
Isolation Unit COVID-19 - bcpft.nhs.uk
9
IPC SOP: Isolation Unit COVID-19 Page 1 of 9 version 1.0 March 2020 Infection Prevention and Control Assurance - Standard Operating Procedure 35 (IPC SOP 35) Isolation Unit – COVID-19 Why we have a procedure? The spread of COVID-19 between patients in our in-patient services can be reduced by physical isolation of symptomatic patients in a dedicated isolation unit. Following this procedure will also ensure compliance with the Health and Social Care Act 2008: Code of Practice for the NHS for the Prevention and Control of Healthcare Associated Infections (revised January 2015) and National guidance on COVID-19. The purpose of this document is to provide clear infection prevention & control guidelines and when caring for a patient requiring isolation due to COVID-19. What overarching policy the procedure links to? This procedure is supported by the Infection Prevention & Control Assurance Policy. Which services of the trust does this apply to? Where is it in operation? Group Inpatients Community Locations Mental Health Services Meadow Ward Learning Disabilities Services Children and Young People Services Who does the procedure apply to? (staff roles and responsibilities) All staff involved in the care of patients on the dedicated isolation unit should adhere to these standard procedures when dealing with a known or suspected case of COVID-19. Matrons, Service Managers, Ward Managers & ALL clinicians involved in the delivery of care Facilities staff When should the procedure be applied? (Context) Whenever it is suspected or confirmed that a patient meets the criteria for transfer to the dedicated isolation facility
Transcript of Isolation Unit COVID-19 - bcpft.nhs.uk

IPC SOP: Isolation Unit COVID-19 Page 1 of 9 version 1.0 March 2020
Infection Prevention and Control Assurance - Standard Operating Procedure 35 (IPC SOP 35)
Isolation Unit – COVID-19
Why we have a procedure?
The spread of COVID-19 between patients in our in-patient services can be reduced by physical isolation of symptomatic patients in a dedicated isolation unit. Following this procedure will also ensure compliance with the Health and Social Care Act 2008: Code of Practice for the NHS for the Prevention and Control of Healthcare Associated Infections (revised January 2015) and National guidance on COVID-19.
The purpose of this document is to provide clear infection prevention & control guidelines and when caring for a patient requiring isolation due to COVID-19.
What overarching policy the procedure links to?
This procedure is supported by the Infection Prevention & Control Assurance Policy.
Which services of the trust does this apply to? Where is it in operation?
Group Inpatients Community Locations
Mental Health Services Meadow Ward
Learning Disabilities Services
Children and Young People Services
Who does the procedure apply to? (staff roles and responsibilities)
All staff involved in the care of patients on the dedicated isolation unit should adhere to these standard procedures when dealing with a known or suspected case of COVID-19.
Matrons, Service Managers, Ward Managers & ALL clinicians involved in the delivery of care
Facilities staff
When should the procedure be applied? (Context)
Whenever it is suspected or confirmed that a patient meets the criteria for transfer to the dedicated isolation facility

IPC SOP: Isolation Unit COVID-19 Page 2 of 9 version 1.0 March 2020
How to carry out this procedure (step step-by-step information)
Additional Information/ Associated Documents
Infection Prevention & Control Assurance Policy
Standard Precautions SOP
Transmission Based Precautions SOP
Waste Management Policy & associated procedures
Hand hygiene policy Novel Coronavirus (COVID-19) has been designated a high consequence infectious disease (HCID). COVID-19 for most individuals causes mild to moderate illness, but in addition may result in pneumonia or severe acute respiratory infection. In order that patients who are isolated in a single room do not feel ostracised, the reason for isolation should be explained to the patient, their close family contacts and carers as best as possible, so that they are aware that no visiting will be allowed. AIMS
Identify suspected cases as soon as possible to prevent potential transmission of infection to other patients and staff.
