its body. The floor of the optic canal projects posteriorly and the roof ...
33
FRACTURES OF THE ORBIT: THE DEMONSTRA- TION OF THE ORBIT BY PLANIGRAPHY (BODY SECTION RADIOGRAPHY)* ARTHUR M. CULLER, M.D. Dayton, Ohio With increasing frequency the ophthalmologist is called to see patients who have sustained trauma to the head. The discovery of a field defect, diplopia, ecchymosis, or proptosis arouses suspicion of fracture of the orbit, but the usual x-ray technique often fails to demonstrate the structures at the apex of the orbit. Only when optic atrophy develops several months after the injury does the ophthalmologist discover that serious damage has been done to the optic nerve. The damage is then irreparable. This article is the result of an effort to improve our diag- nostic armamentarium, first, by making a critical analysis of such clinical signs as have been found valuable to neurologists and surgeons, and, second, by a study of the visualization of the apex and walls of the orbit by x-ray. ANATOMY The orbit is roughly pyramidal in shape. Duke-Elder' gives the average dimensions of the orbital margin as: height, 35 mm.; width, 40 mm. The average depth is 40 mm. The interorbital width is about 25 mm.; the extraorbital width is about 100 mm. The optic canal is situated slightly medial to the apex of the orbit, and is formed by the fusion of the two roots of the lesser wing of the sphenoid with the side of its body. The floor of the optic canal projects posteriorly and the roof anteriorly. There is a great variation in the pneumatization and thick- * Candidate's thesis for membership accepted by the Committee on Theses. 348
-
Upload
truongthuy -
Category
Documents
-
view
215 -
download
0
Transcript of its body. The floor of the optic canal projects posteriorly and the roof ...

FRACTURES OF THE ORBIT: THE DEMONSTRA-TION OF THE ORBIT BY PLANIGRAPHY
(BODY SECTION RADIOGRAPHY)*
ARTHUR M. CULLER, M.D.Dayton, Ohio
With increasing frequency the ophthalmologist is calledto see patients who have sustained trauma to the head. Thediscovery of a field defect, diplopia, ecchymosis, or proptosisarouses suspicion of fracture of the orbit, but the usual x-raytechnique often fails to demonstrate the structures at the apexof the orbit. Only when optic atrophy develops severalmonths after the injury does the ophthalmologist discoverthat serious damage has been done to the optic nerve. Thedamage is then irreparable.
This article is the result of an effort to improve our diag-nostic armamentarium, first, by making a critical analysis ofsuch clinical signs as have been found valuable to neurologistsand surgeons, and, second, by a study of the visualizationof the apex and walls of the orbit by x-ray.
ANATOMYThe orbit is roughly pyramidal in shape. Duke-Elder'
gives the average dimensions of the orbital margin as: height,35 mm.; width, 40 mm. The average depth is 40 mm. Theinterorbital width is about 25 mm.; the extraorbital widthis about 100 mm. The optic canal is situated slightly medialto the apex of the orbit, and is formed by the fusion of thetwo roots of the lesser wing of the sphenoid with the side ofits body. The floor of the optic canal projects posteriorly andthe roof anteriorly.
There is a great variation in the pneumatization and thick-* Candidate's thesis for membership accepted by the Committee on Theses.
348

CULLER: Fractures of the Orbit
ness of the bony walls of the canal. The roof, or superiorroot of the lesser wing of the sphenoid, is fairly thick, andoccasionally contains air cells. Inferolaterally the inferiorroot of the lesser wing of the sphenoid is thin, and dehiscenceshave been reported by Le Double.2 This lower root sepa-rates the canal from the superior orbital fissure. On themesial wall it is separated from the sphenoidal sinus by a thinbony plate. Occasionally a posterior ethmoidal cell lies ad-jacent to it. The sphenoidal sinus varies greatly, and Whit-nall3 and Onodi4 cite cases in which the sinus surrounded thecanal. Onodi classified 38 different forms and 12 groups ofrelations of the sinuses to the optic canal.The anterior opening is the optic foramen. This is oval
in outline, with the long axis up and in. From a study of1,000 optic canals, Goalwin5 found that the average long axismeasures 4.65 mm., and the opposite ax:s, 4.1 mm. The nor-mal range he considered to be from 3 to 5.6 mm. He foundthe minimum cross section usually at the posterior end, al-though Keyes6 believed that this finding was very inconstant.The lateral inclination of the optic canal was 390 to bothhorizontal and median planes. Hartmann7 gave the horizon-tal angle as 35.5°, and Pfeiffer8 as 37°. Hartmann andPfeiffer agreed on a vertical angle of 300, although Pfeifferstated that this varies. Goa.win concluded that the canalattained adult size at the age of three, and that there was noappreciable variation with age, racial stock, or sex, but de-clared that an optic canal that measures less than 2.8 mm.in one of its diameters cannot contain a normal nerve.The length of the optic canal has been variously esti-
mated. Goalwin found the measurement from a perpendicu-lar dropped from the anterior end of the floor to a perpendic-ular dropped from the posterior end of the roof to varybetween 0 and 8 mm. Whitnall claimed that the length variesfrom 4 to 9 mm., and Onodi found that the canal may be aslong as 12 mm.
Goalwin examined his large series of skulls for symmetry,
349

CULLER: Fractures of the Orbit
and concluded that absolute symmetry of the optic canalsmay be expected in about 45 per cent. of normal skulls, dif-ferences of 10 per cent. or less in 40 per cent., and differencesof from 10 to 20 per cent. in 14 per cent. of normal skulls.An enlarged circular optic canal is indicative of tumor. Con-stricted triangular canals are characteristic of oxycephaly orother skull deformity. Any irregularity of any wall is alwayspathologic.The meninges covering the optic nerve are continuous with
those of the brain. The dura splits at the optic foramen.One layer lining the bony orbit-the periorbita-is firmlyattached at the orbital margin, over suture lines and in theoptic canal. Elsewhere it strips quite easily from the bone.The dural sheath of the optic nerve inserts into, and its fibersmerge with, the fibers of the sclera. The pia surrounds thenerve intimately and is continuous with the septa of thenerve. The subdural and subarachnoid spaces surroundingthe optic nerve form the intervaginal space, which containscerebrospinal fluid. Intracranial injections pass readily tothe sclera, where both sheaths of the nerve insert. Highintracranial pressure forces fluid into the perichoroidal spaceor along the lymphatic spaces of the nerve head. Within thedural sheath, the ophthalmic artery lies to the lower outerside of the nerve. The septum dividing the two is normallyfibrous, but may be ossified.The annulus of Zinn encircles the optic foramen and the
mesial end of the superior orbital fissure. Mesially it insertsinto the cleft formed by the splitting of the dural sheath.The lateral part is anchored at the spina recti lateralis, atthe tip of the great wing of the sphenoid. The origins of thesuperior and medial recti are fused with the sheath of theoptic nerve. Pain on movements of the eye with which thesemuscles are concerned is indicative of a lesion in the opticcanal.
350

