IOS Press Resting State Cortical and White Matter Vascular … · 2017. 7. 24. · Neurosci. Osp....
16
Uncorrected Author Proof Journal of Alzheimer’s Disease 25 (2011) 1–16 DOI 10.3233/JAD-2011-101710 IOS Press 1 Resting State Cortical Electroencephalographic Rhythms and White Matter Vascular Lesions in Subjects with Alzheimer’s Disease: An Italian Multicenter Study 1 2 3 4 5 Claudio Babiloni a,b,∗ , Roberta Lizio c , Filippo Carducci d , Fabrizio Vecchio e , Alberto Redolfi f , Silvia Marino g , Gioacchino Tedeschi h,i , Patrizia Montella h , Antonio Guizzaro h , Fabrizio Esposito, j , Alessandro Bozzao k , Franco Giubilei k , Francesco Orzi k , Carlo C. Quattrocchi l , Andrea Soricelli m , Elena Salvatore m , Annalisa Baglieri g , Placido Bramanti g , Marina Boccardi f , Raffaele Ferri n , Filomena Cosentino n , Michelangelo Ferrara n , Ciro Mundi o , Gianpaolo Grilli o , Silvia Pugliese d , Gianluca Gerardi d , Laura Parisi e , Fabrizio Vernieri l , Antonio I.Triggiani a , Jan T. Pedersen p , Hans-G¨ oran H˚ ardemark q , Paolo M. Rossini b,r and Giovanni B. Frisoni f 6 7 8 9 10 11 12 a Department of Biomedical Sciences, University of Foggia, Foggia, Italy 13 b Department of Imaging, SAN RAFFAELE Cassino, Italy 14 c IRCCS San Raffaele Pisana, Rome, Italy 15 d Laboratory of Computational Neuroanatomy, Department of Physiology and Pharmacology, University of Rome “Sapienza”, Rome, Italy 16 17 e A.Fa.R., Dip. Neurosci. Osp. FBF; Isola Tiberina, Rome, Italy 18 f IRCCS “S. Giovanni di Dio-F.B.F.”, Brescia, Italy 19 g IRCCS Centro Neurolesi “Bonino-Pulejo” – Messina, Italy 20 h Department of Neurological Sciences, Second University of Naples, Naples, Italy 21 i Neurological Institute for Diagnosis and Care “Hermitage Capodimonte”, Naples, Italy 22 j Department of Neuroscience, University of Naples “Federico II”, Naples, Italy 23 k Azienda Ospedaliera Sant’Andrea Universit` a di Roma “Sapienza”, Roma, Italy 24 l IRCCS “Ospedale Pediatrico Bambino Ges` u”, Roma, Italy 25 m Fondazione SDN per la Ricerca e l’Alta Formazione in Diagnostica Nucleare, IRCCS Naples, Italy 26 n IRCCS Oasi, Troina (Enna), Italy 27 o Department of Neuroscience, Ospedali Riuniti di Foggia, Foggia, Italy 28 p Section head, Bioinformatics, H. Lundbeck A/S, Valby, Denmark 29 q Astrazeneca, Stockholm, Swerige 30 r Neurol. University “Campus Biomedico” Rome, Italy 31 Accepted 9 April 2011 ∗ Correspondence to: Prof. Claudio Babiloni, PhD, Department of Biomedical Sciences, University of Foggia, Viale Pinto 7, Fog- gia I-71100, Italy. Tel. and Fax: +39 0881 713276 (1716); E-mail: [email protected]. ISSN 1387-2877/11/$27.50 © 2011 – IOS Press and the authors. All rights reserved
Transcript of IOS Press Resting State Cortical and White Matter Vascular … · 2017. 7. 24. · Neurosci. Osp....

Unc
orre
cted
Aut
hor P
roof
Journal of Alzheimer’s Disease 25 (2011) 1–16DOI 10.3233/JAD-2011-101710IOS Press
1
Resting State CorticalElectroencephalographic Rhythmsand White Matter Vascular Lesionsin Subjects with Alzheimer’s Disease:An Italian Multicenter Study
1
2
3
4
5
Claudio Babilonia,b,∗, Roberta Lizioc, Filippo Carduccid, Fabrizio Vecchioe, Alberto Redolfif ,Silvia Marinog, Gioacchino Tedeschih,i, Patrizia Montellah, Antonio Guizzaroh, Fabrizio Esposito, j,Alessandro Bozzaok, Franco Giubileik, Francesco Orzik, Carlo C. Quattrocchil, Andrea Soricellim,Elena Salvatorem, Annalisa Baglierig, Placido Bramantig, Marina Boccardif , Raffaele Ferrin,Filomena Cosentinon, Michelangelo Ferraran, Ciro Mundio, Gianpaolo Grillio, Silvia Pugliesed,Gianluca Gerardid, Laura Parisie, Fabrizio Vernieril, Antonio I.Triggiania, Jan T. Pedersenp,Hans-Goran Hardemarkq, Paolo M. Rossinib,r and Giovanni B. Frisonif
6
7
8
9
10
11
12
aDepartment of Biomedical Sciences, University of Foggia, Foggia, Italy13
bDepartment of Imaging, SAN RAFFAELE Cassino, Italy14
cIRCCS San Raffaele Pisana, Rome, Italy15
dLaboratory of Computational Neuroanatomy, Department of Physiology and Pharmacology,University of Rome “Sapienza”, Rome, Italy
16
17
eA.Fa.R., Dip. Neurosci. Osp. FBF; Isola Tiberina, Rome, Italy18
f IRCCS “S. Giovanni di Dio-F.B.F.”, Brescia, Italy19
gIRCCS Centro Neurolesi “Bonino-Pulejo” – Messina, Italy20
hDepartment of Neurological Sciences, Second University of Naples, Naples, Italy21
iNeurological Institute for Diagnosis and Care “Hermitage Capodimonte”, Naples, Italy22
jDepartment of Neuroscience, University of Naples “Federico II”, Naples, Italy23
kAzienda Ospedaliera Sant’Andrea Universita di Roma “Sapienza”, Roma, Italy24
lIRCCS “Ospedale Pediatrico Bambino Gesu”, Roma, Italy25
mFondazione SDN per la Ricerca e l’Alta Formazione in Diagnostica Nucleare, IRCCS Naples, Italy26
nIRCCS Oasi, Troina (Enna), Italy27
oDepartment of Neuroscience, Ospedali Riuniti di Foggia, Foggia, Italy28
pSection head, Bioinformatics, H. Lundbeck A/S, Valby, Denmark29
qAstrazeneca, Stockholm, Swerige30
rNeurol. University “Campus Biomedico” Rome, Italy31
Accepted 9 April 2011
∗Correspondence to: Prof. Claudio Babiloni, PhD, Departmentof Biomedical Sciences, University of Foggia, Viale Pinto 7, Fog-gia I-71100, Italy. Tel. and Fax: +39 0881 713276 (1716); E-mail:[email protected].
ISSN 1387-2877/11/$27.50 © 2011 – IOS Press and the authors. All rights reserved

Unc
orre
cted
Aut
hor P
roof
2 C. Babiloni et al. / EEG and Vascular Lesion in AD
Abstract. Resting state electroencephalographic (EEG) rhythms do not deteriorate with the increase of white matter vascularlesion in amnesic mild cognitive impairment (MCI) subjects [1], although white matter is impaired along Alzheimer’s disease(AD). Here we tested whether this is true even in AD subjects. Closed-eye resting state EEG data were recorded in 40 healthyelderly (Nold), 96 amnesic MCI, and 83 AD subjects. White matter vascular lesions were indexed by magnetic resonance imagingrecorded in the MCI and AD subjects (about 42% of cases following ADNI standards). The MCI subjects were divided into twosub-groups based on the median of the white matter lesion, namely MCI+ (people with highest vascular load; n = 48) and MCI−(people with lowest vascular load; n = 48). The same was true for the AD subjects (AD+, n = 42; AD−, n = 41). EEG rhythms ofinterest were delta (2–4 Hz), theta (4–8 Hz), alpha1 (8–10.5 Hz), alpha2 (10.5–13 Hz), beta1 (13–20 Hz), beta2 (20–30 Hz), andgamma (30–40 Hz). LORETA software estimated cortical EEG sources. When compared to Nold group, MCI and AD groupsshowed well known abnormalities of delta and alpha sources. Furthermore, amplitude of occipital, temporal, and limbic alpha 1sources were higher in MCI+ than MCI− group. As a novelty, amplitude of occipital delta sources was lower in AD+ than AD−group. Furthermore, central, parietal, occipital, temporal, and limbic alpha sources were higher in amplitude in AD+ than AD−group. Amplitude of these sources was correlated to global cognitive status (i.e., Mini Mental State Evaluation score). Theseresults suggest that in amnesic MCI and AD subjects, resting state posterior delta and alpha EEG rhythms do not deterioratewith the increase of white-matter vascular lesion. These rhythms might be more sensitive to AD neurodegenerative processesand cognitive status rather than to concomitant lesions to white matter.
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
Keywords: Alzheimer’s disease, Alzheimer’s disease neuroimaging initiative, amnesic mild c cognitive impairment, electroen-cephalographic rhythms, low resolution brain electromagnetic tomography, magnetic resonance imaging, resting state, whitematter vascular lesion48
49
50
INTRODUCTION32
Previous studies in Alzheimer’s disease (AD) and33
amnesic mild cognitive impairment (MCI) subjects34
have shown that resting state closed-eye EEG rhythms35
may be promising markers of disease when evaluated36
by quantitative methods. When compared to normal37
elderly (Nold) subjects, AD patients have been char-38
acterized by high power of delta (0–4 Hz) and theta39
(4–7 Hz) rhythms, and low power of posterior alpha40
(8–12 Hz) and/or beta (13–30 Hz) rhythms [2–8]. In41
line with the “transition” hypothesis, amnesic MCI42
subjects have displayed increased theta power [9–11]43
as well as decreased alpha power [4, 8, 10–15]. Further-44
more, power of resting state alpha rhythms in amnesic45
MCI subjects has been found to be intermediate with46
respect to that of Nold and AD subjects [6, 12, 14].47
A bulk of previous evidence indicates that power48
of resting state eyes closed EEG rhythms reflect neu-49
rodegenerative processes in amnesic MCI and AD50
subjects [4, 8, 9, 12, 14, 16]. First, in MCI and AD sub-51
jects, abnormalities of EEG rhythms were associated to52
typical signs of neurodegeneration such as hippocam-53
pal atrophy [17] and impairment of the cholinergic54
tracts from basal forebrain to cerebral cortex [17, 18].55
Second, these abnormalities were also associated to56
altered regional cerebral blood flow/metabolism and57
to impaired global cognitive function in MCI or AD58
subjects [1, 6, 14, 19–21]. Third, decrement of pos-
terior alpha power showed peculiar features in AD 59
subjects when compared to cerebrovascular demen- 60
tia subjects with similar cognitive impairment [7]. 61
Fourth, posterior alpha power was relatively preserved 62
in amnesic MCI subjects in whom cognitive decline 63
was mainly explained by white-matter vascular lesion, 64
thus suggesting that these rhythms are less affected 65
by diffuse white matter vascular lesions than parallel 66
neurodegenerative processes [1, 23]. This hypothe- 67
sis is in line with recent evidence showing that there 68
were fewer neurodegenerative lesions in AD patients 69
with vascular lesions than in those without vascular 70
lesions, suggesting that neurodegenerative and cere- 71
brovascular lesions act as additive/synergistic causes 72
of AD [24–26]. On the other hand, several field studies 73
have reported some interactions between AD and cere- 74
brovascular function. Clinical and cognitive status of 75
AD patients was in part explained by amyloid angiopa- 76
thy of small vessels [27]. Furthermore, AD patients 77
carrying ApoE4 allele as a genetic risk of AD presented 78
an increment of intima-media thickness values with 79
respect to non-carriers and cerebrovascular dementia 80
patients [28]. Finally, evolution of cognitive function 81
in AD was unfavorable as a function of impaired cere- 82
bral vasomotor reactivity [29]. Keeping in mind these 83
data and considerations, current evidence suggests that 84
cerebrovascular dysfunction precedes and accompa- 85
nies cognitive dysfunction and AD neurodegeneration, 86
although its impact on the abnormalities of resting state 87

