
Is it all about Money? A Randomized Evaluation of the Impact of Insurance Literacy and Marketing...
35
Is it all about Money? A Randomized Evaluation of the Impact of Insurance Literacy and Marketing Treatments on the Demand for Health Microinsurance in Senegal Jacopo Bonan (Milan-Bicocca), Olivier Dagnelie (Namur), Philippe LeMay-Boucher (Heriot-Watt) and Michel Tenikue (CEPS) Thanks to: ILO/Bill and Melinda Gates Foundation, Carnegie Trust of Scotland, Fonds National de la Recherche Luxembourg and the GRAIM, Thies. 1
-
Upload
suzan-mcdonald -
Category
Documents
-
view
215 -
download
2
Transcript of Is it all about Money? A Randomized Evaluation of the Impact of Insurance Literacy and Marketing...

Is it all about Money? A Randomized Evaluation of the Impact
of Insurance Literacy and Marketing Treatments on the Demand for Health
Microinsurance in Senegal
Jacopo Bonan (Milan-Bicocca), Olivier Dagnelie (Namur), Philippe LeMay-Boucher (Heriot-Watt)
and Michel Tenikue (CEPS)
Thanks to: ILO/Bill and Melinda Gates Foundation, Carnegie Trust of Scotland, Fonds National de la Recherche Luxembourg and the GRAIM, Thies.
1
IntroductionHealth providers in Senegal:• Organized according to a tiered system:
1) health huts (staffed by community workers)2) health posts (nurses and certified midwives)3) health centres (with medical doctors, etc.)Survey: Thiès (2nd largest city in Senegal)Thies: 1 public hospital and 1 private hospital
2

Introduction• High health costs
-Cost in health huts and posts are small-Hospitals: Xray (6000FCFA); Blood analysis (2000); Consultation (10-25000); Night (>25000)(sample median income 112500FCAF/month)
→ Often too ExpensivePoor people face difficulties to access ‘modern-medical’ health care
3

Introduction1) health shocks → direct expenditures (drugs & treatment) : out-of-pocket payments (OOP)2) indirect costs → reduction in productivity
• OOP in Senegal : 70% of total expenditure in health (WHO)(5% in GBR, 11% in France)
• at low levels of income : strong link between health and income
→ Scope for more health insurance
4

Health Microinsurance Available
• no universal coverage in Senegal No state insurance (ill-functioning: CESAME)
• informal insurance(bilateral transfers; networks :De Weerdt et al.(2006); ROSCAS: Dagnelie et al. (2012))
5

Health Microinsurance Available
• IPM: treasury made up of employees’ compulsory contributions. (for large employers)
• Private health insurers (PAMECAS, etc)
• Mutual Health Organizations (MHO)
6

MHOs expansion• Self or informally employed: no IPM
(>60% in our sample):ill-suited supply of health insurance
• Senegal 1990 in Fandene: first ‘mutuelle de santé’ or MHO
• Grass-root movement: managed by locals• MHOs in Senegal: 13 (1993) → 140+ (2007)
7
MHOs structure and rules• Open to everybody• Membership fees (1000-3000FCFA/hh)
• Monthly premium 100-500FCFA/month/person
• Period of observation (3 months)
• MHO have contracts with all health providers
• cover 25 to 75% of consultation feescover 50% to 100% of medical exams and various inpatients cares fees
8

Microinsurance take-up in Thies
• Out of our sample of 360 heads of hh:32% of have health insurance, (for 73% of all household members)
Of which:→ 19% with IPM (public or private)(several private IPM are not working…)→ 3% with private health insurance → 10% with MHOs
9

Low MHO take-up• Overall MHO take-up rate in Thies region = 5% Smith et al. (2008) & Lépine et al. (2010).
→ Our Research Question:Why is MHO take-up rate so low despite being well established and having the potential to reach poor people?
10

Why low MHO take-up?• From our sample, people who justified the
lack of membership to MHOs:1) lack of information about the product offered and/or MHOs existence (70% of hh)2) lack of means (16%)3) lack of interest (5%) 4) lack of trust (2%).
11