CULLER: Fractures of the Orbit
APPLIED ANATOMYThe appearance of subconjunctival hemorrhage and of ec-
chymoses in the lids several days after a head injury is an im-portant diagnostic sign of basilar skull fracture (Scudder,9McCoollb). Extravasated blood naturally follows connec-tive-tissue planes. The extent of an injury can be estimatedby having a knowledge of the natural barriers that must bepassed when blood reaches the lid or subconjunctival space.
According to Duke-Elder, the septum orbitale preventseffusions from the orbit extending into the lids; the tissuesof the eyebrows prevent effusions from the forehead spread-ing into the upper lid; and to some extent the nasojugal andmalar folds tend to separate the lower lid and the cheek. Twopotential spaces in the upper lid are divided by the levatorpalpebrae muscle: (1) a pretarsal space, between the tarsalplate and the levator, and (2) a preseptal space, limited pos-teriorly by the levator and the septum orbitale.
Other natural compartments of the orbit, according toCharpy," are:
1. Central fatty tissue mass within the muscle cone: ex-travasations in this compartment lead to proptosis andloss of mobility, because anterior extension of fluid is limitedby the scleral insertion of Tenon's capsule.
2. Peripheralfatty tissue, outside the muscle cone, betweenthe muscles and the periosteum, is limited anteriorly by theseptum orbitale. According to Heerfordt,'2 with a pressureof from 40 to 50 mm. Hg, effusions percolate through vascularapertures in the septum into the preseptal space.
3. Subperiosteal compartment, in which blood is confinedunless the periosteum is ruptured. Rupture is most likelyto occur on the roof of the orbit. Effusions then travel intothe peripheral fatty compartment to the orbital septum.
4. The optic nerve sheath, which is continuous with themiddle fossa. Pringle"3 has observed it distended with bloodto its scleral insertion following basal fractures.
351

CULLER: Fractures of the Orbit
Ecchymoses appearing in the upper lid several days afterhead injury, if pretarsal, probably arise from injury to thevessels of the levator or superior rectus.
Subcutaneous ecchymoses in the upper lid seep throughthe orbital septum from the peripheral orbital compartmentprobably through the periorbita, from a fracture of the or-bital plate of the frontal bone, or from injury to branches ofthe supra-orbital artery or superior ophthalmic vein, which liebetween the levator and the roof of the orbit.Ecchymoses in the lower lid have come through the orbital
septum under pressure in the peripheral compartment below,either from direct injury to the vessels in the infra-orbitalcanal, or through a rupture of the periorbita by a fractureof the malar bone or supramaxilla.
Subconjunctival hemorrhage appearing late after an injuryis indicative of blood seeping through the peripheral com-partment from a fracture of the adjacent orbital wall. Gravi-tation of fluid from a fixed position of the patient mightmodify the point of appearance of the hemorrhage.
Proptosis and blood in Tenon's space after injury indicatehemorrhage inside the muscle cone, with probable fractureat the apex of the orbit.
THE DIFFERENTIAL DIAGNOSIS BETWEEN ORBITAL HEMORRHAGE CONSEQUENTUPON A FRACTURED ANTERIOR CRANIAL FoSSA AND ECCHYMOSES
OF DIRECT INJURY.-(Modifted from Bailey.'4)Fracture of Anterior Cranial Fossa
1. Extravasated blood is limited by fascia toorbital margin (circular).
2. Discoloration is purplish at first appear-ance.
3. Subconjunctival hemorrhage, never in con-junctiva.
4. Subconjunctival hemorrhage is fanshaped,apex toward iris; no posterior bordervisible.
5. Appearance delayed hours or days.
6. No evidence of contusion of soft tissues.
"Black Eye"1. No limitation.
2. Discoloration beefy redat first appearance.
3. Hemorrhage may be inconjunctiva and moveson manipulation.
4. Posterior limit of hemor-rhao in conjunctivacan be seen.
5. Ecchymoses developpromptly.
6. Abrasion of skin andswelling at point ofimpact.
352

CULLER: Fractures of the Orbit
LOCATION AND INCIDENCE OF FRACTURES OF THE ORBITThere is an interesting disparity of opinion as to the in-
cidence of involvement of the optic canal in basal skullfractures.
STATISTICS ON BASAL SKULL FRACTURES
Number Orbital Optic HemorrhageReported by of Source Fracures Canal In- in Optic
Cases volvement SheathHolderBerlinl5a.......... 126 Autopsy 80 54Vance6 .......... 512 Autopsy .. 51Pringle .......... 395 Clinical . . 1Pringle .174 Autopsy .. 13 16Battle'b ......... 168 Clinic . 168PhelpslSd. 570 Clinical 6 6Brunlc ........... 470 Clinical .. 8
Rawling'7 stated that-"The vast majority of anteriorfossa fractures avoids the immediate vicinity of the opticforamen and passes by preference between the two foraminaor diverges toward the sphenoidal fissures." Without openingthe highly theoretic and much discussed subject of the mech-anism of basal fractures, the opinion of Bryant and Buck18seems to be sound. The main fracture runs always approxi-mately in the direction of the violence applied. Thus, whenthe force is applied to the frontal bone, the fracture passesthrough the orbital plate (rarely bilaterally) and on throughthe sphenoid bone, usually to the sella turcica. Figure 4,from Rawling, is surprisingly typical of the illustrations insurgical textbooks. There must be less variation in thecourse of these fracture lines than one might anticipate. Theconclusion, from a study of surgical literature, is that anteriorfossa fractures nearly always cross the roof of the orbit. If theyreach the apex, they rarely encroach on the optic canal, buttypically endanger vision by the possibility of fragmenting theclinoidal processes or of inflicting vascular injuries in thisneighborhood.
According to Jefferson,19 fractuires involving the inner end
353

