ISLINGTON LOCAL MEDICAL COMMITTEE MEETING AGENDA · To be held from 1.30 pm to 4.30 pm on Wednesday...
115
The professional voice of general practice in Islington Londonwide LMCs is the brand name of Londonwide Local Medical Committees Limited Registered and office address: Tavistock House North, Tavistock Square, London WC1H 9HX. T. 020 7387 2034/7418 F. 020 7383 7442 E. [email protected] www.lmc.org.uk Registered in England No. 6391298. Londonwide Local Medical Committees Limited is registered as a Company Limited by Guarantee Chief Executive: Dr Michelle Drage ISLINGTON LOCAL MEDICAL COMMITTEE MEETING To be held from 1.30 pm to 4.30 pm on Wednesday 24 October 2012 Laycock Professional Development Centre, Laycock Street, London N1 1TH Lunch will be available from 1 pm. LMC Members only 1.45 – 3.00 pm AGENDA 1.0 Apologies 2.0 2.1 2.2 Standing Orders of LMC and Roles and responsibilities of LMC members To formally adopt the Standing Orders (pages 3-7) To receive and adopt the LMC members Roles and responsibilities (pages 8-10) 3.0 Membership: 3.1 3.2 3.3 3.4 3.5 To receive members’ Terms of Office (page 11) To elect a Chair to serve until 31 August 2014 in accordance with the attached Roles and Responsibilities and Nomination (pages 12-16) To elect a Vice Chair to serve until 31 August 2014 (pages 17-18) To discuss the vacancy To discuss co-options: • Co-options representing a particular class of experience • Co-option of a Practice Manager as an observer • Co-option of a Practice Nurse as an observer 4.0 4.1 4.2 Local LMC Priorities To discuss the LMC’s local priorities and to identify objectives: Suggested priorities could include the following (this is not exhaustive and may not be relevant to your local area) • Education and training • Sources of practice funding • Improvement and development of premises • Engagement with CCGs and CCG Boards To discuss how the committee will lead on and support the agreed objectives 5.0 Schedule and format of meetings for 2013 To discuss the schedule and format of LMC meetings for 2013 in view of the changes in the NHS and as a result of any discussions which take place under item 4.0. 1
Transcript of ISLINGTON LOCAL MEDICAL COMMITTEE MEETING AGENDA · To be held from 1.30 pm to 4.30 pm on Wednesday...

The professional voice of general practice in Islington Londonwide LMCs is the brand name of Londonwide Local Medical Committees Limited Registered and office address: Tavistock House North, Tavistock Square, London WC1H 9HX. T. 020 7387 2034/7418 F. 020 7383 7442 E. [email protected] www.lmc.org.uk Registered in England No. 6391298. Londonwide Local Medical Committees Limited is registered as a Company Limited by Guarantee Chief Executive: Dr Michelle Drage
ISLINGTON LOCAL MEDICAL COMMITTEE MEETING
To be held from 1.30 pm to 4.30 pm on Wednesday 24 October 2012
Laycock Professional Development Centre, Laycock Street, London N1 1TH Lunch will be available from 1 pm.
LMC Members only
1.45 – 3.00 pm
AGENDA
1.0 Apologies
2.0 2.1 2.2
Standing Orders of LMC and Roles and responsibilities of LMC members To formally adopt the Standing Orders (pages 3-7) To receive and adopt the LMC members Roles and responsibilities (pages 8-10)
3.0 Membership: 3.1 3.2 3.3 3.4 3.5
To receive members’ Terms of Office (page 11) To elect a Chair to serve until 31 August 2014 in accordance with the attached Roles and Responsibilities and Nomination (pages 12-16) To elect a Vice Chair to serve until 31 August 2014 (pages 17-18) To discuss the vacancy To discuss co-options:
• Co-options representing a particular class of experience
• Co-option of a Practice Manager as an observer • Co-option of a Practice Nurse as an observer
4.0 4.1
4.2
Local LMC Priorities To discuss the LMC’s local priorities and to identify objectives: Suggested priorities could include the following (this is not exhaustive and may not be relevant to your local area)
• Education and training • Sources of practice funding
• Improvement and development of premises
• Engagement with CCGs and CCG Boards To discuss how the committee will lead on and support the agreed objectives
5.0 Schedule and format of meetings for 2013 To discuss the schedule and format of LMC meetings for 2013 in view of the changes in
the NHS and as a result of any discussions which take place under item 4.0.
1

6.0 Minutes and matters arising: 6.1 To confirm the minutes from the Islington Part 1 LMC meeting on 22 August 2012
(pages 19-26) 6.2 To receive the draft and unconfirmed minutes of the Part 2 LMC meeting on 22 August
2012 (pages 27-36) 6.2.1 Physiotherapy services provided by Whittington Health (minute 3.1.4 refers)
Members to advise of any problems regarding the physiotherapy services
7.0 Members reports of meetings attended 7.1 7.2 7.3
Feedback from interim meeting on 26 September 2012 Feedback from Primary Care Development meeting on 4 October 2012 Reports from members of any other meetings attended
8.0 Islington issues 8.1 Local enhanced services:
• To note process for approval of LESs in Islington (page 37)
• To discuss the proposed LESs and spend for 2012/13
• Clinical commissioning LES (pages 38-59) • Diabetes LES – to follow
• Prevalence Gap LES – to follow 8.2 List inflation/deflation – to discuss 8.3 Section 251 application for linkage of GP data with hospital admissions (pages 60-104) 8.4 Sessional GP issues 8.5 Payment invoices from NCL Cluster
9.0 NCL Cluster and LMC Chairs Group meeting: 9.1 Draft and unconfirmed minutes of NCL Cluster and LMC Chairs meeting on 28 August
2012 (pages 105 – 114)
10.0 10.1
Londonwide LMCs Update LEAD Reference Group To identify a member(s) who would be interested on joining the LEAD Reference Group to ensure that LEAD remains fit for purpose in its provision of training for practices (time commitment would be a maximum of one hour a month)
11.0 11.1
Items to Receive LEAD Events (page 115)
12.0
Date of the next meeting 19 December 2012
13.0 Any Other Business
2

STANDING ORDERS ISLINGTON LOCAL MEDICAL COMMITTEE
Nothing in these Standing Orders shall override conditions in the Committee's Constitution or of Contracts of Employment. OFFICERS
1. The Officers shall be elected members of the Committee and shall consist of a Chair and a Vice-Chair.
2. The Committee at its first meeting after the biennial election shall proceed to
elect the Officers who shall hold office for the next two years, provided that they remain elected members of the Committee.
3. In the event of the resignation, death or removal from office as hereinafter
mentioned of an Officer the Committee shall as soon as may be appoint a member of the Committee in place of such resigned, deceased or removed Officer.
4. An Officer may be removed from office by a resolution to that effect carried by
two thirds of the members of the Committee present and voting at an extraordinary meeting of the Committee summoned for that purpose.
5. No officer may hold an appointment as a member of the Board of the Islington
Primary Care Trust or NHS London or of their successor bodies, and no Officer shall serve as Chair of the Professional Executive Committee or the successor
body. DUTIES OF THE OFFICERS 6. The Chair shall preside at meetings of the Committee and, if absent, the Vice-
Chair shall preside. In the absence of both, the members present at the
meeting shall appoint someone of themselves to act as Chair for that meeting. The Vice-Chair shall also act in the absence of the Chair in all other matters where responsibility is given to the Chair in these Standing Orders.
FUNDING OF THE COMMITTEE
7. The funds of the Committee will be consolidated in the accounts of Londonwide
LMCs Ltd. OFFICIALS OF THE COMMITTEE
8. The Secretary of the Committee shall be the person holding the relevant Contract of Employment with Londonwide LMCs Ltd.
3

9. The Secretary shall be responsible in respect of these Standing Orders for
(1) The issue of notices summoning meetings of the Committee and of any sub-committees.
(2) The keeping of the minutes of all meetings. (3) The safe custody of books, registers and documents.
(4) The conduct of all correspondence. (5) Receiving and bringing to the notice of the Chair all requisitions by
members. (6) Such other matters as the Committee may, from time to time, decide.
10. In the absence of the Secretary the above duties may be assumed by other
staff members of Londonwide LMCs Ltd. 11. The Committee's accountant shall be the accountant appointed by
Londonwide LMCs Ltd to examine the accounts. MEETINGS 12. The Committee shall agree an annual schedule of meetings. If the Chair
deems there is insufficient business, a meeting may be cancelled and the members be notified of the decision.
13. An extraordinary meeting of the Committee shall be summoned on the direction
of the Chair or on the requisition in writing to the Secretary of not less than a quorum of the members of the Committee stating the business to be discussed at such extraordinary meeting.
14. An extraordinary meeting shall transact only the business for which it is
summoned. 15. Agendas will be sent to members seven days before a meeting and supporting
papers and minutes of the preceding meeting, whenever possible, shall accompany the agenda. A notice shall be presumed to have been served one day after posting.
A member desiring a matter to be included on an agenda shall make her/his
request in writing to the Chair or Secretary, at least 10 days before the meeting. Requests made less than 10 days before a meeting may be included on the agenda at the discretion of the Chair or Secretary.
4

PROCEDURE AT MEETINGS
16. At each ordinary meeting of the Committee the minutes of the last ordinary meeting together with the minutes of any extraordinary meeting of the Committee held since the date of the last ordinary meeting shall be submitted for approval.
17. No seconder shall be required for any motions or amendments of which prior
notice has been given in writing or in connection with the presentation of a
report of a sub-committee. All other motions or amendments after being proposed must be seconded.
18. If an amendment to an original motion has been moved and where necessary,
seconded, no second or subsequent amendment shall be moved until the first has been disposed of.
19. If an amendment is carried, the motion, as amended, shall take the place of the
original motion and shall become the question upon which any further amendment shall be moved.
20. Every question at a meeting of the Committee (other than for which a two-thirds
majority is required) shall be determined by a majority of the votes of the
members of the Committee present and voting, and in the case of an equal division of votes, the Chair of the meeting shall have a second or casting vote.
21. Every vote shall be taken by show of hands unless a resolution to the contrary
is moved and where necessary, seconded and supported by a majority of members of the Committee in which event the vote shall be taken by ballot in
such manner as the Chair of the meeting may determine. 22. No motion to rescind a resolution which has been passed within the preceding
six months shall be proposed until after the expiration of six calendar months from the time when it was originally or last proposed and no motion which has been rejected shall, except on the recommendation of a subcommittee, be again proposed until after the expiration of six calendar months from the time
when it was originally or last proposed. 23. Subject to the provisions of these Standing Orders, all questions relating to the
procedure at a meeting of the Committee shall be determined by the Chair of the meeting whose decision shall be final.
MINUTES 24. Action Minutes of the proceedings at every meeting of the Committee and of
every general meeting of the electorate and a record of the attendances at such meetings shall be kept by the Secretary.
25. Unless and until the contrary is proved every meeting where-of the proceedings are recorded in the minutes as aforesaid shall be deemed to have been duly convened and held and all the members present as such meetings shall be deemed to have been duly qualified.
5

GENERAL MEETING OF THE ELECTORATE
26. A General Meeting of the Electorate shall be held if the Chair so decides, or the Committee so decides, or on a requisition in writing to the Secretary of one half of the elected members of the Committee, or on requisition in writing to the Secretary of not less than 25 members of the electorate, stating in each case the business to be transacted at the meeting and such meeting shall be held at a time and place to be determined by the Committee.
27. Notice of a General Meeting of the Electorate will be circulated to all members of the Committee and the Electorate giving the time, date and place of such meeting of which not less that 21 days' notice will be given. The agenda, which shall include all motions of which notice has been given as hereinafter mentioned, shall be circulated to the Electorate not less than seven days before the day of such meeting.
28.
which a member of the electorate shall desire to be considered at a general meeting of the Electorate.
QUORUM OF A MEETING OF THE COMMITTEE 29. One third of the members of the Committee, or if one third is not a whole
number, the next whole number above one third, shall form a quorum of the Committee provided that at least three-quarters of the members present shall be elected representatives of practitioners on the list and, where relevant, elected (or co-opted) representatives of practitioners on the general ophthalmic
list. 30. In the event of the Committee assembling to a meeting that is called and the
assembly does not form a quorum, it may discuss the business to be transacted but no decisions reached shall be considered decisions of the Committee until ratified by a subsequent meeting of the Committee at which a quorum is assembled.
URGENT BUSINESS TO BE CONDUCTED BETWEEN MEETINGS OF THE COMMITTEE 31. The Chair shall be given powers to make decisions on behalf of the Committee
in matters of urgency where there is no early meeting of the Committee at which such business could be considered. The Committee itself will determine from time to time how it will ratify and require reports under such "Chair's Action".
6

SUB-COMMITTEES 32.1 The Committee shall set up such sub-committees to deal with items of
business as it so determines. The decisions of such sub-committees shall not become the decisions of the Committee until such time as they are ratified by the Committee, except in such cases where the Committee gives prior leave for the sub-committee to act on behalf of the Committee.
32.2 In relation to paragraph 32.1 of these Standing Orders, the Committee gives
specific prior leave for the members elected by the Committee to the Standing Joint Committee with Islington Primary Care Trust to act on behalf of the Committee in all matters falling within the remit of the Primary Care Trust concerned.
AMENDMENT AND SUSPENSION OF STANDING ORDERS 33. No amendment of or addition to these Standing Orders shall be made unless
notice of the proposed amendment or addition has been included in the notice of the meeting of the Committee at which it is to be considered and a resolution in favour of the amendment or addition is carried by not less than two thirds of
the members of the Committee present at the meeting and voting. 34. Any Standing Order may be temporarily suspended at any meeting of the
Committee by resolution to that effect carried by not less then two thirds of the members present at the meeting and voting and with the consent of the Chair of the meeting.
35. Any member who has interest, pecuniary or otherwise, in any matter under
discussion by the Committee shall declare that interest. 36. Nothing in these Standing Orders shall prevent the Committee from agreeing to
work together with members of other Local Medical Committees in the area covered by NHS London or its successor body or bodies.
1 September 2012 31 August 2014
7

3
LMC Committee Members Roles and Responsibilities
Title: LMC Committee Member
Accountable to: Constituent GPs and practice teams, the LMC Chair,
Committee and the Medical Director/LMC Secretary and Chief Executive of Londonwide LMCs.
Attendance at Meetings Members are expected to attend regularly at full meetings of the LMC and, if appointed to any additional group as required by the LMC. Non-attendance at three successive meetings (any combination of full and liaison meetings) without good reason may result in the member being asked to stand down. Role of Committee Member
1. Members are elected by constituents and are expected to:
represent them make themselves available to them
listen to and seek their views ensure that those views are fairly represented
agree to use emails as their main form of communication.
2. Members must be aware that, by their election, they have a mandate to make decisions on behalf of their constituents.
3. LMC members are expected to read all relevant papers prior to a meeting and come prepared to discuss all agenda items. The office will ensure, wherever possible, that papers are sent out seven days before a meeting either by post or in electronic format.
4. Members are expected to respond promptly to all relevant communications, including
organisations within the specified timeframe.
5. mainly be in electronic format.
6. Members of the LMC are expected to follow established LMC policy and to fairly
7. If members express a personal view, rather than LMC policy, this should be made
clear in any discussion. Responsibilities of Committee Members
1. Members are expected to ensure punctual arrival at all meetings and to stay for the
duration of the meeting in order to receive full reimbursement.
2. Members are expected to ensure that all communication devices are set to silent
mode and any urgent calls are taken outside of the meeting.
8

4
3. Members are expected to keep themselves up to date with local policies, proposals and processes, including any identified LMC priorities, affecting their constituents and to be aware of national issues affecting the whole profession and the impact locally.
4. Members are expected to work and behave in an inclusive and collaborative manner
and to be respectful of their fellow committee members, the committee Chair, and the
LMC secretariat, both at meetings, and in all their communications in their capacity
as LMC members.
5. Members are expected to adhere to the minuted outcome (party line) of the meeting,
in their LMC capacity, once it has been agreed.
6. Members are expected to adhere to confidentiality where appropriate.
7. Members are expected to use email as their primary method of communication outside of committee meetings.
8. Members must the policy of Londonwide LMCs and must their interests.
9. Members must declare any pecuniary or other interest in any matter under discussion.
10. Members are not expected to raise issues relating to them personally, or to their practices, unless using the issue to introduce or illustrate a point. If they do, the LMC Chair reserves the right to correct the member/s and revert to generic principles.
11. LMC members, who are also PEC/CCG members, should make it clear in which capacity they are acting when involved in discussions or attending meetings. Once stated it is expected that a member will represent the views of that organisation during any meeting or ensuing discussion. Any member who feels unable to avoid a conflict of interest should withdraw from that discussion or meeting.
12. If contacted by the media for an LMC viewpoint, LMC members should first contact the press office at Londonwide LMCs to discuss the request and their proposed response.
13. Diversity and
Equality Policy.
14. Londonwide LMCs is incorporated as a Company Limited by Guarantee. This means the liability of individual LMC members is limited to £1 as long as each LMC member, member:
Completes fice.
Accompanies all written communications in their capacity as an LMC member with
the Company disclaimer.
9

5
Honoraria for Attendance
1. Honoraria for attending LMC meetings are notional flat-rate payments, inclusive of expenses.
2. The level of the honorarium will be determined by the Board of Directors of
Londonwide LMCs on an annual basis.
3. By signing the attendance register members are deemed to be making a claim for honoraria.
4. Members are expected to attend for an entire meeting unless prior notification has been received by the office.
5. Members arriving after the start of a meeting or leaving before the end of the meeting and who have not previously notified the office may be paid a reduced honorarium.
6. Members are responsible for ensuring that information relating to honoraria is
accurate and up to date. quarterly basis net of tax and national insurance directly into a bank account nominated by the LMC member. Members are required to provide the office with their national insurance number and bank account details.
Please note that these roles and responsibilities are subject to periodic review
Reviewed August 2012
10

ISLINGTON
LOCAL MEDICAL COMMITTEE
TERM OF OFFICE FROM 2012
Elected LMC members
Members until 31 August 2014 (5 places) (Term of office 2010-2014)
GP Contractual status Members until 31 August 2016 (5 places) (Term of office 2012-2016)
GP Contractual Status
Dr Sharon Bennett Dr Cornel Fleming Dr Simon Hazelwood Dr Antonia Lile Dr Clifton Woolf
GMS GP Principal Freelance GP/Locum GMS GP Principal GMS GP Principal GMS GP Principal
Dr Robbie Bunt Dr Linden Ruckert Dr Catherine Steven Dr Paddy Glackin Vacancy
GMS GP Principal GMS GP Principal GMS GP Salaried GMS GP Principal
Co-opted member until 31 August 2014 (A practitioner representing a particular class of experience not otherwise represented on the committee) The number of co-opted members should not exceed a quarter of total number of elected members. (Maximum of 3 co-opted members)
Name Reason for Co-option
Observers until 31 August 2014 (No voting rights on the committee, can include Practice Managers and Practice Nurses)
Name
Last updated: 4 September 2012 Version 1.1
11