Avoid direct physical contact and avoid exposure to respiratory and other secretions
To give psychological support and reassurance to the patients whilst he/she is in isolation
To ensure all staff (including housekeeping staff) are aware of the correct precautions to take
To protect vulnerable patients and staff DEFINITIONS
Source Isolation Used for patients who are sources of pathogenic microorganisms which may spread from them and infect other patients and/or staff, i.e. isolating the source patient to prevent transfer of infection
Cohort Nursing Grouping of infectious patients and nursing them within an area of a hospital ward as a strategy for controlling infection
Standard Isolation (Source Isolation)
For most communicable diseases, single room with hand wash sink
Patients requiring isolation due to COVID-19 should be cared for in a single bedroom (ideally en-suite) and with a hand wash sink. Where several patients have the same infection they may be nursed together in one bay, this is called co-horting. The Infection Prevention & Control Team will advise accordingly. If a suitable isolation room is not immediately available on a ward, liaison must take place between the Nurse-in-Charge, Service Manager/Matron and the Infection Prevention & Control Team to enable the rationalisation of isolation needs. This may involve the transfer of the patient to the dedicated isolation facility on Meadow Ward. An incident

IPC SOP: Isolation Unit COVID-19 Page 3 of 9 version 1.0 March 2020
form (DATIX) must be completed for all known/suspected cases of COVID-19, so that appropriate action is taken. * General Do’s & Don’ts – see Appendix 1 * Caring for patients in Source Isolation - see Appendix 2 * General isolation precautions – see Appendix 3 * Plan of care for a patient with known/suspected COVID-19 – see Appendix 4
Where do I go for further advice or information?
Infection Prevention & Control Team
Your Service Manager, Matron, General Manager, Head of Nursing, Group Director or Physical Health Team
Your Group Governance Staff
Training Staff may receive training in relation to this procedure, where it is identified in their appraisal or as part of the specific development needs for their role and responsibilities. Please refer to the Trust’s Mandatory & Risk Management Training Needs Analysis for further details on training requirements, target audiences and update frequencies Monitoring / Review of this Procedure In the event of planned change in the process(es) described within this document or an incident involving the described process(es) within the review cycle, this SOP will be reviewed and revised as necessary to maintain its accuracy and effectiveness.
Equality Impact Assessment Please refer to overarching policy
Data Protection Act and Freedom of Information Act Please refer to overarching policy

IPC SOP: Isolation Unit COVID-19 Page 4 of 9 version 1.0 March 2020
General Notes - Do’s & Don’ts DO:
Wash hands BEFORE entering the unit and regularly throughout your shift and ALWAYS before/after rest breaks and prior to leaving the ward. Ensure ALL staff entering the unit are BARE BELOW THE ELBOWS!
Staff must only bring essential items to work e.g. change of clothes, keys, phone, food/drinks. Remember to clean your personal stuff & bag too. N.B. mobile phones can carry more germs than the toilet seat!
Staff food & drink MUST be labelled (name/date), ideally food should be in a clean plastic container, which should be wiped with a disposable detergent wipe before placing into the staff fridge. Any items not used within 24 hours or non-compliant with this advice, MUST be removed/discarded. The fridge temperature MUST be checked and recorded daily & the fridge cleaned daily. The Nurse-in-Charge must delegate accordingly to ensure this task is completed & documented.
Ensure the correct use of PPE by all staff on the unit including the donning & doffing procedures (See enclosed posters). Staff should be confident and competent in the correct use of personal protective equipment.
An allocated staff member should shop locally for patients ESSENTIAL requirements only, note - this should be kept to a minimum. When returning to the unit with patients shopping, ALL packaged items MUST be decontaminated using a disposable detergent wipe BEFORE passing it to the patients (remember to also clean any contact surfaces involved in this process).
Support each other, everyone is anxious and may have feelings of being overwhelmed – its normal – remember your colleagues as well as the patients!
Face masks must be changed if they become moist when in contact with a patient for unusually long periods. See donning/doffing poster or our useful video on the intranet and follow the procedure carefully to reduce the risk of self-contamination.
Clean your locker after removing your personal belongings and before you leave the unit.
DONT’s
To avoid transmission DO NOT touch your face with unwashed hands and especially when wearing any face protection or gloves.