CULLER: Fractures of the Orbit
of the sphenoid fissure are likely to cause arteriovenousaneurysm, with monocular ophthalmoplegia. This is demon-strable in x-ray by a thinning of the boundary between thesphenoidal fissure and the optic canal.Blows on the inferior margin of the orbit commonly cause
separation of the suture lines of the malar bone. These frac-tures may be comminuted.The fracture lines may extend into the infra-orbital fissure
and the entire floor of the orbit be depressed, the maxillarysinus crumpling beneath it. These fragments are often ro-tated by an oblique blow.
According to Benedict,70a the mesial wall is frequently in-volved in fractures of the nose. This is certainly the thinnestwall of the orbit, and one should anticipate frequent fractures.However, they are not often recognized clinically. Emphy-sema should be the presenting sign.
CLINICAL EVIDENCE OF FRACTURE OF THE ORBIT1. Emphysema.-Escape of air into the soft tissues of the
orbit from a fracture into a sinus occurs especially from com-munication with the ethmoid cells, although we have ob-served it in a case of fracture of the floor of the orbit intothe maxillary sinus. Blowing the nose increases the swellingand crepitation in the lids.
2. Ecchymoses and subconjunctival hemorrhage, coming onseveral hours or days after an injury, are quite pathogno-monic of fracture if differentiated from contusions (fig. 3).
3. Immediate Proptosis.-If there is no gross displacementof fragments, immediate proptosis is due to hemorrhage in-side the muscle cone. This usually indicates a fracture in-volving the apex of the orbit, running into the superiororbital fissure.
4. Proptosis Developing Later.-The first symptom of pul-sating exophthalmos to develop is proptosis. This may notoccur until one or two months after injury. The proptosiscan be reduced by steady pressure on the globe. The globe
354

5up.OPNT1AL VYl£1
eRcct...Levotor
t.-5up.obfiqueMedial Pect.
OPTIC NERVE
r~O0I4THAL ART.
v Na5o.ciliaPy N
>\In. Rect.
Fig. 1.-The apex of the right orbit.Fractures at the apex may cause hemorrhages into three con-
nective-tissue compartments of the orbit: (1) The sheath of theoptic nerve; (2) the muscle cone; (3) the peripheral compart-ment (Duke-Elder).
Su-petior oblique muscle
LevaWor alpebrm supeerWis niuset.eSuperior rectus muscle \U
Medial recta$ musclt 'nlee.Optic Servew 'Ml....
goSP
::.Ahbenth at opfit}enerve Tmfettit- fr .-~ :-i f
Fig. 2.-Diagrammatic seetion of the orbitHemorrhages arising from fractures of the optic canal at (1) are confined to
the sheath of the optic nerve, limited anteriorly by the insertion into the seleraand may cause loss of vision. Hemorrhages due to a fracture involving thesuperior orbital fissure at (2) may be limited to the muscle cone, anteriorly bythe insertion of the muscle and Tenon's capsule into the sclera, and causeproptosis. Fractures of the roof and floor of the orbit at (3) and (4) tear theperiorbita and give rise to hemorrhages in the peripheral compartment whichlater appear as ecchymoses into the lids.
ILeSer wifN

The j{ech mosilmtdbthoriaFig. 3.-A patient with fracture of the left anterior cranial fossa.The ecchymosis limited by the orbital margin appeared four hours after the
accident. The posteirior limit of the subconjunctival hemorrhage could not beseen (Bailey).
Fig. 4.-Typical course of fractures of the orbital plate of the frontal bone:(a) Force applied to the median frontal region. (b) Force applied to the lateralfrontal region (Rawling).
......rVA

CULLER: Fractures of the Orbit
and dilated conjunctival vessels pulsate synchronously withthe heart-beat. As the aneurysm enlarges, a definite thrillcan be felt, and a loud, roaring murmur can be heard onauscultation. This is audible over a wide area. The patientcomplains of noise in the head, which is intensified by bendingforward.
Diplopia may develop secondary to proptosis or to involve-ment of the nerves. Trophic changes and pain may resultfrom involvement of the fifth nerve. The pupil may be di-lated, due to paralysis of the third nerve. If the lids cannotbe closed, keratitis may occur from exposure of the cornea.There is engorgement of the retinal veins, and the disc maybe swollen. Loss of vision, even to complete blindness, maybe due to pressure or stretching of the optic nerve or may fol-low the papilledema.
Rea20 quoted Lock, who found 588 cases of pulsating exoph-thalmos reported in the literature. Of these, 77 per cent.were traumatic and 94 per cent. of these were an arterio-venous communication between the internal carotid and thecavernous sinus. Lock stated that a pulsating swelling abovethe inner canthus is typical of this type and that the proptosisis greater in these cases than in the intra-orbital aneurysms.
5. Extra-ocular Palsies. -Due to the length of the pathwayof the cranial nerves, palsies of the extra-ocular muscles pointonly to a basilar lesion, except when taken in conjunctionwith other findings, such as orbital hemorrhage. Displace-ment of bony fragments, by direct pressure may cause palsiesof the muscles. The author has seen one patient who sus-tained a crushing fracture with loss of the malar eminenceand depression of the inferior orbital margin on both sides.When the patient regained consciousness, ten days after theaccident, there was complete paralysis of all extra-ocularmuscles, with only slight loss of vision. This was due to theupward displacement of the posterior portion of the floor ofthe orbit. Following reduction of the fragments, the paraly-sis disappeared completely. In this case wiring of the zygo-
355

