
Ischemic heart disease Jana Plevkova MD, PhD Associate professor Department of Patophysiology JLF...
61
Ischemic heart disease Jana Plevkova MD, PhD Associate professor Department of Patophysiology JLF UK
-
Upload
anabel-campbell -
Category
Documents
-
view
219 -
download
1
Transcript of Ischemic heart disease Jana Plevkova MD, PhD Associate professor Department of Patophysiology JLF...

Ischemic heart disease Jana Plevkova MD, PhD
Associate professor
Department of Patophysiology
JLF UK

Ischemic heart disease
Acute or chronic disorder of myocardial functions developed on the basis
of reduced coronary blood flow due to damage of the coronary vessels
mostly due to coronary atherosclerosis
So this mean that inbalance between oxygen needs and oxygen supply that was discussed earlier is caused by pathological process in the coronary
arteries.
Clinical stand point – classification
Chronic formsStabile angina pectoris
Inversive (Prinzmetal) angina pectoris
IHD with arrhythmias
Status post MI
Clinically asymptomatic – silent ischemia
Acute formsNon-stabile angina pectoris
Myocardial infarction
Sudden cardiac death
Intermediary coronary syndrome

The heart works permanently and this work requires a lot of energy
The heart is aerobic organ – this means that energy is provided by metabolizing of substrates and the oxygen is necessary for this process
For optimal functions of the heart there should be a precise balance between oxygen supply and the oxygen requirement in the heart cells

Blood flow through the coronary arteriesoxygen supply
Oxygen requirement
Perfusion pressure
Vessel resistance
Heart rate Tension in theventricular wall
Power of contraction
Intraventricular pressure
Ventricularvolume

Coronary circulation
Provides oxygen and substrate supply- Epicardial arteries- Intramyocardial branches- Capillaries
Blood flow through the coronary arteries is determined by: perfusion pressure extra vascular compression of the myocardium heart rate (diastolic period) coronary auto regulation endothelial functions neurohumoral regulation functional condition of the heart and it's metabolic
requirements


Regulation of coronary circulation
- auto regulation, metabolic, hormonal, neural regulation
Coronary perfusion is relatively constant in the ranges of the pressure in aorta between 40 – 160 mmHg – auto regulation
The main regulating factor is metabolic rate of the myocardial cells of the metabolic rate leads to coronary vasodilatation, via factors like
adenosine, CO2, H+, K+, NO released from endothelial cells due to accumulation of metabolic products and sudden vasodilatation
neural regulation is less important

Extravascular pressure – compression of the vessels by the myocardium during systolic phase could result into complete block of the blood flow in the left ventricle and significant reduction of the blood flow in the right ventricle
Intramyocardial branches are perffused only during diastolic phase
Increasing of the heart rate facilitates metabolic requirements of the heart cells, but on the other hand leads to reduction of the diastolic phase – therefore limits the coronary blood flow


diastolic diastolic phasephase
Systolic Systolic phasephase

Myocardial ischemia
Myocardial ischemia is a pathological process developed in condition of reduced coronary blood flow, which does not satisfy energetic requirements of the myocardial cells. Disturbed balance leads to activation of biochemical processes disturbing ionic homeostasis of the heart. Hearse, 1994).
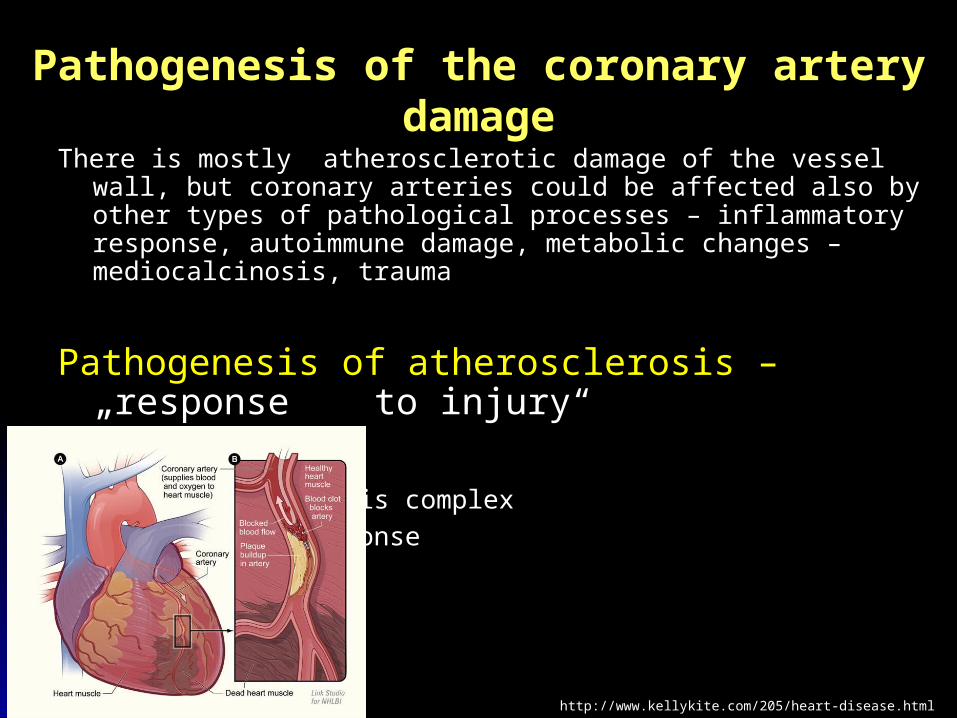
Pathogenesis of the coronary artery damage
There is mostly atherosclerotic damage of the vessel wall, but coronary arteries could be affected also by other types of pathological processes – inflammatory response, autoimmune damage, metabolic changes – mediocalcinosis, trauma
Pathogenesis of atherosclerosis –„response to injury“
new aspect – ATS is complex
inflammatory response
http://www.kellykite.com/205/heart-disease.htmlhttp://www.kellykite.com/205/heart-disease.html

