Irritable Bowel Syndrome
31
Irritable Bowel Syndrome Dr Max Groome Consultant Gastroenterologist Ninewells Hospital, Dundee
-
Upload
james-conner -
Category
Documents
-
view
82 -
download
2
description
Irritable Bowel Syndrome. Dr Max Groome Consultant Gastroenterologist Ninewells Hospital, Dundee. Irritable Bowel: Outline. What is the best way to identify IBS patients? What are the minimum number of relevant Ix? What is the best management?. IBS: Background. Chronic, relapsing problem - PowerPoint PPT Presentation
Transcript of Irritable Bowel Syndrome
Irritable Bowel Syndrome
Dr Max GroomeConsultant Gastroenterologist
Ninewells Hospital, Dundee
Irritable Bowel: Outline
• What is the best way to identify IBS patients?
• What are the minimum number of relevant Ix?
• What is the best management?
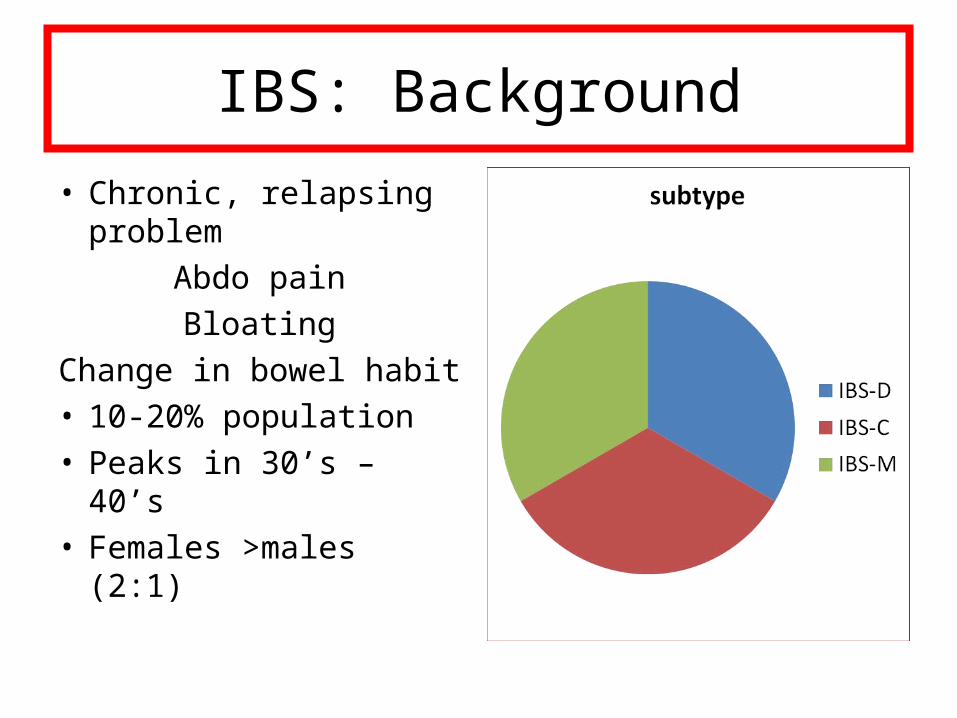
IBS: Background
• Chronic, relapsing problem
Abdo painBloating
Change in bowel habit• 10-20% population• Peaks in 30’s – 40’s• Females >males (2:1)