1
LMC Committee Chair Role and Responsibilities
Title: Chair Accountability to: Constituent GPs and practice teams, in association with the Local
Medical Committee and the Medical Director/LMC Secretary and the Chief Executive of Londonwide Local Medical Committees Ltd
Role of the Chair
1. To attend and preside at all meetings of the Committee, in accordance with the Constitution and Standing Orders of the LMC. If the Chair cannot be present, the Vice Chair will preside. It would be expected that the Chair and Vice-Chair will liaise to ensure that one or other is present at all Committee meetings to provide consistency with proceedings.
2. The Chair will be an ex-officio member of all sub-committees, where these are
appointed by the LMC.
3. The Chair will work with Londonwide LMCs to set the agenda for all LMC, Liaison and other meetings as appropriate.
4. To fulfil the role of being a point of contact for local GPs and practice teams, and
liaise with the Londonwide LMCs on a regular basis on all matters to provide consistent support and information to constituents.
5. Chair support to be provided to Londonwide LMCs in dealing with local issues.
6. To demonstrate leadership through:
chairing and leading meetings of the LMC
securing the active involvement of elected members in pursuit of LMC policy with the PCT/or successor organisations, working closely with the Sector Team at LLMCs
Overseeing effective two-way communication with constituent GPs and practice teams to ensure appropriate inform LMC policy.
7. To agree the priorities for the committee; to act as a resource for the LMC where
there is a need to comment on specific local issues; and to provide professional representation at local, sector and Londonwide level.
8. To work closely with the Communications and Sector Teams on local media coverage, newsletters and other communications as appropriate.
Responsibilities of the Chair
1. The Chair will be responsible for the approval of the draft minutes and action notes of meetings of the committee where attended.
12

2
2. The Chair will ensure that the LMC team is fully informed of any discussions and decisions taken outside of the meeting schedule.
3. ly be in electronic format and Chairs are expected to use email as their primary method of communication outside of committee meetings.
4. The Chair is expected to attend identified and relevant training in order to maintain skills required in performing the role of Chair (e.g. Effective Chairing/Negotiating skills).
5. The Chair will behave in an inclusive manner both at LMC meetings and in all
communications in their capacity as LMC Chair.
6. The Chair will encourage the development and involvement of elected, potential LMC members.
7. The Chair will adhere to the LLMCs Equality and Diversity Policy.
Strategic Responsibilities of the Chair
1. The Chair will lead the representation of GPs and practice teams by forging and maintaining sound working relationships with the PCT or successor organisations and other local statutory organisations.
2. The Chair will work collectively with other LMCs within Londonwide Local Medical Committees Ltd .
3. The Chair may be asked to participate in a reference group from time to time to
4. The Chair and Vice Chair of each LMC hold the proxy votes for the election of
the Board of Directors for Londonwide LMCs Ltd and Londonwide Enterprise Ltd and at company Annual, Extraordinary or Adjourned General Meetings.
5. The Chair is expected to maintain a political and strategic awareness of matters affecting the LMC both locally, regionally and nationally.
6. The Chair is expected to attend the national UK LMC Conference or otherwise to
ensure that the LMC is properly represented. Honoraria for attendance
1. Chairs are entitled to receive honoraria payments over and above what is outlined in the LMC Members roles and responsibilities. The Londonwide LMCs Honoraria Policy will follow with further details.
Reviewed August 2012
13

14

Islington Local Medical Committee
Nomination Form Chair of the Committee
TO BE COMPLETED BY THE CANDIDATE I wish to stand as Chair. (BLOCK CAPITALS PLEASE) I am an elected member. Statement of Intent Please provide in no more than 100 words a brief statement outlining your aims for the direction and working of the LMC in the forthcoming year.
I have read and understood the LMC Chairs Roles and Responsibilities and if elected I am willing to serve until 31 August 2014. Signed: PLEASE PRINT NAME: TO BE COMPLETED BY THE SECONDER
I have read and understood the LMC Chairs Roles and Responsibilities. I support the above nomination. I am an elected member of the LMC.
Signed: PLEASE PRINT NAME: Please return this nomination form to the LMC Secretary not later than the start of the meeting at which the appointment is to be made.
15

16

Islington Local Medical Committee
Nomination Form for LMC Vice Chair
TO BE COMPLETED BY THE CANDIDATE I wish to stand as Vice Chair.
(BLOCK CAPITALS PLEASE) I am an elected member. I have read and understood the LMC Chairs Roles and Responsibilities and if elected I am willing to serve until 31 August 2014. Signed: PLEASE PRINT NAME:
TO BE COMPLETED BY THE SECONDER I have read and understood the LMC Chairs Roles and Responsibilities. I support the above nomination. I am an elected member of the LMC. Signed:
PLEASE PRINT NAME: Please return this nomination form to the LMC Secretary not later than the start of the meeting at which the appointment is to be made.
17

18

Minutes of the Islington LMC meeting on 22 August 2012 from 1.30 pm to 3.00 pm in the
Board Room, NHS Islington, 338-346 Goswell Road, London EC1V 7LQ
PART ONE CONFIDENTIAL
Present:
LMC members Dr Robbie Bunt (Chair) Ms Bernadette Edwards Dr Cornel Fleming Dr Catherine Steven Observer Dr Julie Sharman Secretariat
Mr Greg Cairns Ms Leah Benson Dr Paddy Glackin Miss Nicola Rice
Item no.
Action
Organisation / person
responsible
1.0 Welcome and apologies Dr Bunt welcomed Dr Julie Sharman who would be replacing Dr Paddy Glackin from 3 September 2012 as the LMC Secretary/Medical Director for Camden, Islington, Tower Hamlets, City and Hackney and Newham LMCs to the meeting. Dr Sharman advised that she had been a partner in a PMS practice with 6000 patients in Hoxton for the past 10 years but decided to give this up in March 2012 in order to broaden her experience and to consider other areas of work to be involved in. Apologies for absence were received from Dr Sharon Bennett, Ms Jenny Finch, Dr Simon Hazelwood, Dr Eva Larsson, Dr Antonia Lile, Dr Linden Ruckert, Dr Guido Stefanec and Dr Clifton Woolf.
2.0 Declarations of interest There were no new declarations of conflicts of interests.
3.0 Minutes and matters arising not listed elsewhere on the agenda:
3.1 Minutes of LMC Part one meeting on 25 April 2012 and matters arising: The minutes were agreed as a correct record subject to the following
19

amendment: Item 6.3 – Prescribing Quality Incentive Scheme: The first sentence was amended as follows: ‘Dr Glackin queried whether this was an incentive scheme or a LES as if the former the payments might not be superannuable.’
3.1.1 List maintenance (minute 5.4 refers) Dr Glackin advised that the census figures which had recently been published showed that the conception that there was huge list inflation in Islington was wrong given that the population in Islington had proved to have been very high. In the circumstances he suggested that he raise this issue in the part 2 meeting with a request that the list inflation exercise be stopped.
PG
3.1.2 Locum GP Pension contributions Ms Edwards undertook to remind practice managers at the next Forum that practices should complete and submit Form A within 10 weeks of a locum having undertaken the work in order that his/her pension contribution counted towards the NHS pension.
BE
4.0
4.1
4.2
Membership issues Elected members It was noted that there were three vacancies on the Committee for a four year term commencing 1 September 2012. Ms Rice advised that she had put an item in the July 2012 newsletter inviting expressions of interest but none had been received to date. Dr Catherine Steven confirmed that she would like to continue as an LMC member and explained that she had not stood for election as she had not received the papers having moved while on maternity leave. Dr Glackin confirmed that he would be willing to take up one of the places if not enough people came forward. It was agreed that a further email would be sent out to GPs inviting expressions of interest by 31 August 2012. If no expressions of interest were received Dr Steven and Dr Glackin would be declared elected on to the Committee Practice Manager and Practice Nurse observers It was agreed that expressions of interest would also be sought from Practice Managers and Practice Nurses to be received by the end of September 2012. Any expressions of interest put forward would be circulated to the elected members after that date for a decision so that a Practice Manager and Practice Nurse could be invited to attend the first LMC meeting in the new term.
NR
NR
20

5.0 Chairs and LMC members’ reports of meetings attended as
LMC representatives
5.1 Interim meeting on 19 July 2012 Members noted the minutes of the interim meeting which had been reproduced on the Part 2 agenda.
5.2 Primary Care Development Group meeting on 2 August 2012 Dr Bunt reported that he and Mr Cairns had attended this meeting and one of the main issues which had been discussed had been a Memorandum of working between practices in a locality. He advised that it had been agreed that Mr Cairns and Ms Shah would work jointly on developing principles on general practice working collaboratively in the sub localities within Islington CCG and referred members to the tabled draft. Dr Bunt advised that he had concerns about the following bullet point in the draft: ‘Where local services are commissioned from general practice, consider delivering this at individual practice level and or where appropriate at a locality level with services delivered through host practices.’ He advised that he would prefer wording which would convey the sense that those services which were best delivered at practice level should be delivered at practice level wherever possible and only those most suitable for provision at locality level should be done across the locality. Mr Cairns noted that this was still a working document and confirmed that he would take this back. Ms Edwards asked how the second key principle ‘Ensuring every patient registered with an Islington GP practice has access to all appropriate commissioned services’ was meant to happen. Dr Bunt clarified that this included to ensure that the Islington population had access to all services available and Dr Glackin confirmed that this was already possible in theory in that practices which did not provide certain services which were provided by other practices could refer their patients to those practices but noted that this did not happen. Dr Bunt confirmed that while some form of understanding between practices might be appropriate for this to happen there should not be a legally binding contract. Dr Bunt considered that the borough was moving forward in the right direction with this and considered that the situation might improve with Dr Russell having left the Cluster as there may be less pressure to impose the concept of things such as the super LES.
GC
5.3 Access/OOH Group meeting on 2 August 2012 Dr Bunt expressed the view that the whole issue of out of hours and 111 was a mess. He was concerned as he had heard of proposals that a patient having been triaged by 111 needed to be seen/have contact with a GP within 6 hours. He suggested that if new money
21

would be made available for this one way forward would be to fund practices to make available a certain number of appointments to cover such instances. Dr Glackin advised that he wished to ask the NHS London:
• who were the beneficial owners of pathways and • who were the beneficial owners of Co-ordinate my Care
as he was concerned that there may be conflicts of interest. Dr Bunt further understood that the contract with Harmoni might now be rolled out until the end of next March and noted that a lot of practices used Harmoni for in hours cover when they closed for half a day for training purposes. Dr Glackin advised the Committee that practices did not have to use Harmoni for such in hours cover and noted that other providers such as LCW, Barndoc or screening and telephone answering services could be used. Dr Bunt reminded the Committee that initially the borough had said that practices should not be closing for half days but he had queried this in view of the fact that the CCG Board expected people to attend many meetings during the day. He advised that the CCG Board had appeared to have acknowledged this. Dr Glackin put forward the view that what practices did during opening hours was not the CCG Board’s business and so practices could use other providers if they wished. Dr Bunt ask Ms Edwards if she would undertake a scoping exercise and contact other providers to see if they would provide cover for Islington practices.
PG
BE
5.4 Meeting of EMIS/IT working group on 3 August 2012 Mr Cairns confirmed that he had attended this meeting but Mr Thomas had still not provided the information which the NCL LMC Chairs had been requesting about the roll out of EMIS web. He considered that there had been a push to get a system in place with regard to data sharing and considered that they were looking at a solution without understanding what the issues were. It seemed as though the borough/cluster was of that view that integrated care meant that all data could be shared. Dr Glackin reminded the committee that the LMC was still awaiting answers to questions including who would be responsible for EMIS web in the future, who would pay for it and what training time would there be for practices. Ms Edwards noted that her experience of an EMIS trainer had not been good and Dr Glackin noted that this was one of the reasons why the LMC was reluctant to sign up to this.
5.5 Meeting with Dr Sarah Humphery on 9 August 2012 regarding child protection issues Dr Bunt confirmed that he and Dr Bunt had met with Dr Humphery the Islington Named GP for Child Protection and Safeguarding Children to discuss various forms which she wished GPs to
22

complete. Dr Glackin noted that they had to go over the same issues such as telephone requests from social workers for reports without the patients’ consent, the lack of clarity about whether requests were being made under section 47 of the Children Act, attaching claim forms to requests for reports etc. Dr Humphery undertook to produce a communication to go out but neither he nor Dr Glackin had seen this yet. Dr Glackin reported that Dr Humphery had also asked for GPs’ help in relation to audits for OFSTED.
5.6 Whittington Drugs and Therapeutics Committee Dr Fleming reported the following from a recent Drugs and Therapeutics Committee meeting he had attended:
• Electronic cigarettes could be just as dangerous as real ones • There was a move to convince people to use Optasa
although Asacol was used elsewhere • There was a new policy around the prescribing of Dabigatran
• Thicken up Clear was more effective Dr Bunt understood that a member of the Islington Medicines Management team attended the Whittington Drugs and Therapeutics Committee so any recommendations that came out should be circulated in the Islington weekly GP Bulletin.
6.0 Items for discussion
6.1 Draft and unconfirmed minutes of the NCL Cluster and LMC Chairs Group meeting on 24 April and 26 June 2012 The minutes were received.
6.2 Islington CCG It was noted that comments on the draft constitution had to be submitted by the end of the week. Dr Glackin noted that the GPC had issued guidance that day indicating that as constitutions might need to be changed between now and next March to incorporate further DH guidelines they did not need to be actually signed but that it would be appropriate to provide confirmation that practices agree with the principles. Dr Fleming advised that he had recently attended a meeting where concern had been expressed that many CCGs were looking to performance manage practices. Dr Glackin confirmed that this was an issue but that Islington had not taken that stance and had taken on the LMC’s comments. Dr Bunt reported that two lay members had been appointed to the Board: Ms Anne Weyman and Mr Sorrell Brookes.
23

6.3 Islington Primary Care Strategy
There was no further discussion under this item in addition to the discussion which took place under item 5.2.
6.4 Sessional GP issues Dr Fleming advised that sessional GPs were still not receiving newsletters from hospitals. Dr Glackin noted that practices did not receive such newsletters either. It was agreed, however, that it would be useful to ask at the next NCL Cluster LMC Chairs meeting if the details of a named contact could be provided to whom sessional GPs could provide their email addresses to ensure that they received appropriate communications from the Cluster/boroughs.
6.5
PMS issues Mr Cairns advised that there was an NCL PMS Review Group which met on a monthly basis to discuss the PMS review. He noted that Dr Milan Koya was on the group as the Islington representative. A meeting for Camden and Islington practices jointly hosted by the LMCs and Cluster would be held in September 2012.
6.6 Issues to be raised at Health and Wellbeing Board meeting: Dr Bunt advised that the Health and Wellbeing Board was potentially a useful forum to facilitate good working relationships between the local authority and GPs. He reported that he had requested that an item be included on the agenda of the next Health and Wellbeing Board to raise the sort of issues which create problems for GPs and practices such as requests for housing reports and sick notes for schools. In addition Dr Bunt considered that more could be done jointly in relation to care packages where problems arise. It was agreed that an item would be placed in the next newsletter asking if people had any ideas about how services can be streamlined and improved.
NR
6.7 Invitation to acute Trusts to attend LMC meetings It was noted that this had been discussed at the last interim meeting and that Mr Cairns had undertaken to prepare a paper for discussion.
6.8 Format and schedule of meetings in 2013 It was noted that this would be discussed at the meeting of the new committee in October.
7.0 Part Two agenda:
24

7.1 Appraisals and the clarity toolkit (minute 3.1.3 refers) Dr Glackin considered that even though the NCL Cluster was paying for the Clarity toolkit it should be open to GPs to use whatever toolkit they wished in relation to appraisals. It was agreed that he should raise this in the Part 2 meeting.
7.2 Process agreeing new LES (item 4.2) Dr Bunt noted that many LESs would sit with public health in the future and suggested that it might be helpful to have public health colleagues attending meetings such as the Primary Care Development meetings. Dr Glackin suggested that this should be taken to the Health and Wellbeing Board. It was also noted that there was concern nationally about whether or not LESs funded by public health would be superannuable. Ms Rice advised that this had been raised with the GPC who had confirmed that the negotiators were due to meet with Ms Barbara Hakin to discuss this issue. Dr Bunt noted that at the last Primary Care and Development Group meeting Ms Shah had produced a list of enhanced services with money attached. It was agreed that Ms Shah should be asked to forward this list to the office as it would be useful to scope LMC engagement. Dr Bunt considered that it should be the LMC’s priority to push for more LESs to be commissioned as soon as possible particularly in view of the risk that the money available will not be spent by April 2012.
8.0 Received items:
8.1 BMA guidance on CQC registration, May 2013 The committee agreed that this was a helpful and useful document particularly in relation to the templates provided in the appendices which had been provided for practices to use. Ms Edwards advised that she had attended a CQC workshop at which it had explained that it was more likely that CQC visitors would wish to speak to members of staff rather than be handed lots of protocols so it would be important to ensure that staff were trained for this.
8.2 North Central North East London Local Education and Training Board (LETB) The LMC noted the Londonwide LMCs’ briefing on LETBs and noted that there was a potential risk that the current good general practice education and training would be subsumed and lost when larger and academic organisations took over the responsibility of training from the Deanery. Ms Benson advised that Londonwide LMCs was engaging closely
25

with the three LETBs being set up in London and advised that each of them had agreed in principle to have a GP representative on their Boards although the office was still waiting to be formally approached by the NCNE LETB requesting a representative. Ms Benson further explained that UCL Partners had expressed an interest in being an Academic Health Science Network and had been accepted. Ms Benson would be emailing details of a network event which was due to take place in the near future which people could attend if they wished. In addition Ms Benson advised that Londonwide LMCs was working with the Deanery to develop a GP council type of forum which was very much work in progress. Dr Bunt understood that funding for education and training was likely to be cut and Dr Glackin confirmed that this would be from the central Education, Training and Workforce pot. Dr Glackin also confirmed that the GPC was concerned about a proposal that practices might be expected to pay for ST4s and this was being dealt with on a national level.
8.3 LEAD A list of the forthcoming events was noted.
9.0 LMC newsletter No additional items were identified for inclusion in the newsletter.
10.0 Date of next meeting: 24 October 2012
11.0
Any other business There was no other business.
26

Minutes of the Islington LMC meeting on 22 August 2012 from 3.00 pm to 4.30 pm
The Board Room, NHS Islington, 338-346 Goswell Road, London EC1V 7LQ
PART TWO Present:
LMC members Dr Robbie Bunt (in the Chair) Ms Bernadette Edwards Dr Cornel Fleming Dr Catherine Steven Borough representatives Ms Alison Blair Dr Gillian Greenhough Mr Paul Sinden Observer Dr Julie Sharman Secretariat
Mr Greg Cairns Ms Leah Benson Dr Paddy Glackin Miss Nicola Rice
Item no.
Action
Organisation / person
responsible
1.0 Welcome and apologies Ms Alison Blair was welcomed to the meeting in her capacity as the recently appointed Chief Officer of Islington CCG. Dr Julie Sharman, who would be taking over from Dr Paddy Glackin as LMC Secretary/Medical Director for Islington LMC was also welcomed to the meeting. Apologies for absence were received from Dr Sharon Bennett, Ms Jenny Finch, Dr Simon Hazelwood, Dr Eva Larsson, Dr Antonia Lile, Dr Linden Ruckert, Ms Avni Shah, Dr Guido Stefanec and Dr Clifton Woolf.
2.0 Declaration of conflicts of interest There were no new declarations of interest.
3.0 Minutes and matters arising not listed elsewhere on the agenda:
3.1 Minutes of LMC Part 2 meeting on 25 April 2012
27