Endothelium – is not only a physical barrier between the blood stream and the vessel wall
- high metabolic activity, contribution to vessel reactivity, regulation of thrombogenesis, influence on the circulating cells properties
- endothelial surface is about 500 - 1000 m2 thus providing contact between the circulating cells and the vessel wall endothelium is the largest endcrine organ /1500g/
- metabolic and secretoric systems influence mainly vessel tone and therefore blood flow and blood pressure
- endothelial cells naturally prefer tendency to vasodilatation

Endothelial vasodilatators- production of NO – from L arginine by NO synthasis, created molecule
diffuses into the smooth muscles below the endothelium and activates guanylatcyclase thereby increasing production of cGMP - this leads to relaxation of smooth muscle cells resulting into vasodilatation
- production of NO is responsible for permanently maintained vasodilatation in the arterial system
- production of NO is stimulated by shear stress, molecules released from thrombocytes (ATP, ADP, serotonine), sudden distension of the vessel lumen – dilatation depending on the blood flow
- NO is dominant vasodilating substance in basal condition, but endothelium could also release other molecules PGI2 (prostacycline) PGE2, PGD2 able to enlarge vessel lumen

Endothelial vasconstrictors
Endothelines, thromboxan A2, nonstabile endoperoxides and molecules of RAA system
Endothelines (1, 2, 3) – group of peptides with 21 AMA, originates from molecule of proendotheline, which is fragmented by enzymes and converted into active molecules
ETA a ETB receptors – vasoconstrictive response, long lasting increased concentration of the endothelines provides also proliferating effect on the smooth muscles in the media

ETB receptors – after binding of endothelin1 molecule production of NO a prostacycline – backward regulation - decrease of vasoconstrictive effect of endothelines
Production of endothelines is stimulated by: hypoxia, thrombin, cytokines, ATII, epinephrine
Local system of RAA – endothelial cells in the whole body are able to produce molecules of RAA system, but its role is not entirely understood
Adhesion of the cellsIntact endothelium does not allow adhesion of circulating cells,
but allows rolling of some cells on the endothelial surfaceCAM – expression of cell adhesion molecules on the endothelial
surface and on the surface of circulating cells regulates their rolling, then adhesion onto surface and transmigration through the intima, this process is facilitated during inflammation of endothelial dysfunction

Pathophysiologic classificatin of vascular injury leading to atherosclerosis
Type I injury: functional alteration of endothelial cells without morphologic changes
Type II injury: endothelial denudation and intimal damage with intact internal elastic lamina
Type III injury: endothelial denudation with the damage of both intima and media

Accumulation of lipids and monocytes adhesion Thrombosis
Smooth muscle proliferation
Type I injury mierna not present present
Type II injury ? minimal fibromuscular layer on the plaque surface
Type III injury ? moderate strong organization of the thrombus
I. degree
II. degree
III. degree
Endotel
Intima
Media
Adventitia

