ISSUE 3, M 2017 · Revolver 6 1 5 12 Rifle 3 4 0 7 Shotgun 5 3 2 10 Total 17 11 8 36 SUICIDE D ......
14
Page 1 of 14 Data Perceptions Trends Best practices Issues COORDINATED BY THE ONEIDA COUNTY HEALTH DEPARTMENT I SSUE 3, M ARCH 2017 The is a broad partnership of community agencies and organizations that play a role in the health status of our community. A primary objective of the OCHC is to meet quarterly to prepare a Quarterly Health Report Card on various community health issues. Participants analyze county data, collect stakeholder feedback on perceptions and underlying causes, identify collaborative opportunities and evidence-based resources to address the issue, and compile the information into a Health Report Card. The topic of this Quarterly Health Report Card is:
Transcript of ISSUE 3, M 2017 · Revolver 6 1 5 12 Rifle 3 4 0 7 Shotgun 5 3 2 10 Total 17 11 8 36 SUICIDE D ......

Page 1 of 14
Data
Perceptions
Trends
Best practices
Issues
COORDINATED BY THE ONEIDA COUNTY HEALTH DEPARTMENT
I S S U E 3 , M A R C H 2 0 1 7
The is a broad partnership of
community agencies and organizations that play a role in the health status of
our community. A primary objective of the OCHC is to meet quarterly to
prepare a Quarterly Health Report Card on various community health issues.
Participants analyze county data, collect stakeholder feedback on perceptions
and underlying causes, identify collaborative opportunities and evidence-based
resources to address the issue, and compile the information into a Health
Report Card. The topic of this Quarterly Health Report Card is:

Page 2 of 14
“Depression is the most common type of mental
illness…It has been estimated that by the
year 2020, depression will be the second leading
cause of disability throughout the world, trailing only ischemic
heart disease.” Centers for Disease Control
and Prevention
Mental health is “a state of well-being in which the individual
realizes his or her own abilities, can cope with the normal
stresses of life, can work productively and fruitfully, and is able to
make a contribution to his or her community.” It is estimated that
only about 17% of U.S adults are considered to be in a state of
optimal mental health. There is emerging evidence that positive
mental health is associated with improved health outcomes.
(Centers for Disease Control and Prevention)
AGE-ADJUSTED PERCENTAGE OF ADULTS WITH POOR MENTAL HEALTH FOR 14 OR MORE DAYS IN THE LAST MONTH, 2013-2014
Data Source: 2013-2014 NYS Expanded Behavioral Risk Factor Surveillance System data as of September 2014

Page 3 of 14
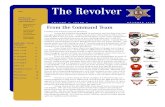
PERCENTAGE OF TEENS WHO EXPERIENCED DEPRESSION OR SUICIDE IDEATION IN
THE PAST YEAR Source: Oneida County 2015 TAP Survey
TEENS AND SUICIDE IDEATION
Source: Oneida County 2015 TAP Survey
40%
28% 27%31%
29%
24%20% 18%
20% 18%
0%
10%
20%
30%
40%
50%
1999 2003 2007 2011 2015
Depression Suicide Ideation
24%
19%
8%
4%
20%18%
9%
3%
18%
14%
10%
3%
20%
17%
8%
3%
18%19%
8%
5%
0%
5%
10%
15%
20%
25%
30%
Seriously ConsideredSuicide
Planned Suicide Attempted Suicide Injured in AttemptedSuicide
1999 2003 2007 2011 2015

Page 4 of 14
PERCENT OF TEENS WHO SERIOUSLY CONSIDERED SUICIDE (FOR ALL AND BY
GENDER) IN THE PAST YEAR Source: Oneida County 2015 TAP Survey
PERCENTAGE OF TEENS WHO IN THE PAST YEAR HAVE HURT THEMSELVES ON PURPOSE WITHOUT INTENDING TO COMMIT SUICIDE
Source: Oneida County 2015 TAP Survey
8%
15%3%
6%
3%
5%
0%
5%
10%
15%
20%
25%
30%
Male Female
Many Times
Several Times
Once or Twice
13%
27%
24%
20% 18%20%
18%
26%
22%
20%
22% 24%
21%
17% 17%18%
13%
0%
5%
10%
15%
20%
25%
30%
1999 2003 2007 2011 2015
FemaleALL
Male

