Is It Time for a Status Update? Transitioning Treatment ... · ©2016 MFMER | slide-1 Is It Time...
37
©2016 MFMER | slide-1 Is It Time for a Status Update? Transitioning Treatment from Status Epilepticus to Super Refractory Status Epilepticus David Roy, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds May 17 th , 2016
Transcript of Is It Time for a Status Update? Transitioning Treatment ... · ©2016 MFMER | slide-1 Is It Time...
©2016 MFMER | slide-1
Is It Time for a Status Update? Transitioning Treatment from Status Epilepticus to Super Refractory Status Epilepticus
David Roy, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds May 17th, 2016
©2016 MFMER | slide-2
Objectives • Differentiate diagnosis of status epilepticus, refractory
status epilepticus, and super refractory status epilepticus
• Describe pathophysiology of pharmacoresistance in status epilepticus
• Discuss different treatment options as status epilepticus becomes more refractory

©2016 MFMER | slide-3
A Silent Epidemic • 8-19% of comatose ICU patients diagnosed with status
epilepticus (SE) on EEG do not have clinical signs of seizures
• Second most common neurological emergency with a risk of major morbidity and mortality
• Generalized Convulsive Status Epilepticus (GCSE) • Non-convulsive Status Epilepticus (NCSE)
• Negative symptoms • aphasia, catatonia, confusion, lethargy
• Positive symptoms • agitation, aggression, delirium, emesis,
psychosis
Brophy GM, et al. Neurocrit Care. 2012;17:3-23 Towne AR, et al. Neurology 2000;54:340-5
Claassen J, et al. Neurology 2004;62:1743-8
EEG: electroencephalogram

©2016 MFMER | slide-4
Incidence & Mortality
Hesdorffer DC, et al. Neurology. 1998;50(3):735-41 Dham BS, et al. Neurocrit Care. 2014;20(3):476-83
Kantanen, AM, et al. Epilepsy Behav. 2015;49:131-34
0
10
20
30
40
50
0
5
10
15
20
25
30
1 3 5 7 9
In-h
ospi
tal M
orta
lity
(%)
SE In
cide
nce
(per
100
,000
)
Decade of Life
Incidence In-hospital Mortality
22%
36%
0
10
20
30
40
50
RSE SRSE1-
yr M
orta
lity
(%)
©2016 MFMER | slide-5
Question #1 What is the minimum continual seizure duration required to diagnose GCSE?
A. 2 minutes B. 5 minutes C. 10 minutes D. 15 minutes
©2016 MFMER | slide-6
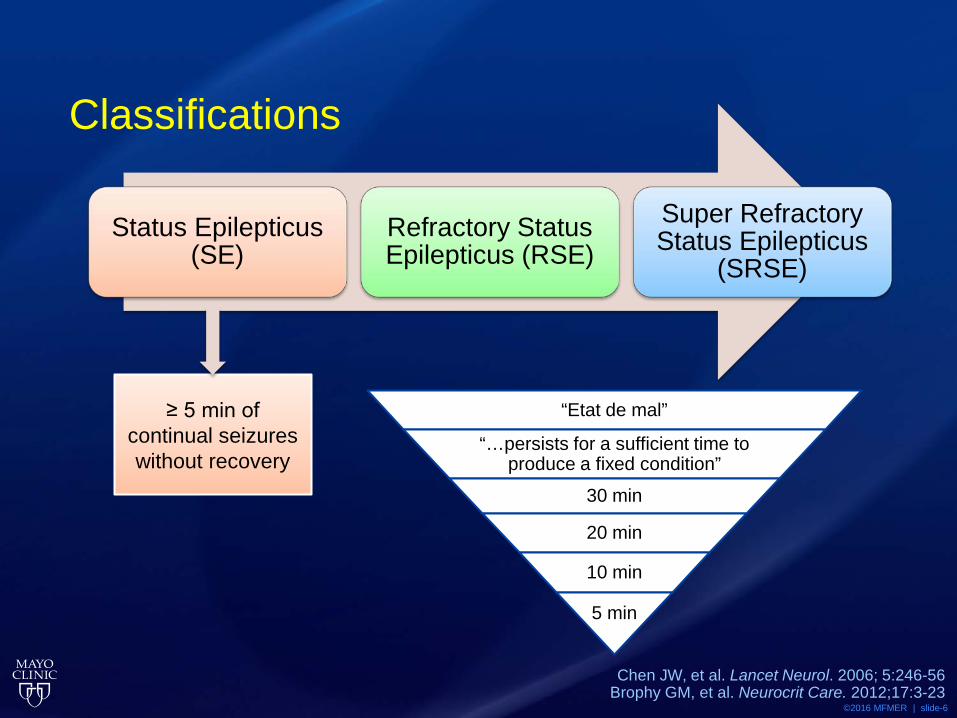
Classifications
Status Epilepticus (SE)
Refractory Status Epilepticus (RSE)
Super Refractory Status Epilepticus
(SRSE)
≥ 5 min of continual seizures without recovery
“Etat de mal”
“…persists for a sufficient time to produce a fixed condition”
30 min
20 min
10 min
5 min
Chen JW, et al. Lancet Neurol. 2006; 5:246-56 Brophy GM, et al. Neurocrit Care. 2012;17:3-23