A new insight into atherosclerosis
Chronic inflammatory process with participation of lipoproteins, macrophages, T – lymphocytes, endothelial cells and smooth muscle cells. The consequence of this complex process is formation of lesions inside the vessel wall – atherosclerotic plaques
The plaques consist of the core - containing pulpy cellular debris and fibromuscular cap
Although ATS is generalized problem in all arteries of the human body, clinical manifestation of the ATS is usually restricted to cerebral and coronary circulation and to circulation of the lower extremities

The basic point of ATS process is damage of the endothelium
Endothelium could by damaged by:- sudden changes of the blood flow direction (in the sites of the vessel
branching)- oxidative stress (overproduction of oxygen reactive species) concentration of pro inflammatory cytokines- some infectious agents and their products level of homocysteine (is toxic for the endothelium)- Increased blood pressure- Long lasting hyperglycaemia – diabetes mellitus

Endothelial injury could result into endothelial dysfunction and its consequences
endothelial permeability for blood plasma proteins and lipoproteins Adhesion of monocytes and their transformation into macrophages Shifting of the balance in the vessel tone regulation into proconstrictive
preparedness
Particles of the LDL cholesterol are now able to enter the vessel wall
LOX 1 receptors – high afinity receptors for oxidative forms of the lipoproteins which are responsible for disposing of the lipids penetrated into the vessel wall

Lipids penetrating the vessel wall (lipids lesions) are phagocyted by macrophages (via LOX1 receptors) they are after lipid ingestion converted into the foam cells
Endothelial cells, thrombocytes and activated macrophages produce growth factors responsible for proliferation and migration of smooth muscle cells towards the lumen of the vessel.
This process is responsible for creation of fibromuscular layer on the surface of the plaque. This cap is like an envelope of the plaque, above the accumulated lipids.
Stable – fibromuscular plaques – strong fibromuscular cap, less lipids plaque is growing progressively disturbing the hemodynamic properties of the vessel, complications are not frequent
Nonstable – lipid plaques - thin fibromuscular cap, plenty of lipids, they are predisposed to complications

Progression of ATS process
Early lesions in the wall + risk factors of ATS growing of the ATS plaques
genetic participation level of LDL a VLDL level of HDL lipoprotein ahypertensiondiabetes mellitusmen gender level of homocysteine level of coagulation factorsobesityfamily history
environmental factors
smoking
lack of physical exercise
faty diet
stress

Intravascular ultrasound in case of ATS plaquesIntravascular ultrasound in case of ATS plaques


growing of the plaques clinical manifestation
slow progression in the growing process of the plaque ~ chronic forms of IHD
Growing of the plaque is caused by increase of the lipid content inside the core and by the fibromuscular proliferation
The surface of the plaque is usually covered by endothelium with impaired functions, which allows creation of small
thrombi on the endothelial surface
These small thrombi are then organized by conversion into the fibroid structure.
Accumulation of such kind of material on the plaque surface leads to its enlargement
Creation of small thrombi is usually asymptomatic

Progression in the plaque growing
http://www.nature.com/nm/journal/v17/n11/full/nm.2538.htmlhttp://www.nature.com/nm/journal/v17/n11/full/nm.2538.html

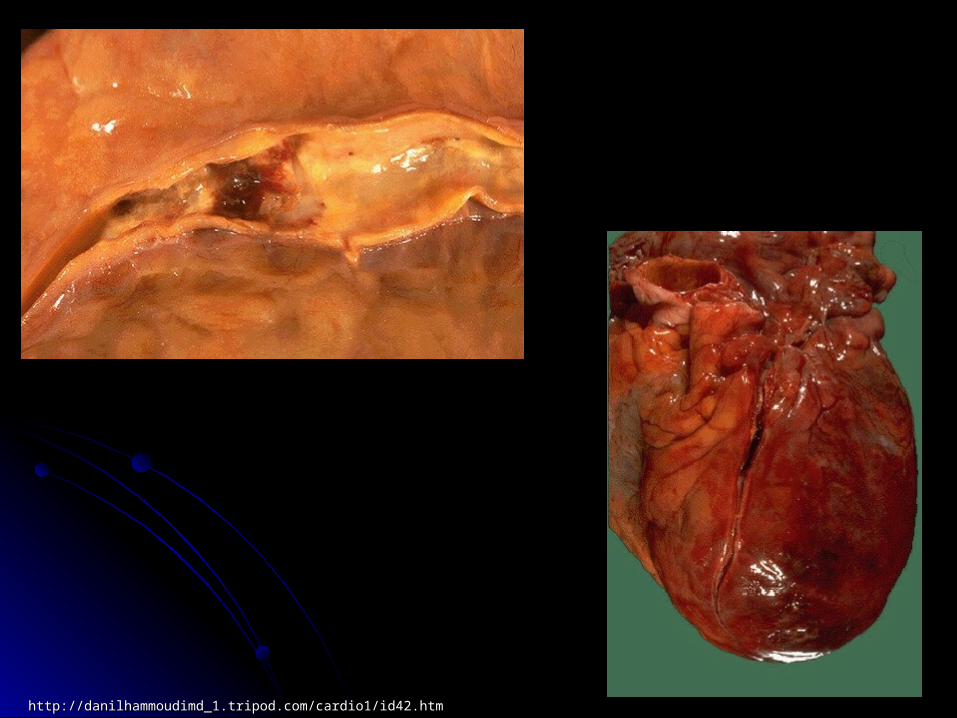
Sudden enlargement of the plaque – acute coronary syndromes – mainly due to complications of nonstable plaques
- Disruption of the plaque surface uncovering of underlying collagen collagen stimulates creation of the thrombus
- Fragmentation of the thrombus with subsequent embolization of smaller particles forward into the periphery of coronary circulation
- Fissuring or disruption of the plaque with subsequent disjunction of some part of the plaque toward the bloodstream
- Disruption with bleeding inside the plaque - Coronary spasm in the arteries with endothelial dysfunction