Page 5 of 14
Source: HealtheCNY Green = the top 50th percentile; Yellow = the 25th to 50th percentile; Red = the “worst” quartile.
OBESITY
(2013-2015) AGE-ADJUSTED DEATH RATE DUE TO SUICIDE deaths/100,000 population
8.0
AGE-ADJUSTED ER RATE DUE TO ADOLESCENT SUICIDE AND INTENTIONAL SELF-INFLICTED INJURY (2012-2014) ER visits/ 10,000 population aged 12-17
26.6
AGE-ADJUSTED ER RATE DUE TO MENTAL HEALTH (2012-2014) ER visits/ 10,000 population 18+ years
107.1
AGE-ADJUSTED ER RATE DUE TO PEDIATRIC MENTAL HEALTH (2012-2014) ER visits/ 10,000 population under 18 years 90.3
AGE-ADJUSTED ER RATE DUE TO SUICIDE AND INTENTIONAL SELF-INFLICTED INJURY (2012-2014) ER visits/ 10,000 population 18+ years 12.1
AGE-ADJUSTED HOSPITALIZATION RATE DUE TO MENTAL HEALTH (2012-2014) hospitalizations/ 10,000 population 18+ years
62.7
AGE-ADJUSTED HOSPITALIZATION RATE DUE TO SUICIDE AND INTENTIONAL SELF-INFLICTED INJURY (2012-2014) hospitalizations/ 10,000 population 18+ years
20.6
% DEPRESSION: MEDICARE POPULATION (2014) Percentage of Medicare beneficiaries who were treated for depression. Medicare is the federal health insurance program for persons aged 65 years or older, persons under age 65 years with certain disabilities, and persons of any age with end-stage renal disease (ESRD).
14.9%
% FREQUENT MENTAL DISTRESS (2014) Percentage of adults who stated that their mental health, which includes stress, depression, and problems with emotions, was not good for 14 or more of the past 30 days.
10.0%
MENTAL HEALTH PROVIDER RATE (2015) providers/ 100,000 population 238
POOR MENTAL HEALTH: 14+ DAYS (2014) Percentage of adults who stated that their mental health was not good 14 or more days in the past month
11.1%
11.4
65.6
117.4
77.5
20.5
89.1
32.2
16.2%
10.9%
143
14.2%

Page 6 of 14
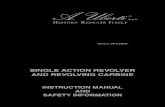
SUICIDE DEATHS BY YEAR (DATE RANGE: 1/1/2013-12/31/2015#)Source: Onondaga County Medical Examiner’s Office
#- As of 1/22/2016, there are pending cases dating back to April 2015. 2015 data is not final. Includes all suicide deaths occurring in Oneida County
SUICIDE DEATHS BY SEX BY YEAR (DATE RANGE: 1/1/2013-12/31/2015#)
Source: Onondaga County Medical Examiner’s Office #- As of 1/22/2016, there are pending cases dating back to April 2015. 2015 data is not final. Includes all suicide deaths occurring in Oneida County
3632
24
0
5
10
15
20
25
30
35
40
2013 2014 2015
6 7 7
0
5
10
15
20
25
30
35
2013 2014 2015
Female Male

Page 7 of 14
SUICIDE DEATHS BY RACE BY YEAR (DATE RANGE: 1/1/2013-12/31/2015#)Source: Onondaga County Medical Examiner’s Office
#- As of 1/22/2016, there are pending cases dating back to April 2015. 2015 data is not final. Includes all suicide deaths occurring in Oneida County
SUICIDE DEATHS BY AGE GROUP BY YEAR (DATE RANGE: 1/1/2013-12/31/2015#)Source: Onondaga County Medical Examiner’s Office
#- As of 1/22/2016, there are pending cases dating back to April 2015. 2015 data is not final. Includes all suicide deaths occurring in Oneida County
Asian Black Caucasian Native American Other 2013 0 2 31 0 1 2014 0 1 31 0 0 2015 0 1 23 0 0
2013 2014 2015 TOTAL
10 - 19 yrs. 2 1 0 3
20 - 29 yrs. 8 5 3 16
30 - 39 yrs. 8 6 4 18
40 - 49 yrs. 4 5 5 14
50 - 59 yrs. 8 5 5 18
60 - 69 yrs. 4 8 6 18
70 - 79 yrs. 1 0 1 2
80 - 89 yrs. 1 2 0 3 Total 36 32 24 92