©2016 MFMER | slide-7
Pathophysiology of SE
• Disruption in balance of excitatory and inhibitory neurotransmitters
• Excitatory: glutamate • Inhibitory: GABA
Ca2+
Na+ Cl-
GABA glutamate
GABA NMDA

©2016 MFMER | slide-8
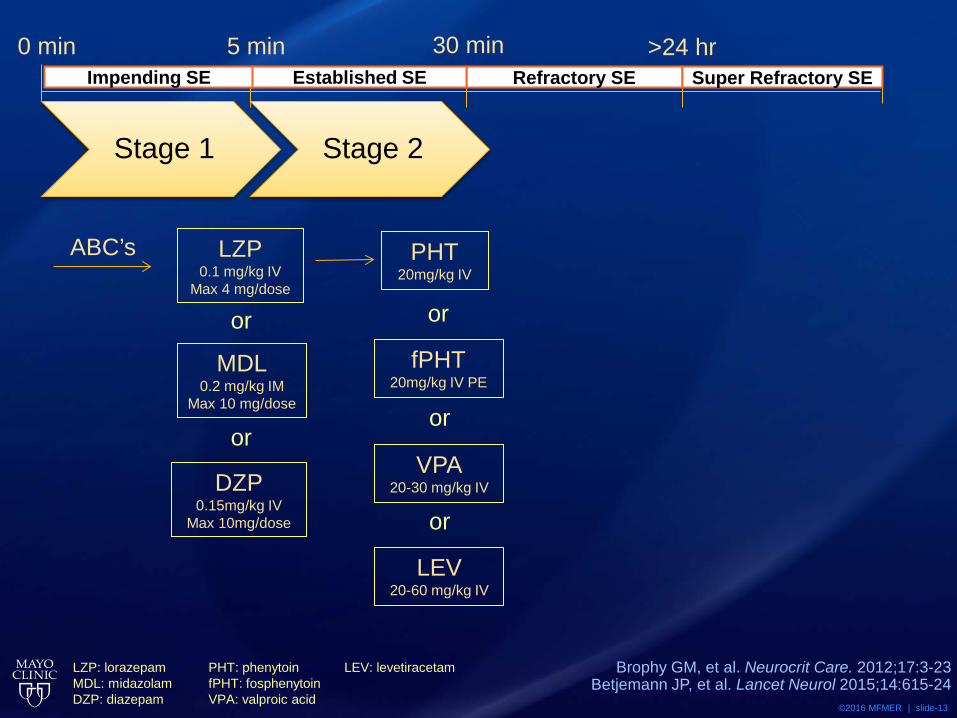
0 min 5 min >24 hr
LZP: lorazepam MDL: midazolam DZP: diazepam
ABC’s LZP 0.1 mg/kg IV
Max 4 mg/dose
MDL 0.2 mg/kg IM
Max 10 mg/dose
or
DZP 0.15mg/kg IV
Max 10mg/dose
or
30 min Refractory SE Impending SE Established SE Super Refractory SE
Stage 1
Brophy GM, et al. Neurocrit Care. 2012;17:3-23 Betjemann JP, et al. Lancet Neurol 2015;14:615-24