Unc
orre
cted
Aut
hor P
roof
C. Babiloni et al. / EEG and Vascular Lesion in AD 3
Table 1Demographic and clinical data of healthy elderly (Nold), mild cognitive impairment (MCI), and mild Alzheimer’s disease (AD) subjects
Subjects (n) Gender (M/F) Age (years) MMSE IAF (Hz) IADL CDR
Nold 40 22/18 72.1 ± (1.0) 27.7 ± (0.2 SE) 9.3 ± (0.2) – –MCI 96 32/64 71.4 ± (1.0) 25.9 ± (0.3 SE) 9.5±(0.1) 2.3 (±0.1 SE) 0.3 (±0.06 SE)AD 83 25/58 69.8 ± (0.8) 19.6 ± (0.5 SE) 8.8 ± (0.2) 4.5 (±0.3 SE) 1.0 (±0.1 SE)
EEG rhythms in AD might be negligible. To address88
to this issue, the present study tested the hypothesis89
that in both amnesic MCI and AD subjects, posterior90
resting state EEG rhythms do not deteriorate with the91
increase of white-matter vascular lesion, according to92
the idea that these rhythms are less affected by such93
vascular than neurodegenerative processes.94
METHODS95
Subjects96
In this study, 96 amnesic MCI subjects and 8397
AD patients were recruited. Furthermore, 40 cogni-98
tively intact elderly (Nold) subjects were selected as99
a control group. The Nold subjects globally matched100
the personal variables of the MCI and AD subjects.101
Table 1 reports demographic and clinical data of the102
AD, amnesic MCI, and Nold groups.103
The study was approved by the local Institutional104
ethics committee, and follows prescriptions of the105
Good Clinical Practice (GCP); informed and overt con-106
sent of subjects or subjects’ legal representatives, in107
line with the Code of Ethics of the World Medical108
Association (Declaration of Helsinki) and the stan-109
dards established by the Author’s Institutional Review110
Board.111
Diagnostic criteria112
The present inclusion and exclusion criteria for113
amnesic MCI subjects were based on international114
standards [30–39]. Summarizing, the inclusion criteria115
were as follows: (i) objective memory impairment on116
ADNI neuropsychological evaluation probing cogni-117
tive performance in the domains of memory, language,118
executive function/attention, etc; (ii) normal activities119
of daily living as documented by the history and evi-120
dence of independent living; and (iii) clinical dementia121
rating score of 0.5.122
The exclusion criteria included: (i) mild dementia123
of the AD type, as diagnosed by standard proto-124
cols including NINCDS-ADRDA [40] and DSM-IV;125
(ii) evidence (including magnetic resonance imag-126
ing – MRI – procedures) of concomitant cerebral 127
impairment such as frontotemporal degeneration, cere- 128
brovascular disease with large vascular lacunar lesions 129
in gray or white matter, and reversible cognitive 130
impairment (including pseudo-depressive dementia); 131
(iii) marked fluctuations in cognitive performance 132
compatible with Lewy body dementia and/or features 133
of mixed cognitive impairment including cerebrovas- 134
cular disease (particular attention was devoted to this 135
point given the working hypothesis focused on cog- 136
nitive stability in MCI subjects); (iv) evidence of 137
concomitant extra-pyramidal symptoms; (v) clinical 138
and indirect evidence of depression as revealed by the 139
Geriatric Depression Scale (GDS; [41]) scores >14; 140
(vi) other psychiatric diseases, epilepsy, drug addic- 141
tion, alcohol dependence (as revealed by a psychiatric 142
interview) and use of psychoactive drugs including 143
acetylcholinesterase inhibitors or other drugs enhanc- 144
ing brain cognitive functions; and (vii) current or 145
previous uncontrolled or complicated systemic dis- 146
eases (including diabetes mellitus) or traumatic brain 147
injuries. 148
Probable AD was diagnosed according to NINCDS- 149
ADRDA [40] and DSM IV criteria. The recruited AD 150
patients underwent general medical, neurological, neu- 151
ropsychological, and psychiatric assessments. Patients 152
were rated with a number of standardized diagnostic 153
and severity instruments that included Mini Mental 154
State Evaluation (MMSE; [42]), Clinical Demen- 155
tia Rating Scale (CDR; [43]), GDS [41], Hachinski 156
Ischemic Score (HIS, [44]), and Instrumental Activi- 157
ties of Daily Living scale (IADL, [45]). Neuroimaging 158
diagnostic procedures (MRI) and complete laboratory 159
analyses were carried out to exclude other causes of 160
progressive or reversible dementias. Exclusion criteria 161
included any evidence of (i) frontotemporal dementia, 162
diagnosed according to current criteria [46], (ii) MRI 163
of cerebrovascular disease with large vascular lacunar 164
lesions in gray or white matter (iii) vascular demen- 165
tia, diagnosed according to NINDS-AIREN criteria 166
[47], (iv) extra-pyramidal syndromes, (iv) reversible 167
dementias (including pseudodementia of depression); 168
and (v) Lewy body dementia, according to the criteria 169
by [48]. 170

Unc
orre
cted
Aut
hor P
roof
4 C. Babiloni et al. / EEG and Vascular Lesion in AD
The present Nold subjects were recruited mostly171
from non-consanguineous patients’ relatives. All Nold172
subjects underwent physical and neurological exam-173
inations as well as cognitive screening (including174
MMSE and GDS). Subjects affected by chronic sys-175
temic illnesses, those receiving psychoactive drugs, or176
with a history of neurological or psychiatric disease177
were excluded. All Nold subjects had a GDS score178
lower than 14 (no depression).179
Magnetic Resonance Imaging (MRI)180
Three-D proton density (PD), T1- and T2-weighted181
volumetric MRIs were recorded by the clinical units182
of the present Italian multi-centric study (University183
of Foggia-Ospedali Riuniti di Foggia; San Raffaele184
Cassino; Isola Tiberina Fatebenefratelli Hospital,185
Rome; IRCCS Fatebenefratelli Brescia; IRCCS Centro186
Neurolesi, Messina; Azienda Ospedaliera Sant’Andrea187
University of Rome “Sapienza”; University of Naples188
“Federico II”; Second University of Naples; Uni-189
versity “Campus Biomedico” Rome; IRCCS and190
Fondazione SDN Naples; IRCCS Oasi, Troina). Some191
of these units (IRCCS Centro Neurolesi “Bonino-192
Pulejo”, Messina; Azienda Ospedaliera Sant’Andrea193
University of Rome “Sapienza”; University of Naples194
“Federico II”; Second University of Naples; University195
“Campus Biomedico” Rome; IRCCS and Fondazione196
SDN Naples; IRCCS Oasi, Troina) collected the197
MRIs following the ADNI protocol (http://www.adni-198
info.org/). In total, about 42% of the whole dataset was199
collected according to the ADNI project.200
Analysis of the 3-D PD, T1-, and T2-weighted vol-201
umetric MRIs was centralized at University of Rome202
“Sapienza”. The MRIs were visually inspected to ver-203
ify the absence of structural abnormalities or technical204
artifacts. Afterwards, they were given as an input to205
Expectation-Maximization Segmentation (EMS) soft-206
ware, which is an SPM99 tool (Wellcome Dept. Cogn.207
Neurol., London; http://www.fil.ion.ucl.ac.uk/spm)208
running under MATLAB 7.0 (MathWorks, Natick,209
MA). On the whole, the EMS tool performs (i) an auto-210
mated, atlas-based classification of brain tissue from211
3-D PD, T1- and T2-weighted volumetric MRIs, (ii)212
builds a stochastic individual model of “normal” tis-213
sue intensity at voxel level on the basis of all MRIs, (iii)214
detects voxels with “vascular lesion” by the computa-215
tion of the Mahalanobis distance. In detail, individual216
MRIs were corrected for field inhomogeneities and217
coregistered each other. The coregistered MRIs were218
normalized to the SPM99 T1 template, which allowed219
the classification of the voxels into three compartments220
including gray matter, white matter or cerebral-spinal 221
fluid. Afterwards, the EMS tool estimated the param- 222
eters of a stochastic model of tissue intensity for 223
“normal” brain MRIs in each individual normalized 224
dataset. Tissue intensities for the “normal” brain model 225
were represented with a 3-classes (i.e., gray matter, 226
white matter, and cerebral-spinal fluid) finite multi- 227
variate Gaussian mixture. All MRI sequences (i.e., 228
3-D PD, T1-, and T2-weighted) were used to create 229
a multidimensional feature space, in order to benefit 230
of the specific inherent information of each sequence. 231
These sequences were iteratively classified into a small 232
number of Gaussian distributions. During this iterative 233
process, the EMS tool rejected voxels that exceed a 234
predefined Mahalanobis distance to each of the Gaus- 235
sians, and updated the model parameters only based 236
on non-rejected voxels [49]. Vascular lesion of white 237
matter was defined as the amount of voxels classified 238
as affected by vascular lesion and rejected from the 239
stochastic model of “normal brain”, according to the 240
mentioned Mahalanobis distance. In this framework, 241
the use of Markov random fields (MRF) discouraged a 242
voxel to be classified as brain lesion in the absence of 243
neighboring white matter. 244
Of note, the EMS tool implements an automated 245
procedure that requires only the Mahalanobis distance 246
threshold parameter (k) to be computed on the basis 247
of a variable defined by the experiment; namely, the 248
parameter k determined the significance level at which 249
voxels are considered as model outliers. An appropri- 250
ate k value had to be chosen in advance by means of an 251
experimentally tuned procedure, because of the choice 252
of k significantly affects the quality of the brain lesion 253
segmentation [49, 50]. The optimal value of the param- 254
eter k was identified on 36 MRI individual datasets. 255
The MRI segmentations were obtained with the auto- 256
matic tool varying the values of k from 3.0 to 5.0 with 257
steps of 0.5. The results were correlated to those of the 258
MRI segmentation performed by our expert neurora- 259
diologists. The highest correlation was obtained with 260
parameter k equal to 4.0 (Pearson r = 0.7; p = 0.001), 261
which is exactly the threshold value suggested by the 262
researcher who developed the EMS tool for the detec- 263
tion of vascular lesions in multiple sclerosis patients 264
(http://www.medicalimagecomputing.com). 265
Based on the above procedure for the estimation 266
of white-matter vascular lesions, the MCI subjects 267
were divided into two sub-groups. The median of the 268
white matter lesion was used as the criterion of the 269
definition of MCI people with highest vascular load 270
or MCI + (≥4960 voxels; mean of 7479 voxels ± 483 271
standard error, SE; n = 48) and of MCI people with 272