Page 8 of 14
SUICIDE DEATHS BY TYPE BY YEAR (DATE RANGE: 1/1/2013-12/31/2015#)Source: Onondaga County Medical Examiner’s Office
#- As of 1/22/2016, there are pending cases dating back to April 2015. 2015 data is not final. Includes all suicide deaths occurring in Oneida County
2013 2014 2015 Total SUICIDE DEATHS BY ASPHYXIA
Hanging 7 12 11 30
Suffocation 1 0 0 1
Total 8 12 11 31 SUICIDE DEATHS BY FIREARM TYPE BY YEAR
Pistol 3 3 1 7
Revolver 6 1 5 12
Rifle 3 4 0 7
Shotgun 5 3 2 10
Total 17 11 8 36
SUICIDE DEATHS BY DRUG/TOXIN TYPE Ethylene Glycol 1 0 0 1
Mixed Drugs (Illicit, Rx) 1 1 0 2 Mixed Drugs (Illicit, Rx) and Ethanol 1 0 0 1
Mixed Drugs (OTC, Rx) 0 1 0 1 Mixed Drugs (Rx) 4 1 2 7
Mixed Drugs (Rx) and Ethanol 1 1 1 3 Single Drug (Rx) 2 0 1 3
Total 10 4 4 18 SUICIDE DEATHS BY ENVIRONMENTAL CONDITIONS
Carbon Monoxide 0 0 1 1
Hypothermia 1 0 0 1
Total 1 0 1 2
SUICIDE DEATHS BY MOTOR VEHICLE Pedestrian 0 2 0 2
Total 0 2 0 2
SUICIDE DEATHS BY SHARP FORCE Other-incised 0 1 0 1
Total 0 1 0 1 SUICIDE DEATHS BY DROWNING
Other 0 1 0 1
River 0 1 0 1
Total 0 2 0 2

Page 9 of 14
PERCEPTIONS, ISSUES, & CHALLENGES
The following represents a summary of feedback received from participants at the December 15th
OCHC brainstorming session (See Attachment A for listing of attendees) and follow up survey on
Mental Health; participants reviewed quantitative data and discussed issues, trends (i.e., social,
economic, and political), challenges and opportunities for improvement:
Lack of good housing and employment.
Those living in poverty often fall through the cracks; culturally,
many will not seek out assistance either due to stigma or you don't
talk about issues outside the family etc.
Unemployment, poverty
Lack of social support, high rate of poverty,
Inability to pay high salaries to attract more psychologists, psychiatrists, especially child specific.
Legal liability costs and general economics contribute to them not wanting to live here.
Need more prevention techniques, such as education.
Self-medication to cope with problems
Individuals with issues often are returned back to their unhealthy environment
Technology – social media postings, overuse of devices, lack sleep
“Imaginative” or creative and socially awkward youths can be labeled negatively
Poor parenting skills
More grandparents are raising grandchildren and often lack adequate understanding of technology
Inability to talk about issues
Relationship issues often contribute to suicide ideation.
Lack of outreach programs, appropriate services, long wait lists
Lack of shelters for women.
Difficulty navigating the system.
Lack of case management services.
Decline in case managers and other wrap around services.
Child and adult psychiatrists; recruitment and retention of mental health professionals.

Page 10 of 14
Lack of availability of psychiatric providers has resulted in a share of the population coping with
substance use, or their primary care doctor adjusting medications randomly.
A need for additional mental health clinics that focus on de-institutionalized clients.
Access to mental health professionals in the rural areas.
Access to crisis services.
Transitional case workers for 18-22 yr olds.
Reduced beds through the years.
A need for more respite beds
Need for skilled translators and community mental health outreach workers who are able to bridge
the gap between refugee/immigrant populations and mental health providers.
Funding for Mental Health First Aid and community support services for people with mental illness
A need for more trauma services and holistic healing modalities.
Program/services that prohibit people from becoming independent.
A need for a Comprehensive Psychiatric Emergency Program (CPEP) with all-inclusive psychiatric
assessments to increase access to services.
Need emergency department staff with sensitivity toward individuals diagnosed with mental illness.
PSAs to educate the general public in a different way rather than having to attend a formal
seminar/workshop that most do not have time to attend or are intimidated by industry jargon.
Something as simple as "if you see something, say something" - many people just need to know
what that "something' may be - what behavior, what conduct, what personal action, etc.
Funding holistic and community popular education methodologies.
Need summer education for students.
Children and youth.
Children ages 0-5; the number of children in preschool with psychological issues is alarming!
Children in homes without strong parents or guardians who offer safety, protection and guidance.
Those living in the more rural areas of the county
Immigrant and refugee populations (male and female) and survivors of gender-based violence.
Individuals with poor financial management skills or individuals that become victims.
Adolescent and middle income adults looking for quality care.
Individuals living in poverty.
Those with emergency psychiatric needs who just need a temporary change in location such as a
crisis residence.
Adults 18-65 with mental illness and individuals that are seriously and persistently mental ill,
mentally disabled individuals
Elderly
Homeless
Veterans returning to no job, no home, broken marriages, trying to deal with PTSD

