Is Urinary Incontinence Dampening Your Days?
43
Urinary Incontinence- the Basics Presented by: Rhonda Walsh, MD February 26, 2015
-
Upload
summit-medical-group -
Category
Health & Medicine
-
view
260 -
download
2
Transcript of Is Urinary Incontinence Dampening Your Days?
Urinary Incontinence- the
BasicsPresented by:
Rhonda Walsh, MD
February 26, 2015

About Me
• Urology Residency at University of Texas-
San Antonio
• Fellowship in Female Urology/Voiding
Dysfunction at NYP-Columbia
• Operate at St. Barnabas, Overlook,
Morristown
• Also treat pelvic pain, prolapse, UTIs,
kidney stones, bladder and kidney cancer

What is incontinence?
• Incontinence is defined as “the inability
to restrain natural discharges or
evacuations of urine or feces”
• For our purposes, it refers to the
involuntary leakage of urine

Female Bladder

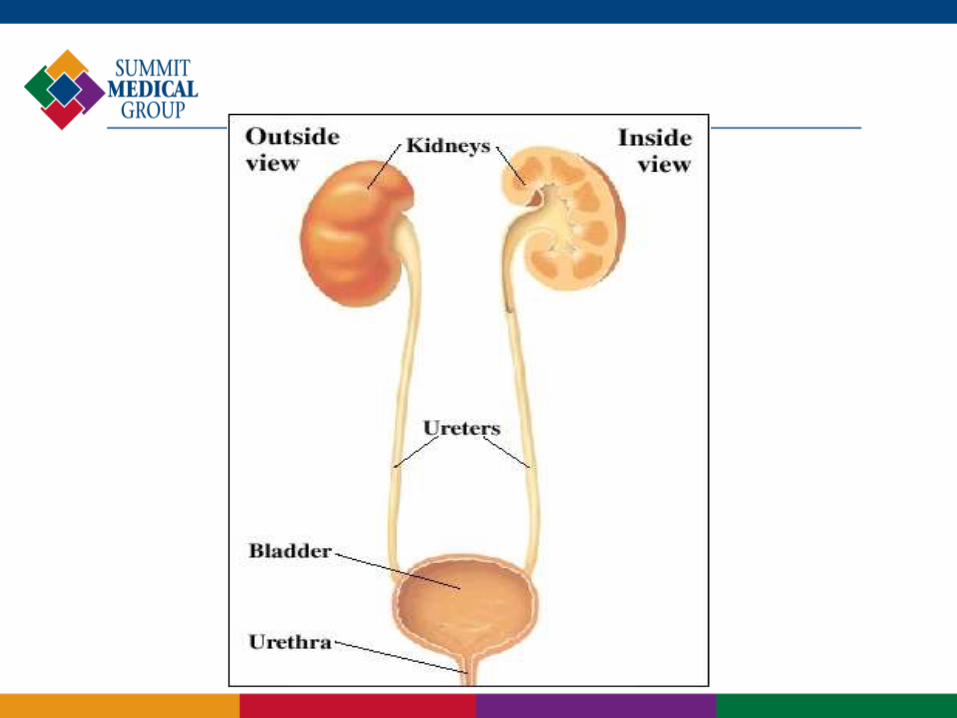
What does the bladder do?
• The function of the bladder is to store
urine
• In theory, the bladder should hold urine,
without leakage, until you say it is time
to empty
• This process can fail either because of
the urethra not holding urine in, or the
bladder squeezing to get urine out
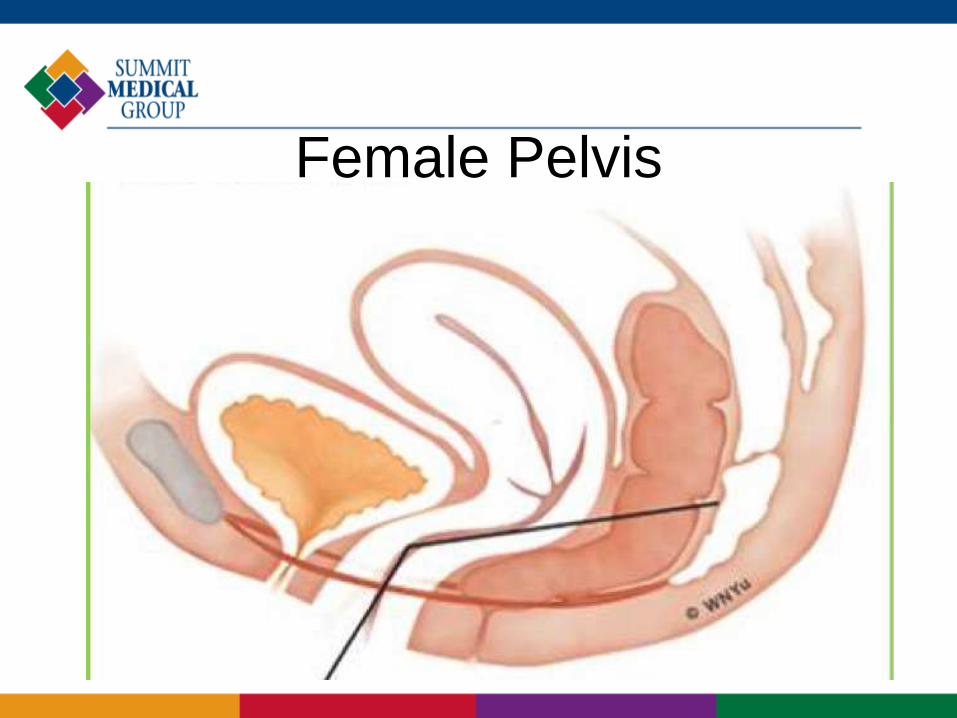
Female Pelvis