Lack of Information• Cai et al. (2009): farmers in China refuse to purchase a heavily
subsidized insurance for sows → lack of awareness of the program.
• Giné et al. (2007); Cole et al. (2009) and Gaurav et al. (2009): → Limited understanding of rainfall insurance mechanisms in rural India.
• Jutting (2003): concept of insurance is alien to a large proportion of people in Senegal.
→ information campaign could have some impact
12

Lack of Means• Jutting (2003) poorer hh in Senegal less member of MHOs. • Chankova et al. (2008) similar results in Ghana and Mali• Giné et al. (2008) : take-up rate of rainfall insurance increases
with household wealth in rural Andhra Pradesh. • Cole et al. (2009) low take-up rates of rainfall insurance :
insurance is expensive. • In our sample: only mentioned by 16% Why?
→ willingness to pay (WTP) = actual premiums → a banana is 100FCFA (!?!)
Bonan (2011) uses this data and the contingency valuation method to get WTP for MHOs premiums.
13

Lack of Trust• Cai et al. (2009) low take-up by Chinese farmers: lack of trust
toward governmental institutions.
• Cole et al. (2009) endorsement of rainfall insurance in India from a third party ↑ purchase by 40%.
• In Thies:We asked the sample of non-members aware of the existence of MHOs: trust towards MHOs 1 to 10
Rescaled median score w.r.t. Trust in mother and family: 8/10
→ Large positive a priori from locals towards MHOs
14
What if we inform and ↓ fees?• Factors at play: Information & Means
impact on membership of: -more info -↓ financial barriers
→ Randomized Control Trials• Design and implement two treatments: 1)Insurance Literacy module2)Marketing with 3 vouchers
15

Our 2 treatments on 360 hh1) Literacy: 180 hh invited to:
3hour module on health microinsurance, MHOs and the concepts of risk and insurance. (given by GRAIM)
After2) Marketing: redeemable for 3 monthsVoucher 1: invitation to GRAIM (120 hh)Voucher 2: membership fees (120 hh)Voucher 3: memb. fees + 3000FCFA obs period
(120hh)16

17

Randomized Evaluation • Old technique:
The first published RCT appeared in the 1948 paper entitled:"Streptomycin treatment of pulmonary tuberculosis“which described a Medical Research Council investigation. -Austin Bradford Hill is credited as having conceived the modern RCT
18

Randomized Evaluation examples (I)
• Very active field in recent years:impulse from MIT and Poverty Action Lab
• Ex.: PROGRESA Mexico (1998)506 communities (half randomly selected)Treatment: cash grants to women conditional on school attendance and preventive health measures.
Results: Gertler et al. (2001)↓ illness, ↑ height, ↑enrollment
19

Randomized Evaluation examples (II)
• Ex: Kenya, free breakfast program effect on school participation.Results: Vermeersch (2002)↑ school participation
• Ex: Kenya, program providing uniforms and textbooks (to 7 randomly selected schools)Results: Kremer et al. (2002)↓ Dropout rates
20

Randomized Evaluation Ex: avg test scores (Duflo et al. 2007)Schools with textbook (T) – Schools without (C)
D = treatment effect + selection bias→ with successful randomization : We can pretend selection bias = 0
21
CYETYETYYED
CYETYEDCi
Ci
Ci
Ti
Ci
Ti
|||
||
^^ DTY olsii

Our data: Thies June 2010• Second city of importance in Senegal
population of 240,000 (2002 census)-its MHOs are the oldest in Senegal: well established supply of MHOs.
• 360 randomly selected households• Urban area: 20 km2• Baseline survey : housing information,
household composition, info on head hh.• Uptake decision: head of hh
22

Survey timeline:
23
May-June 2010:Survey of 360hh
September 2010: deadline for vouchers
Our dependent variable: subscribe or not to MHO between May-Sept
Invitation to Module is made followed by Marketing treatment
Greedy enumerators constantly asking for an increase in salary…

24

• ‘Strongly risk averse’ based on Voors et al. (2010)takes value 1 if individuals always opted for the certain outcome ‘A’ when presented with :
25