CULLER: Fractures of the Orbit
matic fragment to the frontal bone in the temporal wall ofthe orbit was necessary. The patient regained orthophoriaand normal vision.
6. Immediate Blindness.-According to Rea, sudden blind-ness in one eye is a not uncommon finding following a blowon the head. Ophthalmoscopically, nothing abnormal is dis-cernible, but the pupil on the affected side is dilated andinactive to direct light. Beginning optic atrophy may beobserved within a few weeks. The damage to the optic nervemay be complete or incomplete. Barkan and Barkan,2' infive of their 22 cases, found a sector defect extending to andinvolving the macula, and considered it sufficiently charac-teristic as to be almost pathognomonic. They also pointedout that macular involvement points to a poor prognosis, asin their experience central vision has never returned. Thesector defect is typically down and out, corresponding to afracture of the canal up and in through the stronger arach-noid attachment of the nerve to the periosteum.The generally accepted theory of immediate monocular
blindness is that it results from direct injury to the opticnerve.
Berlin, reviewing Holder's 126 coroner's autopsies of skullfractures, found an incidence of 90 per cent. of orbital frac-tures and of 61 per cent. of fractures into the optic canal.Berlin declared that he never found hemorrhage into theoptic sheath unless there was a fracture of the optic canal.
Pringle objected to generalizations from the findings ofBerlin, because of the high percentage of gunshot wounds(suicides) in the latter's series. Pringle treated 395 provedskull fractures due to all causes except gunshot wounds. Ofthese, 174 came to autopsy and 13 showed fracture of theoptic canal. In 16 there was hemorrhage into the sheath ofthe optic nerve. He concluded: "My own belief is that thisform of blindness results from hemorrhage into the nervesheath in the majority of cases." In seven of the 16 patientswith hemorrhage the blood was present only in the sheath,
356

CULLER: Fractures of the Orbit
and did not pass through the canal into the middle cranialfossa. In two of these cases there was no fracture of the opticcanal. These two cases go to prove that intravaginal hemor-rhage resulting from violence is possible without fracture.
Since the typical direction of fractures of the orbital plateof the frontal bone is toward the sella turcica, the possibilityof pressure of fragments, or factual tearing of the intracranialportion of the nerve or the chiasm, has not received sufficientattention.
7. Delayed Blindness.-Margoline22 collected 44 cases ofoptic atrophy resulting from trauma. Eight of these weredue to indirect injury to the nerve, causing delayed loss ofvision. Lillie and Adson23 described two cases of central andannular scotomas produced by callus from a fracture involv-ing the optic canal. At the time of the injury both patientsexhibited ecchymoses of the lids and the pupil was dilated,but vision did not begin to fail until six weeks later.
CASE REPORTK. H., aged twenty-five years, sustained a fracture of the right
frontal fossa in an automobile accident in November, 1937. Onrecovering consciousness two weeks later, he complained of di-plopia. A partial paralysis of the right internal rectus was found,but the eyegrounds were normal and his visual acuity was un-affected. The x-ray did not demonstrate any involvement of theoptic canal. His third-nerve paralysis improved, so that he hadfusion to 200 to the left on April 9, 1938, but fields taken at thattime showed a temporal hemianopic defect to colors and a 300 con-traction to form temporally in the left eye. The fundi were normal.The patient did not return until four months later, when he had asuperior temporal quadrant defect in the right eye and a temporalsector defect extending almost to the center of his left field. Hisvisual acuity was reduced to 6/12 in each eye, with correction, andthere was some pallor of both discs. X-ray studies by Dr. Birkbeckat this time showed a fracture line extending into the sphenoidsinus. Dr. Max Peet operated on him, and found a definite sub-dural pseudomembrane along the base of the right frontal fossa.This extended around the chiasm. There was a small arachnoid
357

CULLER: Fractures of the Orbit
cyst over the chiasm. Two weeks after operation the patient diedof a streptococcus meningitis.
Rea believes that these cases of delayed loss of vision maybe due to the formation of callus, recurrent hemorrhage, trau-matic meningitis in the neighborhood of the optic foramina,or atrophy consecutive to a traumatic papillitis, but he is ofthe opinion that most cases of late post-traumatic atrophyof the optic nerve are probably due to a serous meningitiswith development of a chronic arachnoiditis. Peet has ob-served organization of a hematoma in the sella turcica pro-duce field defects and optic atrophy.
Certainly in all these cases of delayed blindness there werefrontal fossa fractures. The possibility of blindness devel-oping later should encourage careful x-ray studies of the apexof the orbit at the time of the injury.
8. Crepitation of Fragments; Loss of Contour of the OrbitalMargin; Loss of the Malar Eminence; Displacement of theOrbital Contents; Limitation of Motion of the Eye.-Thesesymptoms are commonly found in fractures of the malar boneand need no conmment. Careful inspection and palpation ofthe orbital margin are of prime importance in treating headinjuries. The floor of the orbit is not well demonstrated bythe usual technique for roentgenography of the skull. Theauthor has seen four such fractures that were not diagnosedby x-ray. The ophthalmic surgeon must call the attentionof the roentgenologist to the presence of the fracture, so thathe can ascertain its extent. According to Straith,24 anesthesiaof the lateral aspect of the nose and lip is seen in fracturesthrough the infra-orbital foramen.
OCULAR SIGNS OF BASAL SKULL FRACTUREPupillary Changes.-A patient with a fracture of the base
of the skull is usually brought to the hospital in an uncon-scious condition. Any sign that points to the site and extentof cranial compression is of tremendous value. The reaction
358