Unc
orre
cted
Aut
hor P
roof
C. Babiloni et al. / EEG and Vascular Lesion in AD 5
Table 2Demographic and clinical data of the following sub-groups: AD with low degree of white-matter lesion (AD−, normalized white-matter vascularlesions <3430); AD with high degree of white-matter lesion (AD+, normalized white-matter vascular lesions ≥3430); MCI with low degreeof white-matter lesion (MCI−, normalized white-matter vascular lesions <4960) and MCI with high degree of white-matter lesion (MCI+,
normalized white-matter vascular lesions ≥4960)
Subjects (n) Gender (M/F) Age (years) MMSE IAF (Hz) White matter vascularlesion (voxels)
MCI+ 48 16/32 69.6 ± (1.2 SE) 26.5 ± (0.4 SE) 9.6 ± (0.2 SE) 7479 ± (483 SE)MCI− 48 16/32 70.1 ± (1.0 SE) 25.4 ± (0.4 SE) 9.3 ± (0.2 SE) 3332 ± (179 SE)AD+ 42 13/29 72.2 ± (1.2 SE) 21.0 ± (0.6 SE) 8.9 ± (0.2 SE) 8744 ± (1295 SE)AD− 41 12/29 70.6 ± (1.5 SE) 18.4 ± (0.8 SE) 8.7 ± (0.3 SE) 2298 ± (107 SE)
lowest vascular load or MCI− (<4960 voxels; mean273
of 3332 voxels ± 179 SE; n = 48). The same crite-274
rion based on the median of the white matter lesion275
was used to divide AD subjects into the sub-groups276
of AD+ (≥3430 voxels; mean of 8744 voxels ± 1295277
SE; n = 42) and AD− (<3430 voxels; mean of 2298278
voxels ± 107 SE; n = 41). Table 2 reports demographic279
and clinical data of the AD−, AD+, MCI−, and MCI+280
sub-groups.281
EEG recordings282
Resting state eyes closed EEG data were recorded283
(0.3–70 Hz bandpass) from 19 electrodes positioned284
according to the international 10–20 system (i.e. Fp1,285
Fp2, F7, F3, Fz, F4, F8, T3, C3, Cz, C4, T4, T5, P3,286
Pz, P4, T6, O1, O2) and referenced to linked earlobes287
or cephalic reference. To monitor eye movements, the288
horizontal and vertical electrooculogram (0.3– 70 Hz289
bandpass) was simultaneously recorded. All data were290
digitized in continuous recording mode (about 5 min291
of EEG; 128–512 Hz sampling rate, the sampling rate292
being fixed in each recording research unit of this293
multi-centric study). In all subjects, EEG recordings294
were performed in the late morning. In order to keep295
constant the level of vigilance, an operator controlled296
on-line the subject and the EEG traces, verbally alert-297
ing the subject any time there were signs of behavioral298
and/or EEG drowsiness.299
Preliminary analysis of the EEG data300
The recorded EEG data were segmented and ana-301
lyzed off-line in consecutive 2 s epochs. The EEG302
epochs with ocular, muscular, and other types of arti-303
facts were preliminarily identified by a computerized304
automatic procedure. EEG epochs with sporadic blink-305
ing artifacts (less than 15% of the total) were then306
corrected by an autoregressive method [51]. Two inde-307
pendent experimenters – blind to the diagnosis at the308
time of the EEG analysis – manually confirmed the309
EEG segments accepted for further analysis. Finally, 310
we re-referenced artifact free EEG data to common 311
average for further analysis. 312
Spectral analysis of the EEG data 313
The digital FFT-based power spectrum analysis 314
(Welch technique, Hanning windowing function, no 315
phase shift) was evaluated in order to calculate the 316
individual alpha frequency (IAF) peak, defined as the 317
frequency associated to the strongest EEG power at 318
the extended alpha range of 6–13 Hz [53]. Mean IAF 319
peak was 9.3 Hz (±0.2 SE) in the Nold subjects, 9.5 Hz 320
(±0.1 SE) in the MCI subjects, and 8.8 Hz (±0.2 SE) in 321
the AD subjects. No statistically significant ANOVA 322
differences were found (p > 0.05). However, the IAF 323
peak was used as a covariate (together with age, gender, 324
recording unit site, and use or not of the ADNI protocol 325
in the statistics analyses. Indeed, the IAF is a frequency 326
of special importance, since it is associated with maxi- 327
mum power of resting eyes-closed EEG rhythms [52]. 328
The above procedure minimized the possibility that 329
small differences in the IAF peak could confound the 330
comparisons among the Nold, MCI, and AD groups. 331
The standard frequency bands of interest were delta 332
(2–4 Hz), theta (4–8 Hz), alpha 1 (8–10.5 Hz), alpha 333
2 (10.5–13 Hz), beta 1 (13–20 Hz), beta 2 (20–30 Hz) 334
and gamma (30–40 Hz), in continuity with a bulk of 335
reference previous studies on the cortical sources of 336
resting EEG rhythms in pathological aging [8, 14, 337
53–56]. Choice of the fixed EEG bands did not account 338
for IAF peak. However, this should not affect the 339
results, since more than 90% of the subjects had the 340
IAF peaks within the alpha 1 band (8–10.5 Hz) and the 341
IAF was used as a covariate in the statistical analysis. 342
Cortical source of EEG rhythms as computed 343
by LORETA 344
Low resolution electromagnetic source tomogra- 345
phy (LORETA) as provided at http://www.unizh. 346

Unc
orre
cted
Aut
hor P
roof
6 C. Babiloni et al. / EEG and Vascular Lesion in AD
ch/keyinst/NewLORETA/LORETA01.htm was used347
for the estimation of cortical sources of EEG rhythms348
[57–59]. LORETA is a functional imaging technique349
belonging to a family of linear inverse solution proce-350
dures [60] modeling 3D distributions of EEG sources351
[59]. With respect to the dipole modeling of cortical352
sources, no a priori decision of the dipole position is353
required by LORETA procedure. LORETA belongs to354
the family of linear inverse algorithms like minimum355
norm solution, weighted minimum norm solution or356
weighted resolution optimization [58, 61, 62], and has357
been successfully used in recent EEG studies on patho-358
logical brain aging using the same experimental set359
up (electrode montage, sample frequency, etc.) of the360
present study [3, 7, 14, 53–56].361
LORETA computes 3D linear solutions (LORETA362
solutions) for the EEG inverse problem within a 3-shell363
spherical head model including scalp, skull, and brain364
compartments. The brain compartment is restricted to365
the cortical gray matter/hippocampus of a head model366
co-registered to the Talairach probability brain atlas367
and digitized at the Brain Imaging Center of the Mon-368
treal Neurological Institute [63]. This compartment369
includes 2394 voxels (7 mm resolution), each voxel370
containing an equivalent current dipole. Of note, EEG371
electrode positions were not co-registered to individ-372
ual brain source models; unfortunately, the official373
LORETA package did not include software to do so374
and we could not obtain the digitalization of the elec-375
trode position from our clinical units. LORETA can376
be used from EEG data recorded by low spatial sam-377
pling of 10–20 system (19 electrodes) when cortical378
sources are estimated from resting state eyes-closed379
EEG rhythms [1, 7, 14, 17, 23, 53–56, 64–71]. Indeed,380
resting state eyes-closed EEG rhythms are generated381
by coherent synchronous neural activity of large corti-382
cal areas (i.e., the summed activity of a large number383
of pyramidal neuron assemblies). As a result, these384
rhythms are characterized by low-spatial frequency385
content that can be properly sampled by the 19 scalp386
electrodes placed according to 10–20 system [72].387
LORETA solutions consisted of voxel z-current den-388
sity values able to predict EEG spectral power density389
at scalp electrodes, being a reference-free method of390
EEG analysis, in that one obtains the same LORETA391
source distribution for EEG data referenced to any392
reference electrode including common average. A nor-393
malization of the data was obtained by normalizing the394
LORETA current density at each voxel with the power395
density averaged across all frequencies (0.5–45 Hz)396
and across all 2394 voxels of the brain volume. After397
the normalization, the solutions lost the original physi-398
cal dimension and were represented by an arbitrary unit 399
scale. This procedure reduced inter-subjects variability 400
and was used in previous EEG studies [7, 14, 53–56]. 401
The general procedure fitted the LORETA solutions 402
in a Gaussian distribution and reduced inter-subject 403
variability [73, 74]. Other methods of normalization 404
using the principal component analysis are effective 405
for estimating the subjective global factor scale of the 406
EEG data [75]. These methods are not available in the 407
LORETA package, so they were not used in this study. 408
Solutions of the EEG inverse problem are under- 409
determined and ill conditioned when the number of 410
spatial samples (electrodes) is lower than that of the 411
unknown samples (current density at each voxel). 412
In order to properly address this problem, the corti- 413
cal LORETA solutions predicting scalp EEG spectral 414
power density were regularized to estimate distributed 415
rather than punctual EEG source patterns [57–59]. In 416
line with the low spatial resolution of the adopted tech- 417
nique, we used our MATLAB software to collapse all 418
voxels of LORETA solutions within each of the cortical 419
macroregions of interest (ROIs) such frontal, central, 420
parietal, occipital, temporal, and limbic regions of the 421
brain model. The belonging of a LORETA voxel to 422
a Brodmann area was defined by original LORETA 423
package. Table 3 lists the Brodmann areas (BAs) rep- 424
resented into each ROI. 425
A main advantage of the regional analysis of 426
LORETA solutions, using an explicit source model 427
coregistered into Talairach space, was that our mod- 428
eling could disentangle rhythms of contiguous cortical 429
areas (namely those from the occipital source were 430
disentangled with respect to those of the contiguous 431
parietal and temporal sources, etc). 432
Statistical analysis of the LORETA solutions 433
Statistical analysis aimed at evaluating two main 434
working hypotheses. These hypotheses were the fol- 435
lowing: (1) LORETA solutions of resting state cortical 436
Table 3Brodmann areas included in the cortical regions of interest (ROIs)of the present study. LORETA solutions were collapsed in frontal,
central, parietal, occipital, temporal, and limbic ROIs
LORETA Brodmann areas into the regionsof Interest (ROIs)
Frontal 8, 9, 10, 11, 44, 45, 46, 47Central 1, 2, 3, 4, 6Parietal 5, 7, 30, 39, 40, 43Temporal 20, 21, 22, 37, 38, 41, 42Occipital 17, 18, 19Limbic 31, 32, 33, 34, 35, 36