http://danilhammoudimd_1.tripod.com/cardio1/id42.htmhttp://danilhammoudimd_1.tripod.com/cardio1/id42.htm
http://danilhammoudimd_1.tripod.com/cardio1/id42.htmhttp://danilhammoudimd_1.tripod.com/cardio1/id42.htm

Small parietal thrombi, as well as, healing of the fissuring of the plaque surface – this means fibroproduction, could contribute to development of more serious ATS changes.
Thrombogenesis and organization of the thrombi are simultaneous processes
Fibrotization of the parietal thrombus is regulated by molecules released mainly from thrombocytes -
PGF, TGF - these molecules are
growth factors supporting
fibroproduction
http://www.nature.com/nri/journal/v6/n7/http://www.nature.com/nri/journal/v6/n7/fig_tab/nri1882_F1.html3fig_tab/nri1882_F1.html3

Mechanisms leading to ischemia
stabile fibromuscular plaques in the CA – usually large plaques, poor of lipids, without tendency to complications
presence of the plaque inside the lumen influence the blood flow resulting into stenosis of the lumen
size of the stenosis limits the blood supply in the distal parts of the coronary circulation
limitation of more than 75% of the lumen could be considered as a serious stenosis
Consecutive limitation of the blood flow provide condition for collateral circulation

Stable fibromuscular plaques
Their presence inside the lumen could limit the blood flow thus limit oxygen supply addressed for working myocardial cells
Long lasting tight stenosis (possibility for opening of collateral circulation) used to result into small infarction due to collateral blood supply
Stable plaque ~ stable angina pectoris –
Chest pain occurs usually after the same (stabile, constant) dose of physical exercise or emotional event, but important is that this pain lasts less than 15 min and disappears after stopping of the physical activity or due to nitrate therapy

Nonstable plaque
http://www.nature.com/nm/journal/v17/n11/full/nm.2538.htmlhttp://www.nature.com/nm/journal/v17/n11/full/nm.2538.html
Nonstable angina pectoris
Chest pain occurs after different doses of physical exercise or emotional event (once intensive, another day mild activity could provoke the pain). This pain lasts more than 15 min and does not respond to rest condition or nitrate therapy
Progress of the stenosis in time without appropriate intervention leads to myocardial infarction
Myocardial infarction is necrosis of myocardial cells due to ischemia – clinical symptoms are the same like in nonstable angina, but to make a diagnose of MI we should confirm presence of necrosis by ECG and enzyme analysis – CK – MB, AST, Troponine T


Mechanisms responsible for nonstable AP and MI
The main role in this process plays creation of the thrombus on the basis of ATS damage in coronary arteries, usually on the basis of disrupture of the plaque surface
Disrupture of the plaque could lead to creation of the labile thrombus (not fixed strongly to base) and our endogenous systems are able to destroy the thrombus partially – nonstable angina
If the damage of the plaque surface is too deep to uncover collagen – thrombosis is more intensive, as well as the thrombus is strongly fixed to basis, and endogenous mechanisms are not strong enough to destroy it – MI
The most common cause of myocardial infarction is thrombosis of coronary arteries due to dysruption of the plaque surface.

