04760 - H2S Inhibition By Nitrate Injection On The Gullfaks Field

Investigation report Report Report title Activity number
Undesirable incident with HTV Eagle pipehandling crane – Statoil
Gullfaks B – 7 March 2017
001050062
Security grading
Public
Not publicly available
Restricted
Confidential
Strictly confidential
Summary
The incident occurred at 15.25 on 7 March 2017 on the Gullfaks B (GFB) installation. The boom on
the horizontal to vertical (HTV)) Eagle pipehandling crane, which weighed about 14.4 tonnes, fell 10
metres to the pipe deck after the steel rope failed. Two people had adjusted the grippers on the crane’s
gripper yoke down on the pipe deck immediately before the incident occurred.
Drilling facilities on GFB were upgraded with a new HTV Eagle crane in 2015. This was part of a big
project executed for Statoil by Aibel. MH Wirth was Aibel’s subcontractor for the pipehandling
equipment. Operations resumed after the upgrading in September 2015. KCA Deutag (KCAD) is the
drilling contractor on GFB.
The direct cause of the crane boom falling down was fatigue in the steel rope. This was one of the
main components in the arrangement for the crane’s vertical up and down movement.
The underlying cause was weaknesses in the design of the crane’s hoisting arrangement, which
consists primarily of the winch, sheaves, vertical dolly and steel rope. Owing to the design, the rope
was subject to wear and fatigue over time. Fatigue in the steel rope was not assessed as a relevant
problem for this design.
Risk associated with the equipment was not adequately identified, replacement intervals were not
determined on the basis of durability calculations for the steel rope, and insufficient use was made of
crane and lifting expertise when specifying the crane requirements. In addition, follow-up of earlier
incidents involving damage to steel rope and a failed sheave bearing was inadequate, deficiencies and
errors existed in the maintenance programme for the rope, and follow-up and checking when taking
delivery of equipment and machinery were inadequate.
Under slightly different circumstances, the incident could have caused serious personal injuries or
loss of human life.
The PSA team’s job was to support the police inquiry and to conduct its own investigation of the
incident. The PSA and the police were on board GFB from 8–10 March 2017.
Involved Main group Approved date
T-1 24 August 2017
Members of the investigation team Investigation leader
Anne Marit Lie, Reidar Sune, Gustav W Dunsæd,
Eigil Sørensen, Sigmund Andreassen (did not
participate offshore)
Anne Marit Lie

2
Contents Summary .................................................................................................................................... 3 1 Introduction .......................................................................................................................... 3
Mandate for the investigation ........................................................................ 4 Composition of the investigation team .......................................................... 4
2 Background information ...................................................................................................... 4 3 Course of events ................................................................................................................... 7 4 Direct and underlying causes of the incident ..................................................................... 12
4.1 Direct cause ......................................................................................... 12 4.2.1 Design of the HTV Eagle crane ............................................. 12 4.2.2 Failure to follow up earlier incidents ..................................... 15 4.2.3 Insufficient knowledge of and expertise on steel rope ........... 16 4.2.4 Monitoring/inspection of steel rope ....................................... 16
5 Potential of the incident ...................................................................................................... 17 5.1 Actual consequence ............................................................................ 17 5.2 Potential consequence ......................................................................... 18
6 Observations ....................................................................................................................... 18 6.1 Nonconformities .................................................................................................... 19
6.1.1 Risk assessment of equipment ................................................ 19 6.1.2 Investigation of and improvement measures following
earlier incidents ..................................................................... 19 6.1.3 Utilisation of expertise ........................................................... 20 6.1.4 Responsibility for taking delivery and operation of
equipment ............................................................................... 21 6.1.5 Maintenance ........................................................................... 22
7 Poor visibility from crane cabin ...................................................................... 22 8 Barrier assessment .............................................................................................................. 22 9 Discussion of uncertainties ................................................................................................. 23 10 Statoil’s investigation report ............................................................................................ 24 11 Appendix .......................................................................................................................... 24