©2016 MFMER | slide-9
Treiman DM, et al. – VA Coop Trial
Treiman DM, et al. NEJM 1998. 339(12):792-98
64.9%
58.2% 55.8%
43.6%
17.9%
24.2%
8.3% 7.7%
0
10
20
30
40
50
60
70
LZP PHB DZP+PHT PHT
Suc
cess
ful T
reat
men
t (%
)
Overt GCSESubtle GCSE
p = 0.002
LZP: lorazepam DZP: diazepam
PHB: phenobarbital PHT: phenytoin
©2016 MFMER | slide-10
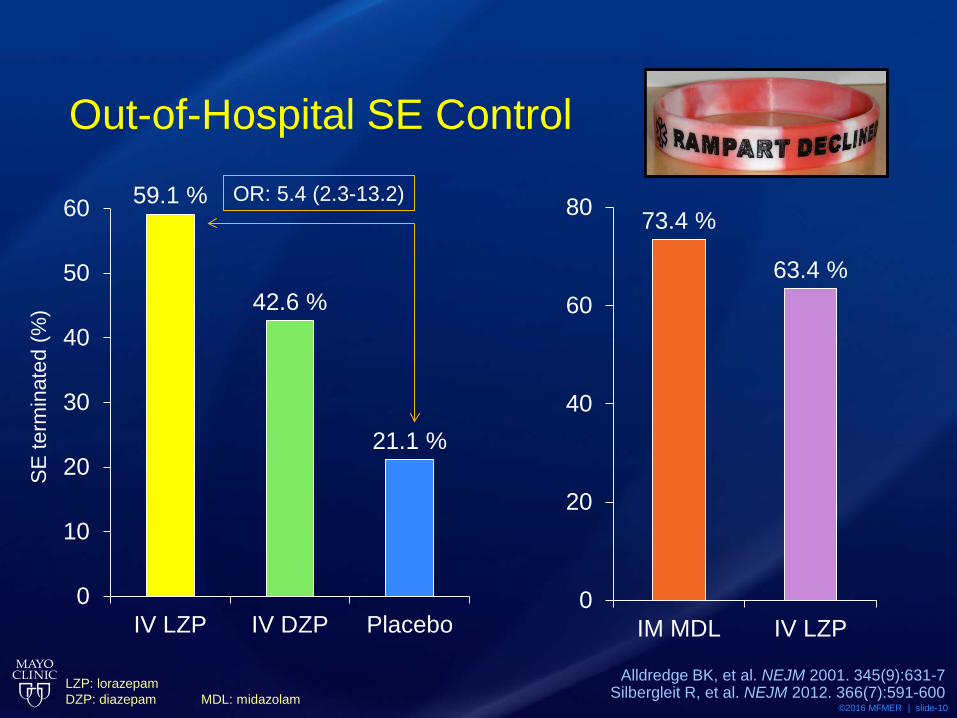
Out-of-Hospital SE Control
59.1 %
42.6 %
21.1 %
0
10
20
30
40
50
60
IV LZP IV DZP Placebo
SE
term
inat
ed (%
)
Alldredge BK, et al. NEJM 2001. 345(9):631-7 Silbergleit R, et al. NEJM 2012. 366(7):591-600
73.4 %
63.4 %
0
20
40
60
80
IM MDL IV LZP
OR: 5.4 (2.3-13.2)
LZP: lorazepam DZP: diazepam
MDL: midazolam

©2016 MFMER | slide-11
Alternative Routes of Administration • Intranasal MDL
• Equally effective as IV DZP in terminating seizures in children
• Buccal MDL • More effective than rectal DZP in children
with convulsive febrile seizures • Rectal DZP
• FDA-approved as Diastat® - 0.2-0.5 mg/kg
Chamberlain JM, et al. JAMA 2014;311(16):1652-60 Thakker A, et al. J Neurol 2013. 260:470-74
Dreifuss FE, et al. NEJM 1998. 338:1869-75 LZP: lorazepam DZP: diazepam
MDL: midazolam

©2016 MFMER | slide-12
Case • 30 y/o male admitted to the ED for generalized
tonic-clonic seizures • Continues to seize for over 5 minutes despite
two 4mg doses of IV lorazepam
©2016 MFMER | slide-13
Brophy GM, et al. Neurocrit Care. 2012;17:3-23 Betjemann JP, et al. Lancet Neurol 2015;14:615-24
0 min 5 min
PHT 20mg/kg IV
fPHT 20mg/kg IV PE
or
VPA 20-30 mg/kg IV
LEV 20-60 mg/kg IV
or
or
LZP: lorazepam MDL: midazolam DZP: diazepam
PHT: phenytoin fPHT: fosphenytoin VPA: valproic acid
LEV: levetiracetam
30 min >24 hr Refractory SE Impending SE Established SE Super Refractory SE
Stage 2
ABC’s LZP 0.1 mg/kg IV
Max 4 mg/dose
MDL 0.2 mg/kg IM
Max 10 mg/dose
or
DZP 0.15mg/kg IV
Max 10mg/dose
or
Stage 1