Unc
orre
cted
Aut
hor P
roof
C. Babiloni et al. / EEG and Vascular Lesion in AD 7
EEG rhythms show difference in amplitude among the437
Nold, MCI, and AD subjects; (2) LORETA solutions438
point to difference in amplitude between AD+ and439
AD− groups as well as between MCI+ and MCI−440
groups. The LORETA solutions showing such signif-441
icant differences are correlated to the cognitive status442
as revealed by MMSE score.443
To test the first working hypothesis, the LORETA444
solutions values were used as a dependent variable445
for an ANOVA design using subjects’ age, gender,446
MMSE, IAF peak, and recording unit site as covari-447
ates. The ANOVA factors (levels) were Group (Nold,448
MCI, AD), Band (delta, theta, alpha 1, alpha 2, beta449
1, beta 2, gamma), and ROI (frontal, central, parietal,450
occipital, temporal, limbic). Mauchly’s test evaluated451
the sphericity assumption. Correction of the degrees of452
freedom was made with the Greenhouse-Geisser pro-453
cedure. Duncan test was used for post-hoc comparisons454
(p < 0.05). Specifically, the working hypothesis would455
be confirmed by a statistical ANOVA effect includ-456
ing the factor Group (p < 0.05), and planned post-hoc457
testing showing differences in line with the pattern458
Nold /= MCI /= AD (p < 0.05).459
To test the second working hypothesis, the LORETA460
solutions values were used as a dependent variable for461
an ANOVA design using subjects’ age, gender, MMSE,462
IAF peak, and recording unit site as covariates. The463
ANOVA factors (levels) were Group (MCI+, MCI−,464
AD+, AD−), Band (delta, theta, alpha 1, alpha 2, beta465
1, beta 2, gamma), and ROI (frontal, central, parietal,466
occipital, temporal, limbic). Mauchly’s test evaluated467
the sphericity assumption. Correction of the degrees468
of freedom was made with the Greenhouse-Geisser469
procedure. Duncan test was used for post-hoc com-470
parisons (p < 0.05). The working hypothesis would be471
confirmed by a statistical ANOVA effect including the472
factor Group (p < 0.05), and planned post-hoc testing473
showing differences between AD+ and AD− groups474
as well as between MCI+ and MCI− groups. Finally,475
EEG sources showing these statistically significant dif-476
ferences as a function of the white matter vascular477
lesions were correlated to MMSE score in the con-478
tinuum of the MCI and AD subjects as a whole group479
(Pearson test, p < 0.05).480
Novelty of the present study481
This study is a part of larger scientific program on482
EEG markers of AD, yet it is well framed and dis-483
tinct from the previous studies of the Authors [7, 14,484
53–56]. Specifically, this is our first study examining485
the relationships between resting state EEG sources486
and white matter vascular lesions in AD. To address 487
this issue, we performed an unedited analysis of white 488
matter vascular lesions by EMS-SPM software in 83 489
AD patients and 96 amnesic MCI subjects, for the com- 490
parison of EEG sources between sub-groups of these 491
subjects with a different degree of white matter vascu- 492
lar lesion. Among these subjects, no AD patient and 64 493
amnesic MCI subjects had been previously used in the 494
reference investigations evaluating white matter vascu- 495
lar lesions by Wahlund visual rating scale [1, 23]. The 496
results of the present analysis are absolutely original 497
(i.e., never published before). 498
RESULTS 499
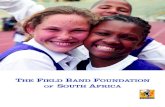
Figure 1 shows the grand average of regional 500
normalized LORETA solutions (i.e., relative power 501
current density averaged with each ROI)) relative to an 502
ANOVA interaction (F(60,6480) = 11.91; p < 0.0001) 503
among the factors Group (Nold, MCI, AD), Band 504
(delta, theta, alpha 1, alpha 2, beta 1, beta 2, gamma), 505
and ROI (frontal, central, parietal, occipital, tempo- 506
ral, limbic). Planned post-hoc testing indicated that 507
occipital alpha2 sources as well as parietal, occip- 508
ital, temporal, and limbic alpha 1 sources were 509
higher in amplitude in the Nold than MCI group 510
(p < 0.000005), and in the MCI than AD group 511
(p < 0.000005 to 0.000001); these results disclosed 512
the pattern Nold > MCI > AD for the parietal, occip- 513
ital, temporal, and limbic alpha 1 and occipital alpha2 514
sources. Furthermore, frontal, temporal, and limbic 515
delta sources were lower in amplitude in the Nold and 516
MCI than in the AD groups (p < 0.05). 517
Figure 2 maps the grand average of the normalized 518
LORETA solutions (i.e., relative power current den- 519
sity) modeling the distributed cortical EEG sources 520
for delta, theta, alpha 1, alpha 2, beta 1, beta 2, and 521
gamma bands in the AD−, AD+, MCI−, MCI+ groups. 522
Posterior alpha sources were generally higher in ampli- 523
tude in the AD+ or MCI+ than AD− or MCI− group, 524
whereas the opposite is true for the posterior delta 525
sources. 526
Figure 3 plots the grand average of regional normal- 527
ized LORETA solutions (i.e., relative power current 528
density averaged with each ROI) relative to an ANOVA 529
interaction (F(90,5250) = 3.50; p < 0.00001) among 530
the factors Group (AD−, AD+, MCI−, MCI+), Band 531
(delta, theta, alpha 1, alpha 2, beta 1, beta 2, gamma), 532
and ROI (frontal, central, parietal, occipital, tempo- 533
ral, limbic). Planned post-hoc testing indicated that 534
occipital, temporal, and limbic alpha 1 sources were 535

Unc
orre
cted
Aut
hor P
roof
8 C. Babiloni et al. / EEG and Vascular Lesion in AD
Fig. 1. Statistical ANOVA interaction (F(60,6480) = 11.91; p < 0.0001) among the factors Group (Nold, MCI, AD), Band (delta, theta, alpha 1,alpha 2, beta 1, beta 2, gamma), and ROI (frontal, central, parietal, occipital, temporal, limbic).
higher in amplitude in the MCI+ than MCI− group536
(p < 0.01 to 0.000001). Furthermore, occipital delta537
sources were higher in amplitude in the AD− than538
AD+ group (p < 0.01). Finally, central, parietal, occip-539
ital, temporal, and limbic alpha sources were higher540
in amplitude in the AD+ than AD− group (p < 0.05 to541
0.000001).542
The mentioned delta and alpha sources showing543
statistically significant differences (p < 0.05) as a func-544
tion of the white matter vascular lesions (i.e., MCI+545
or AD+ versus MCI− or AD−) were correlated546
to MMSE score in the continuum of the MCI and547
AD subjects as a whole group. There was a posi-548
tive correlation between MMSE score and any of the549
mentioned alpha sources at central (alpha 1, r = 0.18,550
p = 0.02; alpha 2, r = 0.20, p = 0.008), parietal (alpha551
1, r = 0.28, p = 0.0001; alpha 2, r = 0.32, p = 0.0001),552
occipital (alpha 1, r = 0.25, p = 0.001; alpha 2, r = 0.27,553
p = 0.0001), temporal (alpha 1, r = 0.31, p = 0.0001;554
alpha 2, r = 0.26, p = 0.001), and limbic (alpha 1, 555
r = 0.30, p = 0.0001; alpha 2, r = 0.30, p = 0.0001) 556
macroregions. The higher the MMSE score, the higher 557
the amplitude of alpha sources. Furthermore, there was 558
a negative correlation between MMSE score and occip- 559
ital delta sources (r = −0.31, p = 0.0001). The lower 560
the MMSE score, the higher the amplitude of occipital 561
delta sources.562
Control analyses 563
We performed some control analyses to ascertain if 564
the results of the main statistical analysis were affected 565
by relevant confounding variables. 566
In a first control analysis, we tested whether the 567
statistical results were influenced by the presence of 568
ADNI and non-ADNI subjects in the MCI and AD 569
groups. We divided the MCI and AD group in ADNI 570

Unc
orre
cted
Aut
hor P
roof
C. Babiloni et al. / EEG and Vascular Lesion in AD 9
Fig. 2. Grand average of LORETA solutions (i.e., normalized relative current density at the cortical voxels) modeling the distributed EEGsources for delta, theta, alpha 1, alpha 2, beta 1, beta 2, and gamma bands in Nold, MCI – (normalized white-matter vascular lesions < 4960),MCI+(normalized white-matter vascular lesions ≥4960), AD – (normalized white-matter vascular lesions < 3430), and AD+(normalized white-matter vascular lesions ≥3430) groups. The left side of the maps (top view) corresponds to the left hemisphere. Legend: LORETA, low resolutionbrain electromagnetic tomography. Color scale: all power density estimates were scaled based on the averaged maximum value (i.e., alpha 1power value of occipital region in Nold).
(18 MCI and 50 AD) and non-ADNI (78 MCI and571
33 AD). Statistical analysis of the LORETA source572
solutions showed no statistically significant difference573
(F(1.91) = 0.01; p < 0.9235) between MCI ADNI and574
MCI non-ADNI sub-groups. The same was true in575
AD patients, namely no statistically significant dif-576
ference (F(1.78) = 0.49; p < 0.4839) between the AD577
ADNI and AD non-ADNI sub-groups.578
In a second control analysis, we compared the Nold,579
MCI, and AD groups matched as number (40 AD,580
40 MCI, and 40 Nold subjects), mean age (AD = 69.5581
years; MCI = 69.8 years; Nold = 72.1 years), and mean582
IAF (AD = 8.6, MCI = 9.3, and Nold = 9.3 hertz). This 583
allowed a good control of the inter-groups variabil- 584
ity. The ANOVA design and covariates were those of 585
the main ANOVA design. The ANOVA factors were 586
Group (Nold, MCI, AD), Band (delta, theta, alpha 1, 587
alpha 2, beta 1, beta 2, gamma), and ROI (frontal, cen- 588
tral, parietal, occipital, temporal, limbic). The results 589
showed a statistically significant interaction among all 590
factors (F(60,3510) = 14.17; p < 0.0001). As expected, 591
ANOVA showed the well known abnormalities of delta 592
and alpha sources, in detail the results disclosed the pat- 593
tern Nold > MCI > AD for the parietal, occipital, and 594