DO NOT wear your gloves & apron for contact with more than one patient.
DO NOT travel home in your uniform – always change and wash your hands. (If laundry facilities are not available at work, place your uniform/work-wear in a carrier bag a. At home discard the carrier bag & place the clothing directly into the washing machine & wash on a hot wash (max temperature the fabric will allow), followed ideally by tumble dry & iron).
DON’T bottle up your emotions/feelings – its normal to feel this way. Talk to a colleague, your manager, occupational health or staff support. Remember we are all in this together.
Appendix 1

IPC SOP: Isolation Unit COVID-19 Page 5 of 9 version 1.0 March 2020
SOURCE ISOLATION – for patients with a known or suspected infection
*The decision to isolate a patient or clinical area should be based on the infection risk posed and decided after discussion with the IPC Team.
Preparing the Source Isolation Room
Care in Isolation Staff & Visitors Discontinuation of Isolation
Ideally the patient must be cared for in a single room with a hand wash basin and preferably an en-suite toilet.
The patient should be informed of the reason & need to comply with isolation requirements.
The care plan must reflect individual specific requirements to prevent transmission.
Ensure that all unnecessary equipment is removed from the room before placing the patient.
Ensure that all the equipment in the room is designated to the isolated patient if possible and safe to do so (i.e. commode, BP machine etc., & clearly labelled).
All personal belongings and equipment should be washable or disposable if possible.
Keep charts and care plans outside the room.
Ensure all clinical waste bags. Paper towels, alcohol hand gels etc. are to hand and if necessary locked in a cupboard.
Place a source isolation sign on the door
Standard infection control precautions must be adhered to at all times.
Hand hygiene must be performed before entering and prior to leaving the room.
Wear all appropriate personal protective equipment (PPE) as directed - disposable gloves, apron and fluid repellent mask to be donned before entering the room and removed in the correct order sequence before leaving the room (observe social spacing) followed by thorough hand washing.
The patient should be advised regarding good respiratory hygiene e.g. catch it, bin it, kill it. Tissues should be provided.
All bodily fluid spillage, waste & soiled linen to be dealt with immediately and removed from the room.
Place all used sharps into an approved sharps bin immediately after use and store safely between uses.
The patient should be encouraged to use their own en-suite facility only during the period of isolation (ADL bathroom use seek IPCT advice).
Visits to other departments are strictly restricted.
As far as possible keep the bedroom door closed at all times, ensuring the situation is regularly assessed and re-evaluated.
Ensure PPE is always available for use.
Bed linen should be changed daily as a minimum.
The room MUST be cleaned at least daily and frequent touch points cleaned more frequently throughout the day.
Remember alcohol gel can only be used on visibly clean hands
Explain in appropriate language the reasons for patient isolation.
Advise on the reason for suspension of visiting and restriction of allowed goods for all patients in isolation.
Visitors and staff from other departments must report to the Nurse-in-Charge before entering the ward – these must be kept to an absolute minimum.
Bank/agency staff working on the isolation ward should not work in any other areas to reduce the risks of further transmission
If unsure discuss specific requirements with the Infection Prevention & Control Team.
Isolation may be discontinued when the patient is no longer a risk for spreading infection to others and following the approval of the Infection Prevention & Control Team (this will be after a minimum of 7 days but may be longer in some cases).
The room must be cleaned thoroughly daily (even if the patient is staying in the room). It should be cleaned again thoroughly when it is vacated and curtains laundered (disposable curtains must be discarded & replaced before the room can be re-occupied).
The care plan must be reviewed and updated and the patient notes must record when the isolation was discontinued.
APPENDIX 2

IPC SOP: Isolation Unit COVID-19 Page 6 of 9 version 1.0 March 2020
GENERAL ISOLATION PRECAUTIONS HANDS Hand washing before and after contact with the patient and their immediate environment is the single most important
measure in preventing the spread of infection. This also includes prior to and after removal of PPE.
‘Bare below the elbows’ & the Hand Hygiene Policy guidelines must be adhered to at all times.