Small plaques are usually rich in lipids and the tendency to complications
These plaques also show tendency to disruption in comparison to plaques with fibromuscular envelope
In general – plaques with high risk of disruption are small, rich in lipids with increased activity of the macrophages inside the plaque.
Disruption of the plaque is usually caused by mechanical events acting on the plaque surface – pressure, shearing or traction internal pressure on the plaque surface - hypertensionchanges of the vessel lumen - spasm of CAmoving of the arteries due to systolic/diastolic phase
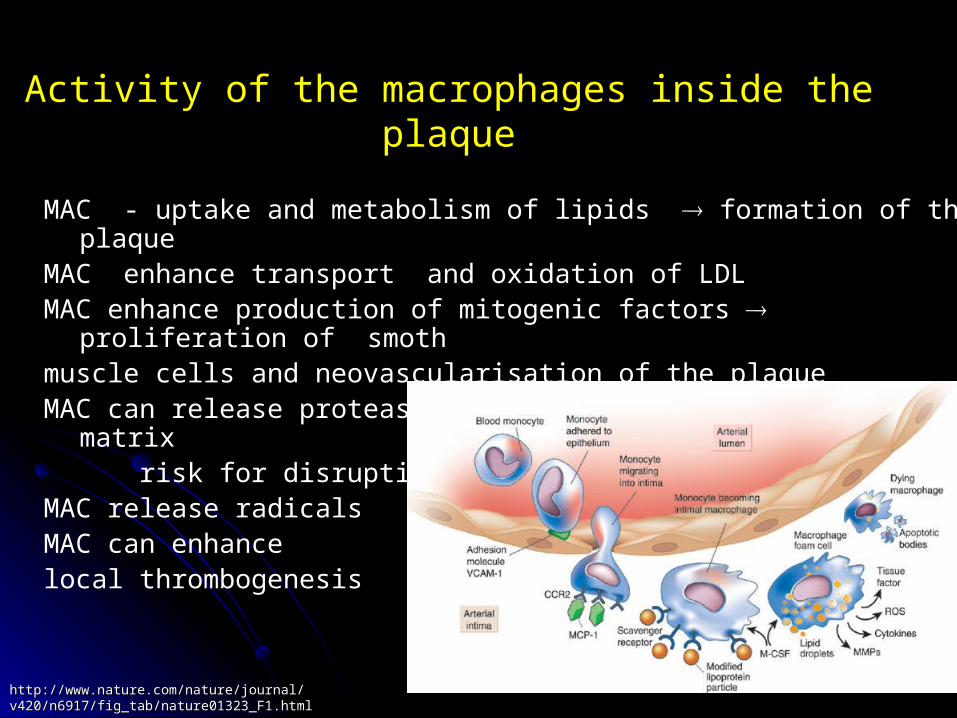
Activity of the macrophages inside the plaque
MAC - uptake and metabolism of lipids formation of the plaqueMAC enhance transport and oxidation of LDL MAC enhance production of mitogenic factors proliferation of smoth muscle cells and neovascularisation of the plaqueMAC can release proteases digestion of extracellular matrix risk for disruptionMAC release radicalsMAC can enhance local thrombogenesis
http://www.nature.com/nature/journal/v420/n6917/http://www.nature.com/nature/journal/v420/n6917/fig_tab/nature01323_F1.htmlfig_tab/nature01323_F1.html

Thrombosis inside the CA
Degree of thrombosis and duration of thrombus deposition are influenced by local and systemic factors present in the affected vessel during plaque disruption
These factors are necessary as triggers of different pathological processes in CA and their clinical manifestation

Local factors
Degree of plague disruption Superficial damage of the plaque – thrombogenic stimulus is relatively
limited, resulting either in small mural thrombosis, or transient thrombotic occlusion similar to nonstable angina pectoris
Deeper damage or ulceration exposes collagen, tissue factor and other factors resulting to relatively persistent thrombotic occlusion – MI
Degree of stenosis - platelet deposition increases with increased degree of stenosis, indicating shear-induced platelet activation
Residual thrombus – predisposed to recurrent thrombotic occlusion

Residual thrombusAfter organization and spontaneous lysis of the thrombi, there are small
remnants – residual thrombiThese residual thrombi predisposed patients with unstable angina or AMI to
residual stenosis and to repeated thrombotic occlusion – rethrombosis could by caused by
- residual mural thrombus encroaches into the vessel lumen - residual thrombus is one of the strongest thrombogenic surface probably due to
increased thrombin activity- there is also increased activity of platelets and thrombin in the site of surrounding
thrombolysis
Systemic thrombogenic factors- Primary hypercoagulative or thrombogenic states can favor local
thrombosis (level of circ. catecholamine, cigarette smoke, hypercholesterolemia)
- Other metabolic abnormalities ( homocysteine level, impaired fybrinolysis, level of fibrinogene, factor VII)