CULLER: Fractures of the Orbit
of the pupils is the most reliable index to the progression ofintracranial hemorrhage and to its location.
HUTCHINSON'S PUPILS FROM THE TImE OF ONSET OFINTRACRANIAL HEMORRHAGES
Stage Pupil on Opposite Side Side on which Compression Started1. Normal Slightly contracted, sluggish reaction2. Normal Moderately dilated, reacts3. Moderately dilated, and reacts Widely dilated, no reaction4. Moderately dilated, and no re- Widely dilated, no reaction
action
Brain surgeons agree that the dilated and fixed pupil isof greater localizing significance than is bleeding from theopposite ear or even hemiplegia. Even if hemiplegia and thedilated pupil are on the same side, operative interventionshould be directed toward the side on which the pupillarychange first manifested itself (Holman and Scott25).
Deviation of Head and Eyes.-A less constant sign is thedeviation of the head and eyes toward the side of major in-jury and away from paralyzed extremities.
Loss of Corneal Reflex. -The trigeminal innervation is con-tralateral. Cerebral hemorrhage on one side may cause lossof corneal sensitivity on the opposite side.The second infallible sign of progressive intracranial hem-
orrhage is the "lucid interval." A patient may recover con-sciousness after the initial concussion, but a subsequent lapseinto unconsciousness is an indication of more bleeding. If thelucid interval is short, the hemorrhage is severe.Papilledema.-Some engorgement of retinal vessels may
be seen shortly after a skull injury. Holman and Scott havereported papilledema as early as eight hours after an injury.Most observers agree that papilledema from traumatic cere-bral edema appears in from three to eight days after theaccident, although, according to Battle, in fractures of theposterior fossa it may be delayed for as long as four weeks.
Cranial Nerve Palsies.-Scudder maintains that injuriesof the cranial nerves in basal skull fractures occur in the fol-lowing order of frequency: (1) Facial (seventh); (2) abdu-
359
CULLER: Fractures of the Orbit
cens (sixth); (3) auditory (eighth); (4) oculomotor (third);(5) optic (second). The long course of the sixth and seventhnerves in the base and their relationship to the apex of thepetrous portion of the temporal bone are cited to explain thefrequency of their involvement in basal fractures. The fourthnerve is rarely affected. The fifth nerve escapes in most mid-dle fossa fractures, but corneal anesthesia following a headinjury may mean trauma to the first division, where it passesthrough the superior orbital fissure.
X-RAY DEMONSTRATION OF FRACTURES OF THE ORBITThe great differences of opinion as to the cause of trau-
matic monocular blindness and the disparity in statistics asto the incidence of fracture of the orbit are due largely toour lack of satisfactory demonstration of the orbit and itsstructures adjacent to the apex by x-ray. This fact has re-cently received considerable attention, and several improve-ments in technique have been developed. However, the usualtechnique still employed by roentgenologists consists of astereoscopic postero-anterior and a lateral exposure. In thismethod there is obvious superimposition of shadows of im-portant structures. The apex of the orbit is lost in a mazeof unpredictable air cells. The failure of the method to dem-onstrate the presence of fractures of the orbit dependably isnot surprising. On the contrary, a positive diagnosis of frac-ture in this difficult region is a tribute to the skill and patienceof the roentgenologist. As Hofman26 pointed out, when re-ferring to fractures of the middle fossa, "X-ray findings arenot to be relied upon except when positive findings are dem-onstrated." In a series of 108 cases of basal skull fracturesat Cincinnati General Hospital, only 14 were demonstratedby the x-ray.Attempts have been made to project the orbit against the
vault. The Titterington method is a projection in a plane230 backward from the vertical plane. E. W6rner27 recom-mended increasing this angle to 300, and reported 22 cases
360

a?K rv . . .,OPTlI.TRAT ISO1 00300
..~~~~02 :: i,
.45Cm T So. 0.- o%2-.~~~~~~1.
Fig. 5.-Dissection to illustrate the bend in the course of the sixth cranial nerveover the petrous apex (Wolff).

Fig. 6.-The visualization of the orbital margins by roentgenogram.

0..I a..
Fig. 7.-The planigraph.
A
I
I
I c

Fig. 8.-Position of the patient with the plane of the left optic canalpaiallel to the film; 52 degrees from a postero-anterior plane.
Fig. 9.-The planes of the orbit in relation to Reid's base line.
.POvj44P:S.A.

(a) (b)Fig. 10.-The roof of the left orbit: (a) By planigraphy; (b) from an anatomic
plate (Duke-Elder).
(a) (b)Fig. 11.-The floor of the right orbit: (a) Planigraphy demonstrates the inferior or-
bital fissure in profile and the nasolacrimal canal in cross section; (b) anatomic figure(Duke-Elder).

......... ...........e.... ...-.-.---
Fig. 12.-The average angles formed by the lateral and mesial walls of theorbit w ith the median plane.
Fig. 13.-Planigraphic section through the mesial wall of the right orbit.

; . minin papyrnoes nol.s etln
, '.rsni- ethioldalhaPwoeeaus orbitalli oasiW palatini ,
:orpus ostis spho.aidatis
: oniee optios# I j
Pisnurs orbitlis superfor i' ;
Sells toroles \
ProbE i_.lom
r@fi:tssidi*me
amsen spheaopalatInumn
Fous pterygoplatin,la j
Lamnine laerell_processue pterygolde ,
Processu. pyremidalis ossls palatluProbe in eanalis palatinus Par *- inus imllaris
Joblaris..nt ::
Fig. 14.-The mesial wall of the right orbit (Spalteholz).
Fig. 15.-Sagittal section one centimeter from the median plane. This sectioncuts through ethmoidal cells and the infundibulum ethmoidale.
Spina IrochlearlsPers orbitalis
'ossi frontalsi
0. lacrimale
Fouss-0cei l .crlmFlis
L., 04 ussale
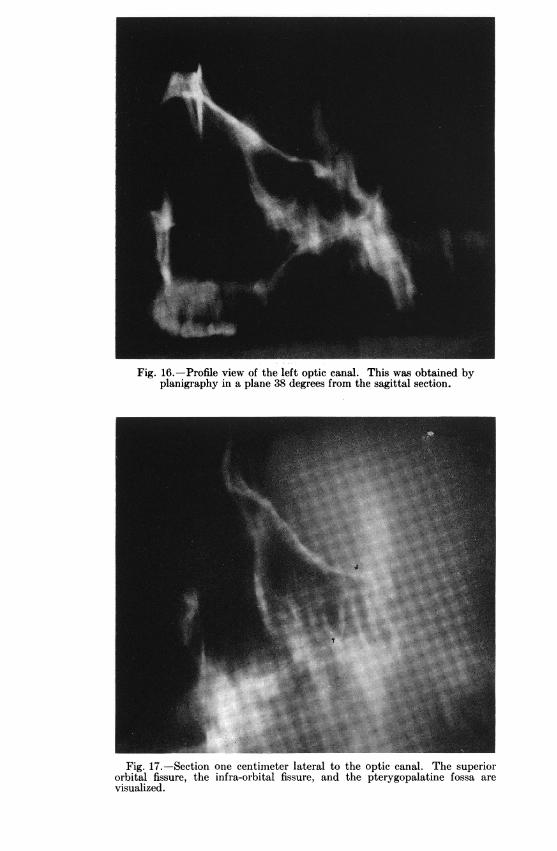
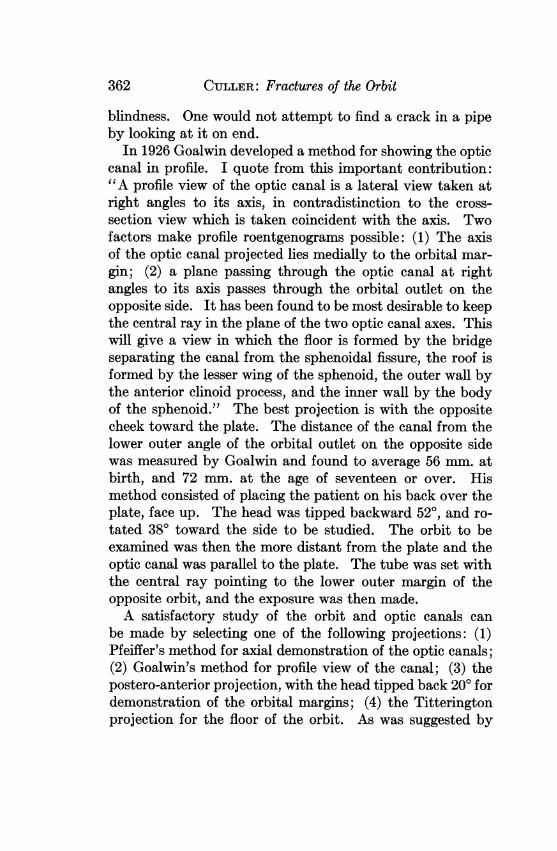
Fig. 16.-Profile view of the left optic canal. This was obtained byplanigraphy in a plane 38 degrees from the sagittal section.
Fig. 17.-Section one centimeter lateral to the optic canal. The superiororbital fissure, the infra-orbital fissure, and the pterygopalatine fossa arevisualized.