©2016 MFMER | slide-14
PHT, VPA or LEV? • Retrospective analysis (n=187)
• LEV higher risk of failure than VPA • OR 2.7, 95% CI 1.2-6.1
• No difference in PHT
• Largest prospective RCT, single-center comparison
Alvarez V, et al. Epilepsia 2011. 52:1292-96 Mundlamuri RC, et al. Epilepsy Res 2015. 114: 52-58
PHT: phenytoin VPA: valproic acid LEV: levetiracetam
AED # controlled
PHT 34/50 (68%)
VPA 34/50 (68%)
LEV 39/50 (78%)
71%
87% 92%
50
60
70
80
90
100
1 AED 2 AED 3 AED
% S
eizu
re C
ontr
ol
©2016 MFMER | slide-15
No Clear Favorite • Phenytoin/Fosphenytoin
• Liver disease, hypotension, QT prolongation, purple glove syndrome, drug interactions
• Valproic Acid • Liver disease, pregnancy, hyperammonemia,
pancreatitis, somnolence, drug interactions • Levetiracetam
• Psychiatric history, agitation, osteoporosis, kidney disease, headache
Hocker, SE. Continuum 2015. 21(5):1362-83

©2016 MFMER | slide-16
Case • 30 y/o male admitted to the ED for generalized
tonic-clonic seizures • Continues to seize for over 5 minutes despite
two 4mg doses of IV lorazepam • Continues to seize despite adequate load
with fosphenytoin
©2016 MFMER | slide-17
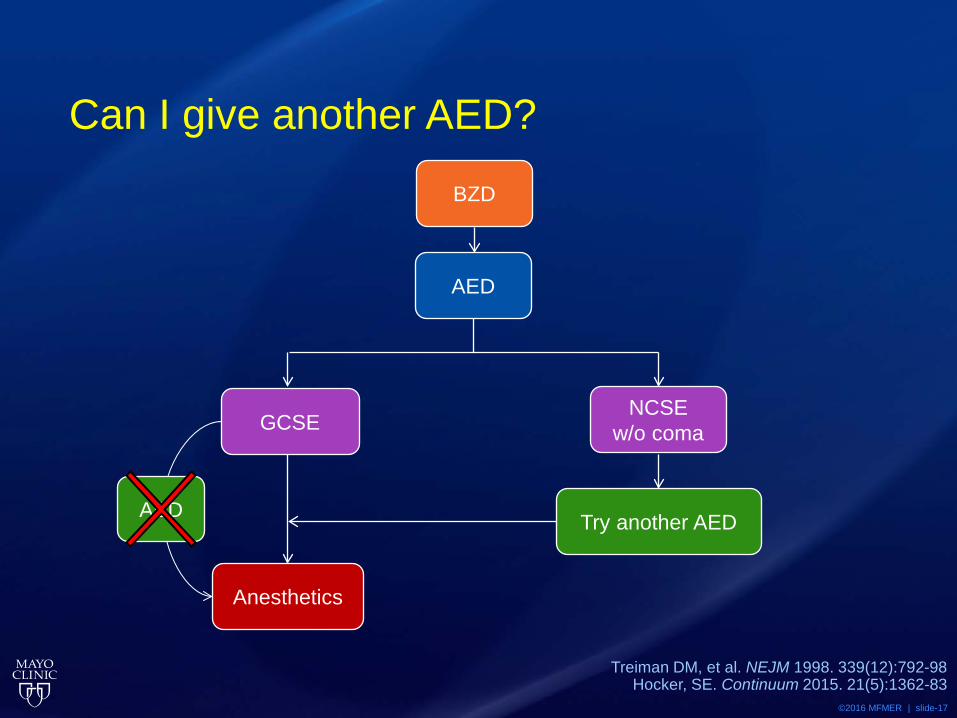
Can I give another AED?
Treiman DM, et al. NEJM 1998. 339(12):792-98 Hocker, SE. Continuum 2015. 21(5):1362-83
NCSE w/o coma GCSE
AED
BZD
Anesthetics
Try another AED AED