The minutes of the meeting on 25 April 2012 were agreed as a correct record.
3.1.1 Appraisal toolkit (minute 3.1.3 refers) Dr Glackin noted that although the Cluster had paid for the Clarity toolkit to be used for appraisals there may be some doctors, particularly those newly qualified who were used to the RCGP toolkit, who preferred to use the RCGP toolkit. Dr Greenhough advised that as the Cluster had supported Clarity it had given no commitment to train every appraiser to use all toolkits available. However, if GPs did not wish to use Clarity they could print off all the relevant information. Ms Blair suggested that this issue be taken up with Dr Henrietta Hughes as it was the Cluster’s responsibility which would be passed to the NHSCB.
3.1.2 Prescribing Quality Scheme 12/13 (minute 5.9 refers) It was noted that Dr Glackin had met with Mr Dutt to discuss Dr Glackin’s concerns and the prescribing quality scheme for 12/13 had now been agreed.
3.1.3 LMC representation on Islington Safeguarding Children’s Board (minute 7.1 refers) It was noted that the Islington Safeguarding Children’s Board did not consider that it would be necessary to have LMC consult the LMC concerning any decisions it made that may impact on GPs.
3.1.4 Physiotherapy services provided by Whittington Health (minute 7.2 refers) Dr Greenhough reported that Whittington Health had been given an action plan in relation to physio referral delays as a result of which there should now be no more than a six week wait for a routine phsyio referral. However, Dr Greenhough had heard anecdotally that one patient who had received a telephone call from Whittington Health four weeks after a referral to say that an appointment would be give in 6-8 weeks’ time which would in effect mean an 12 week wait. Dr Greenhough advised that if people were experiencing similar problems she would be grateful to hear about this with appropriate evidence so that it could be taken up. Mr Sinden advised that something had been included in the previous week’s weekly GP bulletin asking for evidence of any concerns and that this would be repeated the following week. It was agreed that it would not be helpful at this stage for the LMC to include a similar item in its newsletter. Dr Greenhough advised that it had been made clear to the Whittington that any patients waiting over six weeks should be exceptional.
28

Dr Bunt asked whether self referrals were being monitored. Mr Sinden did not know and undertook to take this away and clarify this with the Whittington. Dr Greenhough advised that podiatry appointments should also be down to six weeks but this would not be monitored so closely. Dr Bunt expressed the view that it would be helpful for the average GP to know what the expectations were for services such as MSK triage, podiatry, physio, and REACH team referrals for housebound patients. Dr Greenhough advised that the next area which the CCG would be tackling would be REACH and that Whittington Health was setting up two clinical groups to look at podiatry and physio/MSK services to consider how to control demand. Dr Greenhough advised that Dr Andrew O’Brien, a Darzi Fellow, attached to Laycock Street would be going to these meetings but Dr Greenhough advised that it would also be open to the LMC to send representatives to these groups if it wished. Dr Steven indicated that she would be interested in attending the physio clinical group.
PS
PS
3.1.5 Royal Free Shared Care arrangements for patients with CKD (minute 5.11 refers) Dr Greenhough noted that it appeared that the shared care arrangements for patients with severe CKD was something that had been developed with some GPs some years ago although the practice which had raised this issue had not been involved in these discussions. Dr Greenhough advised that Islington proposed to look at potential ways of dealing with CKD in the community and noted that Dr Karen Sennett was working on this.
3.1.6 Invitation to providers/acute trusts to LMC Part 2 meetings (minute 7.3 refers) Dr Greenhough understood that it had been agreed that providers/acute trusts would only be invited to LMC/borough meetings as issues arose rather than have a regular invitations. The LMC agreed to this suggestion and it was agreed that this item would be taken off future agendas.
3.1.7 POLCE (minute 7.6 refers) Ms Blair explained that due to the transition there had been a delay in responding to Dr Ruckert’s letter of concern about the IFR process. Mr Sinden confirmed that this had now been taken up and that a holding response would be sent to Dr Ruckert. Mr Sinden advised that although people should contact the IFR team at the Cluster about individual cases the borough would be providing a back up email address for a practice with any concerns about the process to use so that the CCG could take it up if necessary. Dr Glackin noted that the problem was that the IFR
29

team never responded to any queries raised and he noted that in one case he had drawn his concerns to the attention of Dr Russell who had not responded either. In fact as no response had been received after 9 months the patient’s MP became involved. Dr Greenhough advised that the Islington team acknowledged that POLCE might not have worked well due to its initial design and reported that Dr O’Brian would be getting involved in some work around POLCE. Dr Greenhough advised that Islington wanted to look at the clinical viability of some of the procedures and Dr Glackin indicated that the LMC would be interested in being involved in this. He advised that GPs needed pathways that worked to which patients could be referred. Furthermore it should be the consultants explaining why patients would benefit from certain treatments where applicable and not GPs. Dr Greenhough considered that both GPs and consultants had a responsibility with regard to POLCE and noted for example that it would not be appropriate for a GP to refer somebody with carpal tunnel syndrome to secondary care when appropriate services were available in the community setting. However, Dr Greenhough did acknowledge that good straightforward clinical pathways were needed. Dr Greenhough noted that some areas such as Camden operated a triage referral management system and this would be one of the areas which Dr O’Brian would be looking at. Dr Greenhough further noted that North Central had experienced problems with UCH and the POLCE policy this year due but hoped that things would improve once the Commissioning Support Unit came into existence in October 2012. The CSU would cover a large number of hospitals in North Central and North East there so there should be opportunities to discuss issues such as POLCE in the round and ensure that different things did not happen in different hospitals. Dr Glackin reminded Dr Greenhough that something needed to be done now in relation to clarifying what the guaranteed turnaround time should be those patients where an IFR had been made. Dr Greenhough undertook to look into this and feature this into the discussions which were taking place with the CSU around SLAs.
3.1.8 Whittington Health and Dossett boxes (minute 7.7 refers) Dr Greenhough confirmed that Whittington Health did not provide Dossett boxes and the Islington prescribing department had looked to see if there were any routes open to it to insist that they should provide this service, including DDA compliance. As there was no legislation requiring hospitals to provide dossett boxes the prescribing team had looked to see what happened elsewhere and many hospitals including The Royal Free and UCH, wrote a script and arranged for a local pharmacy to provide the dossett boxes. Dr Greenhough advised that Islington would ask Whittington to adopt this system and Mr Sinden undertook to liaise with Mr Amalin Dutt to
30

confirm that GPs would not need to be involved in this arrangement. Ms Blair confirmed that discussions with Whittington Health needed to take place around this proposal and suggested that it be kept on the agenda
PS
NR
3.2 Notes of interim meeting on 18 July 2012 The notes were received.
4.0 Islington Local issues
4.1 Report from Chief Officer Ms Blair referred to the recent letter from Mr David Nicholson describing the need for the Cluster and CCG shadow boards to start working in a new structure from 1 October 2012. Ms Blair advised that work was ongoing across the Cluster to think about what the impact of this would be but Ms Blair considered that Islington was in a good position although a check would be done throughout September to ensure that it was ready to take on the new responsibilities. Ms Blair noted that the Commissioning Support Unit (CSU) would be set up from October 2012 and that the Islington CCG Board would start to meet in public. Ms Blair advised that the mock authorisation panel had taken place in August with the formal panel taking place on 18 September 2012. Appointments to the Board were ongoing with Ms Anne Weyman and Mr Sorrell Brookes having been appointed as lay members to the Board. Ms Blaire also reported that Mr Ahmet Koray had been appointed as Chief Financial Officer and would commence in two weeks. Ms Blair further advised that the Board was actively recruiting for a secondary care doctor member. Alongside this an HR process was taking place with the local team to match jobs with the new CCG structure. Financial position Ms Blair reported that as at month four the financial performance was on track. There was a slight underspend but Islington was aware of the reasons for this and it was likely to change. In addition the QIPP programme was on target and an £11m investment plan had been signed off by the CCG Board in June. In addition to the above work usual business was being conducted such as discussions around the annual planning process for next year’s contract round and the development of commissioning intentions for the borough. Commissioning Support Unit Ms Blair confirmed that the CCG was currently in discussion with the CSU and noted that as the CCG would be reliant on the CSU providing a good service it would be critical that the CCG and CSU worked in partnership to ensure a good and flexible service was provided. Ms Blair advised that the CCG would have a
31

commissioning support director at the CSU who would work locally and would be the main point of contact. Mr Blair confirmed the following appointments to the CSU:
• Mr Andrew Ridley – Managing Director
• Ms Helen Pettersen – Interim Chief Operating Officer • Mr Harry Turner –Chief Financial Officer
• Mr Will Huxter – Director of Contracting Dr Greenhough noted that failing trusts and the failure team would sit with the National Trust Development Authority which would be headed up by Ms Alwen Williams. In response to Mr Cairn’s query as to how confident the CCG felt that it would get what it wanted from the CSU rather than what the CSU could provide, Dr Greenhough advised that she felt confident as the CCG had made it clear that there would be joint working. Ms Blair agreed that there was an acknowledgement that it would take some time for the CSU to bed in Dr Greenhough was pleased to report that UCH had signed the Heads of Agreement and contract the previous week.
4.2
4.2.1
4.2.2
Clinical Commissioning Group Constitution Ms Blair noted that the deadline for comments on the CCG constitution was 24 August 2012. Dr Glackin advised that the GPC had issued guidance suggesting that practices did not need to sign on the dotted line before next April but indicate in principle that they would sign up to it as it was anticipated that more guidance would come from the centre which would need to be incorporated into constitutions. Dr Greenhough advised that the borough was keen to have actual sign up by practices and was disappointed that Camden had already achieved this. Dr Bunt referred members to the draft memorandum of understanding between practices in a locality which was still work in progress. It was agreed that Mr Cairns would liaise with Mr Sinden and Ms Shah regarding the document. Process for agreeing new LESs Mr Sinden advised that a paper would be brought to the September 2012 Primary Care Development Group meeting setting out a process in the light of the new guidance which had recently been published. Mr Cairns advised that he was due to meet with Cluster representatives the next day to discuss that guidance. Dr Glackin noted that the LMC considered LESs to be important and ideally would like to see public health LESs integrated into the new structure. He advised that the LMC would also welcome joined up commissioning work and so discussions should take place with the Health and Wellbeing Board. Dr Bunt suggested that the Primary Care Development Group could include representatives from public
GC/PS/AS
32

4.2.3
health. Ms Blair agreed that there would be a need to talk to the local authority regarding local enhanced services. Dr Bunt noted that he had seen a list of new LESs which would be coming into the system with the funding attached and asked that the be sent a copy as the LMC would need to be involved in their development. Mr Sinden undertook to forward a copy to the office. List validation Dr Glackin noted that with the recent publication of the 2011 Census figures it had become apparent that there was not huge list inflation in Islington but that there was in fact under registration. Dr Greenhough advised that the borough had not interpreted the figures in the same way but advised that there would be an emphasis on encouraging people to register. Dr Greenhough reminded the committee that the list validation process was a national requirement and would be done every 2 years. It was agreed that this issue would be discussed further at the next interim meeting.
PS
GG/GC/RB/AS
4.3 Islington Primary Care Strategy Mr Sinden advised that expressions of interest had been invited for four locality clinical leads. In addition 4 locality officer positions to support the clinical leads would be appointed. Mr Sinden further advised that four care-co-ordinators would be recruited and it was likely that expressions of interest would be put out to the voluntary sector. Mr Sinden advised that the borough was beginning to talk to the provider regarding realigning services with the four localities. A meeting with the CMHT was due to take place on 10 September 2012 and he noted that following its reorganisation there would be a single point of access. He advised that the pathways for COPD and diabetes had been signed off by the Integrated Care Board in July and confirmed that the diabetes LES would be brought to the October meeting. Mr Sinden reported that the borough had also been working with UCLH regarding the Medicines Board which was a division of the Medical Consultant Board. Dr Greenhough noted that it had become clear to UCH that it needed to be involved in integrated care and that meetings with them had been positive. Dr Greenhough gave an example of a project being run by UCH which involved people with uncontrollable high blood pressure having a 24 hour blood pressure monitor at home which was assessed by a consultant who would make recommendations remotely.
4.4 Local enhanced services Commissioning LES Dr Bunt asked when practices would receive payments in relation to
33

the work done for the 11/12 PBC LES. Mr Sinden undertook to find out. Dr Bunt reminded the Committee that in the past practices would receive half the money for the PBC LES up front but noted that a LES for 12/13 had still to be produced and it was already August. Mr Sinden hoped that the LES would be signed off in September.
PS
4.5 Out of hours procurement Ms Blair understood that the procurement process had now been completed and the name of the preferred provider should be announced at the end of the following week. Ms Blair considered that the organisation chosen should be large enough to be able to provide in hours cover for practices.
4.6 Borough Urgent Care Strategy including 111 update Dr Bunt noted that as part of 111 there was a proposal that a patient would need to been seen or have contact with a GP within 6 hours of being triaged by 111 and queried how this would be done. He suggested that one way would be to commission a LES for access. It was agreed that there were a number of areas which were unclear and Dr Greenhough noted that a pan Islington meeting had been arranged to take place in September in relation to 111. Dr Glackin reported that it had been agreed by the LMC in the part one meeting that it would ask who were the beneficial owners of the 111 pathway and Coordinate my Care as the Committee wanted an assurance around potential conflicts of interest. In addition he wanted to be sure that CCGs would not be held responsible for a badly designed process. Dr Greenhough agreed that it would be important to ask probing questions and noted that CCG Chairs had made it clear that they wanted a safe system.
4.7 IT issues Dr Bunt expressed concern that despite repeated requests for a briefing paper on EMIS web addressing a number of concerns raised by the LMC Chairs Mr Thomas had not yet produced one or responded to those concerns. He noted that one issue related to confidentiality and the need for patients to be involved in the development and roll out of EMIS web given the unhappiness of some patients in relation to the Summary Care Record. Dr Greenhough advised that EMIS web was likely to be the infrastructure for the future and noted that one of the reasons why Mr Thomas had not provided a briefing paper was because he was taking learning from areas where it had been rolled out. In response to her query for clarification about the clinical governance issues associated with EMIS web Mr Cairns advised that the LMC Chairs
34

had queried where the information would be stored and how it would be used. Dr Glackin also noted that there were anxieties about the speed at which this was being taken forward without any of the concerns being addressed. Dr Greenhough suggested that it might have felt that it was being taken forward quickly due to the fact that the money which had been made available for this had to be spent in year. Dr Greenhough was pleased to report that Docman was ready to be rolled out in Islington but explained that this had been delayed in Islington due to a lack of money. Dr Bunt expressed concern that IT was being handled in an unco-ordinated way. It was agreed that the IT Borough working group which had been established recently would be the best place to discuss the various ongoing IT related workstreams. Ms Edwards advised that the training she had received from an EMIS web trainer had not been particularly helpful and asked whether it would be possible for members of Mr Thomas’ team to provide the training. Dr Greenhough advised that there were not enough people in Mr Thomas’ team to be able to provide this service but noted that if there was variable quality of training provided this would need to be taken back. It was agreed that Mr Cairns would write to Mr Thomas setting out the concerns about the IT strategy which had not been addressed to date.
GC
4.8 Appraisals and the Clarity Toolkit It was noted that an Islington GP had expressed concern about having received a letter setting a date for an appraisal before she had been migrated to Clarity and this had created a lot of problems and time wasted trying to use the toolkit. Dr Bunt noted that he too had experienced problems using the toolkit. Dr Bunt also advised that he had been asked to volunteer to take part in revalidation but he had not heard anything further and was not clear about the process. Dr Greenhough advised that she understood that CCG and LMC Chairs had been asked to volunteer but if not enough came forward others would be asked. It was agreed that this issue would be raised at the next Cluster meeting.
5.0 NCL issues:
5.1 Minutes of the NCL Cluster and LMC Chairs meetings on:
• 24 April 2012 • 26 June 2012 (draft and unconfirmed)
5.2 Patient Choice Pilot LES Dr Bunt advised that the Cluster had forwarded a first draft of the Patient Choice Pilot LES but noted that the costs associated with it
35

were a third of the prices charged by Harmoni and so he considered it unlikely that many practices would take it up. He advised that it was due to be discussed at the meeting with the Cluster the next week.
6.0 Future meeting arrangements This item was not discussed.
7.0 Date of next meeting: 24 October 2012
8.0 Any other business There was no other business.
36

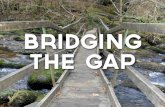
Process for approval of Local Enhanced Services
(to be delivered by primary care contractors (GPs and community pharmacists) that go
beyond the scope of GMS and community pharmaceutical contracts)
Principles:
1. Good governance – clarity about where decisions are made, with a clear audit trail.
2. Decisions are made in a timely manner – the process facilitates decision making and does not hold up the implementation of schemes.
3. The most appropriate people are correctly involved.
4. There is clarity about how projects and schemes are monitored.
5. There are effective checks and balances to GP commissioner/provider conflict of interest
P:\
A) Modification of an
existing LES*
B) Changing an existing
NES* to a LES*
C) Formation of a new LES
BUSINESS CASE REQUIRED
Checklist to complete before proceeding to business case stage:
• Does the proposal duplicate existing incentives? (i.e. QOF, other ESs)
• Does the proposal address a health need which is an Islington priority (CCG /
Local Authority)?
• Does the proposal have evidence-based clinical benefits for patients?
• Does the proposal address one or more objectives or strategies of Islington
CCG/Local Authority?
• Does the proposal meet the requirements of the “Once for London” guidance?
YES
NO YES
NO Business case
unlikely to be
approved - seek
advice from the
Primary Care
Contracts team
at NHS NCL
Proceed to next
stage
DRAW UP BUSINESS CASE & DRAFT LES SPECIFICATION
Step-by-step checklist – For any LES led by either CCG or Local Authority
1. Email NHS NCL Contracts & Performance team to see if there are similar specifications in existence.
2. Set up working group to develop LES if appropriate. Ensure stakeholders, incl. clinical leads, local professional committees* and NHS NCL Contracts and Performance team
is invited to participate in development.
3. A) Populate and agree the business case (using Template 2)
B) Draw up LES specification using ‘Once for London’ LES (Template 3). Where applicable, aim for population coverage (i.e. mechanisms in place for patients to attend
‘host’ practices if theirs is not commissioned for a LES). Ensure that it is accompanied by application information and supporting documents, a claim form and an audit
template (if appropriate).
4. Where delivered by GPs, complete the Conflict of Interest Governance Template (Template 4) to ensure transparency of decision-making in making commissioning
recommendations about LES.
5. Get sign off by working group, including local negotiation of level of remuneration.
YES
YES
YES
NO
NO
NO
• Send documents to formal LMC meeting for approval (meets bi-monthly, however where appropriate can be agreed by email)
• Send documents to CCG Governing Body (meets monthly)
Working group lead to send a copy of the
specification to the Contracts & Performance
team at NHS NCL
A) EXISTING LES BEING MODIFIED C) NEW LES B) CHANGING AN EXISTING NES TO A LES
LES APPROVED LES NOT APPROVED
Tony Hoolaghan/Helen Pettersen (subject to change in
staffing) – turn around approval within 48 hours - email to
Shadow NCB meeting (Meets fortnightly)
Finance Recovery & QIPP Group (Meets monthly)
BRING INITIAL OUTLINE OF LES TO ISLINGTON CCG PRIMARY CARE DEVELOPMENT MEETING VIA COMPLETION OF CCG INVESTMENT PROFORMA TEMPLATE
(Template 1)
IDEA APPROVED
KEY*
• Local Professional Committees –
Local Medical Committee, Local
Pharmaceutical Committee,
• ‘NES’ – National Enhanced Service
(locally commissioned, with a
national specification)
• ‘LES’ – Local Enhanced Service
(specification developed and
commissioned locally)
Send business case, specification and conflict of interest template to Islington CCG Primary Care Development Group (meets monthly)
Send documents to CCG Executive Team (meets weekly)
Approval by Islington Health and Wellbeing Board
CCG process Local authority
process
ROLL OUT OF LES
37