Unc
orre
cted
Aut
hor P
roof
10 C. Babiloni et al. / EEG and Vascular Lesion in AD
Fig. 3. Statistical ANOVA interaction (F(90,5250) = 3.50; p < 0.00001) among the factors Group (AD−, AD+, MCI−, MCI+), Band (delta,theta, alpha 1, alpha 2, beta 1, beta 2, gamma), and ROI (frontal, central, parietal, occipital, temporal, limbic).
limbic alpha and temporal alpha1 sources. Further-595
more, frontal, occipital, and temporal delta sources596
were lower in amplitude in the Nold and MCI than597
in the AD groups (p < 0.05). These results globally598
confirmed those of the main analysis.599
In a third control analysis, we compared white matter600
vascular lesions between MCI+ versus MCI− groups601
as well as between AD+ versus AD− groups. As602
expected, ANOVA showed that there were significantly603
higher values of the white matter vascular lesions in the604
MCI+ than MCI− (p < 0.00001) as well as in the AD+605
than AD− subjects (p < 0.00001).606
A fourth control analysis accounted for the variabil-607
ity of the MMSE score across the groups, although608
the MMSE score was used as a covariate in the main609
ANOVA design. We selected sub-groups of AD−,610
AD+, MCI−, and MCI+ subjects to minimize the dif-611
ference of MMSE score between the AD− and AD+612
groups as well as between the MCI− and MCI+groups613
(Table 4). The ANOVA design and covariates were614
those of the main ANOVA design. The ANOVA factors 615
were Group (AD−, AD+, MCI−, MCI+; independent 616
variable), Band (delta, theta, alpha 1, alpha 2, beta 1, 617
beta 2, gamma), and ROI (central, frontal, parietal, 618
occipital, temporal, limbic). The results showed a 619
statistically significant interaction among all factors 620
(F(90,2700) = 2.81; p < 0.00001). Planned post-hoc 621
testing indicated that central and temporal alpha 1 622
sources were higher in amplitude in the MCI+ than 623
MCI− group (p < 0.05). Furthermore, occipital delta 624
sources were lower in amplitude in the AD+ than AD− 625
group (p < 0.05). Finally, central, parietal, occipital, 626
and temporal alpha 1 sources were higher in amplitude 627
in the AD+than AD− group (p < 0.01). These results 628
globally confirmed those of the main ANOVA design. 629
DISCUSSION 630
In the present study, we tested the novel hypothesis 631
that in AD subjects, resting state closed-eye EEG 632

Unc
orre
cted
Aut
hor P
roof
C. Babiloni et al. / EEG and Vascular Lesion in AD 11
Table 4Demographic and clinical data of the subjects’ sub-groups created to minimize the difference of MMSE between AD− and AD+ as well as
between MCI− and MCI+
Subjects (n) Gender (M/F) Age (years) MMSE IAF (Hz) White matter vascularlesion (voxels)
MCI+ 28 12/21 68.3 ± (1.5 SE) 26.3 ± (0.3 SE) 9.6 ± (0.2 SE) 7800 ± (713 SE)MCI− 28 13/20 69.0 ± (1.1 SE) 26.2 ± (0.3 SE) 9.5 ± (0.2 SE) 2973 ± (227 SE)AD+ 19 8/11 72.1 ± (1.8 SE) 19.5 ± (0.8 SE) 8.8 ± (0.3 SE) 9795 ± (2403 SE)AD− 19 7/12 70.1 ± (2.7 SE) 19.6 ± (0.8 SE) 8.4 ± (0.4 SE) 2231 ± (200 SE)
rhythms are not deteriorated due to the amount of633
white-matter vascular lesion, thus extending previous634
evidence in amnesic MCI subjects [1, 23]. To address635
this hypothesis, we estimated white matter vascular636
lesion with friendly and automated software (i.e., EMS637
tool of SPM) towards possible clinical applications.638
Such procedure was based on the use of PD, T1-,639
and T2-weighted MRIs recorded in amnesic MCI640
and AD subjects. Of note, we collected about 42%641
of the MRIs following the standards of the ADNI642
project (http://www.adni-info.org/), which aims at643
standardizing neuroimaging exams of aged people in644
multicenter AD studies on new markers and drugs.645
In this vein, we estimated cortical sources of resting646
state EEG rhythms by LORETA software, which can647
be freely downloaded by Internet (http://www.unizh.648
ch/keyinst/NewLORETA/LORETA01.htm), and has649
been successfully used by our Consortium in several650
field investigations [7, 14, 53–56].651
In the present study, results of the control statisti-652
cal analysis confirmed that the amnesic MCI subjects653
showed a decrease in amplitude of low-frequency alpha654
sources (8–10.5 Hz) compared to the Nold subjects.655
The AD subjects were characterized by an amplitude656
increase of delta sources (2–4 Hz), along with a strong657
amplitude reduction of low-frequency alpha sources.658
These findings are globally in line with previous evi-659
dence showing a pathological enhancement of the delta660
rhythms in AD subjects [7, 8, 76, 77], and a magnitude661
decrease of default alpha rhythms in MCI and/or AD662
subjects [2, 3, 7, 8, 15, 21, 22, 78]. Therefore, these663
control findings validated the present procedures for664
subjects’ selection and EEG data analysis, thus corrob-665
orating the novel results on the relationships between666
resting state EEG sources and white matter vascular667
lesions in AD subjects.668
Results of the main statistical analysis indicated that669
amplitude of posterior low-frequency alpha sources670
was higher in the amnesic MCI+ than MCI− group.671
As a novel finding, amplitude of occipital delta sources672
was lower in the AD+ than AD− group, whereas the673
opposite was true for central and posterior low- and 674
high-frequency alpha sources. These results suggest 675
that in AD subjects, central and posterior resting state 676
delta and alpha rhythms are not deteriorated with the 677
increase of white-matter vascular lesion, thus extend- 678
ing previous evidence on alpha sources in amnesic MCI 679
subjects [1, 23]. 680
Why were resting state EEG rhythms not deterio- 681
rated by the increase of white matter vascular lesions 682
in amnesic MCI and AD subjects? To answer to this 683
question, a brief overview on “normal” delta and 684
alpha rhythms is helpful. In the condition of slow- 685
wave sleep, corticofugal slow oscillations (<1 Hz) are 686
effective in grouping thalamic-generated delta rhythms 687
(1–4 Hz) and spindling activity (7–14 Hz) rhythms 688
[79]. In the condition of brain arousal, spindles as 689
well as high and low-frequency components of the 690
delta rhythms are blocked by the inhibition of oscilla- 691
tors within, respectively, reticulo-thalamic (7–14 Hz), 692
thalamo-cortical (1–4 Hz), and intracortical (<1 Hz) 693
neuronal circuits. These rhythms are replaced by fast 694
(beta and gamma) cortical oscillations, which are 695
mainly induced by forebrain (nucleus basalis) cholin- 696
ergic inputs to hippocampus and cortex as well as 697
by thalamocortical projections [79, 80]. In the con- 698
dition of awake rest, low-frequency (8–10.5 Hz) alpha 699
would be mainly related to subject’s global attentional 700
readiness [72, 81–84] and would mainly reflect time- 701
varying inputs of cortico-cortical and thalamo-cortical 702
pathways [85]. Noteworthy, there is consensus that 703
alpha rhythms represent the dominant resting oscil- 704
lations of the adult, awake human brain [72, 81–84], 705
and have been linked to intelligent quotient, memory, 706
and cognition [52]. Keeping in mind this physio- 707
logical premise, loss of synapses and neurons along 708
the well known tracks of AD neurodegeneration [86, 709
87] may deteriorate the synchronization of cortical 710
pyramidal neurons generating default alpha rhythms, 711
and may disinhibit pathological delta rhythms in the 712
condition of resting state. In this framework, diffuse 713
white matter vascular lesions may not specifically 714