©2016 MFMER | slide-18
Definitions
Status Epilepticus (SE)
Refractory Status Epilepticus (RSE)
Super Refractory Status Epilepticus
(SRSE)
≥ 5 min of continual seizures without recovery
Seizure activity despite BZD and
one AED
©2016 MFMER | slide-19
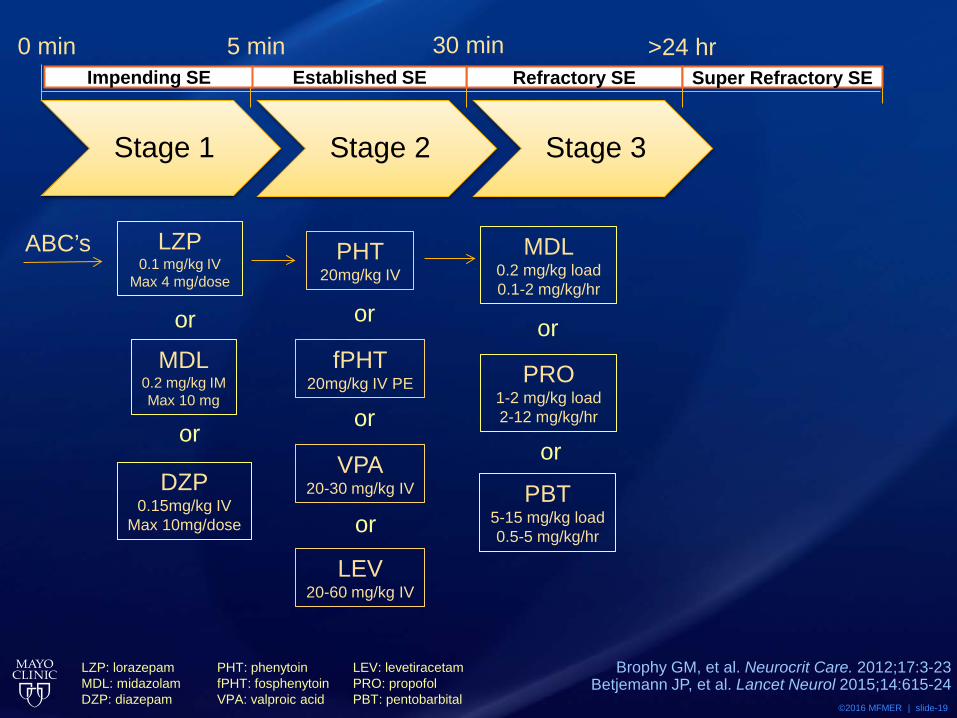
0 min 5 min
MDL 0.2 mg/kg load 0.1-2 mg/kg/hr
PRO 1-2 mg/kg load 2-12 mg/kg/hr
or
PBT 5-15 mg/kg load 0.5-5 mg/kg/hr
or
ABC’s LZP 0.1 mg/kg IV
Max 4 mg/dose
MDL 0.2 mg/kg IM Max 10 mg
or
DZP 0.15mg/kg IV
Max 10mg/dose
or
Stage 1
PHT 20mg/kg IV
fPHT 20mg/kg IV PE
or
VPA 20-30 mg/kg IV
LEV 20-60 mg/kg IV
or
or
Stage 2 Stage 3
Refractory SE Impending SE Established SE Super Refractory SE 30 min >24 hr
LZP: lorazepam MDL: midazolam DZP: diazepam
PHT: phenytoin fPHT: fosphenytoin VPA: valproic acid
LEV: levetiracetam PRO: propofol PBT: pentobarbital
Brophy GM, et al. Neurocrit Care. 2012;17:3-23 Betjemann JP, et al. Lancet Neurol 2015;14:615-24
©2016 MFMER | slide-20
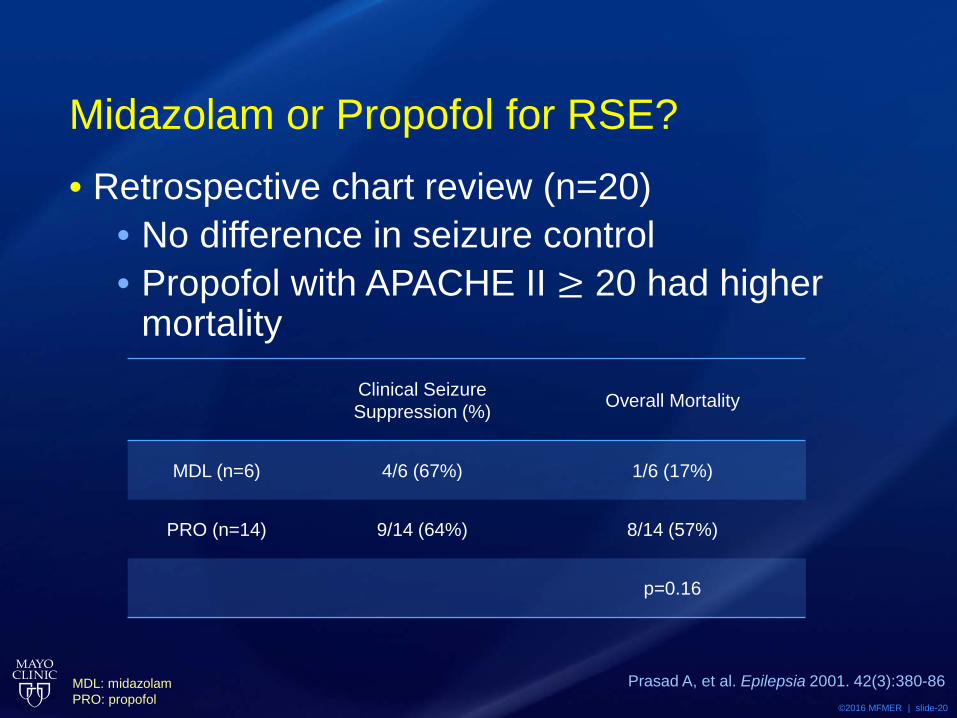