CULLER: Fractures of the Orbit
of orbital hemorrhage associated with skull fracture. Themethod does avoid the superimposition of some of the shad-ows from the base of the skull, but the orbit in this projec-tion is so distorted and foreshortened that considerable ex-perience is necessary to interpret the films. The angle is notof much value in a critical study of the apex of the orbit.The optic canal can be projected on end into the inferior
temporal quadrant of the orbit. This was demonstrated byWhite28 in 1924. Goalwin showed that no precise roentgeno-gram of the optic canal is possible unless the angles of orien-tation are accurately measured. From measurements of1,000 canals this observer concluded that the axis of the canalsubtends an angle of 390 with both the horizontal and medianplanes of the skull, without much variation after the age ofthree. Pfeiffer reduced this to a practical technique by de-vising a head rest that allows the roentgenologist to takestereoscopic contours of both canals. He used an angle of370 to the median plane, and 300 to Reid's base line. Thelatter is the plane of the external auditory canal and theinferior margin of the orbit. Pfeiffer stated that the hori-zontal axis is quite constant, but that some variation in thevertical angle may be found in 10 per cent. of patients.Camp and Gianturco,29 in an attempt to simplify the
measurement of the angulation of the skull for these projec-tions, also devised a localizer. To some extent this develop-ment was unfortunate because, whereas Pfeiffer's method canbe carried out with great accuracy, the simpler method losesin accuracy what it gains in simplicity. Ophthalmologistshave come to disparage this method because of the inaccu-racies of its modifications, a condition exactly comparable tothe one that followed the modification of the original Sweetlocalizer for intra-ocular foreign bodies.
Pfeiffer's method is most successful in providing an axialview of the optic canal, but it leaves much to be desired as ameans of demonstrating the cause of traumatic monocular
361
CULLER: Fractures of the Orbit
blindness. One would not attempt to find a crack in a pipeby looking at it on end.
In 1926 Goalwin developed a method for showing the opticcanal in profile. I quote from this important contribution:"A profile view of the optic canal is a lateral view taken atright angles to its axis, in contradistinction to the cross-section view which is taken coincident with the axis. Twofactors make profile roentgenograms possible: (1) The axisof the optic canal projected lies medially to the orbital mar-gin; (2) a plane passing through the optic canal at rightangles to its axis passes through the orbital outlet on theopposite side. It has been found to be most desirable to keepthe central ray in the plane of the two optic canal axes. Thiswill give a view in which the floor is formed by the bridgeseparating the canal from the sphenoidal fissure, the roof isformed by the lesser wing of the sphenoid, the outer wall bythe anterior clinoid process, and the inner wall by the bodyof the sphenoid." The best projection is with the oppositecheek toward the plate. The distance of the canal from thelower outer angle of the orbital outlet on the opposite sidewas measured by Goalwin and found to average 56 mm. atbirth, and 72 mm. at the age of seventeen or over. Hismethod consisted of placing the patient on his back over theplate, face up. The head was tipped backward 520, and ro-tated 380 toward the side to be studied. The orbit to beexamined was then the more distant from the plate and theoptic canal was parallel to the plate. The tube was set withthe central ray pointing to the lower outer margin of theopposite orbit, and the exposure was then made.A satisfactory study of the orbit and optic canals can
be made by selecting one of the following projections: (1)Pfeiffer's method for axial demonstration of the optic canals;(2) Goalwin's method for profile view of the canal; (3) thepostero-anterior projection, with the head tipped back 200 fordemonstration of the orbital margins; (4) the Titteringtonprojection for the floor of the orbit. As was suggested by
362

CULLER: Fractures of the Orbit
Eitzen,30 in this method the x-ray film may be held by thepatient between his teeth.
PLANIGRAPHY OF THE ORBITVallebona,31 disturbed by the superimposition of shadows
in studies of the cranium, pointed the way to a logical solu-tion of this problem. He obtained excellent projections ofthe sella turcica by joining a plate and tube in a rigid systemand rocking this system about the axis of the sella while theexposure was made. Ziedses des Plantes32 and others, work-ing on this principle, developed the planigraph, which theyapplied particularly to roentgenography of the chest. Anastonishing number of soft-tissue details can be seen in theirx-rays of the chest, and the method is now being widely usedin tuberculosis clinics on the continent.The planigraph (fig. 7) is an instrument designed to blur
out superimposed shadows in roentgenograms. It is basedon the principle of the lever. A rapidly oscillating lever isblurred, except at the fulcrum. An x-ray tube and plate,moving reciprocally past a fulcrum, would give an image ofthe axis of the fulcrum. It was found that if the reciprocalmotion of the tube and plate is along a rectilinear sine curveinstead of the arc of a circle, the fulcrum becomes a verticalplane.Roentgenograms taken with a planigraph show sharp de-
lineation of structures in a body section approximately 1 cm.thick. Structures removed several centimeters from the focalsection are blurred out entirelv. Closer structures throw ablurred shadow on the film. In reading these films one doesnot have to select, from numerous superimposed shadows,the structures in which he is interested, but knows that everysharply defined image on the film is in the plane studied.
This principle appeared applicable to the x-ray study ofthe orbit. Early investigations with the planigraph, whichwas used in chest radiography, and placed at the writer'sdisposal by Dr. Warren Breidenbach, soon gave convincing
363