3
Summary
The incident occurred at 15.25 on 7 March 2017 on the Gullfaks B (GFB) installation. The
boom on the horizontal to vertical (HTV)) Eagle pipehandling crane, which weighed about
14.4 tonnes, fell 10 metres to the pipe deck after the steel rope failed. Two people had
adjusted the grippers on the crane’s gripper yoke down on the pipe deck immediately before
the incident occurred.
Drilling facilities on GFB were upgraded with a new HTV Eagle crane in 2015. This was part
of a big project executed for Statoil by Aibel. MH Wirth was Aibel’s subcontractor for the
pipehandling equipment. Operations resumed after the upgrading in September 2015. KCA
Deutag (KCAD) is the drilling contractor on GFB.
The direct cause of the crane boom falling down was fatigue in the steel rope. This was one of
the main components in the arrangement for the crane’s vertical up and down movement.
The underlying cause was weaknesses in the design of the crane’s hoisting arrangement,
which consists primarily of the winch, sheaves, vertical dolly and steel rope. Owing to the
design, the rope was subject to wear and fatigue over time. Fatigue in the steel rope was not
assessed as a relevant problem for this design.
Risk associated with the equipment was not adequately identified, replacement intervals were
not determined on the basis of durability calculations for the steel rope, and insufficient use
was made of crane and lifting expertise when specifying the crane requirements. In addition,
follow-up of earlier incidents involving damage to steel rope and a failed sheave bearing was
inadequate, deficiencies and errors existed in the maintenance programme for the rope, and
follow-up and checking when taking delivery of equipment and machinery were inadequate.
Under slightly different circumstances, the incident could have caused serious personal
injuries or loss of human life.
The PSA team’s job was to support the police inquiry and to conduct its own investigation of
the incident. The PSA and the police were on board GFB from 8–10 March 2017.
Statoil conducted its own investigation.
1 Introduction
In connection with transferring materials from the pipe deck to the drill floor on GFB, the
crane boom dropped 10 metres without warning to the pipe deck. Statoil notified the PSA of
the incident at 17.55 on 7 March 2017.
The police requested support from the PSA for its inquiry into the incident. At the same time,
the PSA conducted its own investigation.
Four members of the PSA’s investigation team were on board GFB together with the police
from 8–10 March 2017. During this time, the team supported the police during site
inspections and in interviews with personnel.
Following its stay on GFB, the team received further information from interviews with
relevant personnel at KCAD, MH Wirth, subcontractors involved and Statoil.

4
The steel rope and one sheave were confiscated by the police. By agreement with the police
and the PSA, Statoil sent the confiscated components to W Giertsen Services AS in Bergen
for assessments and analyses.
Statoil’s investigation report was received by the PSA on 8 June 2017. A meeting was held
with Statoil on 19 June 2017 to clarify certain points in this document.
The investigation team has utilised the human, technological and organisational (HTO)
approach as its methodology. This builds on the concept of operational, organisational and
technical barrier elements.
Mandate for the investigation
a. Clarify the incident’s scope and course of events with an emphasis on safety, working
environment and emergency preparedness aspects.
b. Assess the actual and potential consequences
1. Harm caused to people, material assets and the environment.
2. The potential of the incident to harm people, material assets and the
environment.
c. Assess direct and underlying causes, with an emphasis on human, technology and
organisation (HTO) and operational aspects, from a barrier perspective.
d. Discuss and describe possible uncertainties/unclear aspects.
e. Identify nonconformities and improvement points related to the regulations (and
internal requirements).
f. Discuss barriers which have functioned (in other words, those which have helped to
prevent a hazard from developing into an accident, or which have reduced the
consequences of an accident).
g. Assess the player’s own investigation report (the PSA’s assessment is to be
communicated in a meeting or by letter).
h. Prepare a report and a covering letter (possibly with proposals for the use of
reactions) in accordance with the template.
i. Recommend – and contribute to – further follow-up.
Composition of the investigation team
The PSA’s investigation team has comprised:
Anne Marit Lie – investigation leader, logistics and emergency preparedness
discipline area
Reidar Sune, logistics and emergency preparedness discipline area
Gustav W Dunsæd, drilling and well discipline area
Eigil Sørensen, drilling and well discipline area
Sigmund Andreassen (did not participate offshore), logistics and emergency
preparedness discipline area
2 Background information