Midazolam or Propofol for RSE? • Retrospective chart review (n=20)
• No difference in seizure control • Propofol with APACHE II ≥ 20 had higher
mortality
Prasad A, et al. Epilepsia 2001. 42(3):380-86
Clinical Seizure Suppression (%) Overall Mortality
MDL (n=6) 4/6 (67%) 1/6 (17%)
PRO (n=14) 9/14 (64%) 8/14 (57%)
p=0.16
MDL: midazolam PRO: propofol
©2016 MFMER | slide-21
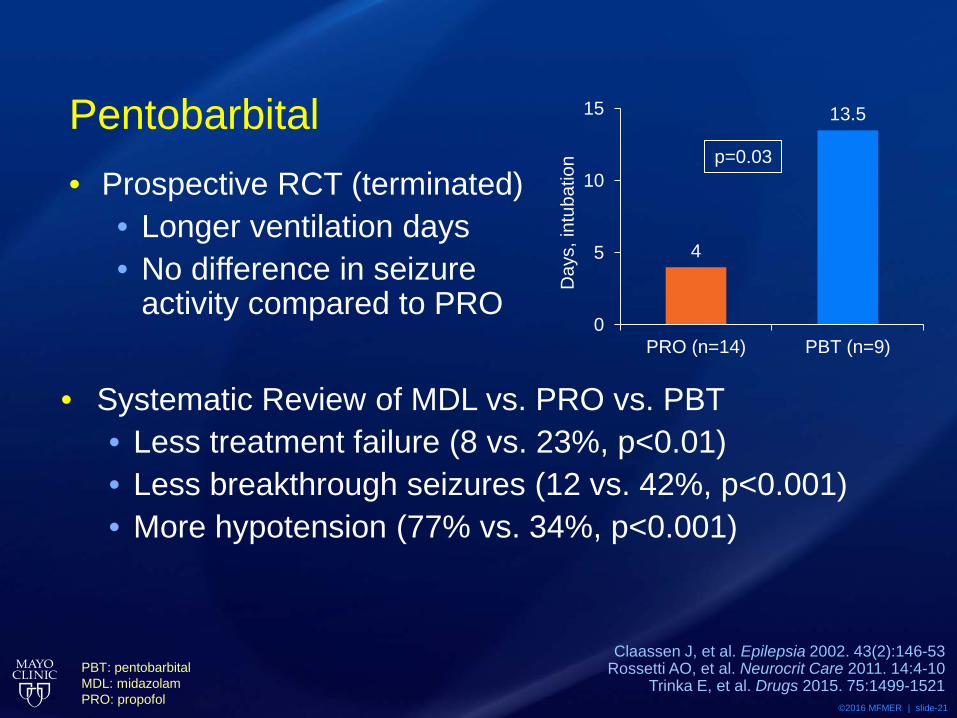
Pentobarbital • Prospective RCT (terminated)
• Longer ventilation days • No difference in seizure
activity compared to PRO
Claassen J, et al. Epilepsia 2002. 43(2):146-53 Rossetti AO, et al. Neurocrit Care 2011. 14:4-10
Trinka E, et al. Drugs 2015. 75:1499-1521
4
13.5
0
5
10
15
PRO (n=14) PBT (n=9)
Day
s, in
tuba
tion p=0.03
• Systematic Review of MDL vs. PRO vs. PBT • Less treatment failure (8 vs. 23%, p<0.01) • Less breakthrough seizures (12 vs. 42%, p<0.001) • More hypotension (77% vs. 34%, p<0.001)
PBT: pentobarbital MDL: midazolam PRO: propofol