Spasm of CA
Inversive angina – Prinzmetal AP – chest pain occures in rest condition, mainly in bed
Spasm of CA can result into acute myocardial infarction – typical clinical signs, positive ECG, positive enzymes, but autopsy does not reveal the thrombus
Endothelial dysfunction is a consequence of ATS process As we mentioned before – normal endothelium reveal tendency to
produce vasodilating molecules, but endothelium with impaired functions preffer production of pro constrictive substances
After provoking stimulus (catecholamine, pressure, emotive event) endothelium could produce vasconstrictvie molecules resulting into coronary artery occlusion due to spasm
http://www.invasivecardiology.com/article/1156http://www.invasivecardiology.com/article/1156

Summary of basic mechanisms responsible for myocardial ischemia
• Myocardial ischemia is the consequence of inappropriate blood supply that leads to inbalance between oxygen supply and real oxygen requirements
Inbalance is caused by reduction or complete block of coronary blood flow, or by increased requirement of oxygen for working cardiomyocytes, these mechanisms are usually combined
• Lumen of the coronary artery can be reduced to 30-20% of normal lumen without ischemia in subject in rest condition. But if this patient will start the physical activity thus increasing oxygenrequirements, myocardial ischemia with chest pain can occur
• Extension of myocardial ischemia depends on the level (site)of arterial occlusion, size of the occluded vessel, presence and quality of collateral circulation. Ischemic area could be small –microischemia or extremely large affecting more than 40 % ofleft ventricle mass
• Intensity of myocardial ischemia may form mild forms to strong and serious ischemia is depending on the tight of stenosis, duration of vessel occlusion, collateral circulation and on the preload and afterload of cardiomyocytes
• Duration of myocardial ischemia can be transient short lasting, can occur repeatedly or can be long lasting (permanent), if theocclusion is permanent

Development of ischemic injury of myocardium
Myocardial cells become ischemic within 10 sec of coronary occlusion, no-flow ischemia
Early consequences: ATP production, contractility, enhanced glycogenolysis,
intracellular acidosis, extracellular hyperkalemia, other ionic and metabolic disturbances
After several minutes of ischemia the cells lack the ability to contract, anaerobic processes take over, lactic acid is accumulated inside the cells, myocytes are edematous, content of glycogene is decreased and ultrastructural changes can be seen

Cardiac cells remain viable 20 min under these condition of non-flow ischemia, during this time they can be recovered if blood flow is restored to 20 min from the beginning of the heart attack – there is only functional impairment of the cells
After this time irreversible changes (morphological changes) of the cells can be seen – damage of intracellular organelles, more than 20 min non flow status results into necrosis - MI
Consequences of myocardial ischemia include changes of electrophysiological properties of the cells and changes of mechanical properties – the pump function

Electrophysiological changes
- Due to lack of ATP, ionic inbalance, accumulation of metabolic products, formation of free radicals and neurotransmitter release
- decrease of rest membrane potential due to increased extracellular level of K+, decrease of RMP means that this value is nearer to 0 point /absolute value is decreased/ normal is -90 mV, after ischemia can be -70, - 60 mV
- decrease of maximal speed of the action potential upstroke- changes of action potential duration- changes of excitability, refractoriness- onset of abnormal automacy- cell to cell electrical uncoupling- changes in conduction speedThese mechanisms could be responsible for arrhythmias

Mechanical properties
Decreased contractility of myocardial cells can be seen after several seconds of non flow status
Absolute contractile dysfunction is developed after 3-5 minutes of non flow status
After 10-15 min – ischemic contracture
There are two mechanisms probably responsible for this phenomenon 1. Decrease of ATP level – which is necessary for contraction2. Rapidly developing intracellular acidosis
Intracellular acidosis leads to ionic inbalance and influence binding of Ca++
onto contractive elements – myofibriles abnormality of excitatory and contractile cycle contractile dysfunction
For the same reasons myocardial relaxation is impaired

Intensity of contractile dysfunction depends on intensity and duration of occlusion
Hypokinesis – ischemic part of the ventricular wall moves during systolic and diastolic phase less than normal nonischemic myocardium
Akinesis – ischemic wall does not move Dyskinesis – ischemic wall moves paradoxically during systolic and
diastolic phase
Nonischemic myocardium has increased contractility as a compensatory reaction to improve cardiac output (sympathetic system, Frank – Starling mechanism)
Contractile dysfunction is usually accompanied by diastolic dysfunction – relaxation is also active process, decreasing ventricular compliance