CULLER: Fractures of the Orbit
evidence that while the principle was sound, satisfactorystudies of the orbit required a much greater power than didchest radiography. Accordingly, a more powerful unit wasobtained and installed.Our early hopes of demonstrating soft-tissue structures in
the orbit were not realized, for the power necessary to pene-trate the dense bones of the skull was found to burn outmany soft-tissue shadows. However, bony planes were wellvisualized.
It was argued that fractures can be visualized best if thebone is perpendicular to the x-rays. Fractures of the wallsof the orbit should be seen clearly if a method could be de-vised that would place the wall in question in the plane of thefulcrum of the planigraph. Fractures of the optic canalwould be demonstrated best by a body section showing thecanal in profile.
It soon became evident that Goalwin's dictum, that nocritical study of the apex of the orbit can be made withouta device for fixing the head and capable of proper angulation,was well founded.A head rest was designed and attached to the planigraph.
We wished to use Reid's base line, the plane of the externalauditory canal and the inferior wall of the orbit as our planeof orientation, in order to correlate this work with Pfeiffer'sstudy of the axial demonstration of the optic canal. How-ever, models using the external auditory canals as two of threepoints of fixation all proved too cumbersome, and this planwas abandoned in favor of the bite as a fixation. The presentmodel of the head rest is illustrated in figure 8.
The Visualization of the Roof and Floor of the Orbitby Planigraphy
Reid's base line is determined by inserting one end of anespecially designed level into the external auditory canal, andlining the inferior orbital margin with the other end. Thepatient's head is fixed in this position with a bite on the
364

.... ..,
Fig. 18.-Straith's method of reducing depressed frac-tures of the floor of the orbit.

CULLER: Fractures of the Orbit
tongue blade, and the angle with the vertical plane read onthe protractor which turns in the axis of the tongue blade.This is established as the zero position.The roof of the orbit (fig. 9) forms an average angle of 200
with Reid's base line. The patient is placed with his backto the plate. The head is tilted backward 700, placing theplane of the roof of the orbit parallel with the x-ray plate.The perpendicular distance between the roof of the orbit andthe film is measured, and the fulcrum of the planigraph is setin this plane (fig. 10).The floor of the orbit (fig. 9) forms an average angle of
230 with Reid's base line. The floor can be demonstrated byplanigraphy by placing the patient facing the plate and bend-ing the head forward 670, about the axis of the tongue blade.The perpendicular distance from the inferior orbital marginto the plate is measured, and the fulcrum of the planigraphis set in this plane (fig. 11).The angles formed by these planes and Reid's base line
may be greater by as much as 100 than the figures given, butare rarely less.
Body Section Radiography of the Lateral and MesialWalls of the Orbit
For planigraphy of the lateral wall of the orbit (fig. 12),the patient is placed facing the plate and turned 400 towardthe side to be studied. Two horizontal protractors providea means of bringing the patient's head close to the plate, butthis displacement must be added to the horizontal angulationof the patient. The long bar of the head rest slides in asleeve, to allow for lateral movement for orientation. Theperpendicular distance from the lateral orbital margin to theplate is measured, and the fulcrum of the planigraph is setin the plane of the lateral wall.
For planigraphy of the mesial wall (fig. 12) the patient isturned 70 from a true lateral position. The perpendicular
365

CULLER: Fractures of the Orbit
distance from the mesial orbital margin to the plate is meas-ured, and the fulcrum set in this plane (figs. 13, 14, and 15).
All the walls are curved slightly. The mesial wall particu-larly is tipped at an angle of about 100, base down. Theseirregularities will probably not interfere with the demonstra-tion of fracture lines.
Prof le View of the Optic Canal. -The horizontal axis of theoptic canal forms an angle of 38° with the median plane. Aprofile view of the canal is obtained by turning the patient'shead 38° toward the plate from the true lateral position, andmeasuring the distance from the plate to the inferior temporalquadrant of the orbit farther removed from the plate (figs. 16and 17).A cross-section of the canal can be obtained at right angles
to this position with the head tilted back 300.
TREATMENT OF FRACTURES OF THE ORBITTwo classes of orbital fractures require prompt diagnosis
and treatment. Fractures in this region cannot be reducedafter about ten days following the injury (Figi33).
1. Malar bone fractures, if untreated, leave serious deform-ities and loss of function. These fractures should always bereduced. According to Straith (fig. 18), this can be accom-plished by-(1) grasping and elevating the bone by meansof a large towel clip inserted through an incision in the lowerlid and cheek; (2) opening the canine fossa and elevating themalar bone through the antrum, packing the antrum, if nec-essary, to maintain position of the fragment; (3) passing anantral trocar through the mucous membrane behind the lastupper molar, up and beneath the malar bone behind themaxilla. Upward pressure against the depressed portion usu-ally suffices to elevate it satisfactorily. If this fails to main-tain proper elevation, the antrum may be packed, or pref-erably the fragments may be wired in place through drillholes at the frontal fracture line.
2. Fractures Involving the Apex of the Orbit.-Monocularblindness following head injury requires careful study by
366

CULLER: Fractures of the Orbit
x-ray. If the loss of vision is due to fragmentation of thecanal or the clinoid processes, one should be able to demon-strate the fracture by the methods previously outlined.Barkan and Barkan suggested Naffziger's subdural approachto the apex of the orbit, as for a pituitary tumor. If no frac-ture is demonstrated, one must suspect hemorrhage into thesheath of the optic nerve, as Pringle contended that this wasthe common cause of traumatic monocular blindness. Everyophthalmologist sees the optic nerve often enough in detach-ment operations. A Kr6nlein operation should not be neces-sary in order to explore the retrobulbar space sufficiently toobserve whether the sheath is distended with blood, a con-dition pathologists contend they frequently find at autopsy.
SUMMARYThe most common fractures of the orbit are depressed frac-
tures of the floor and those of the anterior fossa involvingthe roof. Either of these may involve the apex of the orbit,endangering vision. Fractures of the anterior fossa nearlyalways cross the roof of the orbit. If they reach the apex,they rarely encroach on the optic canal, but typically endan-ger vision by the possibility of fragmenting the clinoid proc-esses or inflicting vascular injuries in this neighborhood.Ecchymoses and subconjunctival hemorrhages appearing
several hours or days after an injury are quite pathognomonicof fracture of the orbit. Emphysema of the soft tissues of theorbit indicates a fracture into one of the accessory sinuses ofthe nose. Fractures involving the superior orbital fissuremay lead to hemorrhage into the muscle cone and immediateproptosis. Pulsating exophthalmos developing later is a signof traumatic arteriovenous aneurysm. Extra-ocular palsiesmay occur from injuries at the apex. The most importantevidence of injury at the apex is immediate or delayed loss ofvision.The superimposition of shadows renders it difficult to vis-
ualize fractures of the apex of the orbit by x-ray. A method
367