Pathophysiology of IBS
• Genes + Environment
• Disturbed GI motility; high-amplitude propagating contractions - exaggerated gastro-colic reflex, pain
• Visceral hypersensitivity
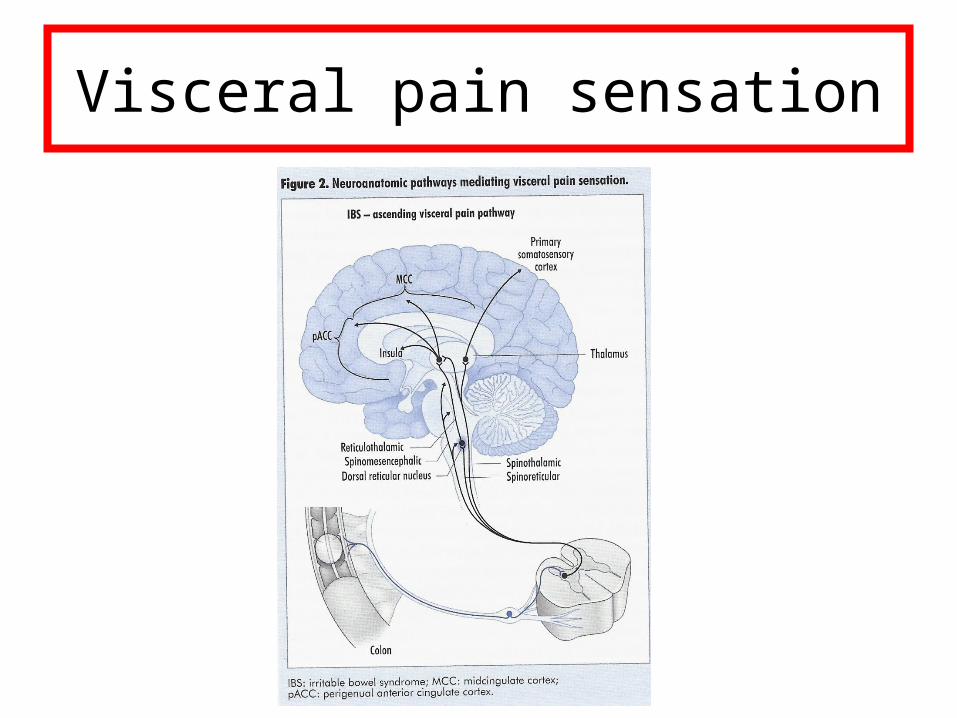
Visceral pain sensation
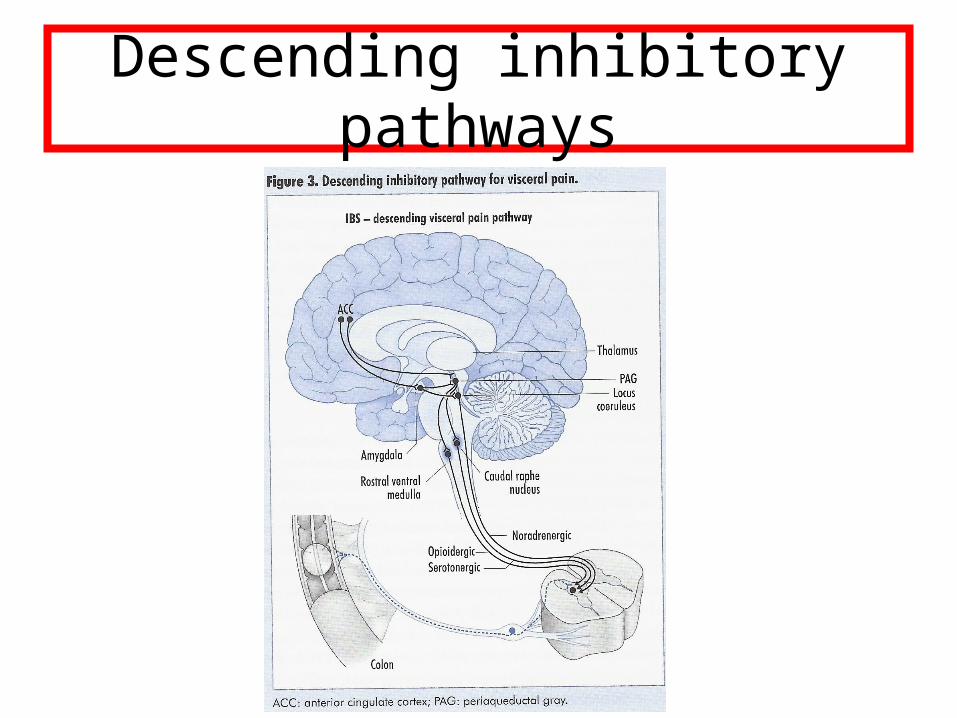
Descending inhibitory pathways
Visceral hypersensitivity
Seen in 2/3 patients (gut distension studies)Mechanisms• Peripheral sensitisation:Inflammatory mediators up-regulate sensitivity
of nociceptor terminals• Central sensitisation:Increased sensitivity of spinal neurones
Evidence of hypersensitivity?
• Peripheral:Up to 20% recall onset after infectious
gastroenteritis
• Central:Increased pain radiation to somatic structures
eg fibromyalgia
Rome III criteria
• Recurrent abdo pain/discomfort for at least 3 days per month for 3 months
+ 2 or more of:
• Improvement with defecation• Onset assoc. with ∆ stool frequency• Onset assoc. with ∆ stool form (appearance)
Additional clues...