5
Gullfaks is a Statoil-operated field located in 130-220 metres of water in the northern North
Sea. It has been developed with three installations, each featuring integrated process, drilling
and quarters modules, a concrete support structure and a steel topside. Oil and gas from GFB
are transferred to Gullfaks A and C for processing and storage. The oil is loaded into shuttle
tankers on the field, while the gas gets piped to the processing facilities at Kårstø.
GFB is a quarters, drilling and oil production/water injection facility of the Condeep type,
standing in 145 metres of water.
Activities before the incident
- Well B-14C was drilled to a depth of 5 145 metres.
- Seven-inch casing was installed at 5 144 metres and cemented.
- The well was tested to 237 bar using mud with a specific gravity of 1.65.
- The well and blowout preventer were tested (no drilling had taken place out of the
seven-inch liner).
Pipehandling equipment involved in the incident
The pipehandling system primarily comprises a traverse crane on the pipe deck and an
HTV Eagle crane installed in connection with the V-door to the drill floor. Drill pipe is
transported horizontally by the traverse crane from the pipe deck to the catwalk for further
handling by the HTV Eagle crane to and from the drill floor.
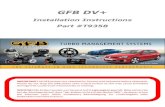
The HTV Eagle crane comprises a vertical dolly, which is installed between two vertical
guide beams for up and down movement with the aid of a hoisting arrangement, and equipped
with a boom. Its role is to hoist drill pipe from the catwalk on the pipe deck, where the pipes
lie horizontally, to a vertical position on the drill floor.
In the hoisting arrangement, steel rope from an electric winch runs over a sheave at the top of
one guide beam and under two sheaves on the dolly to its anchoring point on top of the other
beam. A load cell is installed as part of the anchoring arrangement. See figures 1 and 2 for the
arrangement of the HTV Eagle crane.

6
Figure 1 HTV Eagle arrangement, with the steel rope in red. (Statoil’s investigation report)
Figure 2 The HTV Eagle crane in the derrick and the traverse crane on the pipe deck.
HTV Eagle crane
Catwalk
Traverse crane

7
3 Course of events
A new HTV Eagle crane was installed in 2015 as part of a major conversion of the drilling
facilities on GFB. Statoil outsourced the work to Aibel in 2013, which awarded the
subcontract for the HTV pipehandling equipment (specified as the HTV Eagle crane and
tubular feeding machine) to MH Wirth. The latter bought the winch with drum from
Kverneland Aqua AS.
When designing the HTV Eagle crane, MH Wirth carried out a criticality assessment using
failure mode, effects and criticality analysis (FMECA). But this analysis failed to identify the
steel rope as a critical component in the system.
The GFB project drew on experience with the HTV Eagle crane on Gullfaks C in an effort to
improve the design. Emphasis was given, for example, to protecting the steel rope in the
hoisting arrangement from being damaged by the deck crane when the latter was used to lift
loads in and out through the V-door to the drill floor. On Gullfaks C, the rope had previously
been damaged during material handling by the offshore crane.
To improve the design, the GFB project team sought to give the rope more protection by
incorporating it in the guide beams. That was also why a sheave diameter 18 times greater
than the rope diameter (18xD/d) came to be chosen, since this dimension was better adapted
to the design while also simplifying the structure.
Where safety aspects of the HTV Eagle design are concern, the primary emphasis appears to
have been on preventing loads and objects dropping from the crane and on ensuring that drill
pipe could not slip out of the gripper yoke.
Following a review of the documentation and conversations with personnel involved at
Statoil, MH Wirth and KCAD, the team’s understanding is that no particular attention was
devoted to the hoisting arrangement with regard either to the choice of rotation-resistant steel
rope or the assessment of expected service life for this rope in the relevant winch and sheave
arrangement. The choice of rotation-resistant rope was not based on assessments of several
rope types.
MH Wirth issued a conformity declaration for the HTV Eagle crane on 16 July 2015.
DNV GL issued a certificate for the HTV Eagle lifting facility/equipment on 5 September
2015. This was based on a low-level verification as defined in DNV-OSS-308, which is used
for lifting facilities/equipment with a low risk level. The certification identified no design
weaknesses or conditions to be kept under observation in the operating phase.
The investigation identified inadequate spare-part lists and maintenance routines at the point
of delivery from project to operations. No documentation has been found which shows that
maintenance and inspection routines have taken account of the fact that rotation-resistant steel
rope is difficult to inspect visually for fatigue. Such conditions should have been covered in
the manuals from MH Wirth.
The crane became operational in September 2015. Before start-up, Statoil gave emphasis to
educating and training the personnel who were to use new equipment.