Local Enhanced Service Specification for Clinical Commissioning LES Specification for GPs
Commencement date 1st April 2012 – 31st March 2013 A local enhanced service between NHS NCL and Borough GP Practices.
1. Introduction and Background
The Clinical Commissioning LES has been running in Islington for a number of years, but prior to 2011/12 was named the Practice Based Commissioning LES. This LES has always sought, and continues to seek, to incentivise clinicians to review and improve their performance in secondary care, and be involved in designing and shaping new pathways and secondary care services.
In the past the LES has required practices to audit patient-level data for specific clinical areas for which data showed greater acute activity, and produce a report reflecting on the results of that audit. This has served well to highlight variation between clinicians within the practice and to uncover errors in coding by secondary care which could be used by contract managers to challenge our acute providers.
However as time has moved on, a number of these areas have already been reviewed in the past, and other requirements, such as Quality and Productivity Markers under QOF now cover the requirement for reviewing outpatient referrals, emergency ACS admissions and A&E areas. In order not to duplicate work, and to support a new direction of travel for Islington, Components 2 & 3 for 2012-13 are new components which seek to address and support the journey and priorities of NHS Islington Clinical Commissioning Group (ICCG) on the delivery of Primary Integrated Care.
2. Aims
The NHS Islington Clinical Commissioning Group was set up in June 2011. It was assigned delegated authority / responsibility for all appropriate budgets, such as community health, acute, prescribing etc by February 2012 and hence is currently acting as commissioner in shadow form until April 2013, when it will take over full responsibility for these budgets as a statutory organisation following the assurance process of authorisation.
It is proposed that the 2012/13 Local Enhanced Service (LES) will aim to:
• Encourage clinical involvement in commissioning generally, including assessing local needs, helping to identify local priorities, and proposing new care pathways
• Promote partnership working between GP practices
• Promote the importance of patient involvement in commissioning and strengthening links with one’s own patients
• Strengthen two-way communication and sharing of ideas between ICCG governing body and constituent practices
• Support constituent practices to use data effectively (e.g. referrals, prescribing) to help change and improve outcomes through peer support.
38

2
• Support risk stratification and implement care planning as key enablers for integrated care
The scheme has been developed following feedback from previous locality commissioning forum discussions and previous years’ schemes, and has transformed further to accommodate new Quality and Outcomes Framework (QOF) Quality and Productivity Markers, and support a new direction of travel for Islington towards integrated care models.
It is proposed that to support achievement of the ICCG objectives for 2012/13, including integrated care and driving up quality through peer support, this LES will cover a range of indicators with a total funding of £538,000. The LES is not dependent upon savings from reduced use of secondary care services.
3. Eligibility
All Islington GP Practices
4. Service Specification
The Clinical Commissioning LES will consist of 6 components which include:
Component1: Active participation at the Pan Islington Engagement Events – reimbursed on attendance for the full meeting together with dissemination and simple documentation and feedback
Component 2: Practice participation with the Governing Body Link (CCG Board Link) twice a year
Component 3: Establishing and developing localities
o Work collaboratively with the elected clinical lead of each locality in identifying Organisational Development/educational needs of the locality through a series of 3 meetings in the year.
Component 4: Integrated Care – Care planning o Development of electronic care plans on EMIS or equivalent GP system for a
percentage of patients identified as medium risk by using PARR ++ (Appendix 6 gives the risk stratification per practice and per locality)
o Implement MDT case conferences for highly complex/high risk patients at locality level including input from secondary care acute (aim to initiate multi disciplinary case conferencing in September following recruitment of case managers)
Component 5: Attendance at the Monthly Multi-disciplinary Case conferences for high risk complex tier 4 patients
Component 6: Continued participation at the locality Patient Participation Group including dissemination of information to patients through display of appropriate leaflets, newsletters, posters etc.
39

3
4.1 Component 1 - Investing clinical and managerial time in Clinical Commissioning
Rationale:
• Empowering professionals and providers by devolving the power and responsibility of commissioning services directly to GPs and their practice teams working in a Clinical Commissioning Group with patient care at its heart, is the core building block of the government’s White Paper.
• In order to support the development of the Clinical Commissioning Group (CCG), it is vital to engage with all constituent practices of the CCG and to get a bottom-up feed into the process, rather than giving information in a top-down approach.
• The inclusion of this indicator in the LES is to recognise that GP input should be adequately resourced to enable clinicians to give the time required without cost.
Requirements:
• Practices to ensure lead commissioning GP engages, participates and attends the Pan Islington commissioning forums. Practice managers/nurses are also encouraged to attend these meetings.
• There will be 6 forums a year pan Islington wide, each lasting minimum 3 hours.
• The attending GP will ensure that he/she feeds back commissioning, QIPP areas, pathway/service development and budgetary information discussed at the forums to the rest of the practice team including practice nurses, practice manager and where appropriate other non-clinical staff.
• Members of the practice are expected to stay for the full duration of the meeting, unless there are exceptional circumstances, as the payment for this component is intended for locum backfill time.
Payment: Payment for Component 1 is contingent on completion of the following:
• GP attendance at GP commissioning forums. Payment will be made on a pro-rata basis for each attendance.
• Practices are asked to complete a feedback form (appendix 2) following dissemination of information and discussion within the practice team
• The payment for this element will be:
Requirement Amount Attendance at 6 forums £3000 per annum
Dissemination/feedback 15 pence per list size Total per practice (based on average list size of 6000)
£3,900 per annum
For single-handed practices ONLY, a Practice Manager may deputise if the GP is unable to attend, however this should be the case for not more than 2 of the 6 meetings.
40

4
4.2 Component 2 – Investing practice time in Board Link peer support sessions
Rationale: The revised model constitution, which is currently out with practices for consultation, supports the role of the Governing Body/Board link Peer Review across its member practices. Each GP member of the governing body has been assigned to a group of practices across Islington – this table is available in Appendix 1 of this LES. The aim of this Board Link process is to:
� Encourage linkages to be developed across localities through shared information and learning across localities as the board link GP may not necessarily be from the same locality as the practice
� Promote integration and integrated working across Islington � Build on the sense of cohesiveness, through the development of relationships
between the CCG Governing body and constituent practices, facilitating communication and the development of shared values
� Have a bottom up approach to commissioning and engagement to ensure all GPs, clinicians and whole practice teams are empowered to drive commissioning forward in Islington
� Support the education development of all clinicians and practice teams through the shadow period to the point of authorisation as a statutory organisation
� Ensure information is available to practices to support their developmental needs and the strategic needs of the practice working within the CCG.
Through practice visits, GP Board Link members will keep practices up to date with relevant strategic areas being developed at Governing Body level, such as analysis of referrals data, primary care prescribing data and analysis of practice budget performance. Practices will be supported to understand and utilise the new data streams to inform their daily practice and will be supported through educational initiatives and mentorship to develop action plans to deliver any changes. This new component of the Clinical Commissioning LES acknowledges that the new process will take time for the practice to engage with the Board Link member. Payment for this component will support practices to have a full practice meeting with their Board Link member, form an appropriate action plan in partnership with their Board Link member, and implement those actions for improvement. Requirements: Meeting with Board Link member:
• At least two practice meetings (ideally with all clinical and non-clinical staff of the practice) with Board Link member per year (1-2 hours per meeting). Each meeting will aim to address any areas of development and support required as well as any concerns/anxieties and how this can be resolved through organisation development.
• The agenda will be agreed before the meeting.
• Information around the practice/locality performance on key indicators will be circulated before the meeting (minimum 5 working days prior to the visit)
41

5
• First meeting to be scheduled between September to mid-November – please send your availability to Margaret Small at [email protected]
Creating an action plan:
• Practices will be required to develop a simple action plan based on their discussions with the Board Link member (areas for inclusion will be agreed during the meeting). A template action plan has been provided for practices to use (appendix 3)
• The action plan must be sent to the Board Link member, who will confirm the actions that the practice will undertake, and the thresholds to aim for.
• The action plan will be sent by the Board Link member to the Commissioning Development office.
Delivering on the action plan:
• Practices are required to create a report (template provided) which outlines the actions implemented by the practice, and the change which has resulted. This will serve to show delivery of the action plan and show evidence for payment of this part of Component 2.
Payment: The following payments are allocated for this component, as outlined below.
Pre-meet within the practice to discuss agenda/actions etc.
Practices will be required to hold pre-meet meetings to agree the agenda and actions and implement within the practice following each meeting
10 pence per registered list size
Meeting with Board Link member
Minimum of 2 x supportive meeting per year with allocated Board Link member.
£300 per meeting
Development of Board Link action plan
Practice to draw up action plan based on discussions with Board Link member at meeting. Action plan is to include goals and reasonable thresholds to measure change and improvement.
£300 per action plan
Performance against action plan
Practice to complete short report discussing actions implemented and the evidence of resulting change / improvement. Payment of this part depends upon the practice achieving the goals and thresholds set out in the action plan
£500 for performance against action plan
Total available for Component 2
£1,700 per practice per board link visit on average list size of 6000
42

6
4.3 Component 3 – Establishing and Developing the Localities
Rationale: This component has been included to support practices to build relationships by coming together in a locality and working together to improve health care for all patients across the locality. This contributes to the overarching vision and objectives of the Islington CCG. It will promote and enable collaborative working within a locality through sharing best practice. Practices will be expected to contribute to the Islington extranet where appropriate, sharing material and experience across the four localities. To support GPs through this transition towards more collaborative working, Islington CCG will establish a development programme for the 4 GP localities which will be led by the elected Clinical GP lead of the locality. This will include: An Organisation Development framework which allows groups of practices to identify gaps/weakness or areas of development which will support the implementation of Islington primary integrated care plan as well as the vision and objectives of the Clinical Commissioning Group.
Requirement:
• A GP member from each practice to meet in the locality for 3 meetings during 2012/13 (ideally same GP to attend all three meetings – except for unforeseen circumstances where another GP from the practice or practice nurse will attend)
Each meeting would aim to last maximum 3 hours
43

7
Please note this is NOT about practices merging but about working collaboratively to achieve the best outcomes for their patients and the wider population. Payment: All practices within the locality will be reimbursed £300 per meeting. Total per practice per annum £900 per meeting
4.4 Component 4 – Integrated Care - Care Planning
Developing care plans with the patient/carer is aimed at addressing an individual’s full range of needs, taking into account their health, personal, family, social, economic, educational, mental health, ethnic and cultural background and circumstances. It is a holistic process which recognises that other issues apart from medical ones, can impact on a person’s total health and well-being. The process focuses strongly on helping people (together with their carers where appropriate) to achieve the outcomes they want for themselves; for example to live independently, or return to work. It is important to note that whilst people with long term conditions might spend 3 hours per year with a healthcare professional, they spend 8000 hours per year taking care of themselves. Care planning can support them to do just that, and can lead to a range of benefits for individuals, commissioners, providers of services and the health and social care workforce
1.
These centre on:
• embedding the personalisation of care and services ‘adding life to years’;
• promoting health through information and self-care, people staying healthier for longer and therefore ‘adding years to life’;
• promoting independence and achievement of other goals such as returning to work or living independently;
• reducing health inequalities by standardising care across the country;
• promoting integration and partnership working;
• stimulating genuine choices, and those choices feeding into commissioning decisions;
• promoting a more planned, proactive approach to health and social care services;
• efficiency savings, e.g. reductions in hospital admissions, outpatient appointments and GP consultations;
• improved user and staff satisfaction, including fewer complaints
1 ‘Supporting people with long term conditions – Department of Health, 2009, at
http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_093360.pdf
44

8
A) Identifying the appropriate patients for care planning
Islington is currently looking at a range of risk stratification tools which use a range of data sources such as acute, primary care and social care to risk stratify the whole population. In order to progress forward with care planning, it has been agreed to begin looking at the population at risk of readmission using the acute data set and running it through the PARR tool. Appendix 6 indicates the number of patients in each risk category per practice and per locality. The graph below gives the risk per 1000 patients/per practice and grouped in each proposed locality. Please NOTE the data below will NOT be used as part of performance
45

9
management but will be used to support the peer review discussion as well as through the Board link peer review support. Graph 1: Average risk per 1000 patients per practice in each locality using PARR tool – acute data for 2011/12
Key Elements for a Care Plan including implementation of organisational changes within the practice to implement elements years of care which include sharing appropriate test results prior to the care planning consultation
46

10
Process for developing a care plan includes: Medium Risk Patients
a) Initial appointment of the identified patient with a GP. GP to explain care planning
and what it means to the patient and obtain written consent from the patient or carer.
b) Practice staff to arrange for appropriate blood tests/diagnostics prior to care planning consultation with the results sent to the patients with a brief description where appropriate to empower patients to have an informed discussion at the care planning consultation
c) Practice nurse/GP to set a 40 minute appointment for care planning consultation with the patient/carer.
Care plan may identify gaps in patient’s care management and may require involvement of other multidisciplinary groups such as Community Matrons, Social worker, District nurses, community mental health team etc. Practices must code each patient for whom they have completed a care plan – practices are to use the defined read codes (the CCG are currently developing a care planning template and further information will be sent out as soon as possible) Care planning may include signposting to traditional and non-traditional services. Practices must provide a copy of this care plan to the patient – whether this be via a print out at the time of the consultation or by letter after the consultation.
d) 2 week telephone follow up following agreement of care plan via practice staff – HCA/receptionist
47

11
e) Agree a 3 month review following care plan with GP – note progress made on agreed goals and make appropriate referrals to wider community/specialist team
f) Review at 6 months with GP
Training for GPs and practice team on care planning is being sought at present and this will be provided with a range of options for practices to support development of care planning and to embed the culture shift in primary care on goal setting and delivering a patient centred care plan. Practices will be given a list of patients to be prioritised for year one to support the implementation of care planning process in practice hence payment in the overarching clinical commissioning LES is based on the list size rather than per care plan as it is recognised that practices need to set up systems to support the implementation of this. Payment: Practices to be paid 75p per registered patient based on list size (31
st march 2012). For
a practice with an average list size of 6000 this will equate to approximately £4,500. Payment is subject to submission of:
• Number of completed care plans against identified list of medium risk patients
• A reflection report which will include a summary of outcomes achieved or not achieved. It is expected that these will also form part of the education programme of the locality led by the nominated clinical lead.
Templates on EMIS web with prompts are currently being developed and will be circulated shortly.
4.5 Component 5 – Multi Disciplinary Team Meetings
Rationale: As outlined in the Primary Care Implementation Plan, it is proposed to have monthly multidisciplinary (MDT) case conferences to manage the high risk complex tier 4 patients. GPs will represent their patients at these monthly meetings (face to face or virtual as agreed by the locality). All MDT meetings will be chaired by the locality Clinical Lead GP and supported by the locality integrated care administrator and clinical case manager (generalist community matron).
Please note it is essential for nay patients identified under Component 4/5 should have consented to be involved in the care planning as well as more importantly in the multidisciplinary team meetings. Process map for MDT is attached in Appendix 4 Requirements
• Practices to participate face to face/virtually through clinical representation initially GP
monthly case conferencing for tier 3 or 4 complex patients.
48

12
• Practices to act on actions following the meeting. Actions co-ordinated by the locality
care co-ordinator
Payment:
Practices to be paid £100 per hour for attendance and participation and carrying out any
actions at each monthly MDT meetings (monthly maximum £300)
4.6 Component 6 - Patient and Public Participation
Rationale:
• The Health and Social Care Act 2012, enacted on 27 March 2012 puts patients at the heart of the NHS through shared decision-making and being given the information they need to be able to exercise choice.
• ‘Clinical Commissioning: Our Vision For Practice-Based Commissioning’ published by the Department of Health, notes: ‘Successful practice-based commissioning will be rooted in strong systems and cultures of patient and public engagement, ensuring that decisions reflect the diverse needs of local patients’.
• The purpose of this component of the LES is to engage and involve patients through all levels of commissioning, as well as to identify areas of patient need, which helps ensure a bottom-up approach to commissioning and service re-design in light of the White Paper and the new Health and Social Care Act 2012.
• Locality patient participation / engagement groups (PPGs) were formed through practice based commissioning and meet quarterly in North, Central and South localities. Every alternate patient group meeting has a one-hour section which brings the localities together for Pan-Islington discussion. The reason for the merge is to increase patient involvement and interaction by forming a larger group with better ability to share and discuss information across the whole of Islington, and increase efficiency by running one group instead of several.
• The patients who are to be involved in this quarterly PPG should be sourced from the practices’ Patient Reference Groups which have been set up as part of the Patient Participation DES. This will facilitate the sharing of information between Islington-wide / locality groups, and the smaller practice reference groups.
• This element of the LES aims to enable GP Clinical Commissioners to engage patients in the commissioning process and to use the patient groups to discuss commissioning issues.
• Note that in the past, the patient group voice has led to the setting up of South and Central phlebotomy outreach clinics.
Requirement:
• Practices must sign up to the Patient Participation DES to be eligible for payment under Component 5 of this Clinical Commissioning LES, as this closely ties in with DES Practice Patient Reference Groups.
• Practices must advertise information on the Islington-wide patient group and proactively identify patients who may be interested.
49

13
• All practices will participate in consultations with the patient group and reflect on the impact of the consultations at borough level, locality level or at practice level where appropriate.
• Practices must attend the PPG with at least one patient from their Reference Group to gain full payment at each meeting.
• They must disseminate the written update / newsletter on areas from the PPG including community alternative services etc. where appropriate. There should be 3 updates produced in a year.
Payment: Payment for Component 5 is made to practices on the following basis: £400 will be paid to each practice per meeting, as long as:
• The practice has signed up to the Patient Participation DES.
• The Commissioning Lead GP for the practice and at least one patient from their patient reference group attends the meeting.
• Practices to act on the actions following the PRG and make appropriate changes in practice which may include improving notice boards, ensuring the information on services is readily available to the patients including display information on the Patient group, the benefits, dates in the diary etc as well as to display patient update / newsletter on a regular basis when available etc
• If a practice manager attends each quarterly meeting with a patient from the practice instead of the Commissioning GP, this will amount to £600 total for each practice per year.
5. Payment Schedule
Following sign up to the LES, practices will be awarded 50% upfront payment (by end of October 2012) with the remainder to be paid on achievement of the markers at year end.
Payment through Proposed LES Breakdown of payments
Average practice payment (based on average list size of 6000)
Component 1 £3,000 + 15p per list size £3,900
Component 2
10p per list size + £300 per Board Link Member meeting £300 per action plan £500 for performance against action plan £2,800
Component 3 £300 for 3 meetings £900 Component 4 75p per list size £4,500
Component 5 £100 per hour £3,600 Component 6 £400 x 4 meetings £1,600
Total payment for LES £16,900
6. Monitoring
The Performance Measure
Method i.e. Monitor, Audit or Portfolio
Frequency Responsibility of
GP attendance at commissioning forum. Feedback forms
Attendance sheets & submission of feedback form
Bi-monthly Practice
50

14
Meeting with Board Link GP. Forming action plan. Reporting on action plan implementation
Submission of action plan & follow up report
Twice a year Practice
Attendance at locality Organisation Development meetings
Attendance sheet 3 meetings per year
Practice
Completed care plans for identified patients. Reflection report
Review number of care plans Submission of reflection report.
3month review, 6 month review and Yearly
Practice
Attendance/involvement at MDT meetings
Attendance report from care coordinator
Monthly Practice
Sign up to patient participation DES. Attendance at PPG meetings. Action follow up
Evidence of DES sign up. Attendance sheet Monitor practice changes
Quarterly Practice
7. Review of the Service
The Clinical Commissioning LES has been drawn up by the Primary Care Commissioning Development team working closely with CCG colleagues and LMC colleagues. It will be managed and monitored by the ICCG Primary Care Commissioning Development team. The Clinical Commissioning LES will be reviewed on an annual basis and feedback from practices will be used to shape a future LES.
8. Variation/Termination of Agreement
NHS NCL will also give a minimum of 3 months notices to the practice.
9. Protecting Patient Confidentiality
All patient level data should be sent to [email protected] as per the agreement outlined in section 6 and inline with Caldicott Guardianship principles.
9. Supporting Documents
See Appendices 1 – 5 below
51