Unc
orre
cted
Aut
hor P
roof
12 C. Babiloni et al. / EEG and Vascular Lesion in AD
impair the neural circuits responsible for the transfer715
of signals into brain pathways that generate resting716
state alpha rhythms and inhibit pathological delta717
rhythms.718
The present results support the notion that cere-719
brovascular and AD lesions do not represent additive720
or synergistic factors in the determination of the rest-721
ing state EEG abnormalities during the evolution of722
the disease, although these lesions contribute to the723
development of cognitive impairment in AD patients724
[24, 26, 88]. In AD, cognitive and clinical conditions725
are affected by the severity of both neurodegener-726
ative and cerebrovascular lesions in hippocampal,727
anterior cingulate gyrus, and parieto-temporal regions728
[89, 90–94]. Furthermore, these conditions depend on729
amyloid angiopathy of small vessels and on their struc-730
ture/function [27–29]. Current evidence suggests that731
there is decreased vascular density in aging and AD,732
with a cerebrovascular dysfunction that precedes and733
accompanies cognitive dysfunction and neurodegener-734
ation [95]. A decline in cerebrovascular angiogenesis735
typically inhibits recovery from hypoxia-induced cap-736
illary loss and cerebral blood flow may be inhibited by737
tortuous arterioles and deposition of excessive collagen738
in veins and venules [96]. In this framework, hypoper-739
fusion may occurs early in AD, inducing white matter740
lesions and correlating with dementia [95–99]. How-741
ever, resting state EEG abnormalities would be mainly742
affected by the AD neurodegenerative impairment of743
brain circuits, which may be not specifically targeted744
by diffuse white matter vascular lesions. Therefore, it745
can be speculated that resting state EEG rhythms might746
be more sensitive to neurodegenerative processes than747
cerebrovascular lesions in AD.748
In conclusion, we tested whether cortical synchro-749
nization mechanisms at the basis of resting state EEG750
rhythms are abnormal in AD subjects, as a function751
of vascular lesion of white matter. The present results752
showed that in both amnesic MCI and AD subjects,753
posterior delta and alpha sources did not deteriorate754
with the increase of white matter vascular lesion,755
although white matter is known to be impaired along756
AD neurodegenerative process. These results need to757
be validated with a follow-up study evaluating resting758
state EEG rhythms and white matter vascular lesion. In759
principle, the present results suggest that abnormalities760
of resting state EEG rhythms might be related to AD761
neurodegeneration specifically impinging on the brain762
circuits generating these rhythms and cognitive sta-763
tus rather than to white matter vascular lesion globally764
affecting the whole brain.765
ACKNOWLEDGMENTS 766
We thank Dr. Paul Suetens of Medical Image Com- 767
puting Group at KU Leuven, for providing software 768
EMS used for MRI data analysis. We also thank 769
Prof/Drs. Carla Buttinelli, Brunello Lecce, Anna- 770
maria Papantonio, Paolo Tisei, Antonella De Carolis, 771
Silvia Guidoni, Teresa Falco, Daniela Buonanno, 772
Manuela De Stefano, Federica Scrascia, Livia Quin- 773
tiliani, Simone Migliore, Daniela Cologno, Loreto 774
Gesualdo, Elena Ranieri, Ivan Cincione, Antonello 775
Bellomo, Annamaria Petito, Mario Altamura, Pietro 776
Fiore, Andrea Santamato, Tommaso Cassano, Dario 777
Colella, Giuseppe Cibelli, and Giancarlo Rossi-Fedele 778
for their excellent clinical, biometrics, tecnica, and 779
data analysis work. This research was developed 780
thank to the financial support of Tosinvest Sanita’ 781
(Cassino, Pisana) and Italian Ministry of Health 782
(Strategic research project entitled “Diagnosis of incip- 783
ient Alzheimer disease”) for the collection but not for 784
the analysis of the data reported in this manuscript. 785
The research leading to the present results has also 786
received funding from the European Community’s 787
Seventh Framework Programme (FP7/2007–2013) for 788
the Innovative Medicine Initiative under Grant Agree- 789
ment no 115009 (Prediction of cognitive properties 790
of new drug candidates for neurodegenerative dis- 791
eases in early clinical development, Pharmacog). It 792
was conducted as part of the analysis of “historical” 793
(archive) EEG and MRI data in control, amnesic MCI, 794
and AD subjects performed by two units of the Phar- 795
maCog Consortium, namely the University of Foggia 796
(Prof./Dr. Claudio Babiloni, Loreto Gesualdo, Elena 797
Ranieri, Ivan Cincione, Antonello Bellomo, Anna- 798
maria Petito, Mario Altamura, Pietro Fiore, Andrea 799
Santamato, Tommaso Cassano, Dario Colella, and 800
Gaetano Serviddio) and IRCCS Fatebenefratelli of 801
Brescia (Dr. Giovanni B. Frisoni, Marina Boccardi, 802
and Alberto Redolfi). PharmaCog funding was used 803
to support the analysis but not the collection of the 804
data reported in this manuscript. After a gentleman 805
agreement among all participants to this research, 806
only Prof./Dr. Claudio Babiloni, Fabrizio Vecchio, 807
Giovanni B. Frisoni, Marina Boccardi, and Alberto 808
Redolfi represented the PharmaCog Consortium in the 809
Author list. We thank Prof./Drs. Elaine irving, Gian- 810
luigi Forloni, Francesco Mattia Noe’, Tilman Hensch, 811
Oscar Dalla Pasqua, David Bartres-Faz, David Wille, 812
Giuseppe Bertini, and Paolo Fabene for a fruitful scien- 813
tific discussion of the results in the framework of the 814
PharmaCog Consortium. For further information on 815

Unc
orre
cted
Aut
hor P
roof
C. Babiloni et al. / EEG and Vascular Lesion in AD 13
the PharmaCog project please refer to www.alzheimer-816
europe.org.817
Authors’ disclosures available online (http://www.818
j-alz.com/disclosures/view.php?id=847).819
REFERENCES820
[1] Babiloni C, Frisoni GB, Pievani M, Toscano L, Del Percio C,821
Geroldi C, Eusebi F, Miniussi C, Rossini PM (2008) White-822
matter vascular lesions correlate with alpha EEG sources in823
mild cognitive impairment. Neuropsychologia 46, 1707-1720.824
[2] Dierks T, Ihl R, Frolich L, Maurer K (1993) Dementia of the825
Alzheimer type: effects on the spontaneous EEG described826
by dipole sources. Psychiatry Res 50, 51-162.827
[3] Dierks T, Jelic V, Pascual-Marqui RD, Wahlund LO, Julin828
P, Linden DEJ, Maurer K, Winblad B, Nordberg A (2000)829
Spatial pattern of cerebral glucose metabolism (PET) cor-830
relates with localization of intracerebral EEG-generators in831
Alzheimer’s disease. Clinical Neurophysiology 111, 1817-832
1824.833
[4] Huang C, Wahlund LO, Dierks T, Julin P, Winblad B, Jelic V834
(2000) Discrimination of Alzheimer’s disease and mild cogni-835
tive impairment by equivalent EEG sources: a cross-sectional836
and logitudinal study. Clin Neurophysiol 11, 1961-1967.837
[5] Ponomareva NV, Selesneva ND, Jarikov GA (2003) EEG838
alterations in subjects at high familial risk for Alzheimer’s839
disease. Neuropsychobiology 48, 152-159.840
[6] Jeong J (2004) EEG dynamics in patients with Alzheimer’s841
disease. Clin Neurophysiol 115, 1490-1505.842
[7] Babiloni C, Binetti G, Cassetta E, Cerboneschi D, Dal Forno843
G, Del Percio C, Ferreri F, Ferri R, Lanuzza B, Miniussi844
C, Moretti DV, Nobili, Pascual-Marqui RD, Rodriguez G,845
Romani GL, Salinari S, Tecchio F, Vitali P, Zanetti O, Zap-846
pasodi F, Rossini PM (2004) Mapping Distributed Sources847
of Cortical Rhythms in Mild Alzheimers Disease. A Multi-848
Centric EEG Study. NeuroImage 22, 57-67.849
[8] Koenig T, Prichep L, Dierks T, Hubl D, Wahlund LO,850
John ER, Jelic V (2005) Decreased EEG synchronization in851
Alzheimer’s disease and mild cognitive impairment. Neuro-852
biol Aging 26, 165-171.853
[9] Zappoli R, Versari A, Paganini M, Arnetoli G, Muscas GC,854
Gangemi PF, Arneodo MG, Poggiolini D, Zappoli F, Battaglia855
A (1995) Brain electrical activity (quantitative EEG and bit-856
mapping neurocognitive CNV components), psychometrics857
and clinical findings in presenile subjects with initial mild858
cognitive decline or probable Alzheimer-type dementia. Ital859
J Neurol Sci 16, 341-376.860
[10] Jelic V, Julin P, Shigeta M, Nordberg A, Lannfelt L, Win-861
blad B, Wahlund LO (1997) Apolipoprotein E epsilon4 allele862
decreases functional connectivity in Alzheimer’s disease as863
measured by EEG coherence. J Neurol Neurosurg Psychiatry864
63, 59-65.865
[11] Grunwald M, Busse F, Hensel A, Kruggel F, Riedel-Heller S,866
Wolf H, Arendt T, Gertz HJ (2001) Correlation between cor-867
tical theta activity and hippocampal volumes in health, mild868
cognitive impairment, and mild dementia. J Clin Neurophys-869
iol 18, 178-184.870
[12] Jelic V, Johansson SE, Almkvist O, Shigeta M, Julin P,871
Nordberg A, Winblad B, Wahlund LO (2000) Quantitative872
electroencephalography in mild cognitive impairment: lon-873
gitudinal changes and possible prediction of Alzheimer’s874
disease. Neurobiol Aging 21, 533-540.875
[13] Grunwald M, Busse F, Hensel A, Riedel-Heller S, Kruggel F, 876
Arendt T, Wolf H, Gertz HJ (2002) Theta-power differences in 877
patients with mild cognitive impairment under rest condition 878
and during haptic tasks. Alzheimer Dis Assoc Disord. Jan-Mar 879
16, 40-48. 880
[14] Babiloni C, Binetti G, Cassetta E, Dal Forno G, Del Percio C, 881
Ferreri F, Ferri R, Frisoni G, Hirata K, Lanuzza B, Miniussi C, 882
Moretti DV, Nobili F, Rodriguez G, Romani GL, Salinari S, 883
Rossini PM (2006) Sources of cortical rhythms change as 884
a function of cognitive impairment in pathological aging: A 885
multi-centric study. Clin Neurophysiol 117, 252-268. 886
[15] Rossini PM, Rossi S, Babiloni C, Polich J (2007) Clinical 887
neurophysiology of aging brain: from normal aging to neu- 888
rodegeneration. Prog Neurobiol 83, 375-400. 889
[16] Elmstahl S, Rosen I (1997) Postural hypotension and EEG 890
variables predict cognitive decline: results from a 5-year 891
follow-up of healthy elderly women. Dement Geriatr Cogn 892
Disord 8, 180-187. 893
[17] Babiloni C, Frisoni GB, Pievani M, Vecchio F, Lizio R, 894
Buttiglione M, Geroldi C, Fracassi C, Eusebi F, Ferri R, 895
Rossini PM (1) (2009a) Hippocampal volume and cortical 896
sources of EEG alpha rhythms in mild cognitive impairment 897
and Alzheimer disease. Neuroimage 44, 123-135. 898
[18] Babiloni C, Frisoni GB, Vecchio F, Pievani M, Geroldi C, 899
De Carli C, Ferri R, Vernieri F, Lizio R, Rossini PM (2010) 900
Global functional coupling of resting EEG rhythms is related 901
to white-matter lesions along the cholinergic tracts in subjects 902
with amnesic mild cognitive impairment. J Alzheimers Dis 19, 903
859-871. 904
[19] Sloan EP, Fenton GW, Kennedy NSJ, MacLennan JM (1995) 905
Electroencephalography and single photon emission com- 906
puted tomography in dementia: A comparative study. Psychol 907
Med 25, 631-638 908
[20] Rodriguez G, Nobili F, Rocca G, DeCarli F, Gianelli MV, 909
Rosadini G (1998) Quantitative electroencephalography and 910
regional cerebral blood flow: Discriminant analysis between 911
Alzheimer’s patients and healthy controls. Dement Geriatr 912
Cogn Disord 9, 238-274. 913
[21] Rodriguez G, Copello F, Vitali P, Perego G, Nobili F (1999) 914
EEG spectral profile to stage Alzheimer’s disease. Clin Neu- 915
rophysiol 110, 1831-1837. 916
[22] Rodriguez G, Nobili F, Copello F, Vitali P, Gianelli MV, 917
Taddei G, Catsafados E, Mariani G (1999) 99mTc-HMPAO 918
regional Cerebral Blood Flow and quantitative Electroen- 919
cephalography in Alzheimer’s disease: a correlative study. J 920
Nucl Med 40, 522-529. 921
[23] Babiloni C, Frisoni GB, Pievani M, Vecchio F, Infarinato 922
F, Geroldi C, Salinari S, Ferri R, Fracassi C, Eusebi F, 923
Rossini PM (2008) White matter vascular lesions are related to 924
parietal-to-frontal coupling of EEG rhythms in mild cognitive 925
impairment. Hum Brain Mapp 29, 1355-1367. 926
[24] Snowdon DA, Greiner LH, Mortimer JA, Riley KP, Greiner 927
PA, Markesbery WR (1997) Brain infarction and the clinical 928
expression of Alzheimer disease. The Nun Study, JAMA 277, 929
813-817. 930
[25] Nagy Z, Esiri MM, Jobst KA, Morris JH, King EM-F, 931
McDonald B, Joachim C, Litchfield S, Barnetson L, Smith 932
AD (1997) The effects of additional pathology on the cogni- 933
tive deficit in Alzheimer disease, J Neuropathol Exp Neurol 934
56, 165-170 935
[26] Zekry D, Duyckaerts C, Moulias R, Belmin J, Geoffre C, Her- 936
rmann F, Hauw JJ (2002) Degenerative and vascular lesions 937
of the brain have synergistic effects in dementia of the elderly. 938
Acta Neuropathol 103, 481-487. 939

