment is cheaper and less demanding on thepatient, IVF is the most effective treatment for infertility.
Human Reproduction Update, Vol.15, No.3 pp. 265–277, 2009. Intrauterine insemination. The ESHRE Capri Workshop Group.

NICE Guidelines 2012, 2013
Intrauterine insemination. The ESHRE Capri Workshop Group.Human Reproduction Update, Vol.15, No.3 pp. 265–277, 2009.
WHO 2010 laboratory manual for the Examination and processing of human semen
IUI Intrauterine Insemination By Chakravarty Mukherjee
Manual on IUI: What, When and Why By Nusrat Mahmud, Narendra Malhotra, MalhotraJaideep