Different types of incontinence
• Stress
• Urge
• Mixed
• Overflow
• Associated symptoms like frequency,
urgency, nocturia

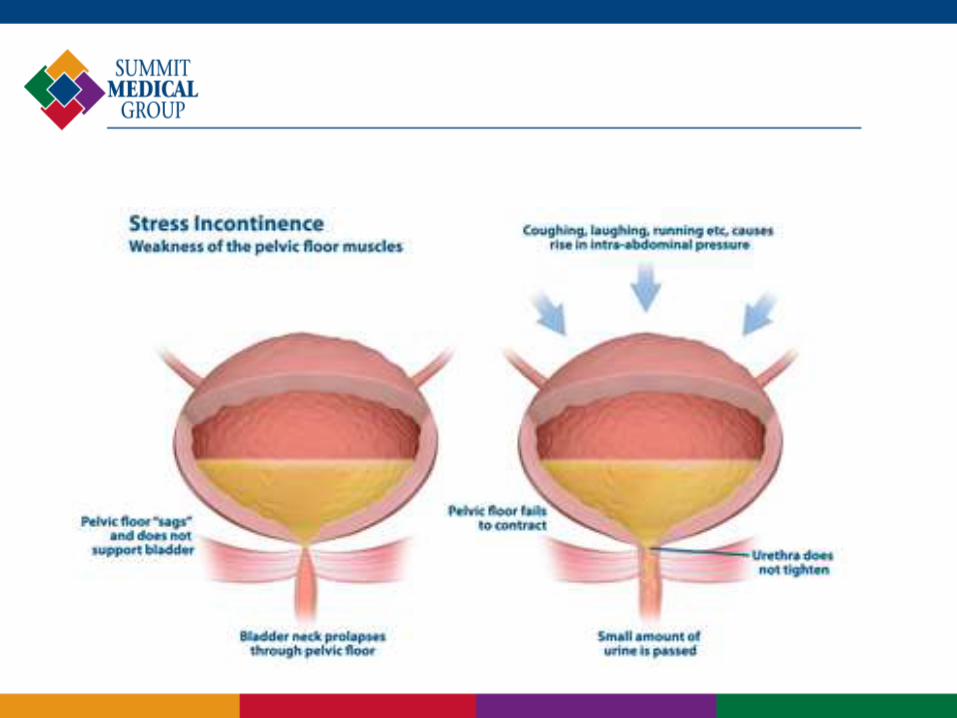
Stress Incontinence
• Leakage of urine with increases in
abdominal pressure
• Often described as happening when
coughing or sneezing, or bending to lift
an object
• Caused by a lack of urethral support
• Often seen in women after childbearing
years- extended labor can damage the
perineal nerve worsening incontinence
in those prone to it