Unc
orre
cted
Aut
hor P
roof
14 C. Babiloni et al. / EEG and Vascular Lesion in AD
[27] Zekry D, Duyckaerts C, Belmin J, Geoffre C, Herrmann F,940
Moulias R, Hauw JJ (Aging) (2003) The vascular lesions941
in vascular and mixed dementia: The weight of functional942
neuroanatomy. Neurobiol Aging 24, 213-219.943
[28] Altamura C, Squitti R, Pasqualetti P, Tibuzzi F, Silvestrini M,944
Ventriglia MC, Cassetta E, Rossini PM, Vernieri F (2007)945
What is the relationship among atherosclerosis markers,946
apolipoprotein E polymorphism and dementia? Eur J Neurol947
14, 679-682.948
[29] Silvestrini M, Pasqualetti P, Baruffaldi R, Bartolini M, Han-949
douk Y, Matteis M, Moffa F, Provinciali L, Vernieri F. (2006)950
Cerebrovascular reactivity and cognitive decline in patients951
with Alzheimer disease, Stroke 37, 1010-1015952
[30] Albert M, Smith LA, Scherr PA, Taylor JO, Evans DA,953
Funkenstein HH (1991) Use of brief cognitive tests to iden-954
tify individuals in the community with clinically diagnosed955
Alzheimer’s disease. Int J Neurosci 57, 167-178.956
[31] Devanand DP, Folz M, Gorlyn M, Moeller JR, Stem J (1997)957
Questionable dementia: clinical course and predictors of out-958
come. J Am Geriatr Soc 45, 321-328.959
[32] Flicker CS, Ferris H, Reisberg B (1991) Mild cognitive960
impairment in the elderly: predictors of dementia. Neurology961
41, 1006-1009.962
[33] Petersen RC, Smith GE, Ivnik RJ, Tangalos EG, Schaid SN,963
Thibodeau SN, Kokmen E, Waring SC, Kurland LT (1995)964
Apolipoprotein E status as a predictor of the development of965
Alzheimer’s disease in memory-impaired individuals. JAMA966
273, 1274-1278.967
[34] Petersen RC, Smith GE, Waring SC, Ivnik RJ, Kokmen E,968
Tangelos EG (1997) Aging, memory, and mild cognitive969
impairment. Int Psychogeriatr 9 Suppl 1, 65-69.970
[35] Petersen RC, Doody R, Kurz A, Mohs RC, Morris JC, Rabins971
PV, Ritchie K, Rossor M, Thal L, Winblad B (2001) Current972
concepts in mild cognitive impairment. Arch Neurol 58, 1985-973
1992.974
[36] Petersen RC (2004) Mild cognitive impairment as a diagnostic975
entity. J Intern Med 256, 183-194.976
[37] Rubin EH, Morris JC, Grant EA, Vendegna T (1989) Very977
mild senile dementia of the Alzheimer type. I. Clinical assess-978
ment. Arch Neurol 46, 379-382.979
[38] Zaudig M (1992) A new systematic method of measurement980
and diagnosis of “mild cognitive impairment” and dementia981
according to ICD-10 and DSM-III-R criteria. Int Psychogeri-982
atr. 4 Suppl 2, 203-219.983
[39] Portet F, Ousset PJ, Visser PJ, Frisoni GB, Nobili F,984
Scheltens P, Vellas B, Touchon J (2006) MCI Working Group985
of the European Consortium on Alzheimer’s Disease Mild986
cognitive impairment (MCI) in medical practice: a critical987
review of the concept and new diagnostic procedure. Report988
of the MCI Working Group of the European Consortium on989
Alzheimer’s Disease. J Neurol Neurosurg Psychiatry 77, 714-990
718.991
[40] McKhann G, Drachman D, Folstein M, Katzman R,992
Price D, Stadlan (1984) Clinical diagnosis of Alzheimer’s993
disease: report of the NINCDS- ADRDA Work Group under994
the auspices of Department of Health and Human Services995
Task Force on Alzheimer’s disease. Neurology 34, 939-996
944.997
[41] Yesavage JA, Brink TL, Rose TL, Lum O, Huang V, Adey998
M, Leirer VO (1982-83) Development and validation of a999
geriatric depression screening scale: a preliminary report. J1000
Psychiatr Res 17, 37-49.1001
[42] Folstein MF, Folstein SE, McHugh PR (1975) ‘Mini Mental1002
State’: a practical method for grading the cognitive state of1003
patients for clinician. J Psychiat Res 12, 189-198.1004
[43] Hughes CP, Berg L, Danziger WL, Coben LA, Martin RL 1005
(1982) A new clinical scale for the staging of dementia. Br J 1006
Psychiatry 140, 566-572. 1007
[44] Rosen WG, Terry RD, Fuld PA, Katzman R, Peck A (1980) 1008
Pathological verification of ischemic score in differentiation 1009
of dementias. Ann Neurol 7, 486-488. 1010
[45] Lawton MP, Brodie EM (1969) Assessment of older people: 1011
self maintaining and instrumental activity of daily living. J 1012
Gerontol 9, 179-186. 1013
[46] Knopman DS, Boeve BF, Parisi JE, Dickson DW, Smith GE, 1014
Ivnik RJ, Josephs KA, Petersen RC (2005) Antemortem diag- 1015
nosis of frontotemporal lobar degeneration. Ann Neurol 57, 1016
480-488. 1017
[47] Roman GC, Tatemichi TK, Erkinjuntti T, Cummings JL, Mas- 1018
deu JC, Garcia JH, Amaducci L, Orgogozo JM, Brun A, 1019
Hofman A, et al (1993) Vascular dementia: diagnostic criteria 1020
for research studies. Report of the NINDS-AIREN Interna- 1021
tional Workshop. Neurology 43, 250-260. 1022
[48] McKeith IG, Perry EK, Perry RH (1999) Report of the second 1023
dementia with Lewy body international workshop: diagnosis 1024
and treatment. Consortiumon Dementia with Lewy Bodies. 1025
Neurology 53, 902-905. 1026
[49] Van Leemput K, Maes F, Vandermeulen D, Colchester A, 1027
Suetens P (2001) Automated segmentation of multiple scle- 1028
rosis lesions by model outlier detection. IEEE Trans Med 1029
Imaging 20, 677-688, 1030
[50] Dempster AP, Laird NM, Rubin DB (1977) “Maximum like- 1031
lihood from incomplete data via the EM algorithm.” J Roy 1032
Statist Soc 39, 1-38. 1033
[51] Moretti DV, Babiloni F, Carducci F, Cincotti F, Remondini 1034
E, Rossini PM, Salinari S, Babiloni C (2003) Computerized 1035
processing of EEG-EOG-EMG artifacts for multicentirc stud- 1036
ies in EEG oscillations and event-related potentials. Int J 1037
Psychophysiol 47, 199-216. 1038
[52] Klimesch W (1999) EEG alpha and theta oscillations reflect 1039
cognitive and memory performance: a review and analysis. 1040
Brain Res Rev 29, 169-195. 1041
[53] Babiloni C, Binetti G, Cassarino A, Dal Forno G, Del Percio 1042
C, Ferreri F, Ferri R, Frisoni G, Galderisi S, Hirata K, Lanuzza 1043
B, Miniussi C, Mucci A, Nobili F, Rodriguez G, Romani GL, 1044
Rossini PM (2006) Sources of cortical rhythms in adults dur- 1045
ing physiological aging: a multi-centric EEG study. Human 1046
Brain Mapp 27, 162-172. 1047
[54] Babiloni C, Benussi L, Binetti G, Bosco P, Busonero G, 1048
Cesaretti S, Dal Forno G, Del Percio C, Ferri R, Frisoni G, 1049
Ghidoni R, Rodriguez G, Squitti R, Rossini PM (2006) Geno- 1050
type (cystatin C) and EEG phenotype in Alzheimer disease 1051
and mild cognitive impairment: a multicentric study. Neu- 1052
roimage 29, 948-964. 1053
[55] Babiloni C, Benussi L, Binetti G, Cassetta E, Dal Forno G, Del 1054
Percio C, Ferreri F, Ferri R, Frisoni G, Ghidoni R, Miniussi C, 1055
Rodriguez G, Romani GL, Squitti R, Ventriglia MC, Rossini 1056
PM (2006) Apolipoprotein E and alpha brain rhythms in mild 1057
cognitive impairment: A multicentric EEG study. Ann Neurol 1058
59, 323-334. 1059
[56] Babiloni C, Frisoni G, Steriade M, Bresciani L, Binetti G, 1060
Del Percio C, Geroldi C, Miniussi C, Nobili F, Rodriguez 1061
G, Zappasodi F, Carfagna T, Rossini PM (2006) Frontal 1062
White Matter Volume and Delta EEG Sources Negatively 1063
Correlate In Awake Subjects With Mild Cognitive Impair- 1064
ment and Alzheimer’s Disease. Clin Neurophysiol 117, 1113- 1065
1129. 1066
[57] Pascual-Marqui RD, Michel CM (1994) LORETA (low reso- 1067
lution brain electromagnetic tomography): new authentic 3D 1068
functional images of the brain. ISBET Newsletter ISSN 5, 4-8. 1069