15
52

16
Appendix 1: GP Board Link Members attached to a Practice
GP F-CODE
LEAD GP NAME
PRACTICE NAME
Name of GP Board Member
F83012 MULVIHILL Elizabeth Ave Group Practice
Anjan Chakraborty
F83034 SKELLY New North Health Centre
Anjan Chakraborty
F83064 COLEMAN City Road Medical Centre
Anjan Chakraborty
F83678 SEGARAJASINGHE
The Pine Street Medical Centre
Anjan Chakraborty
F83031 FLINDERS Bingfield Practice
Anjan Chakraborty
F83010 MARSHALL Islington Central Medical Centre
Gillian Greenhough
F83015 AARONS St Johns Way Medical Centre
Gillian Greenhough
F83039 SALKIND The Rise Group Practice
Gillian Greenhough
F83671 MONEEB Hornsey Rise Health Centre
Gillian Greenhough
F83002 BUNT River Place Health Centre
Jo Sauvage [email protected]
F83021 HAZELWOOD Ritchie Street Group Practice
Jo Sauvage [email protected]
F83060 KINSELLA The Northern Medical Centre
Jo Sauvage [email protected]
F83686 CHAKRABORTY
Stroud Green Medical
Jo Sauvage [email protected]
F83004 KOYA Archway Medical Centre
Karen Sennett [email protected]
F83053 WHEELER Mildmay Medical Practice
Karen Sennett [email protected]
GP F-CODE
LEAD GP NAME
PRACTICE NAME
Name of GP Board Member
Email address
53

17
F83056 RATNAVEL The Surgery, 2 Mitchinson Road
Karen Sennett [email protected]
F83648 HANS 18 Dartmouth Park Hill
Karen Sennett [email protected]
F83681 ROSENTHAL Partnership Primary Care Centre
Karen Sennett [email protected]
F83013 WOOLF 94-96 Holloway Road
Katie Coleman [email protected]
F83033 HAFFIZ Barnsbury Medical Practice
Katie Coleman [email protected]
F83045 BENNETT The Miller Practice
Katie Coleman [email protected]
F83660 TROSSER Highbury Grange Health Centre
Katie Coleman [email protected]
F83008 BATTLE Goodinge Health Centre
RathiniRatnavel [email protected]
F83063 SENNETT Killick Street Health Centre
RathiniRatnavel [email protected]
F83664 MCDAID The Village Practice
RathiniRatnavel [email protected]
F83673 EDOMAN 140 Holloway Road
RathiniRatnavel [email protected]
F83680 GUPTA Sobell Medical Centre
RathiniRatnavel [email protected]
F83007 SHAH Roman Way Medical Centre
Sabin Khan [email protected]
F83032 HAUGHEY St Peters Street Medical Centre
Sabin Khan [email protected]
F83051 KO 244 Tufnell Park Road
Sabin Khan [email protected]
F83674 KATEB 244 Tufnell Park Road
Sabin Khan [email protected]
Y01066
MCLEAN Hanley Primary Care Centre
Sabin Khan [email protected]
F83027 BOWRY The Family Practice
Sharon Bennett [email protected]
F83624 BAINES Clerkenwell Medical Practice
Sharon Bennett [email protected]
F83630 HUSSAIN 5 Wedmore Gardens
Sharon Bennett [email protected]
F83652 DAVIES The Amwell Practice
Sharon Bennett [email protected]
54

18
F83666 VARMA Andover Medical Centre
Sharon Bennett [email protected]
Key Principles of attaching Board members to GP
practices
1. No Board GP member will be attached to their own practice
2. No Board GP member attached to any locality
3. All Board GP Members to have a mix of single-handed and group practices
Appendix 2 FEEDBACK FORM This report is to be completed following dissemination of information with the practice teams following the bimonthly Pan Islington events.
55

19
Practice Name and address: Date of Submission of Report: Practice Clinical Commissioning Lead:
Date of practice meeting to discuss the information from the Pan Islington Forum:
Attendance: (must include all clinical and non-clinical members within the practice)
Name Job Title Name Job Title
1. 5.
2. 6.
3. 7.
4. 8.
Areas/Topics discussed Please state in the box below the areas/topics discussed within the practice following Pan Islington event
2.Please state any agreed actions for implementation within the practice following the event
Key Actions for Implementation and Achievement of Objectives Objective Action Plan Expected
Outcome Completion Date
Person Responsible
**Please add more lines to the action table as appropriate Sign off: The Clinical Commissioning lead of the practice should sign off this report.
Name Signature Date
Thank you. Please submit to [email protected]
By XX
Appendix 3 – Board Link Peer Review Action Plan Template
56

20
SUMMARY REPORT – This report is to be completed following Board Link Peer Review Meeting with the practice teams
Practice Name and address: Date of Board Link Meeting: Name of the Board Link GP: Practice Clinical Commissioning Lead:
Attendance: (must include all clinical and non-clinical members within the practice)
Name Job Title Name Job Title
1. 5.
2. 6.
3. 7.
4. 8.
2.Please state any agreed actions for implementation within the practice following the event
Key Actions for Implementation and Achievement of Objectives Objective Action Plan Expected
Outcome Completion Date
Person Responsible
**Please add more lines to the action table as appropriate.
Sign off: The Clinical Commissioning lead of the practice should sign off this report.
Name Signature Date
Thank you. Please submit to [email protected]
By XX
APPENDIX 4: PROCESS MAP FOR MDT CASE CONFERENCING *Patients on the Community Caseload – assumes care plan available and consent obtained
List of patients per practice in sub-
Identification of Tier 4 Complex
patients across Islington using risk
stratification tool
57

21
Patient Consent Obtained –
initially verbally but ideally
requires written consent from
patient/carer
Patient registered GP practice
informed of these patients
Care co-ordinator to put
all the patients’
information on the
database
GP and CM to agree who is best
placed to develop a care plan for the
identified patients (GP, CM, CMHT,
SS or DN)
Care Co-ordinator in liaison with the CM schedule monthly MDT case
conferencing at agreed locations in the sub-locality and invites all key
stakeholders appropriately. Agenda and actions from previous meeting
to be circulated in advance.
Sub-locality Clinical
Lead to Chair the MDTs
Appropriate GP
attendance for each
MDT – face to face or
virtual
Each monthly MDT approximately 3 hours; Approximate time per
case is initially 20-25 minutes; Total cases per MDT approximately 5-
7
Following each MDT, care co-ordinator writes up actions and follows
them up with the appropriate leads before the next meeting.
Lead professional allocated per patient informs the patient/carer of the
outcome of the case conference and update care plan accordingly
following patient consensus.
Clinical lead
identifies areas of
development or
gaps in services,
feeds back &
develops an
action plan
Where
appropriate,
patient can
attend the
case
conferencin
g
58

22
Appendix 5 - Risk Stratification Using PARR tool
59

From: Dougan, Sarah [mailto:[email protected]]
Sent: 05 October 2012 17:53 To: Robbie Bunt
Cc: Nicola Rice; Osuagwu, Uche Subject: Section 251 application for linkage of GP data with hospital admissions
Robbie
You will recall that I came along to an LMC meeting several months ago now to discuss getting
permission from the NIGB via a section 251 application to link patient identifiable GP data with
hospital admissions data. Their process has been quite lengthy (partly because it’s been changing
because of the transition) but we have recently heard that we have obtained permission to
undertake the linkage and that section 251 will provide the legal basis for us to do so without the
need to get individual patient consent.
The next steps would therefore be to obtain individual GP practice consent, and so I would like to
write to all GP practices shortly to ask for this.
I’ve attached the proposed letter, the suggested wording for the patient information poster, and the
data sharing agreement, as well as the original application form and the final approval from the
NIGB. I haven’t included the full dataset specification and the system level security policy as the
number of documents was getting quite large, but if you wanted to see these then Uche Osuagwu
(cc’d in here) can provide copies as I will be on leave next week. He can also answer any initial
questions you/colleagues may have.
I’d be happy to receive any comments on the letter, information poster and data sharing agreement
from the LMC before I send this out to practices. I appreciate that you are all busy but I’d be grateful
if we could get comments back on this fairly quickly, as I’m going on maternity leave from mid-
December and want to make sure I’m around to oversee all of the linkage and deletion of the
patient identifiable information in plenty of time before I go.
Best wishes
Sarah
Dr Sarah Dougan
Senior Public Health Manager: Health Intelligence & Needs Assessment
Islington Public Health
0207 527 1258
60

Chair: Paula Kahn NHS North Central London is a collaborative working arrangement between Barnet, Camden, Enfield, Haringey and Islington Primary Care Trusts Chief Executive: Caroline Taylor
Islington Public Health 1st floor
222 Upper Street London N1 1XR
Dear Colleague
RE: Identifiable GP dataset for public health analysis under section 251 agreement – extraction from your practice
With the full support of Islington’s LMC and Islington’s CCG, the Public Health team applied to the
National Information Governance Board (NIGB) for Health and Social Care to obtain permission to
link patient identifiable GP data with hospital admissions data in Islington. We have just heard that
this application has been successful and that we have been granted permission to do this.
Being able to link GP data with hospital admissions data will allow us to look at what is happening
across primary and secondary care, enabling us to answer questions such as:
1. What percentage of people are being diagnosed with long term conditions through an
emergency admission? Who are these people?
2. Are those being admitted for flu and pneumonia admissions people who have not been
immunised?
3. What is the impact of serious mental health problems and/or alcohol abuse on hospital
admissions in Islington? Are these particular groups within this population who are
disproportionately using secondary care?
4. What are the patterns of hospital use for people living with diabetes and other long term
conditions?
At a pan-Islington level, answers to these questions and others will enable us to provide evidence
to underpin local strategies to reduce hospital admissions and to provide integrated care for
patients. It will also help us to better target some of our public health programmes, such as
immunisation and initiatives to diagnose people earlier. We also hope that by providing practice-
level analysis that the work will also help inform priorities for your GP practice in relation to
improving population health outcomes.
Our Ref: Your Ref: Direct Line: e-mail: web: Date:
GPPHdataset_section251 0207 527 1258 [email protected] www.ncl.nhs.uk 5th October 2012
61

Chair: Paula Kahn NHS North Central London is a collaborative working arrangement between Barnet, Camden, Enfield, Haringey and Islington Primary Care Trusts Chief Executive: Caroline Taylor
While we now have a legal basis for using patient identifiable data (NHS number and postcode) for
the purposes outlined in the section 251 application, we still require your individual GP practice
consent as you are the data controllers for your patients’ data1. All of the details of the section 251
application and approval, the security policy, and the specification for data extraction are included
in the attachments which have been sent out with this letter.
For all EMIS practices, extractions will be undertaken via EMIS’ central data warehouse, which will
have no impact on the running of your practice system. For VISION, we will be working with an
extraction company and/or GP IT to undertake the extraction and will be in touch separately about
this.
If you would be happy for your practice’s data to be used for the purposes outlined, then I would be
grateful if you could complete the attached data sharing agreement. You need to sign page X
and return the signed form to [email protected] or to Sarah
Dougan at the address above. If you do consent, then we will also provide your practice with
some updated patient information posters which outline that patient data may be used for these
purposes and which we would strongly recommend that you display in your waiting rooms.
I hope that you and your team will be supportive of this initiative to improve the understanding of
population health outcomes across Islington, and to provide evidence to support the design and
implementation of pan-Islington strategies. The public health team are always happy to come and
talk to your practice about our work, so if you would like a visit to discuss this project or have any
questions about this, please let me know.
Yours sincerely
Dr Sarah Dougan Senior Public Health Manager: Health Intelligence and Needs Assessment
Inc.:
1. Section 251 application 2. Approval letter from the NIGB 3. Data sharing agreement (including full data specification and system level security policy in
appendices)
1Individual patient consent is not required as we have permission under the section 251 application to
undertake this work.
62

63

64

65

66

67

68

69

70

71

72

73

74

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 1 17/10/12
Islington PCT - GP Practice - Public Health PID Extraction Data Sharing Agreement
75

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 2 17/10/12
Who is sharing the Information?
Lead Organisation Islington Primary Care Trust GPs Other Organisations Islington Primary Care Trust
Executive Summary
Introduction The Public Health Intelligence team in Islington PCT have made a section 251 application to extract and then link Islington GP data to hospital admissions data (i.e. SUS data) and demographic data (postcode-level data: MOSAIC, Indices of Multiple Deprivation scores) before being anonymised. This application was made with full support of Islington’s LMC and Islington’s CCG. The anonymised dataset will enable public health (population-level) analysis to be carried out. The outputs from the analysis will be used to inform commissioning and strategic decision-making by Health and Wellbeing partners in Islington. Findings will directly inform the Joint Strategic Needs Assessment which will form the basis of the local Health and Wellbeing Strategy, and will be used to evaluate public health interventions. Specific analysis will also directly inform the work of the newly formed Clinical Commissioning Group (CCG) and the implementation of the local primary care strategy. In addition, tailored outputs will be sent back to individual GP practices so that, where appropriate, they can also take steps to improve the quality of their patient care and management. This document seeks to establish a framework and agreement to share this data between General Practices in Islington and the Public Health Intelligence team in Islington Primary Care Trust (PCT) in order to ensure that information is managed and shared on a legitimate and secure basis. The main objectives of this data sharing agreement are:
• To ensure compliance with the conditions for processing the data as defined by the Ethics and Confidentiality Committee of the National Information Governance Board in the section 251 approval letter;
• To increase awareness and understanding of the relevant legislation and especially the Data Protection Act 1998;
• To provide information and guidance with regards to the lawful management, access and sharing of data held on both EMIS and INPS VISION systems
• To encourage lawful flows of information;
• To support a process, which will monitor and review information flows; and
• To raise accountability across the organisations signatory to this Agreement. This data sharing agreement will be used in conjunction with the contracts, service level agreements or any other formal agreements that already exist between the organisations signatory to this agreement.
76

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 3 17/10/12
Background
For the purposes of this activity, the vast majority of the data will be extracted from Islington GP practices from EMIS’ central data warehouse. EMIS is a modular clinical IT system primarily used in primary care settings. The data are held on a remote server which contains the records of the General Practices that have successfully completed the streaming phase. Data is streamed to the remote server from the practice’s own EMIS Web, EMIS LV or EMIS PCS system.
The EMIS central data warehouse can provide access to the data or the records of patients via the central EMIS team, once the GP practice has granted specific permission via a signed data sharing agreement to view a specific dataset made up of individual patient records.
The vast majority of the GP Practices in Islington run EMIS systems. However, there is one practice in Islington that runs INPS’ VISION system. The data extraction process from this practice will be different to those described above for EMIS. However, data is needed from this practice as well and therefore this agreement also covers this type of system. The GP IT department of Islington PCT will manage and process the data securely on behalf of the Public Health Intelligence team. The Public Health Intelligence team will carry out analysis using anonymised dataset after the linkage processes have been carried out by the GP IT team. Following the linkage process, the patient identifiable data (PID) used to link the GP data and the hospital admissions data will be destroyed.
77

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 4 17/10/12
The Process EMIS will carry out data extractions for the vast majority of Islington GP practices. This data will include some patient identifiable data (PID). The following identifiers will be used:
• NHS Number;
• Postcode. For those practices using EMIS systems, the extractions will be carried out by EMIS from their Data Warehouse. The data will be transferred securely to the GP IT department via a secure FTP download provided by EMIS. For the practice using In Practice Systems (VISION) data will either be extracted using MIQUEST or SQL queries carried out by a contracted data extraction company. The data extracted in this method will be transferred securely to the GP IT department either via NHSMail or via a secure FTP download provided by the company. NOTE – At this stage the contracted company is still to be nominated. All GP data containing PID will be transferred and held on a stand-alone server located in the GP IT department and only accessed by the two members of the GP IT team listed in the appendix. PID will only be stored on the server for the time period that allows for the data to be linked to SUS data to create the anonymised dataset. For each practice, this is expected to be one week after its data is uploaded, after which time the PID parts of the data will be deleted. Due to the variations of time that data extractions from all practices will be received, the maximum retention period for any PID as part of this project will be 30 days. It is essential to note that under the section 251 application approval conditions, PID data may only be used / retained until 31/03/2013. Islington PCT will fully comply with this condition by undertaking this project before this deadline.
Legal Basis It is essential that the sharing of data is permitted by the Data Protection Act 1998, complies fully with the Common Law Duty of Confidentiality, the Caldicott Principles and contractual obligations. To establish whether there is a legitimate basis for sharing data, the purpose must be justified taking account of the core legislation that governs data sharing between General Practices and Commissioning Organisations. An outline of the purposes for sharing data and the legal principles governing the sharing of data between Islington GP Practices and Islington PCT is as follows:
Purpose and Justification for Sharing the Information
1. Use of full postcode and linkage to geographical areas and deprivation Islington PCT’s Public Health Intelligence team want to extract full postcode from GP IT systems for each patient so that geographical analysis can be undertaken to look at the impact of the wider determinants of health. Without extracting full postcode from GP IT systems it will not be possible to undertake public health analysis by area of residence (e.g. ward and lower superoutput area) or to look at differences by deprivation, Mosaic™ type (geodemographic segmentation) and housing tenure at a population level. We were able to do this in 2011 because we used took an anonymised data extract for public health analysis from the data that had been extracted from GP IT systems to run the King’s Fund Combined Tool to identify individual patients that were at risk of being admitted to hospital. Patient identifiable data was used in the King’s Fund Combined Tool as it was directly informing patient care (ie. high risk patients would be contacted by their GP / specialist nurse). This tool is no longer running in Islington, so now we need to extract the data directly from GP practices. 78

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 5 17/10/12
Using the postcode to link to other key variables is important for the following reasons:
- a. Understanding different geographical patterns in disease prevalence and uptake of interventions (eg. smoking cessation) is important to enabling us to focus public health and NHS resource to the right locations. This includes investment in community settings (eg. offering of NHS Health Checks in supermarkets), as well as at pharmacies, and the distribution of nursing teams across Islington. b. Having information on deprivation, types of housing and geodemographic segmentation information via Mosaic™ is important to have a better understanding of the wider determinants of health. This includes the impact of poverty on health and wellbeing which is a key factor in understanding why some people experience worse population health outcomes. In Islington, taking poverty into account in public health analyses is vital as Islington is one of the most deprived boroughs in London and there are substantial health inequalities among different groups within the borough.
2. Linkage of GP data and hospital admissions data using NHS number
To link the GP data to hospital admissions data, NHS number is required as this is the shared unique identifier. Linking of the GP data to hospital admissions presents a major opportunity to inform commissioning strategies and intentions, reduce hospital admissions (making best use of resources), bring care closer to home, and to generally improve patient outcomes and quality of care. Specific areas which would be informed by this approach include:
- quantifying the differences in who is being admitted to hospital (eg. how much more likely is someone with a mental health problem likely to be admitted and for what?). This would inform the amount of resource being invested in particular issues, and particularly the cross-cutting ones like mental health problems, alcohol, smoking and obesity, as well as common comorbidities (eg. across cardiovascular conditions and with CKD). Currently it is impossible to capture the impact of these cross-cutting issues on secondary care using hospital admission records because underlying conditions are not systematically recorded.
- determining whether those admitted had previously had their conditions diagnosed and if so, if it was under control. This would inform our local integrated care strategies as late diagnosis would indicate missed opportunities for diagnosis and prevention of hospital admissions. If we are able to identify clear patterns from our analysis we will be able to make system-level changes.
- helping to explain variation in admissions rates by GP practice. This is important for individual GP practices to better understand what more they can do to reduce hospital admissions among their patients and to explain practice-level variation.
- looking at the impact of local interventions to reduce hospital admissions. We have several local initiatives to reduce hospital admissions, including for example, a scheme in which GPs are incentivised to better manage patients with COPD. We are currently unable to evaluate whether or not this is having an impact on hospital admissions because we cannot link the GP data with the hospital admissions. We also have a very high rate of flu and pneumonia admissions but it is currently not possible, on a population level, to determine whether these patients have received vaccinations for flu and pneumonia.
Using routinely available data, it is currently not possible to do any of the above without expending a lot of resource and clinical time on getting GPs to audit their patients. In addition, they would be unable to do this for the whole population which may introduce bias
and would not allow us to identify less common issues.
79