• ‘Patient’We elicit discount factors (Voors et al. (2010))→ discount factors at one month of:5%, 10%, 25%, 50%, 75%, 100%, 150%, 200%. dummy if head is more patient half of our sample.
26
•Aside: experience with real money gave very different results…
27
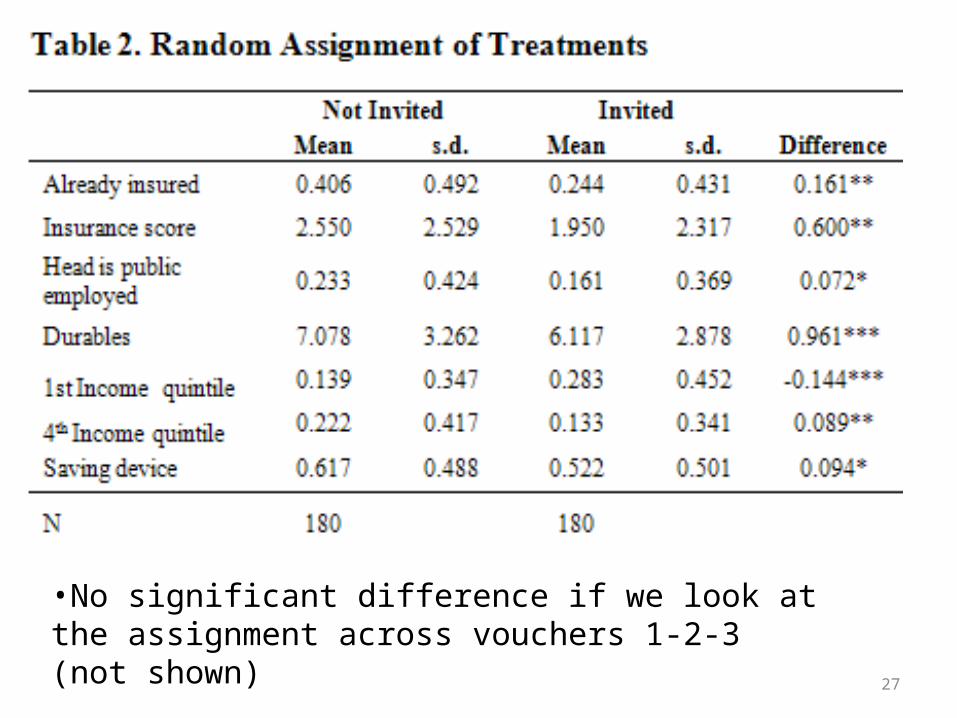
•No significant difference if we look at the assignment across vouchers 1-2-3 (not shown)

28
CYETYETYYED Ci
Ci
Ci
Ti |||
Not good newsSelection bias is clearly not equal to zero.Treatment group:-less insured (↑ intake)-less rich (↓ intake)-less knowledge about insurance (minor)-less public servant (↑ intake)
Bias can be + or – difficult to guess

29

Empirical Strategy• Our model:
-M takes value 1 if hh subscribes to a MHO following our treatments-E takes value 1 if hh was invited to module -Voucher takes value 1 if hh was given either voucher 2 or 3
• Results similar with probit (shown) and OLS
30

Our estimates• E measures the ‘invitation effect’
- does not measure the actual participation effect - α :‘intend to treat’ effect
• Low compliance rate (58%)we compute also ‘treatment on treated’ or ‘average treatment effect’ (Imbens-Angrist 1994) IV (instrument attendance by invitation)
• Both techniques give similar results31

32

Randomized Evaluation related to insurance
• Rainfall insurance intake1)Gaurav et al (2009): Gujarat, India (600hh)Treatments: insurance educ module & Marketing→ module ↑ intake; little impact from marketing
1)Cole et al. (2009): India (2000hh)Treatment: insurance educ module
→ no impact from module
33

34
Conclusion• Literacy module has no significant impactWhy?- Representative present (not being the head)- Health insurance is a simple product (relative
to rainfall insurance): no need- Quality of our module delivery?• Vouchers 2-3 have strong and positive impact-efficient to only distribute voucher 2
35


