Unc
orre
cted
Aut
hor P
roof
C. Babiloni et al. / EEG and Vascular Lesion in AD 15
[58] [58] Pascual-Marqui RD, Lehmann D, Koenig T, Kochi1070
K, Merlo MC, Hell D, Koukkou M (1999) Low resolu-1071
tion brain electromagnetic tomography (LORETA) functional1072
imaging in acute, neuroleptic-naive, first-episode. productive1073
schizophrenia. Psychiatry Res 90, 169-179.1074
[59] Pascual-Marqui RD, Esslen M, Kochi K, Lehmann D (2002)1075
Functional imaging with low resolution brain electromag-1076
netic tomography (LORETA): a review. Meth Find Exp Clin1077
Pharmacol 24, 91-95.1078
[60] Valdes P, Picton TW, Trujillo N, Bosch J, Aubert E, Riera J1079
(1998) Constraining EEG-MEG source imaging with statisti-1080
cal neuroanatomy. Neuroimage 4, 635.1081
[61] Phillips C, Rugg MD, Friston KJ (2002) Systemic regulariza-1082
tion of linear inverse solutions of the EEG source localization1083
problem. Neuroimage 17 287-301.1084
[62] Yao D, He B (2001) A self-coherence enhancement algorithm1085
and its application to enhancing three-dimensional source1086
estimation from EEGs. Ann Biomed Eng (2001) 29, 1019-1087
1027.1088
[63] Talairach J, Tournoux P (1988). Co-Planar Stereotaxic Atlas1089
of the Human Brain, Stuttgart Thieme.1090
[64] Anderer P, Saletu B, Semlitsch HV, Pascual-Marqui RD1091
(2003) Non-invasive localization of P300 sources in nor-1092
mal aging and age-associated memory impairment. Neurobiol1093
Aging 24, 463-479.1094
[65] Anderer P, Saletu B, Saletu-Zyhlarz G, Gruber D, Metka M,1095
Huber J, Pascual-Marqui RD (2004) Brain regions activated1096
during an auditory discrimination task in insomniac post-1097
menopausal patients before and after hormone replacement1098
therapy: low-resolution brain electromagnetic tomography1099
applied to event-related potentials. Neuropsychobiology 49,1100
134-153.1101
[66] Babiloni C, Bosco P, Ghidoni R, Del Percio C, Squitti R,1102
Binetti G, Benussi L, Ferri R, Frisoni G, Lanuzza B, Cas-1103
setta E, Anello G, Gurzı M, Bartesaghi S, Lizio R, Tombini1104
M, Rossini PM (2007) Homocysteine and electroencephalo-1105
graphic rhythms in Alzheimer disease: a multicentric study.1106
Neuroscience 145, 942-954.1107
[67] Babiloni C, Cassetta E, Binetti G, Tombini M, Del Percio1108
C, Ferreri F, Ferri R, Frisoni G, Lanuzza B, Nobili F, Parisi1109
L, Rodriguez G, Frigerio L, Gurzı M, Prestia A, Vernieri F,1110
Eusebi F, Rossini PM (2007) Resting EEG sources corre-1111
late with attentional span in mild cognitive impairment and1112
Alzheimer’s disease. Eur J Neurosci 25, 3742-3757.1113
[68] Babiloni C, Pievani M, Vecchio F, Geroldi C, Eusebi F, Fra-1114
cassi C, Fletcher E, De Carli C, Boccardi M, Rossini PM,1115
Frisoni GB (2009) White-matter lesions along the choliner-1116
gic tracts are related to cortical sources of EEG rhythms in1117
amnesic mild cognitive impairment. Hum Brain Mapp 30,1118
1431-1443.1119
[69] Laufer I, Pratt H (2003) Evoked potentials to auditory move-1120
ment sensation in duplex perception. Clin Neurophysiol 114,1121
1316-1331.1122
[70] Laufer I, Pratt H. (2003b) The electrophysiological net1123
response (‘F-complex’) to spatial fusion of speech elements1124
forming an auditory object.Clin Neurophysiol 114, 818-834.1125
[71] Mulert C, Gallinat J, Pascual-Marqui R, Dorn H, Frick K,1126
Schlattmann P, Mientus S, Herrmann WM, Winterer G (2001)1127
Reduced event-related current density in the anterior cingulate1128
cortex in schizophrenia. Neuroimage 13(4), 589-600.1129
[72] Klimesch W. (1996) Memory processes, brain oscillations and1130
EEG synchronization. Int J Psychophysiol 24, 61-100.1131
[73] Leuchter AF, Cook IA, Newton TF, Dunkin J, Walter DO,1132
Rosenberg Tompson S, Lachenbruch PA, Weiner H (1993)1133
Regional differences in brain electrical activity in dementia:1134
use of spectral power and spectral ratio measures. Electroen- 1135
ceph clin Neurophysiol 87, 385-393. 1136
[74] Nuwer MR (1988) Quantitative EEG. I: tecniques and prob- 1137
lems of frequency analysis and topographic mapping. J Clin 1138
Neurophysiol 5, 1-43. 1139
[75] Hern, aacute, ndez JL, Vald, eacute, s P, Biscay R, Viru, 1140
eacute, s T, Szava S, Bosch J, Riquenes A, Clark I (1994) A 1141
global scale factor in brain topography. Int J Neurosci 76, 267- 1142
278. 1143
[76] Prichep LS, John ER, Ferris SH, Reisberg B, Almas M, Alper 1144
K, Cancro R (1994) Quantitative EEG correlates of cognitive 1145
deterioration in the elderly. Neurobiol Aging 15, 85-90. 1146
[77] Wolf H, Jelic V, Gertz HJ, Nordberg A, Julin P, Wahlund LO 1147
(2003) A critical discussion of the role of neuroimaging in 1148
mild cognitive impairment. Acta Neurol Scand 107, 52-76. 1149
[78] Moretti DV, Babiloni C, Binetti G, Cassetta E, Dal Forno G, 1150
Ferreri F, Ferri R, Lanuzza B, Miniussi C, Nobili F, Rodriguez 1151
G, Salinari S, Rossini PM (2004) Individual analysis of EEG 1152
frequency and band power in mild Alzheimer’s Disease. Clin 1153
Neurophysiol 115, 299-308. 1154
[79] Steriade M (2003) Cerebello-cerebral interactions during 1155
states of vigilance. Cerebellum 2, 82-83. 1156
[80] Steriade M (1996) Awakening the brain. Nature 383, 24-25. 1157
[81] Klimesch W, Doppelmayr M, Pachinger T, Russegger H 1158
(1997) Event-related desynchronization in the alpha band and 1159
the processing of semantic information. Brain Res Cogn Brain 1160
Res 6, 83-94. 1161
[82] Klimesch W, Doppelmayr M, Russegger H, Pachinger T, 1162
Schwaiger J (1998) Induced alpha band power changes in 1163
the human EEG and attention. Neurosci Lett 244, 73-76. 1164
[83] Rossini PM, Desiato MT, Lavaroni F, Caramia MD (1991) 1165
Brain excitability and electroencephalographic activation: 1166
non-invasive evaluation in healthy humans via transcranial 1167
magnetic stimulation. Brain Res 13, 111-119. 1168
[84] Steriade M, Llinas RR (1988) The functional states of the 1169
thalamus and the associated neuronal interplay. Physiol Rev 1170
68, 649-742. 1171
[85] Ricceri L, Minghetti L, Moles A, Popoli P, Confaloni A, De 1172
Simone R, Piscopo P, Scattoni ML, Di Luca M, Calamandrei 1173
G (2004) Cognitive and neurological deficits induced by early 1174
and prolonged basal forebrain cholinergic hypofunction in 1175
rats. Exp Neurol 189, 162-172. 1176
[86] Braak H, Braak E (1996) Evolution of the neuropathology of 1177
Alzheimer’s disease. Acta Neurol Scand Suppl 165, 3-12. 1178
[87] Braak H, Braak E (1998) Evolution of neuronal changes in 1179
the course of Alzheimer’s disease. J Neural Transm Suppl 53, 1180
127-140. 1181
[88] Regan C, Katona C, Walker Z, Hooper J, Donovan J, 1182
Livingston G (2006) Relationship of vascular risk to the pro- 1183
gression of Alzheimer disease. Neurology 67, 1357-1362. 1184
[89] Etiene D, Kraft J, Ganju N, Gomez-Isla T, Gemelli B, Hyman 1185
BT, Hedley-Whyte ET, Wands JR, De La Monte SM (1998) 1186
Cerebrovascular pathology contributes to the heterogeneity 1187
of Alzheimer’s disease. J Alzheimers Dis 1, 119-134. 1188
[90] Heyman A, Fillenbaum GG, Welsh-Bohmer KA, Gearing M, 1189
Mirra SS, Mohs RC, Peterson BL, Pieper CF (1998) Cerebral 1190
infarcts in patients with autopsy-proven Alzheimer’s disease: 1191
CERAD, part XVIII. Consortium to Establish a Registry for 1192
Alzheimer’s Disease. Neurology 51, 159-162. Erratum in: 1193
Neurolog 51, 1809. 1194
[91] Esiri MM, Nagy Z, Smith MZ, Barnetson L, Smith AD (1999) 1195
Cerebrovascular disease and threshold for dementia in the 1196
early stages of Alzheimer’s disease. Lancet 354, 919-920. 1197
[92] Lee JH, Olichney JM, Hansen LA, Hofstetter CR, Thal LJ 1198
(2000) Small concomitant vascular lesions do not influence 1199

Unc
orre
cted
Aut
hor P
roof
16 C. Babiloni et al. / EEG and Vascular Lesion in AD
rates of cognitive decline in patients with Alzheimer disease.1200
Arch Neurol 57, 1474-1479.1201
[93] Jellinger KA (2001) Small concomitant cerebrovascular1202
lesions are not important for cognitive decline in severe1203
Alzheimer disease (letter). Arch Neurol 58, 520-521.1204
[94] Mungas D, Reed BR, Ellis WG, Jagust WJ (2001) The effects1205
of age on rate of progression of Alzheimer disease and demen-1206
tia with associated cerebrovascular disease. Arch Neurol 58,1207
1243-1247.1208
[95] Brown WR, Thore CR (2011) Cerebral microvascular pathol-1209
ogy in ageing and neurodegeneration. Neuropathol Appl1210
Neurobiol 37, 56-74.1211
[96] Balthazar ML, Yasuda CL, Pereira FR, Pedro T, Damasceno1212
BP, Cendes F Differences in grey and white matter atrophy1213
in amnestic mild cognitive impairment and mild Alzheimer’s1214
disease. Eur J Neurol 16, 468-474.
[97] Serra L, Cercignani M, Lenzi D, Perri R, Fadda L, Calta- 1215
girone C, Macaluso E, Bozzali M (2010) Grey and white 1216
matter changes at different stages of Alzheimer’s disease. J 1217
Alzheimers Dis 19, 147-159. 1218
[98] Teipel SJ, Meindl T, Grinberg L, Grothe M, Cantero JL, 1219
Reiser MF, ouml M, ller HJ, Heinsen H, Hampel H (2011) 1220
The cholinergic system in mild cognitive impairment and 1221
Alzheimer’s disease,An in vivo MRI and DTI study. Hum 1222
Brain Mapp. doi:10.1002/hbm.21111. 1223
[99] . Teipel SJ, Meindl T, Wagner M, Stieltjes B, Reuter S, Hauen- 1224
stein KH, Filippi M, Ernemann U, Reiser MF, Hampel H. 1225
Longitudinal Changes in Fiber Tract Integrity in Healthy 1226
Aging and Mild Cognitive Impairment: A DTI Follow-Up 1227
Study. J Alzheimers Dis 22,2, 507-522. 1228