8
Incident January 2016: damage to steel rope
Personnel discovered damage to the steel rope on the HTV Eagle crane on 1 January 2016
(Synergi # 1461090).
Four of 34 strands proved to have parted, and the rope was deformed. A birdcage had formed.
See figure 3. The reason for this damage was assessed to be the wrong type of rotation-
resistant rope. While rope with a right-hand lay was used on the winch drum, this was
designed to handle left-hand lay.
MH Wirth drafted a major operational failure report on 10 January. The rope was replaced
with a left-hand lay type, and the problem was regarded as solved. MH Wirth ordered new
rope from Kverneland Aqua AS, which received this from Westfalische Drahtindustrie.
MH Wirth asked Kverneland Aqua AS to assess the possible cause of the damage to the rope.
The latter did as requested and submitted its report to MH Wirth. Dated 12 January, this
recommends that the hoisting arrangement be designed with a sheave diameter of 26xD/d and
warns that the service life of the steel rope would be shortened by using sheaves with small
dimensions.
Figure 3 Damage to the steel rope on the HTV Eagle crane. (Synergi # 1461090, January 2016)
In an asset integrity report of 17 January, the KCAD field engineer for crane and lifting expresses concern that the fleet angle of the steel rope from the electric winch drum to the upper sheave (S1, see figure 4) atop the one guide beam is at the upper limit of the tolerable and must be followed up. MH Wirth responded that the fleet angle was within the sheave’s tolerance.
On 19 January, MH Wirth submitted a technical report on the damage to the rope, where it maintains the view that this was caused by using rope with right-hand instead of left-hand lay. The report did not incorporate the assessments provided by Kverneland Aqua AS in its report of 12 January.
MH Wirth made no reassessment after receiving the input from Kverneland Aqua AS and KCAD. No service life was calculated for the rope on this occasion either.

9
Incident of July 2016
On 30 July, personnel heard strange noises from the HTV Eagle crane (Synergi # 1480757).
These proved to originate not from the winch but from the S1 sheave at the top of the guide beam. Soon afterwards, while the crane was in use, rollers from the sheave bearing fell to the winch deck.
ß
Figure 2 The HTV Eagle crane when bearings were replaced in S1. (Synergi # 1480757)s
The bearing of S1 on the guide beam was replaced on that same day.
KCAD submitted a major operational failure report on 1 August covering the damage to the
bearing in S1. This identified the fleet angle of the steel rope from the drum to the sheave as
the cause of the roller bearing failure. Furthermore, the sheave was to be replaced every six
months (established as the maintenance interval).
Upper sheave (S1), where rollers fell from the
bearing
Position of the winch for hoisting the crane
Two sheaves on the dolly (S2 and S3)