Alcohol gel can be used if hands are clean. Staff should also ensure they used an approved moisturizing cream to reduce skin drying.
PPE Gloves, aprons & face protection must be donned prior to direct patient contact (see Donning Poster)
Gloves, aprons & face protection must be removed in the correct order & discarded as clinical waste prior to leaving the room & hand washed (see Doffing Poster)
Face/eye protection to be worn as/when required for personal care e.g. within 2 metre contact with the patient in same room
ROOM DOOR Provided the patient’s safety is not compromised, the isolation room door should remain closed. Regular checking must be clearly described in the individuals care plan including the frequency.
A sign indicating type of isolation precautions required should be placed on the door
ACTIVITES/ THERAPIES
All group/communal activities must be suspended for duration of isolation – specific advice can be sought from the Infection Prevention & Control Team. Individualised therapeutic interventions should be documented.
VISITORS Generally NO visiting allowed to the unit. No food, toiletries or other items to be accepted onto the unit on behalf of patients. (Staff will be allocated to shop daily for essential items if required for the patients’ individual needs). All packaged items to be decontaminated using a detergent wipe before being given to the patients and hands must be washed.
EQUIPMENT Limit the number of items taken into or stored in the isolation room to essential equipment only.
All equipment must be cleaned after use & when removed from the room prior to re-use
CROCKERY & CUTLERY
No special precautions, cleaning crockery (including medicine tots if not disposable) should only be carried out in a dishwasher (avoid quick cycle).
LINEN Infected/heavily soiled linen must be placed into an Alginate water soluble bag & secured then into a linen bag. Bags must be secured & removed immediately and placed ready for collection. Patients’ personal laundry must be managed carefully as per Trust guidelines.
WASTE All waste is classed as clinical waste. Bins to be emptied at least daily. Further information available in the Waste Management policy & procedures.
DECONTAMINATION BLOOD/BODY FLUID
Any spillage of blood or body fluid should be made safe prior to regular cleaning using a chlorine releasing agent (see standard infection control procedures).
CLEANING OF ROOMS
Separate cleaning equipment must be reserved for each isolation room i.e. disposable mops/cloths
Rooms must be cleaned daily as a minimum as per standard procedures.
Nursing staff are responsible for the standard of hygiene in isolation rooms and for decontaminating spillages of blood & body fluids, in addition to identifying hazards and undertake a risk assessment before allowing domestic staff to clean the room