Page 11 of 14
Still a stigma related to mental illness.
There is no voice in for people with mental illness.
Need more vocational rehabilitation training.
Need more peers and peer run community activities to encourage people to move on and grow.
Families are calling and voicing frustration on the fragmentation and long wait times for mental
health care. Workers in the field are saturated with a case load.
There are plenty of services but not enough providers and the 'fix' is not quick enough.
Mental health service providers are challenged to meet community needs. Community service
providers are being asked to do much more with less funding/resources. People needing inpatient
treatment can no longer stay in group homes as long as they need to.
Some feel it is impossible to get help and have no idea of how to get help
Long wait lists to see a therapist to get medications then a long time in between appointments
We are in need of more child specific mental health providers.
Below is a summary of some of the suggested areas for improvement taken from the above qualitative
analysis:
Increase case management, residential housing, peer involvement and congregate care case
management.
Tele-psychiatry and small clinics in rural areas.
More funding for community programs, more involvement of direct service providers in planning
programs and developing solutions
Increase collaboration with Oneida County Mental Health and the distribution of funds for
community mental health services.
Develop more housing and accessible shelters for people
with mental health issues.
Better access to services: Doors to offices open earlier or
later in the day, office locations closer to those they strive
to serve, transportation opportunities for those seeking
services.
Getting into the homes of families with children ages 0-5 and making mental health resources
available in elementary schools.
Better mental health supports for students in school.
More training to identify issues and screenings to identify a problem early on when the issue may
be more manageable and treatable.
Provider education regarding testing of specific labs to address potential mental health issues.

Page 12 of 14
Below is a listing of multi-agency partnerships or collaborative groups that are addressing the selected topic and related issues. It is not a listing of the host of individual agencies and provider resources in the community that provide services related to this topic**; it does, rather, identify some local coalitions or groups for which individual agencies and providers may want to collaborate with or support:
(facilitated by United Way of the Valley and Greater Utica Area and Utica Safe Schools Healthy Students): A variety of community providers that convene to discuss issues facing youth and families, trends, concerns, resources, facilitate effective interagency communication and coordination of services, respond to professional development needs and advocate for needs.
(facilitated by Oneida County Health Department): Public health partners meet quarterly to analyze county data on multiple health topics, provide feedback on perceptions and underlying causes, identify collaborative opportunities and evidence-based resources to address the issue, and compile the information into a Health Report Card.
(facilitated by SUNY POLY): A group of individuals and organizations that are working collaboratively to develop and implement a community wide intervention plan to prevent the progression of negative physical and mental health implications of ACEs through increased public education and awareness and by strengthening the support systems that serve individuals affected by ACEs.
(facilitated by Oneida County Mental Health):
Substance abuse providers, law enforcement, emergency department staff, first responders, MCAT, MHD staff, and others, meet to review and promote better practices for responding to 9.41 situations (Mental Health Law permitting officers to take into custody a person who appears to be mentally ill).
(facilitated by United Way of the Valley
and Greater Utica): This group is charged with evaluating, accessing and providing community involvement and solutions to the issue of persistent poverty in the community.
(facilitated by United Way of the Valley and Greater Utica):
A collaborative education initiative to address students' social, emotional, literacy and physical needs. The goal is to unite families, schools, and community resources to prepare children to reach their full potential by focusing on school readiness. It is a partnership with Central Valley, Dolgeville and Remsen School Districts, the Literacy Coalition of Herkimer and Oneida Counties, Oneida County Youth Council, Stop ACES, and the new R4K Coalition.

Page 13 of 14
Coalition for Evidence-Based Policy
The Community Guide – The Community Guide
County Health Rankings: What Works for Health
HealtheCNY Promising Practices
NOTES
*Data: This Report Card is only a summary of data related to the topic of focus in this report card; however, additional relevant data are available at the following sources: NYSDOH Data Sources HealtheCNY.org **Community Programs and Services: Comprehensive information regarding individual health and human services and programs in the community to support issues related to this and other report card issues can be found at the 2-1-1 Mid-York website at http://www.211midyork.org/ or by dialing 2-1-1.
All OCHC Report Cards and other materials are available at:
HealtheCNY.org/OneidaCountyHealthCoalition

Page 14 of 14
Attendees of OCHC Quarterly Report Card Discussion: Mental Health December 15, 2016
Adams, Melanie – Oneida County Health Department
Bassett, Chip – Herkimer-Oneida Comprehensive Planning Program
Chares, Deanna – Regional Primary Care Network
Conklin, Katrina – Utica WIC
Drake, Krista – Oneida County Health Department
Ellis, Phyllis – Oneida County Health Department
Fentiman, Sandra – Mohawk Valley Health Systems
Finn, Carole – Oneida County Department of Mental Health
Hanrahan, June – Oneida County Office for the Aging
O’Brien, Robin – Oneida County Department of Mental Health
Paulus Jeannette – Oneida County Department of Mental Health
Petronio, Emmie – Planned Parenthood Mohawk Hudson, Inc.
Przelomic, Selden – Oneida County Department of Mental Health
Schnier, Diane – Mohawk Valley Perinatal Network
Stein, Tracy – House of the Good Shepherd
Tanner, Lisa – Kids Oneida
Vail, Jane – CNY Health Homes, Inc.
Worden, Lisa – Oneida County Health Department