• Bloating• Urgency• Sensation of incomplete emptying• Mucus per rectum• Nocturia (and poor sleep)• Aggravated by stress
Association with other illnesses
• Fibromyalgia• Chronic fatigue syndrome• Temporomandibular joint dysfunction• Chronic pelvic pain
Overlap cases likely to have more severe IBS, psychiatric problems
Psychological features
• At least 50% are depressed/anxious/hypochondriacal
• In tertiary centres, 2/3 have depression/anxiety
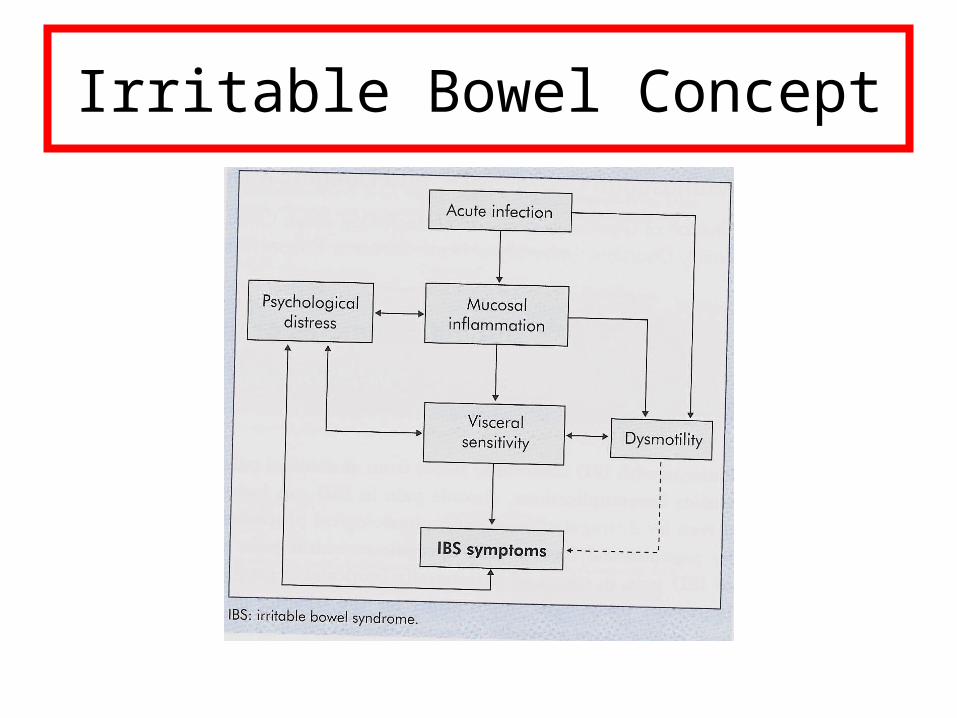
Irritable Bowel Concept
What is best way to identify IBS patients?
History
• A good history will make the diagnosis:Bowel habitBloating, nocturiaDiet (bread, fibre, meal times, bizarre exclusions)Trigger factors (infection, menstruation, drugs)Opiate use (codeine and Opiate/Narcotic bowel
syndrome)Psychosocial factors (stress)Underlying fears (‘cancer’)
Alarm features
• Age > 50• Short duration of symptoms• Woken from sleep by altered bowel habit• Rectal bleeding• Weight loss• Anaemia• FH of colorectal cancer• Recent antibiotics
What are the minimum number of relevent investigations?
Investigations
• FBC• ESR / plasma viscosity• CRP• Antibody testing for coeliac disease (TTG)• Lower GI tests if aged >50 or strong FH of CRC
What is the best management plan?
Treatment of IBS
• DietRegular meal times
Reduce fibre• Drugs:
Stop opiate analgesiaanti-diarrhoealsAnti-spasmodicsAnti-depressants
Fibre and IBS
• NICE guidance 2008:Evidence for ‘weak’ , ‘inconclusive’, ‘may be
detrimental’Suggest:‘review fibre intake, adjusting (usually reducing)
while monitoring symptoms. If fibre is necessary – suggest oats’
Stop opiates
With prolonged use can lead to ‘opiate/narcotic bowel syndrome’:
• Worsening pain control despite escalating dose• Reliance on opiates• Progression of frequency, duration and intensity of
pain• No GI explanation for pain
Poor quality studiesMetanalysis:*Global benefit vs placebo (NNT 5.5)Relief of pain vs placebo (NNT 8.8)No benefit for diarrhoea / constipation
*Poynard T Alimentary Pharm & Ther 2001
Anti-spasmodics (Mebeverine, Hyoscine)
Laxatives
• Fibre aggravates pain• Stimulant laxatives eg Senna not a long-term
solution (tachyphylaxis)• Lactulose promotes flatulence• PEG-based laxatives > lactulose*
*Attar A Gut 1999
Anti-diarrhoeals
• Loperamide (tablets or syrup)Opiate analogueinhibits peristalsis, gut secretionsBenefits diarrhoea. No effect on pain.No dependencyUse PRN / prophylactic
Cann P 1984 Dig Dis Sci.
Anti-depressants
Tricyclics eg Amitriptyline• Reduce diarrhoea• Reduce afferent signals from gut (‘central analgesics’)• Helps restore sleep pattern• Fits with ‘neuroplasticity’ theories:Loss of cortical neurones in psychiatric traumaBrain-derived neurotrophic factor increases with Rx (pre-cursor of
neurogenesis)• Low dose 10 – 75mg @ night (NNT 5.2)*Side effects limit use (NNH 22)
*Drossman DA 2003 Gastroenterology
Psychological treatment
• If severe anxiety / depression• If no response to empiric anti-depressantsOptions:Relaxation therapyCognitive Behavioural therapyHypnosis(moderate efficacy)
Irritable Bowel: Conclusions
• What is the best way to identify IBS patients?
• What are the minimum number of relevant Ix?
• What is the best management?
What does the patient want?
• Support and understanding• Clear explanation that IBS is an illness• Symptoms can be controlled by the patient• There is no miracle cure• There will be good days and bad• Explanation of treatment options
BSG IBS Guidelines 2007
Summary of management
• Careful history• Positive diagnosis of IBS• Simple management plan:
DietSymptom relief:
Loperamide / movicol / anti-spasmodicAmitriptyline
Further reading
• BSG IBS Guidelines 2007• NICE IBS Guidance 2008• AGA technical review 2002