©2016 MFMER | slide-22
Which anesthetic?
Drug Mechanism Metabolism Advantages Disadvantages
Midazolam GABA potentiator Hepatic; active
metabolites excreted renally
Short half-life Hypotension, tachyphylaxis, prolonged elimination half-
life in obesity
Propofol
GABA agonist, Na channel antagonist, NMDA inhibition, Ca channel modulator
Hepatic Short half-life Hypotension, PRIS*, hypertriglyceridemia,
pancreatitis
Pentobarbital GABA potentiator Hepatic Can be used for prolonged
periods
Hypotension, ileus, immunosuppression,
hepatotoxicity, metabolic acidosis (propylene glycol
toxicity), long half-life
• Insufficient data to support one agent over another
Iyer VN, et al. Crit Care Med 2009. 37(12):3024-30 Hocker, SE. Continuum 2015. 21(5):1362-83
*Propofol-related Infusion Syndrome
©2016 MFMER | slide-23
Case • 30 y/o male admitted to the ED for generalized
tonic-clonic seizures • Continues to seize for over 5 minutes despite
two 4mg doses of IV lorazepam • Continues to seize despite adequate load
with fosphenytoin/levetiracetam • Continues to seize despite 2mg/kg/hr IV
midazolam infusion

©2016 MFMER | slide-24
Definitions
Status Epilepticus (SE)
Refractory Status Epilepticus (RSE)
Super Refractory Status Epilepticus
(SRSE)
≥ 5 min of continual seizures without recovery
Seizure activity despite BZD and
one AED
Breakthrough seizures while on CI anesthetics for
24 hours
©2016 MFMER | slide-25
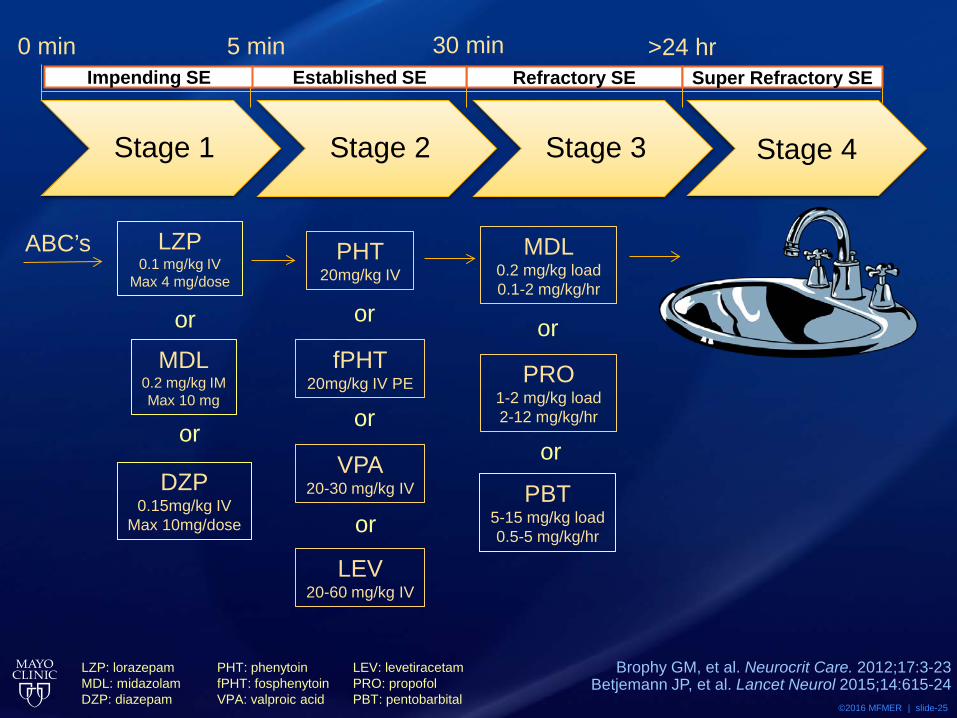
0 min 5 min Refractory SE Impending SE Established SE Super Refractory SE
30 min >24 hr
LZP: lorazepam MDL: midazolam DZP: diazepam
PHT: phenytoin fPHT: fosphenytoin VPA: valproic acid
LEV: levetiracetam PRO: propofol PBT: pentobarbital
Brophy GM, et al. Neurocrit Care. 2012;17:3-23 Betjemann JP, et al. Lancet Neurol 2015;14:615-24
ABC’s LZP 0.1 mg/kg IV
Max 4 mg/dose
MDL 0.2 mg/kg IM Max 10 mg
or
DZP 0.15mg/kg IV
Max 10mg/dose
or
Stage 1
PHT 20mg/kg IV
fPHT 20mg/kg IV PE
or
VPA 20-30 mg/kg IV
LEV 20-60 mg/kg IV
or
or
Stage 2
MDL 0.2 mg/kg load 0.1-2 mg/kg/hr
PRO 1-2 mg/kg load 2-12 mg/kg/hr
or
PBT 5-15 mg/kg load 0.5-5 mg/kg/hr
or
Stage 3 Stage 4