Domestic staff should be advised on specific precautions by the Nurse-in-Charge/Infection Prevention & Control prior to entering/cleaning the room.
APPENDIX 3
IPC SOP: Isolation Unit COVID-19 Page 7 of 9 version 1.0 March 2020
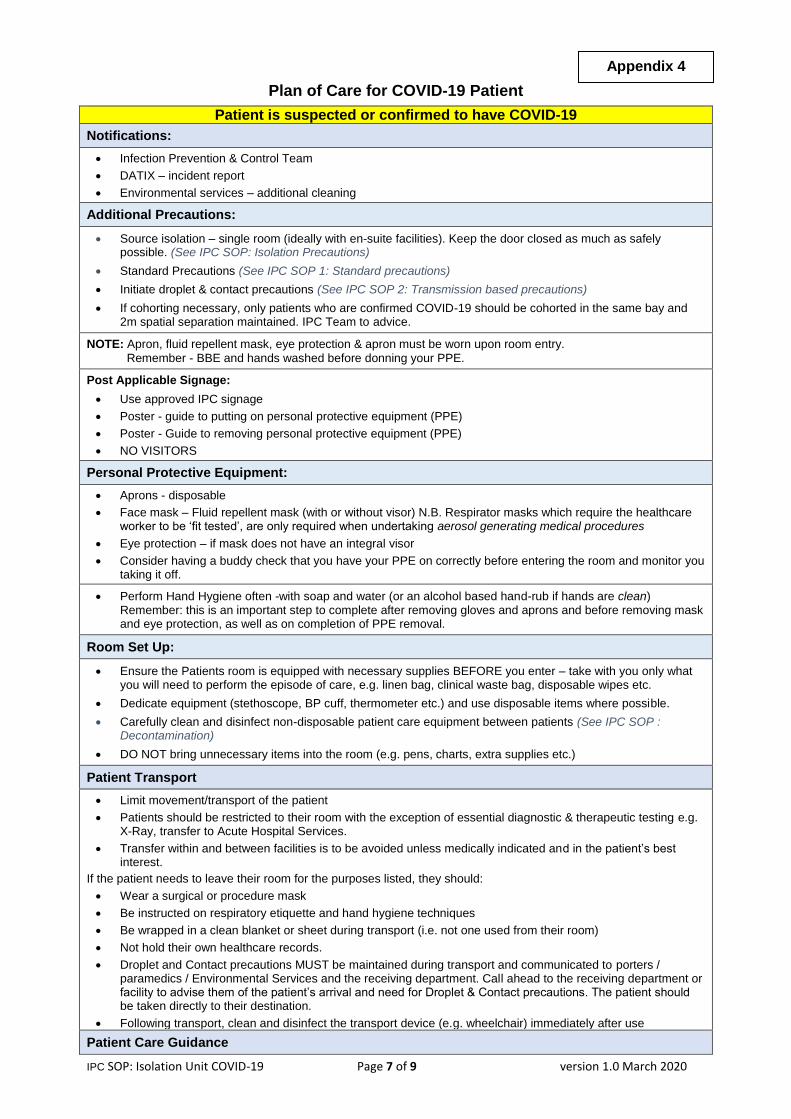
Plan of Care for COVID-19 Patient
Patient is suspected or confirmed to have COVID-19
Notifications:
Infection Prevention & Control Team
DATIX – incident report
Environmental services – additional cleaning
Additional Precautions:
Source isolation – single room (ideally with en-suite facilities). Keep the door closed as much as safely possible. (See IPC SOP: Isolation Precautions)
Standard Precautions (See IPC SOP 1: Standard precautions)
Initiate droplet & contact precautions (See IPC SOP 2: Transmission based precautions)
If cohorting necessary, only patients who are confirmed COVID-19 should be cohorted in the same bay and 2m spatial separation maintained. IPC Team to advice.
NOTE: Apron, fluid repellent mask, eye protection & apron must be worn upon room entry.
Remember - BBE and hands washed before donning your PPE.
Post Applicable Signage:
Use approved IPC signage
Poster - guide to putting on personal protective equipment (PPE)
Poster - Guide to removing personal protective equipment (PPE)
NO VISITORS
Personal Protective Equipment:
Aprons - disposable
Face mask – Fluid repellent mask (with or without visor) N.B. Respirator masks which require the healthcare worker to be ‘fit tested’, are only required when undertaking aerosol generating medical procedures
Eye protection – if mask does not have an integral visor
Consider having a buddy check that you have your PPE on correctly before entering the room and monitor you taking it off.
Perform Hand Hygiene often -with soap and water (or an alcohol based hand-rub if hands are clean) Remember: this is an important step to complete after removing gloves and aprons and before removing mask and eye protection, as well as on completion of PPE removal.
Room Set Up:
Ensure the Patients room is equipped with necessary supplies BEFORE you enter – take with you only what you will need to perform the episode of care, e.g. linen bag, clinical waste bag, disposable wipes etc.
Dedicate equipment (stethoscope, BP cuff, thermometer etc.) and use disposable items where possible.
Carefully clean and disinfect non-disposable patient care equipment between patients (See IPC SOP : Decontamination)
DO NOT bring unnecessary items into the room (e.g. pens, charts, extra supplies etc.)
Patient Transport
Limit movement/transport of the patient
Patients should be restricted to their room with the exception of essential diagnostic & therapeutic testing e.g. X-Ray, transfer to Acute Hospital Services.
Transfer within and between facilities is to be avoided unless medically indicated and in the patient’s best interest.