368 CULLER: Fractures of the Orbit
is described for the blurring of extraneous shadows by theapplication of planigraphy (body section radiography) to thex-ray study of the orbit. The plane of each wall of the orbitcan be projected in x-ray, and the optic canal can be demon-strated in profile.The author is indebted to Dr. Warren Breidenbach and
Mr. Joseph Glaser for their patient collaboration in the appli-cation of planigraphy to the orbit.
REFERENCES1. Duke-Elder, W. S.: Text-book of Ophthalmology. St. Louis, 1933, vol. 1,
pp. 168, 209.2. Le Doubie, A. F.: Trait6 des variations des os du crAne de l'homme et de
leur signification au point de vue de l'anthropologie zoologique. Paris,1903.
3. Whitnall, S. E.: The Anatomy of the Human Orbit and Accessory Organsof Vision. 2. ed. London, 1932.
4. Onodi, A.: The Optic Nerve and the Accessory Sinuses of the Nose. NewYork, 1910.
5. Goalwin, H. A.: J.A.M.A. 89: 1745, 1927.Goalwin, H. A.: Arch. Ophth. 35: 1, 1926.Goalwin, H. A.: Am. J. Roentgenol. 17: 573, 1927.
6. Keyes, J. E. L.: Arch. Ophth. 13: 538, 1935.7. Hartmann, E.: La radiographie en ophtalmologie. Ch. IV. Radiog-
raphie du canal optique. Paris, 1936.8. Pfeiffer, R. L.: Am. J. Roentgenol. 29: 410, 1933.9. Scudder, C. L.: The Treatment of Fractures. 10. ed. Philadelphia, 1926,
p. 34.10a. Benedict, W. L.: Diseases of the Orbit. In: The Eye and its Diseases.
Edited by C. Berens. Philadelphia, 1936, p. 331.10b. McCool, J. L.: Diseases of the Eyelids. In: Ibid., p. 366.11. Charpy: Bibliogr. anat. 20: 1, 1910. (Quoted by Duke-Elder, p. 181.)12. Heerfordt, C. F.: Arch. f. Ophth. 58:123, 1904. (Quoted by Duke-
Elder.)13. Pringle, J. H.: Brit. M. J. 2: 1156, 1924.14. Bailey, H.: Demonstrations of Physical Signs in Clinical Surgery. 5. ed.
Baltimore, 1935, p. 62.15a. Berlin, R.: In: Handbuch der gesamten Augenheilkunde (Graefe-
Saemisch), Leipzig, 1880, v. 6, p. 604.15b. Battle, W. H.: Lancet, 2: 1; 57; 107; 1890.15c. Brun, H.: Beitr. z. klin. Chir. 38: 289, 1903.15d. Phelps, C.: Ann. Surg. 49: 466, 1909. (Quoted by Barkan and Barkan.)16. Vance, B. M.: Arch. Surg. 14: 1023, 1927.17. Rawling, L. B.: Head Injuries. London, 1934.18. American Practice of Surgery. Edited by J. D. Bryant and A. H. Buck.
New York, 1908, v. 5, p. 49.19. Jefferson, G.: Alterations in the Optic Foramina. Internat. (2) Neurol.
Cong., London, 1935.20. Rea, R. L.: Neuro-Ophthalmology. St. Louis, 1938, p. 415.21. Barkan, O., and Barkan, H.: Am. J. Ophth. 11: 767, 1928.22. Margoline, E.: Internat. Clin., 28. ser. 3: 186, 1918.23. Lillie, W. I., and Adson, A. W.: Arch. Ophth. 12: 500, 1934.
ELLES: Rhinosporidiosis seeberi Infection in Eye 369
24. Straith, C. L.: J.A.M.A. 109: 940, 1937.Straith, C. L.: J.A.M.A. 108: 101, 1937.
25. Holman, E., and Scott, W. M. J.: J.A.M.A. 84: 1329, 1925.26. Hofman, A. P.: Ohio State M. J. 35: 515, 1939.27. Worner, E.: Arch. f. klin. Chir. 178: 224, 1934.28. White, L. E.: Laryngoscope, 34: 255, 1924.29. Camp, J. D., and Gianturco, C.: Am. J. Roentgenol. 29: 547, 1933.30. Eitzen, A. C.: J. Kansas M. Soc. 39: 15, 1938.31. Vallebona, A.: Radiol. med. 17: 1090, 1930.32. Ziedses des Plantes, B. G.: Fortschr. a. d. Geb. d. R6ntgenstrahlen,
47: 407, 1933.33. Figi, F. A.: S. Clin. North America, 12: 949, 1932.
RHINOSPORIDIOSIS SEEBERI INFECTIONIN THE EYE*
NORMA B. ELLES, M.D.Houston, Texas
INTRODUCTIONMycotic infections of the eye are being recognized more
often in recent years, as our knowledge of the variousmycoses has increased. Since many ophthalmologists areunfamiliar with the clinical and pathologic features of a some-what rare fungus disease of the mucous membranes of theeye called "rhinosporidiosis," and since this disease must bemore prevalent than the few reported cases would seem toindicate, the occurrence of a case in my own practice has beenthe incentive for a review of the literature on this subject.
CLASSIFICATION OF PARASITEThe parasite was at first believed to be a sporozoon (Seeber,'
1900) somewhat analogous to the Polysporea of Schneider,a subdivision of the Coccidiidea. Other investigators(Minchin and Fantham,2 1905) concluded that Rhinospor-idium was an annectate form that showed marked affinitieswith the typical Neosporidia and also with the simpler Haplo-* Candidate's thesis for membership accepted by the Committee on Theses.