10
Figure 5: The steel rope bearing Figure 6: The fleet angle between drum and sheave.
against the sheave.
Statoil’s asset integrity unit and the crane and lifting supervisor in the process section of GFB
expressed concern in an e-mail of 19 October over the design of the HTV Eagle crane. They
stated in part: “Several conditions exist here, [such as] bearing failures and abnormal sheave
wear, which derive from a large fleet angle. If nothing is done, failure of sheave bearings or
the actual sheave, or a new incident with the steel rope, can be predicted with certainty.”
This expression of concern went to Statoil’s rig representative and the KCAD maintenance
manager. It had not led to any special follow-up by either Statoil or KCAD before the rope
failed.
Measures taken
A new sheave was installed on the HTV Eagle crane in January 2017, with a visual inspection
carried out for the rope. The latter was re-installed after the inspection because no external
damage was found. Possible fatigue damage to the rope was not assessed.
Course of events, 7 March 2017
15.05. The HTV Eagle crane is used to lay steel rope offcuts on the deck after a slip and cut of
drill line operation.
15.10–15.11. Two men stood under the crane and disconnected the load on the deck.
15.12–15.13. A new load was connected – a magnet mounted on a short length of 3 ½-inch
drill pipe.
15.14–15.20. The load was readied, and the magnet lifted to the drill floor.
15.21. The magnet was unhooked on the drill floor.
15.22. The crane boom was lowered to the deck without a load.
15.23. Two people stood under the crane and adjusted the grippers to 3 ½-inch drill pipe.

11
15.24. The gripper yoke was readied, and the crane hoisted up to give the traverse crane
access to the pile of drill pipe on the deck.
15.25. Without warning, the steel rope failed and the crane boom fell 10 metres to the
pipe deck.
15.27–15.28. The borehole was covered and the platform management notified.
15.30–15.40. A site inspection was conducted, the area cordoned off was expanded, all work
permits were withdrawn and all work was halted.
15.40. All personnel involved from the drilling contractor were assembled in the coffee bar.
The emergency response organisation was not mobilised.
Figure 7 presents the approximate position of the steel rope when it failed.
Figure 7 The red arrow shows the point where the steel rope failed.
Upper sheave (S1), where rollers fell from
the bearing
Two sheaves (S2 and S3) on the dolly
Failure site

12
4 Direct and underlying causes of the incident
4.1 Direct cause
The direct cause of the boom falling to the pipe deck was fatigue in the steel rope. The rope is
a safety-critical main component in the arrangement for the up and down crane movement. It
carries the whole weight of the crane’s hoisting and boom arrangement – a maximum of 17.9
tonnes with load and about 14.4 tonnes without load.
The load on the hoisting and boom arrangement can be reduced by parking in a cradle on the
pipe deck, but use of the parking cradle depends on the position of the derrick. When the
incident occurred, the cradle was not accessible because of the derrick’s position in relation to
the pipe deck. In order to use the traverse crane on the pipe deck, the HTV Eagle crane boom
had to be parked in a position above the V-door and drill floor.
When the HTV Eagle crane is parked above the pipe deck, the boom is held in place only by
the rope. The latter will then be subject to a continuous load of about 14.4 tonnes. In addition
comes a good deal of motion and vibration in the derrick during drilling, which could be
unfavourable for the rope in terms of fatigue. That has not been included as a contributory
factor in the investigation.
The crane was not provided with any form of safety system which prevented its hoisting and
boom arrangement from falling if the steel rope or other load-bearing components failed. Nor
had any arrangement been installed which hangs off or relieves the load on the rope when the
crane is parked in a position above the pipe deck. A parking cradle is used when the crane is
parked on a level with the pipe deck.
4.2 Underlying causes
4.2.1 Design of the HTV Eagle crane
The PSA’s view is that fatigue occurred in the steel rope because of the inadequate design of
the hoisting arrangement for up and down movement of the crane. During the design phase,
assessment errors were made in choosing component dimensions and insufficient attention
was paid to how these would function in combination with the steel rope. This has result in a
very low service life for the rope. No service life calculations were made for it.
This applies to the following components.
Rotation-resistant steel rope
According to the technical literature and supplier information, using rotation-resistant steel
rope in this type of hoisting arrangement has little point in design terms. Such rope has
primarily been developed for systems with a free end, where it is desirable to reduce rotation
in the latter. Rotation-resistant steel rope is commonly used in a crane or hoisting winch
where the smallest possible rotation of the crane hook is desirable. However, this was not a
problem in the GFB system since the rope is permanently anchored at both ends (in the winch
drum and at the end attachment). Providing the rope is correctly installed in such systems, no
further rotation of the rope will be introduced and rotation will not be a challenge. No design
reason exists for choosing rotation-resistant steel rope in this type of hoisting arrangement.