If the patient needs to leave their room for the purposes listed, they should:
Wear a surgical or procedure mask
Be instructed on respiratory etiquette and hand hygiene techniques
Be wrapped in a clean blanket or sheet during transport (i.e. not one used from their room)
Not hold their own healthcare records.
Droplet and Contact precautions MUST be maintained during transport and communicated to porters / paramedics / Environmental Services and the receiving department. Call ahead to the receiving department or facility to advise them of the patient’s arrival and need for Droplet & Contact precautions. The patient should be taken directly to their destination.
Following transport, clean and disinfect the transport device (e.g. wheelchair) immediately after use
Patient Care Guidance
Appendix 4

IPC SOP: Isolation Unit COVID-19 Page 8 of 9 version 1.0 March 2020
General Care of the Patient
Limit the number of staff entering the patients’ room to essential personnel.
Avoid unnecessary entries into the room. Ensure you have all necessary equipment/supplies on entry, and try to batch care tasks i.e. provide personal care while in the room to deliver scheduled medications or perform vital sign (NEWS) observations.
Closely monitor patient for clinical deterioration and ensure rapid escalation to higher level of care as required. Have a plan in place for this in advance.
Aerosol Generating Medical Procedures (e.g. intubation, extubating, manual ventilation & suctioning, tracheostomy procedures) require Airborne Precautions. N.B. these procedure are generally only performed in Acute Hospital Trusts (See when to use an FFP3 respirator when caring for a patient with COVID-19, Public Health England, 2020).
Environmental Cleaning
ALL horizontal and frequently touched surfaces should be cleaning with detergent, followed by a chlorine releasing disinfectant (1,000 PPM concentration) at least twice daily and when visibly soiled. Ensure the ‘contact time’ of the disinfectant is achieved as per the manufacturer’s guidelines.
Standard cleaning procedures for Isolation Rooms must be followed.
Ensure that all unused disposable equipment and supplies are discarded during the Terminal Cleaning of the patients’ room (discharge clean) in addition to the routine discharge cleaning procedures.
Discharge Information:
Discharges to home/community when patient is medically stable:
Assess stage of exposure or disease communicability.
Consult with the Infection Prevention & Control Team/Consultant Microbiologist/PHE
Provide patient with information from Public Health England on self-isolation. This information is available in a variety of languages. Patients may be required to self-isolate at home if the period of communicability of the illness is not over. (If unsure the Infection Prevention & Control Team can advise).
Provide patient with a mask to wear during transport home if still considered infectious. Patients should not take public transport. Precautions will remain in place until the period of communicability and as directed by Public Health. (See gov.uk/coronavirus for latest information).
Care providers in the home or community should be advised of the need for droplet and contact precautions. Precautions will remain in place until the completion of the period of communicability and as directed by Public Health.
Additional Information:
Manage these patients with the same approach as you would any patient with Influenza-like illness, following the guidelines above.
Please contact the Infection Prevention & Control Team for additional support and any questions that may arise.
This guidance may change as new information becomes available or there are new developments in the current Pandemic situation. Always ensure this care plan is obtained directly from the Trust’s Intranet to
ensure you have the most up-to-date version.

IPC SOP: Isolation Unit COVID-19 Page 9 of 9 version 1.0 March 2020
Standard Operating Procedure Details – to be completed by Corporate Governance
Review and Amendment History - to be completed by Corporate Governance
Version Date Description of Change
1.0 Mar 2020
This is a new procedure developed in response to the COVID-19 Pandemic.
Unique Identifier for this SOP is BCPFT-COI-POL-05-35
State if SOP is New or Revised New
Policy Category Infection Prevention & Control
Executive Director whose portfolio this SOP comes under
Executive Director of Nursing, AHPs and Governance
Policy Lead/Author Job titles only
Infection Prevention & Control Team
Committee/Group Responsible for Approval of this SOP
COVID-19 Incident Management Team
Month/year consultation process completed
March 2020
Month/year SOP was approved April 2020
Next review due March 2021 unless National Guidance changes
Disclosure Status ‘B’ can be disclosed to patients and the public


