Urge Incontinence
• Leakage of urine when there is an urge to go to
the bathroom and one does not get there in
time
• Thought to be caused by overactive bladder
(OAB)- the bladder muscle squeezing without
permission
• Possible to have urgency without incontinence-
OAB wet vs. OAB dry
• OAB is a symptom complex that can include
urgency, frequency, incontinence, and nocturia

Other types
• Mixed incontinence- stress and urge
together
• Overflow incontinence- Leakage of
urine because bladder is full and cannot
be emptied
• Constant urine leakage following pelvic
surgery or childbirth can be due to a
fistula

How common is incontinence?
• The prevalence of incontinence in
studies ranges from 11% to 72%,
depending on the definition used
• A more accurate assessment may be
21% of women over 70 having at least
weekly incontinence
• Stress is most common (49%), followed
by mixed (29%) and urge (22%)

Risk factors
• Exercise
• Childbirth
• Obesity
• Aging
• Back injuries and neurologic problems
can contribute to bladder dysfunction

Other causes of incontinence
• Urinary tract infections sometimes cause
incontinence
• Very rarely, bladder cancer will cause the
bladder to be overactive
• It is important to see your doctor about
incontinence as it may be a sign of
another problem (sudden)
• Some medications (lithium, SSRIs)
• Diabetes can cause urgency and
frequency

Nocturia
• Defined as waking from sleep to void
• More common with age
• Caused by increased urine production
at night due to hormonal changes as
well as sleep apnea, cold
• Difficult to treat

Workup
• Making sure you empty your bladder
(ultrasound)
• Checking for urine infection
• Physical examination including pelvic exam to
make sure there are no abnormalities
• Voiding diary
• Possibly cystoscopy (looking in the bladder with
a camera)
• Urodynamic testing (looking at how the bladder
squeezes)

Physical Exam

Voiding diary

Cystoscopy

Urodynamics

How is incontinence treated?
• Behavior changes
• Exercises
• Medication (URGE)
• Surgery (STRESS)

Why is incontinence treated?
• “No one ever died from wetting their
pants”
• Caveat: sometimes increases injury and
infection in the elderly
• If incontinence is limiting your ability to
live your life, it should be treated

Treatment Algorithm
Leaking
Urge
Neuro-modulation
Medication Botox
Stress
Biofeedback Surgery
Overflow
Behavior Modification

Behavioral Changes
• Quitting smoking- less coughing!
• Losing weight
• Managing fluid intake- what goes in
must come out
• Managing constipation
• Managing stress and depression
Exercise Therapy
• In conjunction with behavioral
modification, can work for both types of
incontinence
• Special pelvic floor physical therapists
teach kegel exercises and do muscle
stimulation/biofeedback

Urge incontinence treatment
Urge incontinence
Medication Urodynamics
Neuro-modulation
Botox
Antimuscarinics
• Most common medications/least expensive
• Work on the bladder to relax it and reduce
involuntary contractions
• Reduce urgency episodes by 2-3/day and
incontinence episodes by 2/day
• Drawbacks are side effects of dry mouth
and constipation
• Used with caution in elderly due to
cognitive side effects

Mirabegron (Myrbetriq- Astellas)
• B3 agonist
• Works to increase bladder capacity
• Significantly reduces voids by 1.75/day
and incontinence episodes by 1.5/day
• NO constipation and dry mouth
• Most common side effect is elevation of
systolic blood pressure, but no more
than other bladder medications

Posterior Tibial Nerve Stimulation
• Treats frequency, urgency, and urge
incontinence
• Involves 12 weeks of 1-30 minute session a
week, then monthly maintenance
• Needle inserted into ankle stimulates the tibial
nerve
• Results are similar to medications- Decreases
incontinence episodes by 3 a day and urge
episodes by 5