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 6 17/10/12
80

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 7 17/10/12
Legislation The following provide the core legislation that govern the sharing of information within the NHS: The General Medical Services (GMS) Contract The GMS contract places an obligation on General Practices to provide this information. Clause 439 of the GMS contract states: the Contractor shall, at the request of the PCT, produce to the PCT or to a person authorised in writing by the PCT or allow it, or a person authorised in writing by it, to access, on request-439.1. any information which is reasonably required by the PCT for the purposes of or in connection with the Contract; and 439.2. any other information which is reasonably required in connection with the PCT’s functions. This is then qualified by 442. The Contractor shall not be required to produce information under clause 441 which- 442.1. is confidential and relates to a living individual, unless at least one of the conditions specified in clause 443 applies; and 443 states 443.1. the information can be disclosed in a form from which the identity of the individual cannot be ascertained taking account of other information which is in the possession of, or likely to come into the possession of, the person to whom the information is to be disclosed; or 443.2. the individual consents to the information being disclosed. Clause 443.1 of the GMS Contract is satisfied by: As of 28
th September 2012, the National Information Governance Board has granted
permission to Islington PCT to access PID data without patient consent in line with section 251 of the NHS Act 2006 and the Health Service (Control of Patient Information) Regulations 2002. This permission is valid until up to 31
st March 2013. If at a later time a further extraction is
required then another application will be required. National Health Service Act 2006 section 251:
251 Control of patient information
(1) The Secretary of State may by regulations make such provision for and in connection with requiring or regulating the processing of prescribed patient information for medical purposes as he considers necessary or expedient—
(a) in the interests of improving patient care, or
(b) in the public interest.
(2) Regulations under subsection (1) may, in particular, make provision—
(a) for requiring prescribed communications of any nature which contain patient information to be disclosed by health service bodies in prescribed circumstances—
(i) to the person to whom the information relates,
81

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 8 17/10/12
(ii) (where it relates to more than one person) to the person to whom it principally relates, or
(iii) to a prescribed person on behalf of any such person as is mentioned in sub-paragraph (i) or (ii),
in such manner as may be prescribed,
(b) for requiring or authorising the disclosure or other processing of prescribed patient information to or by persons of any prescribed description subject to compliance with any prescribed conditions (including conditions requiring prescribed undertakings to be obtained from such persons as to the processing of such information),
(c) for securing that, where prescribed patient information is processed by a person in accordance with the regulations, anything done by him in so processing the information must be taken to be lawfully done despite any obligation of confidence owed by him in respect of it,
(d) for creating offences punishable on summary conviction by a fine not exceeding level 5 on the standard scale or such other level as is prescribed or for creating other procedures for enforcing any provisions of the regulations.
(3) Subsections (1) and (2) are subject to subsections (4) to (7).
(4) Regulations under subsection (1) may not make provision requiring the processing of confidential patient information for any purpose if it would be reasonably practicable to achieve that purpose otherwise than pursuant to such regulations, having regard to the cost of and the technology available for achieving that purpose.
(5) Where regulations under subsection (1) make provision requiring the processing of prescribed confidential patient information, the Secretary of State—
(a) must, at any time within the period of one month beginning on each anniversary of the making of such regulations, consider whether any such provision could be included in regulations made at that time without contravening subsection (4), and
(b) if he determines that any such provision could not be so included, must make further regulations varying or revoking the regulations made under subsection (1) to such extent as he considers necessary in order for the regulations to comply with that subsection.
(6) Regulations under subsection (1) may not make provision for requiring the processing of confidential patient information solely or principally for the purpose of determining the care and treatment to be given to particular individuals.
(7) Regulations under this section may not make provision for or in connection with the processing of prescribed patient information in a manner inconsistent with any provision made by or under the Data Protection Act 1998 (c 29).
(8) Subsection (7) does not affect the operation of provisions made under subsection (2)(c).
(9) Before making any regulations under this section the Secretary of State must, to such extent as he considers appropriate in the light of the requirements of section 252, consult such bodies appearing to him to represent the interests of those likely to be affected by the regulations as he considers appropriate.
(10) In this section “patient information” means—
(a) information (however recorded) which relates to the physical or mental health or condition of an individual, to the diagnosis of his condition or to his care or treatment, and
82

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 9 17/10/12
(b) information (however recorded) which is to any extent derived, directly or indirectly, from such information,
whether or not the identity of the individual in question is ascertainable from the information.
(11) For the purposes of this section, patient information is “confidential patient information” where—
(a) the identity of the individual in question is ascertainable—
(i) from that information, or
(ii) from that information and other information which is in the possession of, or is likely to come into the possession of, the person processing that information, and
(b) that information was obtained or generated by a person who, in the circumstances, owed an obligation of confidence to that individual.
(12) In this section “medical purposes” means the purposes of any of—
(a) preventative medicine, medical diagnosis, medical research, the provision of care and treatment and the management of health and social care services, and
(b) informing individuals about their physical or mental health or condition, the diagnosis of their condition or their care and treatment.
(13) In this section—
• “health service body” means any body (including a government department) or person engaged in the provision of the health service that is prescribed, or of a description prescribed, for the purposes of this definition,
• “processing”, in relation to information, means the use, disclosure or obtaining of the information or the doing of such other things in relation to it as may be prescribed for the purposes of this definition.
Section 251 of the NHS Act 251 is satisfied by: As of 28
th September 2012, the National Information Governance Board has granted
permission to Islington PCT to access PID data without patient consent in line with section 251 of the NHS Act 2006 and the Health Service (Control of Patient Information) Regulations 2002. This permission is valid until up to 31
st March 2013. If at a later time a further extraction is
required then another application will be required.
Human Rights Act 1998 Article 8:
Right to respect for private and family life
1 Everyone has the right to respect for his private and family life, his home and his correspondence.
2 There shall be no interference by a public authority with the exercise of this right except such as is in accordance with the law and is necessary in a democratic society in the interests of national security, public safety or the economic well-being of the country, for the prevention of disorder or crime, for the protection of health or morals, or for the protection of the rights and freedoms of others.
83

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 10 17/10/12
Article 8 of the DPA 1998 is satisfied by:
In pursuit of a legitimate aim
Conducting the analysis to look at the impact of the wider determinants of health and
improve public health services and investment is a legitimate aim.
Proportionate Information to be shared through this agreement shall be limited to that required to
support the work of this activity in line with the conditions set by the Ethics and Confidentiality Committee.
Confidentiality
As of 28
th September 2012, the National Information Governance Board has granted
permission to Islington PCT to access PID data without patient consent in line with section 251 of the NHS Act 2006 and the Health Service (Control of Patient Information) Regulations 2002. This permission is valid until up to 31
st March 2013. If
at a later time a further extraction is required then another application will be required.
Appropriate and necessary to a democratic society
Conducting public health analysis and working to increase the effectiveness of the health services offered to patients whilst complying with the law and respecting the confidentiality of personal data.
The Data Protection Act 1998 (“DPA 1998”) 1. Compliance with the DPA 1998 should ensure that when personal information is used
or disclosed, it is done safely and with regard to the rights of the individual concerned. The DPA 1998 does not apply to information relating to the deceased.
2. The personal information falling within the meaning of “Personal Data” includes
expressions of opinion about individuals and indications of intentions of persons in relation to individuals. The DPA 1998 applies to manual and electronic records. For some categories of manual personal information there are exemptions from some aspects of the DPA 1998 up to 24 October 2007.
3. The “processing” of personal information by “data controllers” (i.e. the person or
organisation that alone or jointly with others determines the purposes for which, and the manner in which, personal information is processed) is regulated by eight Data Protection Principles. “Processing” is defined very broadly and encompasses more or less anything that might be done with personal information, including just holding it. The eight Data Protection Principles are:
(a) personal information shall be processed fairly and lawfully and, in particular,
shall not be processed unless:
• (subject to limited exemptions) the “fair processing code” information has been supplied;
• at least one of the conditions in Schedule 2 of the DPA 1998 is met; and
• in the case of personal information which is “sensitive personal data”, at least one of the conditions in Schedule 3 of the DPA 1998 is also met.
(b) personal information shall be obtained only for one or more specified and
84

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 11 17/10/12
lawful purposes, and shall not be further processed in any manner incompatible with that purpose or those purposes;
(c) personal information shall be adequate, relevant and not excessive in relation
to the purpose or purposes for which it is processed;
(d) personal information shall be accurate and, where necessary, kept up to date;
(e) personal information processed for any purpose or purposes shall not be kept longer than is necessary for that purpose or purposes;
(f) personal information shall be processed in accordance with the rights of
individuals under the DPA 1998;
(g) appropriate technical and organisational measures shall be taken against unauthorised or unlawful processing of personal information and against accidental loss or destruction of, or damage to, personal information; and
(h) personal information shall not be transferred to a country or territory outside
the European Economic Area unless that country or territory ensures an adequate level of protection for the rights and freedoms of individuals in relation to the processing of personal information.
4. Schedule 2 of the DPA 1998 is a list of conditions, at least one of which must be met
before personal information can be processed fairly and lawfully. 5. The DPA 1998 defines “sensitive personal data” as personal information which
relates to:
(a) the individual’s racial or ethnic origin; (b) the individual’s political opinions;
(c) the individual’s religious beliefs or other beliefs of a similar nature;
(d) whether the individual is a member of a trade union;
(e) the individual’s physical or mental health or condition;
(f) the individual’s sexual life;
(g) the commission or alleged commission by the individual of any offence; or
(h) any proceedings for any offence committed or alleged to have been
committed by the individual, the disposal of such proceedings or the sentence of any court in such proceedings.
6. Schedule 3 of the DPA 1998 provides an additional list of conditions for processing
sensitive personal data fairly and lawfully. Unless an exemption applies, the individual must give his or her explicit consent or one of the other conditions must be met. These conditions – importantly - contain a medical purposes condition allowing processing without consent.
At least one of the following conditions must be satisfied, in addition to at least one of the conditions for processing in Part 1 of this Appendix (which apply to the processing of all personal information), before processing of sensitive personal data can comply with the First Principle of the DPA 1998:-
1 The individual has given his explicit consent to the processing of the personal
information.
85

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 12 17/10/12
2 The processing is necessary for medical purposes (including the purposes of preventative medicine, medical diagnosis, medical research, the provision of care and treatment and the management of healthcare services) and is undertaken by:
(a) a health professional (as defined in section 69 of the DPA 1998); or (b) a person who owes a duty of confidentiality which is equivalent to that which
would arise if that person were a health professional. 4 The processing is necessary:
(a) in order to protect the vital interests of the individual or another person, in a
case where:
(i) consent cannot be given by or on behalf of the individual, or (ii) the data controller cannot reasonably be expected to obtain the
consent of the individual, or (b) in order to protect the vital interests of another person, in a case where
consent by or on behalf of the individual has been unreasonably withheld. The DPA 1998 principles are satisfied by: Principle 1 Lawful processing
As of 28th September 2012, the National Information Governance Board has granted
permission to Islington PCT to access PID data without patient consent in line with section 251 of the NHS Act 2006 and the Health Service (Control of Patient Information) Regulations 2002. This permission is valid until up to 31
st March 2013. If
at a later time a further extraction is required then another application will be required. Fair processing
The data are obtained during the patient registration and consultation process that takes place in General Practices. Patients are informed during the registration that the purposes for processing the data are assessment and delivery of patient care by the NHS. An updated patient information poster will also be provided to all GP practices who consent for use of the data in this way to inform patients about the uses of the data and the identity of the data controller.
Schedule 2 Consent - Whilst no explicit patient consent is obtained to support data sharing for this particular activity, patients can already request that their GP does not allow the use of their medical record for such purposes by using READ codes 9Nd9 (“Declined consent for Primary Care Trust to review patient record”), 93C1 (“Refused consent for upload to local shared electronic record”) and 93C3 (“Refused consent for upload to national shared electronic record”) in the GP IT system, so we will ensure that these records are not used in line with the wishes of these patients. As the data controllers, Islington GP practices respect the wishes of their patients by managing patient dissent on sharing data by entering the above READ codes on their systems as appropriate. In addition, As of 28
th September 2012, the National Information Governance Board
has granted permission to Islington PCT to access PID data without patient consent in line with section 251 of the NHS Act 2006 and the Health Service (Control of Patient Information) Regulations 2002. This permission is valid until up to 31
st March 2013. If
at a later time a further extraction is required then another application will be required. Schedule 3
Medical Purposes - The purposes of processing data for this activity are closely linked with the management of healthcare services as we aim to improve the quality of care provided in the locality. Therefore we believe that we can rely on a medical purpose ground for complying with Schedule 3 conditions as this activity is closely
86

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 13 17/10/12
linked with preventative medicine and the management of healthcare services. Consent - As of 28
th September 2012, the National Information Governance Board
has granted permission to Islington PCT to access PID data without patient consent in line with section 251 of the NHS Act 2006 and the Health Service (Control of Patient Information) Regulations 2002. This permission is valid until up to 31
st March 2013. If
at a later time a further extraction is required then another application will be required. Principle 2
Islington Primary Care Trust has notified the Information Commissioner’s Office that one of the purposes for which it will process data is “Health Administration and Services (provision and administration of patient care)”.
Principle 3
The adequacy, relevance and excessiveness of the data to be extracted has been considered with local clinicians in meetings of the Local Medical Committee where it has been agreed that the requested identifiers are the minimum data necessary for this activity.
Principle 4
General Practices collect the data from patients at point of registration using clinical IT systems that are accredited to the NHS Connecting for Health standards. In addition, staff employed by General Practices are trained sufficiently to ensure accurate recording and processing of the data. Where Islington Primary Care Trust is notified that it has received inaccurate personal data, Islington PCT will inform the General Practice from which the data were extracted.
Principle 5
The personal data will be retained for 30 days which is the maximum necessary period needed to undertake the data matching activity. It is essential to note that under the section 251 application approval conditions, PID data may only be used / retained until 31/03/2013. Islington PCT will fully comply with this condition.
Principle 6
Islington Primary Care Trust will co-operate with GPs and re-direct any requests from patients asking for copies of their information to the General Practices as the data controllers responsible to respond to any subject access requests or the exercise of other rights in the DPA 1998 given the nature and type of information and the degree of control that GPs exercise over the patient data.
Principle 7
The technical and organisation measures required to ensure the security of the data have been assessed via the Hosted Secondary Use Team/Project IG Toolkit Assessment (ECCRef:3-03(b)/2012). The results of this assessment have been reviewed by Connecting for Health who have accepted them as satisfactory and accordingly informed the decision of the NIGB to approve the section 251 application.
Principle 8 No data will be transferred outside the United Kingdom.
The Common Law Duty of Confidentiality 7. The NHS Code of Practice on Confidentiality provides helpful guidance on this
aspect. 8. All Personnel working in both the public and private sectors should understand that
they are subject to the common law duty of confidentiality, and must abide by this. The duty of confidentiality applies to information about an identifiable individual and not to aggregated data derived from such personal information or to personal information that has otherwise been effectively anonymised — i.e. it is not possible for anyone to link the information to a specific individual.
87

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 14 17/10/12
9. The duty of confidentiality means that confidential information should only be used for
purposes that the subject has been informed about and has consented to unless there is a statutory requirement to use information that has been provided in confidence, in this case the allowance of the DPA 1998 to permit such processing.
The Common Law Duty of Confidentiality is satisfied by:
As of 28th September 2012, the National Information Governance Board has granted
permission to Islington PCT to access PID data without patient consent in line with section 251 of the NHS Act 2006 and the Health Service (Control of Patient Information) Regulations 2002. This permission is valid until up to 31
st March 2013. If
at a later time a further extraction is required then another application will be required.
88

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 15 17/10/12
C.1- Description of information to be shared and procedure for
collection of the information.
1. LEVEL AND TYPE OF INFORMATION TO BE SHARED – PLEASE SPECIFY
1.1 Anonymised or Aggregated Data
The dataset created by linking GP extraction data to Hospital admissions data (SUS) using NHS Number. Full postcode would be converted to super output area, Mosaic type, and to give an indication of the types of housing in the postcode. After these linkage steps the PID data (i.e. NHS Number and full postcode) will be deleted from the dataset. Please include data items: See appendix 3 (anonymised dataset specification)
1.2 Pseudononymised Data
See 1.1 above None
1.3 Fully identifiable patient data
NHS Number and full postcode; note that this will be deleted once data has been linked to hospital admissions data. NHS Number and full postcode
2. PROCEDURE FOR COLLECTION OF INFORMATION
Islington PCT will use the data extraction facility that EMIS Ltd has available now that practices are streaming their data centrally. The data from practices currently running EMIS systems will extracted by EMIS Ltd and then transferred to Islington’s GP IT Team via a secure FTP download that will provided by EMIS. The data from the practice that is running the VISION system will be extracted by an external company that specialises in GP data extraction and the data saved on each practice network file area. The data will be transferred to Islington’s GP IT Team via a secure FTP download. When this method is not available then data will be transferred via e-mail exchange using two NHSMail accounts (sent from one at the practice to one used by the GP IT Team). The data will be stored on a stand-alone server in the offices of the GP IT department, and will only be accessible by the two members of the GP IT team listed in the Appendix. Once data linkage has been carried out the PID sections of the data will be deleted from both the server and any NHSMail account e-mails that were used to transfer the data. The newly anonymised dataset will only be made available to Islington PCT’s Public Health Intelligence team.
89

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 16 17/10/12
C.2 – Status of Parties under the DPA in This Data Sharing Agreement
• The status of General Practices under this data sharing agreement is ‘data controller’.
• The status of Islington PCT for data extracted into the local system under this data sharing agreement is “joint data controller”.
C.3 - Staff roles permitted to access the information in this Data
Sharing Agreement
1. Details of staff permitted to access data relevant to this Data Sharing Agreement.
NAME OF PARTY JOB TITLE OF STAFF CONTACT
Jacques Van der Merwe GP IT Information Analyst [email protected] Asim Khan GP IT Infrastructure manager [email protected]
C.4 - Details Of Contact Staff For Compliance, Advice And Arbitration Issues Concerning This Data Sharing Agreement.
Name of party Job title of staff Contact details
Sarah Dougan Head of Health Intelligence [email protected] Uche Osuagwu Public Health Data Manager [email protected]
C.5 - Procedure for transfer of data, updating of data, transfer in
emergencies and transfer to non signed up organisations.
N/A
C.6 - Audit trail, retention and subject access rights details for this
Data Sharing Agreement
• See appendix 4 – system level security policy (SLSP)
• Islington Primary Care Trust will co-operate with GPs and re-direct any requests from patients asking for copies of their information to the General Practices as the data controllers responsible to respond to any subject access requests or the exercise of other rights in the DPA 1998 given the nature and type of information and the degree of control that GPs exercise over the patient data.
90

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 17 17/10/12
C.7 - Agreed guidance for staff All staff involved must undertake the following training:
• Online e-learning information governance training � Introduction to Information Governance or Introduction to Information Governance for
General Practices. � Information Governance: The Refresher Module (to be completed the following year
once the above module has been completed)
• PID Information Governance training where PID data are to be accessed (provided by NHS North Central London).
C.8 - Parties to the agreement - addresses, contacts & signatures
Organisation
Address
Contact Details
Islington PCT, Public Health Intelligence Department
222 Upper Street, London N1 1XR
Tel: 020 7527 1258 or 1250
Signature
Name: Dr Sarah Dougan
Designation: Head of Health Intelligence
Date: 05/10/2012
C.9 Any other Information
• All parties retain the right to request any further information that may be reasonably
necessary to determine the validity and lawfulness of each information request to be produced before this agreement is signed.
• The Islington PCT Local Medical Committee will be invited to comment on this Agreement.
91