©2016 MFMER | slide-26
Pharmacoresistance of SE • Increased NMDA receptors • Decreased GABA receptors
• 50% decrease in GABA receptors after 1 hour of SE
• 20-fold decrease in BZD potency within 30 minutes of SE
Naylor DE, et al. J Neurosci 2005;25:7724-33 Kapur J, et al. J Neurosci 1997;17:7532-40
Mazarati AM, et al. Brain Res 1998;814:179-85

©2016 MFMER | slide-27
Ketamine • NMDA-receptor antagonist • Animal data endorses efficacy • Human data suggests safety and efficacy
• 32% RSE controlled after ketamine • 1.5-4.5 mg/kg load then 2-7.5 mg/kg/hr
• Minimum dose response: 0.9 mg/kg/hr • Earlier it was added, higher chance of control
• No increase in morbidity or mortality
Borris DJ, et al. Epilepsy Res 2000. 42:117-22
Gaspard N, et al. Epilepsia 2013. 54(8):1498-1503

©2016 MFMER | slide-28
Lacosamide • Enhances slow inactivation of sodium channels • 9 case-series, 10 case-reports
• No data for RSE • 136 patients; 56% success rate
• TRENdS 2013 • LCM 400 mg vs. fPHT 20 mg/kg for NCSE • Terminated in 2014 due to low enrollment
Hofler J, et al. Epilepsia 2013. 54 (3):393-404 Fountain NB, et al. Epilepsia 2013. 54 (1):58-65
Husain AM, et al. Epilepsy Behav 2015. 49:337-39 LCM: Lacosamide fPHT: Fosphenytoin
©2016 MFMER | slide-29
Super Refractory Status Epilepticus • Isoflurane
• Enhances GABA • Case reports show possibly effective when
combined with hypothermia • Possibly neurotoxic
• Perampanel • AMPA-receptor antagonist • Case reports suggest variable efficacy • Unknown long-term safety profile
Fugate, JE et al. Anesth Analg 2010; 111:1520-4 Husain AM, et al. Epilepsy Behav 2015. 49:337-39

©2016 MFMER | slide-30
Immunotherapy for SRSE • SRSE may be caused by antibodies against
neural cell receptors • IV immunoglobulins (IVIG)
• 0.4 gm/kg/day x 5 days • Methylprednisolone
• 1 gm/day x 5 days • Plasma exchange
Zeiler FA. Seizure 2015. 32:100-108

©2016 MFMER | slide-31
• Pyridoxine • Cofactor necessary for GABA
production • 100-300 mg IV
• Magnesium • NMDA-receptor antagonist • 2-6 gm/hr until level of 3.5 mmol/L • 50% controlled in non-eclamptic SE in
recent systemic review • Neurosurgery if lesion identified
Super Refractory Status Epilepticus
Zeiler FA. Seizure 2015. 32:100-108
Glutamate
GABA
GAD, B6

©2016 MFMER | slide-32
Review • Benzodiazepines to stop initial seizure • Load with an AED to prevent future seizure • Repeat different AED if remain in NCSE with
consciousness; transition to anesthetics more quickly if in GCSE
• Choose anesthetics based on comorbidities and drug properties
• Kitchen sink
©2016 MFMER | slide-33
Question #2 • Which of the following underlying mechanism(s)
of SRSE makes ketamine an attractive option? A. Increased sensitivity of GABA receptors B. Increased number of GABA receptors C. Increased number of NMDA receptors D. All of the above

©2016 MFMER | slide-34
Question #3 • When compared to propofol and midazolam,
which of the following is a disadvantage of pentobarbital for RSE?
A. Development of tachyphylaxis B. Increased incidence of hypertriglyceridemia C. Likelihood of developing rhabdomyolysis D. Profound hypotension
©2016 MFMER | slide-35
Summary • Seizure duration and failure of treatments
differentiate the stages of status epilepticus • Agents used early may no longer be effective
due to development of pharmacoresistance • Increased morbidity and mortality as status
epilepticus becomes more refractory • Treat quickly; time is brain

©2016 MFMER | slide-36
Questions & Discussion
©2016 MFMER | slide-37
Is It Time for a Status Update? Transitioning Treatment from Status Epilepticus to Super Refractory Status Epilepticus
David Roy, PharmD PGY1 Pharmacy Resident Pharmacy Grand Rounds May 17th, 2016