PTNS (Uroplasty)
Interstim (Medtronic)
• A device placed for overactive bladder
that does not respond to medication
• Stimulates the pelvic nerves to reduce
overactivity
• Like a pacemaker for the bladder,
providing constant low-level stimulation
to override errant signals


Botulinum toxin
• Injected through a cystoscope into the
bladder wall
• Partially paralyzes the bladder
• Works for 3-6 months the first time, then
6-12 months with subsequent injections
• Decreases urge episodes by 3 and
incontinence episodes by 2/day
• Risk of urinary retention
Stress incontinence
Stress incontinence
Mid-urethral sling
Injectibles
Kegels

Pelvic floor muscle exercises• 10 slow-twitch contractions and 10 fast
5 times daily
• Learn to contract these muscles at
times of increased abdominal pressure
• Works for urge incontinence as well
• 70% improvement rate, but must keep
doing them
Mid-urethral Sling
• Multiple surgeries have been done over
the years for stress incontinence
• In the past, women had open abdominal
surgery to “lift the bladder”
• Now the most common is a sling put in
through the vagina
• Often will help with mixed incontinence
• Successful in 80-90% of women

Mid-urethral sling
TVT
TOT


Vaginal Mesh
• YES it is safe in properly selected
patients
• The FDA warning is for PROLAPSE
REPAIR, not for slings
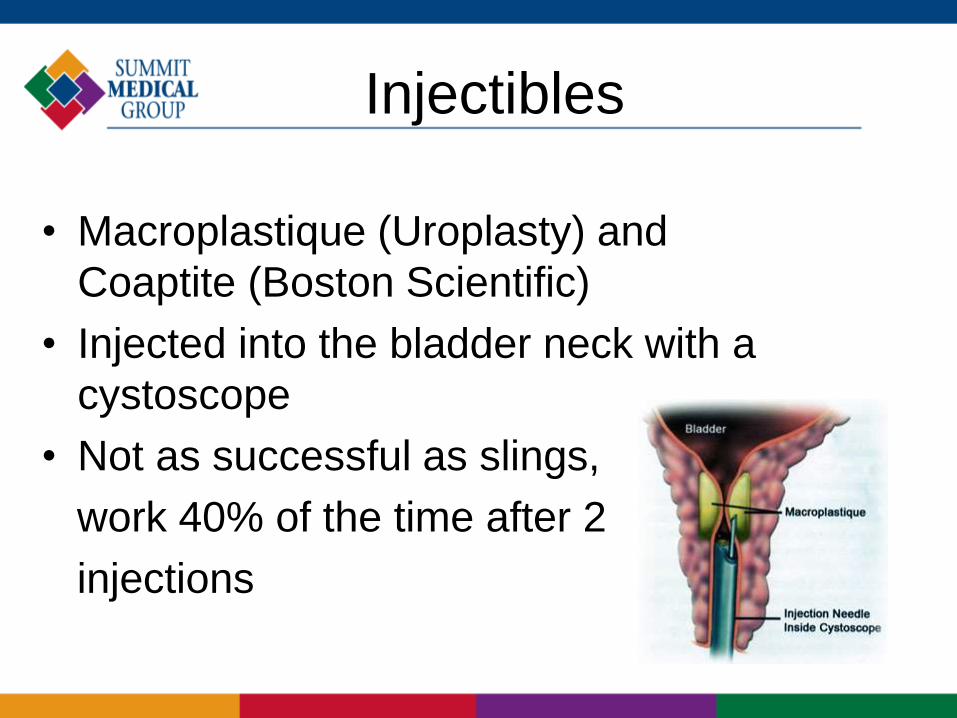
Injectibles
• Macroplastique (Uroplasty) and
Coaptite (Boston Scientific)
• Injected into the bladder neck with a
cystoscope
• Not as successful as slings,
work 40% of the time after 2
injections

Summary
• Incontinence is a common problem
• Incontinence can be treated with
minimal side effects
• If your urine leakage is bothering you,
please get it treated

Thank you
• Questions???