Clinical signs of IHD
- Chest pain- ECG abnormalities- Myocardial enzymes elevation- Systolic/diastolic heart failure

Symptoms and signs of IHD and mechanisms of their onset
Chest pain – stenocardia, is related to the accumulation of some molecules within the myocardium, which are able to stimulate afferent nociceptive vagal fibers to induce pain – these molecules are: lactic acid, potassium, proton, adenosine... They may be ascribed as a products or consequences of anaerobic metabolic pathway
Angina – stable, nonstable This pain is usually described as sharp, burning, pressure, very
intensive, the pain is spreading into the left arm, carotid region, or into the epigastrium, or interscapular region, is accompanied with vegetative symptoms
Silent ischemia- Short lasting episodes of ischemie, no affecting IVP, or distribution of
vagal nociceptive afferents, senile or diabetic neuropathy

Nausea, vomiting – general symptom, mostly in patients with diaphragmatic localization of MI
Fear, sweating, pallor, sudden diarrhea – activation of vegetative NS
Dysrythmias – premature beats, ventricular tachycardia, or flutter, different types of AV blocks – electrophysiological changes
Signs of heart failure, or cardiogenic shock according to extent of MI
Symptoms and signs of IHD and mechanisms of their onset
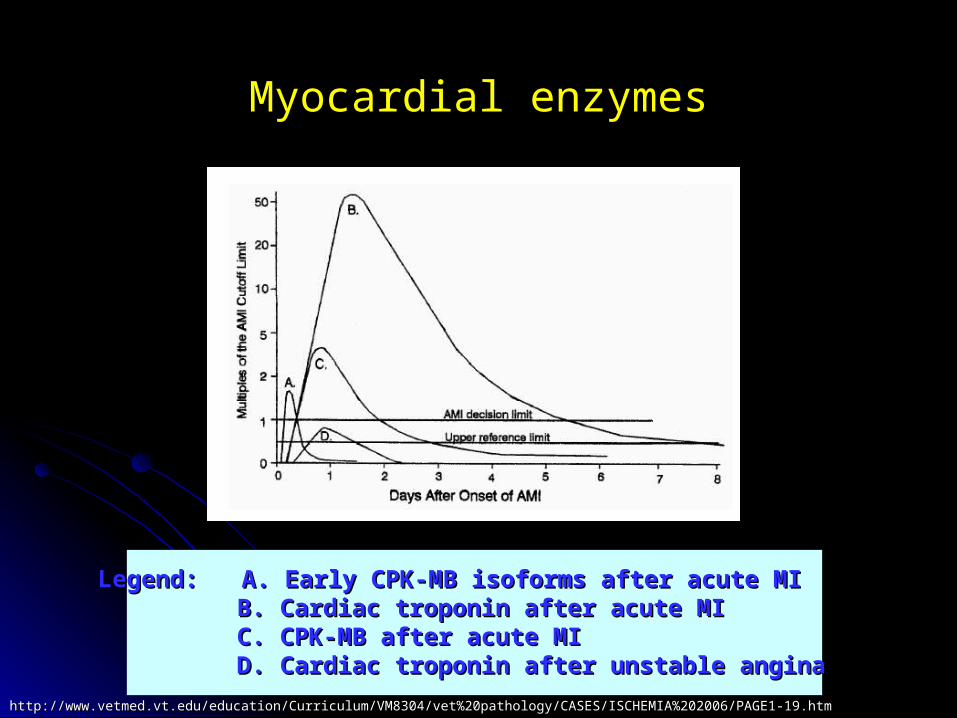
Myocardial enzymesMyocardial enzymes
Legend: A. Early CPK-MB isoforms after acute MILegend: A. Early CPK-MB isoforms after acute MI B. Cardiac troponin after acute MIB. Cardiac troponin after acute MI C. CPK-MB after acute MIC. CPK-MB after acute MI D. Cardiac troponin after unstable anginaD. Cardiac troponin after unstable angina
http://www.vetmed.vt.edu/education/Curriculum/VM8304/vet%20pathology/CASES/ISCHEMIA%202006/PAGE1-19.htmhttp://www.vetmed.vt.edu/education/Curriculum/VM8304/vet%20pathology/CASES/ISCHEMIA%202006/PAGE1-19.htm

http://cyhsanatomy1.wikispaces.com/What+do+Myosin+and+Actin+do%3Fhttp://cyhsanatomy1.wikispaces.com/What+do+Myosin+and+Actin+do%3F