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 18 17/10/12
Appendix 1 - Pro-forma for EMIS Web Data Sharing Agreement
Terms and Conditions of the Data Sharing Agreement
A PID Extraction Data Sharing Agreement is the template that General Practices that provide primary medical services in north central London can use to record information sharing between General Practices and Islington PCT. The PID Extraction Data Sharing Agreement template asks the services to record:
1. Why is the information shared? 2. Who is sharing the information? 3. How is the information shared?
The PID Extraction Data Sharing Agreement is available to all other member organisations who may wish to alter a completed PID Extraction Data Sharing Agreement to meet there own local information sharing needs. A PID Extraction Data Sharing Agreement can be completed by any authorized employee of a General Practice in north central London or NHS North Central London.
1. Definitions
In this PID Extraction Data Sharing Agreement, the following terms have the following meanings:
“DPA 1998” the Data Protection Act 1998
“data controller” “data controller” as defined in the DPA 1998
“data processor” “data processor” as defined in the DPA 1998
“Consent” has the meaning described in Article 2 (h) of the EC Directive 95/46/EC
“personal information” “personal data” as defined in the DPA 1998
“Personnel”
the Parties’ employees, officers, elected members, directors, voluntary staff, consultants and other contractors and their sub-contractors (whether or not subject to legally binding contracts) and such contractors’ and their sub-contractors’ Personnel
“receiving Party” has the meaning in paragraph 4.3.1 below
“sensitive personal data”
“sensitive personal data” as defined in the DPA 1998
2. The subject of this PID EXTRACTION DATA SHARING AGREEMENT
The purpose of this PID Extraction Data Sharing Agreement is to identify:
. The organisation/parties/individual involved in the collection and sharing of information
The procedures for secure and confidential sharing of information between the organisations/parties
92

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 19 17/10/12
The business case why the organisations/Parties have agreed to share personal information;
. The method of collection of personal information by the organisation/party How this PID Extraction Data Sharing Agreement will be implemented,
monitored and reviewed.
3. Scope
3.1. Application and Indemnities
3.1.1. The Parties to this PID Extraction Data Sharing Agreement agree that as between themselves the provisions of the PID Extraction Data Sharing Agreement apply to and are deemed binding to that effect.
3.2. Relationship to other Data Sharing Agreement between the Parties:
If this PID Extraction Data Sharing Agreement applies to subject matter to which any other data sharing agreement or protocol applies, nothing in this PID Extraction Data Sharing Agreement shall prejudice such other Agreement, provided that if there shall be any conflict between this PID Extraction Data Sharing Agreement and such other Agreement it shall be resolved by agreement between the Parties and the parties to such other Agreement or in the absence of such agreement then at the request of any party to this PID Extraction Data Sharing Agreement or such other Agreement by decision of the NHS North Central London Information Governance Steering Group.
4.1 Internal compliance with this PID Extraction Data Sharing Agreement
Each Party shall instruct its Caldicott Guardian, data protection officer or equivalent for the time being to oversee compliance with this PID Extraction Data Sharing Agreement within such Party’s organisation. This PID Extraction Data Sharing Agreement will be retained within each service that has undertaken to access and process data via EMIS Web and/or other primary care clinical IT systems. Both parties undertake that any staff that may need to access PID under this PID Extraction Data Sharing Agreement also receive authorisation from the Caldicott Guardian of the organisation as appropriate.
4.2 The collection of personal information
4.2.1 Each Party agrees that:
(a) it is responsible for maintaining the personal information that it has collected on its own account, or jointly with another Party, in accordance with the DPA 1998;
(b) it will retain legal responsibility for correcting personal information where it is factually incorrect; and
(c) it will not amend the record of an opinion or judgement recorded by a health or social care professional, whether accurate or not, because the recorded opinion or judgement is essential for understanding the clinical decisions that were made and to audit the quality of care.
4.3 Sharing of personal information
4.3.1 Personal information may be disclosed to a receiving Party only if the personal information is necessary to perform a function or responsibility identified for such receiving Party to perform in the table in Part C.1 and (if there has been a request) the request for the information has been made in accordance with the procedures in appendix 1 of the Protocol.
93

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 20 17/10/12
UNLESS:
(a) the service user or some other person to whom such personal information relates has refused consent for the sharing of such personal information; or
(b) the personal information is sensitive personal data as defined by the
DPA 1998 and paragraph 4.5 below does not permit its disclosure.
4.3.2 The persons holding the job titles listed in the table in Part C.3, and only those persons, will be permitted access to personal information shared under this PID Extraction Data Sharing Agreement which is not sensitive personal data. Alterations from time to time to the above list shall be notified by the Parties to each other in accordance with paragraph 9.4 below.
4.3.3 Any requests for personal information sharing which is not permitted by this
PID Extraction Data Sharing Agreement should be considered under the terms of Part C.5 and the Protocol.
4.4 Sharing of sensitive personal data
4.4.1 Sensitive personal data may be disclosed to a receiving Party ONLY IF:
(a) the sensitive personal data is necessary to perform a function or responsibility identified for such receiving Party to perform in the table in PartC.1.
AND EITHER
(b) the service user or other person to whom such sensitive personal data relates has given his or her Explicit Consent for the sharing of such sensitive personal data;
OR
(c) some other lawful ground for sharing the sensitive personal data without Explicit Consent exists as described in the Protocol appendix 1 section 13.
4.4.2 Each Party’s Caldicott Guardian, data protection officer or equivalent shall:
(a) notify the other Parties’ Caldicott Guardians, data protection officers or equivalent of the roles of persons in such Party who will be permitted access to sensitive personal data held by such Party and any changes to such list from time to time; and
(b) maintain a list of the roles of persons in each of the Parties who will be permitted access to sensitive personal data held by the Parties,
and only those persons whose roles are identified on the list kept by the Parties’ Caldicott Guardians, data protection officers or equivalent shall have access to sensitive personal data. All persons whose roles are identified on such list will be provided with a copy of the list to enable them to be fully aware of the identity of persons with whom they are authorised to share information. The list may be qualified, and access to sensitive information further protected, by limiting access to information by some persons on the list in relation to specifically named service users.
4.4.3 The persons holding the job titles listed in the table in Part C.3, and only those persons, will be permitted access to sensitive personal data shared under this PID Extraction Data Sharing Agreement. Alterations from time to time to such list shall be notified by the Parties to each other in accordance with paragraph 9.4 below.
94

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 21 17/10/12
4.4.4 Any requests for sensitive personal data sharing which is not permitted by this PID Extraction Data Sharing Agreement should be considered under the terms of Part C.5 and the Protocol
4.5 Audit trail procedure
The Parties shall abide by the audit trail procedure as set out in Part C.6.
5 Service planning, commissioning, statutory returns and review
5.1 Procedure for sharing information for service planning, commissioning, statutory returns and review
5.1.1 The Parties recognise that service planning, commissioning, statutory returns
and review requires sharing of information about the incidence and nature of the contribution that they make to service users’ care.
5.1.2 [DELETE OR ADD PROCEDURE BELOW AS APPROPRIATE]
[Either]
The Parties will ensure that information has been anonymised before they make it available for service planning, commissioning, statutory returns and review purposes.
[Or] Sharing information for service planning, commissioning, statutory returns
and review purposes will strictly follow the procedure below, which has been approved by the Parties’ respective Caldicott Guardians, data protection officers or equivalent.
[In Part C.8 describe the procedure for information sharing for service planning and
review if you will not be anonymising the information]
6 Sharing Personal Information in Emergencies or with Organisations that are not Parties to the Protocol
See Part C.5 for procedures for transfer of data, updating of data and transfer of data in emergencies or transfer to non signed up organisations.
7 Agreed guidance for staff
The information contained in Part C.7 is agreed between the Parties as practice that must be complied with to help ensure consistency in the processes adopted in sharing personal information.
8 No third party rights
Save as provided in paragraph 3.1.2 above, each Party agrees that no term of this Data Sharing Agreement is enforceable under the Contracts (Rights of Third Parties) Act 1999 by a person who is not a Party to this Data Sharing Agreement.
9 General
9.1 In this PID Extraction Data Sharing Agreement:
(a) Please use clear language
(b) unless the context otherwise requires, references to paragraphs to this PID
Extraction Data Sharing Agreement.
95

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 22 17/10/12
9.2 No variation, waiver or modification of any of the terms of this PID Extraction Data Sharing Agreement shall be valid unless in writing and signed by or on behalf of the authorised representatives of the Parties.
9.3 Nothing in this PID Extraction Data Sharing Agreement shall constitute or be
deemed to constitute a legal partnership between any of the Parties or any Party the agent of any other Party and none of them shall have any authority to bind the others in any way by virtue of this PID Extraction Data Sharing Agreement, save as otherwise expressly provided in this PID Extraction Data Sharing Agreement.
9.4 All notices to be given under this PID Extraction Data Sharing Agreement will be in
writing and will be sent to the address and contact name for the receiving Party or any other address the relevant Party may designate by notice given in accordance with this paragraph 9.4 to all other Parties. Notices may be delivered personally, by first class pre-paid letter or by fax. Notices will be deemed to have been received:
(a) by hand delivery - at the time of delivery (b) by first class post - 48 hours after the date of posting
(c) by fax – immediately on transmission provided a confirmatory copy is sent by
first class pre-paid post or delivered by hand by the end of the next business day
96

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 23 17/10/12
Appendix 2 - Key staff involved in process Islington Public Health Intelligence: Dr. Sarah Dougan, Senior Public Health Manager: Health Intelligence & Needs Assessment Tel: 020 7527 1258 E-mail: [email protected] Islington PCT GP IT Team: Mr Jacques Van Der Merwe, GP IT Analyst Tel: 020 7527 1252 E-mail: [email protected] Mr Asim Khan, GP IT Infrastructure Manager Tel: 020 7527 1096 E-mail: [email protected]
97

Islington Public Health PID Extraction Data Sharing Agreement
Thanas Loli and Uche Osuagwu Page 24 17/10/12
Appendix 3 – fields of data to be extracted
- See extraction specification document attached in e-mail
Appendix 4 – System Level Security Protocol (SLSP)
- See document attached in e-mail
98

The information you give your GP will be held securely and treated as confidential by everyone at the surgery. However, information about you might sometimes be shared with other agencies such as NHS North Central London PCT Cluster. The NCL PCT Cluster consists of five of primary care trusts (PCTs) which are Barnet, Camden, Enfield, Haringey and Islington. Your name and address is generally not included in this information so it can’t be traced back to you. Sometimes your NHS number and postcode may also be shared with the PCT Cluster. The PCT Cluster uses this information to help plan health services and understand how health services in our area are being used. After the information has been used by the PCT Cluster for planning, identifiable information will be deleted and no information will be published or shared further. There may also be times when the information we give to the PCT Cluster does include your name and address. For example, the PCT Cluster may need to send you a letter to let to you know about a screening programme that will prevent illness. GPs at this surgery will only agree to give the PCT Cluster your name and address and other personal information if they think it will give you better healthcare. You are entitled to give your consent or refuse to allow information that includes your name, NHS number, address and/or postcode to be shared with the PCT Cluster. If you do not want to have your information shared, you should tell your GP or a member of staff. Whatever you choose, you can be sure that everyone who works here will treat your personal information as confidential and keep it secure. The surgery will always follow all legal requirements in relation to data protection. If you have any questions, concerns, or would like more information, please speak to your GP or a member of staff. Alternatively, you can speak to: NHS North Central London’s confidential Patient Advice and Liaison Service Team (PALS) Tel: 020 3317 3003 (9.00am - 5.00pm, Monday to Friday) Email: [email protected]
99

NIGBEthics and Confidentiality Committee
On behalf of the Secretary of State for Health
1
Dr Sarah DouganSenior Public Health ManagerPublic Health1st Floor222 Upper StreetLondonN1 1XR
28 September 2012
Dear Dr Dougan
ECC 3-03 (b)/2012 Extraction, linkage and anonymisation of Islington GP data to hospital admissions data
Thank you for your application for approval under the Health Service (Control of Patient Information) Regulations 2002 to process patient identifiable information without consent.Approved applications enable the data controller to provide specified information to the applicant for the purposes of the relevant activity, without being in breach of the common law duty of confidentiality. The role of the NIGB Ethics and Confidentiality Committee (ECC) is to review applications submitted under these Regulations and to provide advice to the Secretary of State for Health (SofS) on whether an application should be approved, and if so, any relevant conditions.This application was considered on 30 May 2012.
Secretary of State decision
Following consideration of the ECC advice, reproduced below, the Secretary of State has determined the following:
1. The application is approved, subject to the specific and standard conditions of support.
Context
This application from Islington Primary Care Trust set out details of the creation of an anonymised dataset linking Islington GP data, hospital admissions and demographics to enable population level analyses. Outputs from the analyses would be used to inform commissioning and strategicdecision-making by Health and Wellbeing Partners in Islington.
Confidential information requested
The application requested access to full postcode from GP data to enable linkage to lower super output areas for deprivation analysis. NHS Number was also requested to enable linkages between GP records and hospital admission records. The data would be anonymised once linkages had taken place.
5th
Floor, Skipton House
80 London Road
London
SE1 6LH
Tel: (020) 7004 1539
Email: [email protected]
100

NIGBEthics and Confidentiality Committee
On behalf of the Secretary of State for Health
2
ECC advice
The original advice by the ECC was set out in the letter dated 11 June 2012. A recommendation of provisional support had been provided, subject to requests for clarification and confirmation of satisfactory security arrangements.
The responses provided were welcomed and satisfied the queries. Members did reiterate that they could only recommend support for the PCT as the appropriate custodian of the data, and that the support would last only until 31 March 2013.
Specific conditions of support
1. Support is provided up to 31st
March 2013, at which point support expires.
2. If support is required from 01 April 2013, when the appropriate local authority or appropriate custodian is identified, as this will lead to changes in data controller arrangements, please note that an updated application, providing full details of these changes are submitted to the Committee for review. Please also note that a satisfactory IG Toolkit submission is required for those processing data under these Regulations, therefore this should be highlighted and planned for accordingly.
3. Any external release of data should be fully anonymised, and guidance should be sought and followed from the Health and Social Care Information Centre.
4. Satisfactory security arrangements via IG toolkit submission. The NIGB received confirmation from the IG Toolkit team on satisfactory toolkit arrangements on 26 September 2012. This condition is complete; noting that a satisfactory toolkit submission must be provided on an annual basis where support is in place.
IMPORTANT CHANGES
Annual review
Please note that the current administration of applications made under these Regulations by the NIGB Ethics and Confidentiality Committee is due to transfer to a new body by 01 April 2013, therefore please be advised that arrangements might have changed by the time the next annual review is due. Such arrangements will be communicated once confirmed.
Security review
Please note that due to a change in Department of Health policy, all bodies processing NHS data will be expected to provide up to date assurance of their security arrangements via the Information Governance Toolkit instead of system level security policy submission. Details on this change are available here http://www.nigb.nhs.uk/s251/security%20review. Please note that prior to your next annual review you will need to have provided a relevant IG Toolkit submission to the IG Toolkit Team. Any queries on this aspect should be directed to [email protected] so as to ensure there are no delays to any future continuing approval.
101

NIGBEthics and Confidentiality Committee
On behalf of the Secretary of State for Health
3
Please do not hesitate to contact me if you have any queries following this letter, I would be grateful if you could quote the above reference number in all future correspondence.
Yours sincerely
Natasha DunkleyNIGB Approvals Manager
102

NIGBEthics and Confidentiality Committee
On behalf of the Secretary of State for Health
4
Standard conditions
The approval provided by the Secretary of State for Health is subject to the following standard conditions.
The applicant will ensure that:
1. The specified patient identifiable information is only used for the purpose(s) set out in the application.
2. Confidentiality is preserved and there is no disclosure of information in aggregate or patient level form that may inferentially identify a person, nor will any attempt be made to identify individuals, households or organisations in the data.
3. Requirements of the Statistics and Registration Services Act 2007 are adhered to regarding publication when relevant.
4. All staff with access to patient identifiable information have contractual obligations of confidentiality, enforceable through disciplinary procedures.
5. All staff with access to patient identifiable information have received appropriate ongoing training to ensure they are aware of their responsibilities.
6. Activities are consistent with the Data Protection Act 1998.
7. Audit of data processing by a designated agent of the Secretary of State is facilitated and supported.
8. The wishes of patients who have withheld or withdrawn their consent are respected.
9. The NIGB Office is notified of any significant changes (purpose, data flows, security arrangements) to the application.
10. An annual report is provided no later than 12 months from the date of your final confirmation letter. Details are available on the NIGB website.
11. Any breaches of security around this particular flow of data should be reported to the NIGB within 10 working days, along with remedial actions taken/to be taken.
103

The professional voice of general practice in Islington Londonwide LMCs is the brand name of Londonwide Local Medical Committees Limited Registered and office address: Tavistock House North, Tavistock Square, London WC1H 9HX. T. 020 7387 2034/7418 F. 020 7383 7442 E. [email protected] www.lmc.org.uk Registered in England No. 6391298. Londonwide Local Medical Committees Limited is registered as a Company Limited by Guarantee Chief Executive: Dr Michelle Drage
National Information Governance Board Office Floor 5 Skipton House 80 London Road London SE1 6LH 13 March 2012 Dear Sir Islington LMC is writing in support of the section 251 application to the National Information Governance Board on Health and Social Care for the use of full postcode and NHS numbers on GP data by Islington’s Public Health team to enable analysis by deprivation and linkage to hospital admissions. The LMC considers that the temporary use of patient identifiable information to enable these linkages is in the wider public interest of Islington’s registered population. This is particularly given the large health inequalities and poor population health outcomes experienced by our patients. We hope that the analytical outputs from the data will enable the wider LMC and its constituent members to work in partnership to identify priority areas to further improve the quality of our care and in particular, ways to reduce hospital admissions and make best use of NHS resources. While the LMC supports this application, full consent for extraction of the patient identifiable data from each of the individual GP practices in Islington (the data controllers) will be sought prior to any extraction if this application is successful. The LMC can also confirm that Islington GPs provide information to patients about their rights to informed dissent in the use of their data for secondary purposes in practice waiting rooms. The wishes of patients who do not want their data to be shared with the PCT are respected by their GP who records this wish on their clinical IT system using standard coding. If you require further information then please contact me. Yours faithfully
Dr Robbie Bunt Chair Islington LMC
104

Draft and unconfirmed minutes of the NCL Cluster and LMC Chairs Group on 28 August 2012 at
1.30 pm in Room 6LM1 Stephenson House, 75 Hampstead Road, London NW1 2PL
Present: LMC Chairs
Dr Robbie Bunt Dr Claire Chalmers-Watson Dr Patrick Keating Dr Martin Lindsay Londonwide LMCs
Mrs Jane Betts Mr Greg Cairns Dr Paddy Glackin Dr Tony Grewal Ms Laura Quirke Miss Nicola Rice Observer: Dr Julie Sharman
NCL Cluster Mr Tony Hoolaghan (in the Chair items Dr Angela Lennox Ms Helen Pettersen (in the Chair items Mr David Thomas (item 4.3) Ms Denise Tyrrell Ms Anne Whateley
Item no.
Action Organisation/person
responsible 1.0 Apologies for absence
Apologies were received from Dr Martin Harris, Dr Henrietta Hughes and Ms Caroline Taylor.
2.0 Declarations of conflicts of interest There were no new declarations of interest.
3.0 Minutes and matters arising:
3.1 Minutes of NCL Chairs and Cluster Group meeting on 26 June 2012 The minutes of the meeting on 26 June 2012 were agreed as a correct record.
3.2 Matters arising: There were no matters arising.
4.0 Strategic issues:
4.1
4.1.1
Report from Chief Executive Financial report Ms Pettersen advised that Camden and Islington were in a good financial position although there was a risk that they would not manage to spend
105

4.1.2
all the investment monies. With regard to Barnet, Enfield and Haringey, Ms Pettersen noted that early figures suggested that each would have an overspend of £7m to £10m. This was being looked into but Ms Pettersen acknowledged that their QIPP plans had been ambitious. In addition to this there were overspends in the acute providers and the CCGs and commissioning team were looking to see what contractual levers there were to bring them back into control. Transition Ms Pettersen referred to the David Nicholson letter advising of the flip over of responsibility to the new organisations on 1 October 2012 which meant that it would be the CCGs and CSUs which would plan spend for the next year. It was hoped that senior members would be in post by that date so the new structure would be up and running from then. Ms Pettersen advised that the NHS Commissioning Board had not yet released its structure although it was expected in the next few weeks but noted that most of the CCGs in North Central London had been out to engagement regarding their structures. Ms Pettersen advised that the majority of staff would be going to the CSU. Interim appointments had been made to the top level posts but there would be another recruitment process and it was hoped that senior staff appointments would be made by the end of September 2012. In the meantime the legacy handover and closure of the five PCTs needed to take place which would mean that from October to March 2013 two systems would have to be run. Ms Pettersen advised that much time was being spent on preparing the formal handover documentation which had to be submitted to the NHS Commissioning Board. Dr Grewal asked what the position was with regard to the contract or SLAs between the CCGs and the CSU. Ms Pettersen advised that discussions were ongoing although she understood that national guidance around a template SLA was due to be published. Ms Pettersen further noted that the CCGs were not all buying all the services the CSU would offer so there would be room for variation in the SLAs.
4.2 NCL Cluster Primary Care Strategy: Ms Tyrrell reported that all the borough primary care strategy implementation plans had now been approved and the boroughs were making progress with implementation. Ms Tyrrell explained that the focus on this year was on access, long term conditions and the frail and elderly. Clinical leads were being recruited as were support staff which would be based around the networks or collaboratives including, as in the case of Barnet, Project Managers. Ms Tyrrell reported that some additional funding had been made available opportunistically for practice nurse training and to date 20 places for attendance at courses on diabetes and long term conditions had been approved. Ms Tyrrell advised that the funding was a one-off but the Cluster would try to make it long standing. Dr Bunt asked how this opportunity had been advertised to practices as
106

he had not been aware of it and wanted to be assured that the access to training was equitable. MsTyrrell confirmed that it had been advertised through the practice nurse networks although acknowledged that the process needed to be reviewed for the future and undertook to provide a report of the process at the next meeting. Dr Grewal suggested that in the future such information could be passed to the LMC office for inclusion in the newsletters which were sent to every practice. Dr Bunt asked what was what the future of the NCL Primary Care Strategy now that Dr Russell had left and what were the must dos particularly around networks and super LESs. He noted that he was hearing different things happening in different boroughs and asked where the NCL strategy would sit given that the Cluster would cease to exist in six months. Mr Hoolaghan expressed the view that a lot of the strategy was being led and implemented by boroughs via the implementation plans but the aspects of the strategy being led by the Cluster were IT, premises and performance around contractual and individual issues. He explained that some funding had been taken from the strategy money to fund performance and contract management. In response to Dr Bunt’s specific question as to the role of the NCL Cluster in terms of the primary care strategy Ms Tyrrell advised that each of the boroughs was working within the overall framework of the NCL primary care strategy and the 9 domains it set out. Ms Tyrrell noted that each borough had a different focus and that the Cluster was taking a supportive and developmental role. Ms Tyrrell further advised that the role of the Cluster via the Project Board was to look at the boroughs’ implementation plans to ensure that the £47m which had been released for the strategy was spent and retained. Mr Hoolaghan advised that the NHS CB would have a department which would ensure CCGs fulfilled their responsibilities and would look at how they were developing primary care. In addition to this the NHS CB would be doing the contractual and performance work. Dr Lennox shared her vision of networks as being practices working together in a locality which shared the same or similar profiles in relation to theregistered population. Dr Lennox considered that it would take time for individual practices to grow into more general localities but explained that bringing in GPs as clinical leads would help to achieve a locality feel. Dr Lennox expressed the view that an unacceptable variation in the delivery of services such as poor access and no call and recall systems for patients with long term conditions would not be sustained and she noted that there was a huge variation on practice outcomes. Dr Lennox considered that it was about GPs understanding what was good practice and in a locality beginning to question why one practice might have a high level of prescribing antibiotics for example and was of the view that having networks would enable peer to peer and clinician to clinician discussions to take place. Dr Lennox emphasised that the growth of localities would be organic and explained that it had taken 18 months for practices in her locality in Leicester to see the benefits of working in this way. Dr Lennox advised
DT
107

that Dr James Kingsland had been invited to attend a forthcoming NCL workshop on transforming primary care through collaborative working which would tease out the practical consequences around collaborative working and to learn from what was happening elsewhere. Dr Chalmers-Watson asked for clarity around the relationship between the boroughs and the Cluster in relationship to the 7 domains of the strategy which sat at borough level as there was a perception that the boroughs had to do what they were advised by the Cluster. Ms Tyrrell advised that each borough had a steering group in relation to primary care strategy implementation and that the borough implementation plans had to be approved by the NCL Project Board so that the funding could be released. Ms Tyrrell considered that the NCL Cluster was working closely with the boroughs so there should be no surprises by the time issues were discussed at the Project Board. Mr Hoolaghan advised that CCGs were embryonic and the approach which NCL Cluster was taking was to try and support and enable them to take on the work. He reminded the group that post March 2013, CCGs would be performance managed by the NHSCB and although the Cluster was trying to encourage and support CCGS to undertake the necessary work there had to be checks and balances in the meantime. He confirmed that the Cluster said the same things to all five boroughs but they did not always hear the same message. He asked that if there were examples of people suggesting that the NCL Cluster had indicated that something had to be done in a particular with regard to the implementation of the primary care strategy that details be forwarded to Ms Tyrrell to take up. Dr Grewal noted that he had not seen one mechanism whereby any of the £47m would reach practice accounts as the money was being used to develop or impose networks and to appoint clinical leads. Dr Grewal reminded members that even though the borough CCGs might be leading on their own implementation plans they were still subcommittees of the PCT Board until the end of April 2012. Mr Hoolaghan responded to advise that everything which was being done currently was affected by the transition but it was important not to lose the benefits of the funding for the primary care strategy.
4.3
4.3.1
GP IT strategy Support for GP IT and Registration Authority Mr Thomas reported that the IT support for the five boroughs became an NCL wide service in March 2012 and explained that this helped to standardise services across the five boroughs and was a more effective use of resources. A survey was being conducted among practices regarding the services offered and the response had been favourable so far. Mr Thomas advised that the NCNE CSU prospectus set out a proposal for a managed service and it had been sent to the CCGs as funding for primary care IT would sit with them. In response to Dr Bunt’s concerns about the document containing insufficient details Mr Thomas advised that the document had been kept light purposefully as the individual detailed discussions would take place with the CCGs.
108

4.3.2
Dr Grewal noted that GP IT was meant to be cost neutral and queried why CCGs were taking control of primary care IT costs as they were supposed to be focusing on commissioning and secondary care. He considered that funding for IT should sit with the NHS CB. Ms Pettersen noted that this was a national decision. EMIS web implementation Mr Thomas noted that EMIS web was a key enabler of the primary care strategy and acknowledged that there had been more of a focus on IT and the technical side of things rather than on other areas such as data sharing and confidentiality issues. He explained that 24 practices were now on a web enabled system with a further 150 practices having expressed an interest and it was expected that at least 80 to 100 of those would go live this financial year. He advised that people from EMIS had been seconded to work in the Cluster and that a Programme Manager and Project Manager had been appointed. He further advised that 10 days training per practice had been identified. He noted that a text messaging service which was already embedded in Camden and Islington practices was in the process of being rolled out in Barnet, Enfield and Haringey. He explained that this would be fully funded for this year and the next two. He advised that the IT department was looking to roll out Docman as another management solution but advised that lessons were currently being learned from the roll out in Barnet. He acknowledged that EMIS had promised many things last year which had not yet materialised such as increased bandwidth for N3, and practices having experienced problems with a number of applications running simultaneously, but he explained that the IT department was looking into these. Dr Lindsay advised that he had major concerns from both a GP indemnity point of view and from a patient perspective. As data controllers GPs would be held responsible if something went wrong even if it was beyond their control and the considered that EMIS should be held accountable and should indemnify GPs against this. Similarly he considered that if hospitals had access to this information and a third party accessed and misused information GPs should not be held responsible and so hospitals should also indemnify GPs. With regard to the issues from a patient perspective Dr Lindsay considered that EMIS web could be seen as the NHS Spine being implemented by the back door and was of the view that there should not be an automatic opt out but that patients should have to opt in to ensure that they were aware about it. It was noted that a meeting was to take place immediately after this Cluster meeting to discuss the concerns further to be attended by Mr Thomas, Dr Lennox, Mr Cairns and Dr Lindsay.
109

4.4 Procurement of GP Practices Mr Hoolaghan advised that some lessons had been learned from the closure of the 142 Camden Road practice which had been factored into the forthcoming procurement processes. He confirmed that the Cluster had requested an LMC representative for the evaluation panel. Mr Cairns reported that he and Mr Hoolaghan had discussed the lessons learned from the 142 Camden Road practice closure and that assurances had been given that future procurement processes would focus on quality rather than price, that the ownership of the contract could not be transferred without a discussion with the commissioner and that any premises leases would last the duration of the contract. Mr Cairns further requested that people already working in the surgeries which were up for tender should have an opportunity to bid and asked how the doctors working in Brunswick Medical Practice and Kings Cross Road would be given an opportunity to submit a bid. He also asked for an assurance that the contracts for these practices would be monitored in a more structured way and that due process would be followed if the contract was not followed such as imposing sanctions for none delivery of contract. He further asked what process would be in place to work out whether the prices quoted in the bids were actually workable. Finally he requested that the LMC representatives be fully involved in all aspects of the procurement process. Mr Hoolaghan responded that the process would be heavily weighted to quality and that a legal clause would be included in the contract to prevent it being transferred to another provider without discussion with the commissioner. He further confirmed that there would be no problems in relation to the length of the leases with the premises of the practices out to procurement. He also advised that APMS contracts were monitored robustly. With regard to the Brunswick Medical Practice and Kings Cross Road Practice he advised that the GPs who worked there who had expressed an interest had missed the deadline for submission. He had advised them that they should have scanned the Supply2Health website and had suggested that they might wish to speak to other practices which might be interested in submitting a bid with a view to seeing if they could join with them. He explained that procurement documentation could not be made available other than by the Supply2hHealth website. Dr Lindsay advised that GPs were not used to looking at websites to scan for procurements and asked whether the GPs currently employed in Brunswick Medical Centre and Kings Cross Road were told that the procurement would be coming up and where to look for such information. Dr Grewal agreed that for GPs not to know where to look was a missed opportunity and it was agreed that it would be more appropriate for the LMC office to scan the relevant website to look for procurements which could then be disseminated to practices. It was also agreed that it would be helpful if LLMCs produced general guidance on how to do procurements. Dr Chalmers-Watson noted that there had been a lack of continuity in
110

clinicians over the past 5 years in the three practices in Camden and asked how this would be dealt with in the new procurement specification. Mr Hoolaghan advised that it would be the responsibility of the bidders to indicate what services would be provided and how they would provide those under the quality section. In addition the contract would include KPIs about continuity of care. Dr Chalmers-Watson considered that continuity of care was very important but the KPI might only amount to 1% or 2% of the contract. Mr Hoolaghan confirmed that the Cluster would not want a service populated by lots of locums and one way in which this would be assessed would be by way of the presentation topic when bidders would be asked to explain how they would provide continuity.
4.5 Letter to practices regarding day of industrial action Dr Grewal queried how the Cluster intended to take the matter further following the letters which they had sent to those practices which had taken industrial action. Mr Hoolaghan confirmed that the Cluster had received feedback from all practices and a discussion was due to take place at the London Directors of Primary Care meeting the next day about how this should be taken forward. Mr Hoolaghan confirmed that he would feed back the outcome of that meeting to the LMC office.
TH
5.0 Operational issues:
5.1 Primary Care QIPP:
5.1.1 PMS reviews Mr Hoolaghan reported that the group which had representation from each of the five LMCs had been meeting on a regular basis. He advised that the financial figures had been pulled together which he considered to be fairly robust and that there would now be a need to look to see what additional services PMS practices could provide in addition to essential and additional services. He confirmed that the group was currently considering a menu of services which PMS practices could deliver. He advised that specifications would be developed jointly with CCGs, LMCs and public health although there would be some element of local flexibility around student practices for example. He confirmed that borough based workshops would be held for PMS practices to discuss the review and these would take place in September/October. In response to a query from Dr Grewal Mr Hoolaghan confirmed that there was no planned QIPP saving in relation to PMS.
5.1.2 List maintenance Dr Grewal tabled a list of figures which he had produced showing the discrepancies between the census figures for 2011 and the registered patient population for the five boroughs. He considered this threw into
111

question the list maintenance exercise which was currently being undertaken and suggested that attention should now focus instead on encouraging people to register. Mr Hoolaghan advised that the primary care strategy did set out an aim to have all eligible patients registered and reminded members that the Operating Framework required that list maintenance exercises be undertaken by March 2013 so the Cluster could not stop those currently underway. He noted that this would become the responsibility of the NHS Commissioning Board post April 2013. Mr Hoolaghan advised that he would raise this issue at the meeting of the London Primary Care Directors the following day and Ms Pettersen advised that a decision to stop list maintenance would need to be taken on a pan London basis. In response to Dr Bunt’s query about what policies were being put in place to improve patient registration figures Mr Hoolaghan advised that there had been some discussion about doing a social marketing exercise although nothing had been done to date. Ms Pettersen suggested that this was something which needed to be done by the CCGs and advised that she would take this back to the Primary Care Strategy Board.
HP/TH
5.2 Patient Choice Pilot LES Dr Grewal asked whether, if no practices signed up to the LES, the Cluster would commission the services from an out of hours provider at the same prices as those set out in the specification. Dr Grewal did not consider that the prices offered would cover the average cost of practices of seeing such patients. Mr Hoolaghan advised that the prices in the specification were taken from the DH guidance. He noted that the Cluster would like to circulate the LES so that it could take a view depending upon response received. It was agreed that he would give an update at the next meeting regarding the number of practices who had signed up to the LES.
TH
5.3 NHS 111 update Dr Grewal asked why the Cluster had not taken up the option of delaying the implementation of 111 for six months as announced by the Secretary of State. He also expressed concern about the proposals around Coordinate My Care as this was not a clinical service but a commercial data sharing service and he was aware of concerns which had arisen in other areas where this had been used. He advised that in order for data to be accessed from this system all staff in the practice would be required to undergo training and the training would not be tailored to individuals according to the level of access. He presumed that CMC would be providing the training and it was not clear how much the training would cost. In addition he noted that it was not clear who set up the contract and how much it was worth. Ms Pettersen undertook to ask her colleagues working on 111 to pass on these concerns.
HP
112

5.4 Premises:
5.4.1 Premises survey Ms Tyrrell confirmed that the premises surveys would be conducted by the Oakleaf Group and it was hoped that they would be completed by the end of November 2012. Ms Tyrell noted that a meeting would be taking place on 26 September to consider the Improvement Grant bids. Dr Grewal asked to see the tool which Oakleaf would be using and the criteria which the improvement grant panel would be using to assess the bids. Mr Hoolaghan advised that both these had already been sent to Dr Grewal but undertook to forward further copies to him. Mrs Betts queried why the improvement grant panel was taking place before the survey had been finished. Mr Hoolaghan acknowledged that this was not ideal but noted that if the improvement grant money was not spent it would be lost. He advised that the Cluster had taken a pragmatic decision to launch the process in the absence of having all the audit information although some initial information would be available. In response to a query from Mrs Betts as to whether there would be targeting around the predicated outcomes of the survey Mr Hoolaghan advised that the Cluster would be using information which practices had already given and which the Cluster already held. He noted that Mrs Betts would be on the panel representing the LMCs and confirmed that the bids would be assessed in a fair and transparent way.
TH
5.4.2 PCT owned premises It was agreed that Ms Betts would liaise with Mr Hill outside the meeting to discuss leases in relation to PCT owned premises.
JB
6.0 Date of next meeting: 30 October 2012
7.0 Any other business:
7.1 PALS conciliation Dr Bunt advised that a constituent had contacted him in relation to a complaint his practice had received but that when he had contacted PALS for a conciliator he was told that due to cuts in services conciliators could not be provided any more. Dr Bunt explained that he had contacted LINkS for advice and had been advised that para 5.2 of the NCL PALS complaints policy stated that ‘ a Lay Conciliator/Mediator can be provided in exceptional circumstances to support practices …’and he queried what was meant by ‘exceptional circumstances’. Dr Bunt further noted that paragraph 3.1.8 of the ‘Making Experiences Count: Complaints a guide for general practice’, which was produced by the London Primary Care Complaints Consortium in March 2009, indicated that ‘practices or complainants can approach the PCT and ask for help of a conciliator at any stage of the complaint’.
113

It was agreed that Mr Hoolaghan would contact colleagues who dealt with complaints to clarify the situation and would report the outcome to the LMC office.
TH
7.2 CQC registration Ms Whateley advised that the Cluster had been sent a list of practices showing who had registered with the CQC and asked whether the LMC had sent out reminders as the Cluster was considering contacting those practices which had not yet registered. Dr Grewal confirmed that LLMCs had sent emails to practices advising them about the registration requirements.
7.3 Staff changes Ms Pettersen noted that it was likely that a number of staff at the Cluster would have moved jobs before the next scheduled meeting and reported that Mr Hoolaghan had been appointed as the CSU Commissioning Support Director for Camden and Islington, and Ms Tyrrell the CSU Commissioning Support Director for Haringey. Ms Pettersen assured the LMC Chairs that a comprehensive handover would take place. Dr Grewal congratulated them on their new roles and noted that the LMC Chairs found this meeting with the Cluster useful and asked that Ms Pettersen feed this back to those who would be attending this meeting in the future.
114

Events Calendar
October 2012
Tuesday, 25 Mastering the GP Patient Survey and Improving your Results
Contact: [email protected]
GPs and practice staff
November 2012
Wednesday, 7 Preparing for Partnership: Business Skills for GPs Seminar
Contact: [email protected]
GPs
Wednesday, 14 Alternatives to saying “No” to Patients and Promoting Effective Behaviour Change
Workshop 1 – Alternatives to saying “No” to patients Workshop 2 – Promoting Effective Behaviour Change
Contact: [email protected]
GPs and practice staff
Thursday, 15 Practice Manager Seminar: Finance
Contact: [email protected]
PMs
Thursday, 22 Practice Nurse Event workshop on Cognitive Behaviour Therapy (CBT)
Contact: [email protected]
GPNs
Wednesday, 28 Medical records in primary care
Contact: [email protected]
GPs and GPNs
December 2012
Wednesday, 5 Complaints procedure in general practice seminar
Contact: [email protected]
GPs and practice staff
All events take place in a Central London venue and charge a delegate fee. Full
details are available on the LMC website (www.lmc.org.uk)
115