EKG diagnosis EKG diagnosis ST segment elevationST segment elevation ST segment depressionST segment depression T wave inversionT wave inversion Q wave formationQ wave formation
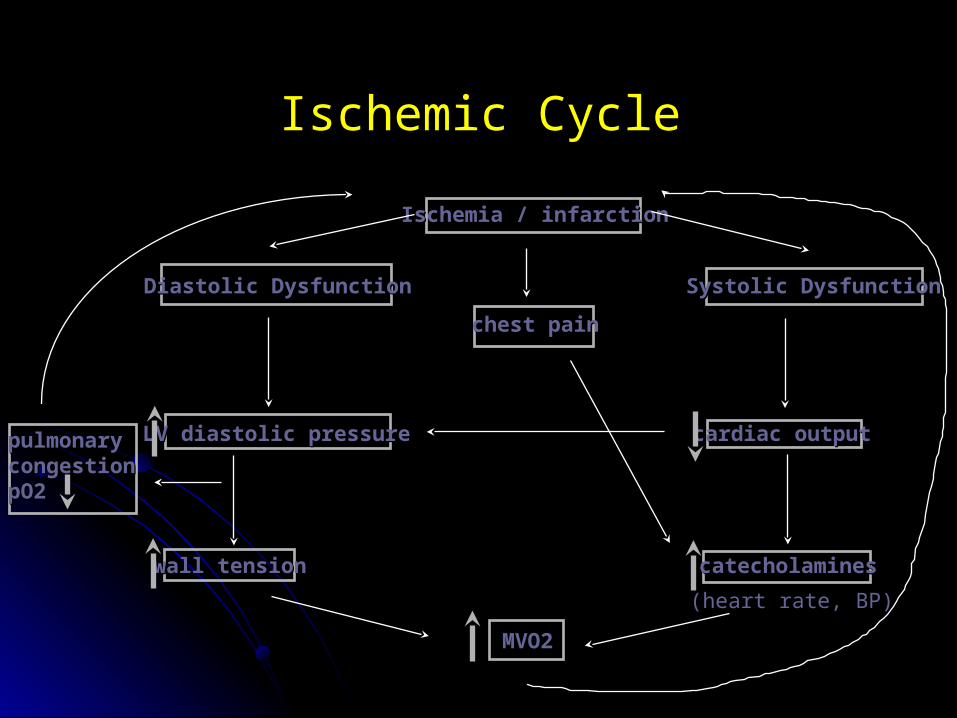
Ischemic Cycle
Ischemia / infarctionIschemia / infarction
chest painchest pain
Diastolic DysfunctionDiastolic Dysfunction Systolic DysfunctionSystolic Dysfunction
cardiac outputcardiac output
catecholaminescatecholamines
MVO2MVO2
wall tensionwall tension
LV diastolic pressureLV diastolic pressurepulmonarypulmonarycongestioncongestionpO2pO2
(heart rate, BP)(heart rate, BP)

Reperfusion of ischemic myocardium
• spontaneous or therapeutical
• reperfusion after short lasting myocardial ischemia could recover the cardiomyocytes and restitute their function ad integrum
Stunned myocardiumTotal non flow ischemia does not last to long to cause irreversible damage of the cells – necrosisBut these cells lack the ability to contract or their contractility is significantly reduced – it is a phenomenon of stunned myocardiumDecreased contractility could be improved but this improvement requires time (sometimes several days or weeks)Prolonged depression of myocardial function present after recovery of non flow ischemia is caused by insensitivity of myofilaments to calcium

Hibernating myocardium
• reversible reduction of power of contraction present during mild degree of coronary insufficiency
•typical for chronic forms of coronary flow reduction and the myocardium could reduce contractility appropriately to reduced blood supply (down - regulation)
• there is prolonged depression of contractility with simultaneous reduction of energy consumption, adequately to decreased blood flow
•Just after the improvement of coronary blood flow the contractility becomes improved too
•Contractile dysfunction is caused by reduced entrance of CaContractile dysfunction is caused by reduced entrance of Ca++++ into the into the cardiomyocytescardiomyocytes

Contractile dysfunction in hypoxic, stunned and hibernating myocardium
Hypoxia
Stunning
Hibernation
Ca2+ transientamplitude
Myofilament Ca2+
sensitivity
Maximal Ca2+
activated pressPi / pH i
/
= / =
= / = = =
Pi - inorganic phosphate; pHi - intracellular pH
- increased relative to control; - decreased; = - unchanged


