13
The steel rope in use when the incident occurred had a tensile strength of 2 160 N/mm2. That
gives it high strength, but is unnecessary to meet the rope’s required safety factor. Steel rope
with such a high tensile strength is less elastic and unsuitable for a sheave with a diameter as
small as 18xD/d, which will reduce its fatigue life even further. Product information from the
manufacturer of the relevant rope recommends a minimum sheave diameter of 20xD/d.
According to the report from W Giertsen Service AS, the theoretical applied working life
would be about 50 per cent of the calculated service life (until fatigue/strand fracturing occurs
internally). Internal strand fracturing means the rope must be scrapped, see ISO 4309, while
scattered external strand fractures can be tolerated. See the table in ISO 4309. Only three
external scattered strand fractures within a length of 6xd are permitted for this type of steel
rope. The maximum applied service life for this rope is therefore theoretically about seven
months, assuming that the crane has been in normal use for 15 months,
The investigation found that MH Wirth had not documented requirements for steel rope and
the type of rope the system was designed for. No service life calculations were carried out for
the system. Nor was this issue covered in the user or maintenance manuals, or in other project
documents.
Sheave with a diameter of 18xD/d
It emerged in interviews that experience from Gullfaks C called for the steel rope to be
protected inside the guide beams to avoid being damaged during material handling when the
deck crane was used for lifts to the pipe deck. As a result, 18xD/d was chosen because it fitted
well with the design and dimensioning of the beams. This choice also accords with the
recommendation in DNV GL 2.22 that 18xD/d can be used as the smallest sheave diameter.
The standard is normative and fairly general and has failed, among other considerations, to
address complicated assemblies and arrangements involving the use of multiple sheaves and
where the steel rope could be led over several sheaves, change direction several times and so
forth. Special assessments must be made where such designs are concerned. The standard was
probably not entirely suitable for this particular design.
Winch with a drum diameter of 18xD/d
It emerged during interviews with MH Wirth that the choice of drum diameter was related to
the sheave diameter. The use of a drum diameter of 18xD/d is unlikely to have made any
appreciable contribution to steel rope fatigue, since the latter runs in and out of the drum less
frequently than over the sheaves.
Positioning of the winch
The winch drum is positioned at right angles to the sheaves. This reflects limited space and
the need to avoid blocking an exit from the drilling module. It has resulted in an unfortunate
fleet angle between winch drum and S1, which has contributed to fatigue in the rope and the
load on the sheave. The fleet angle has a bigger impact on rotation-resistant rope than on
traditional types. It was 1.9 degrees for S1, and the winch drum was offset in relation to this
sheave. In addition, a fleet angle was introduced by the positioning of the winch drum and the
rope track within it, so that the total fleet angle was considerably larger than 1.9 degrees. This
meant that the point on the rope subject to the biggest load (where the break occurred) has
been subject to a fleet angle considerably larger than 1.5 degrees, which is the maximum
angle specified by the manufacturer for the relevant rope.

14
Winch/sheave arrangement and load on the steel rope
The average service life for steel rope will depend on the number of sheaves and the spooling
direction in a hoisting arrangement. See figure 8.
Figure 8 An example of the average service life of steel rope, depending on the number of sheaves and the
direction of the rope. (Casar)
The winch drum on the HTV Eagle was underspooled in relation to S1, which was
underspooled and thereby gave rise to an S bend (reversed bend) on this sheave. S2 was also
underspooled, and the rope acquired a further S bend from S1. S3 is spooled the same way as
S2, producing a total of two successive S bends for S2 and S3. See figure 9.
Figure 9 The winch arrangement for the HTV Eagle crane. (Statoil investigation report)
Key: Endefeste = end attachment; Last = load
According to W Giertsen Service AS, it is unfortunate that the angle between S1 and the drum
means that the rope is only in contact with one side of S1. That creates rotation in the rope,
which reduces service life while greatly enhancing the threat of a kink (birdcage/twist),
particularly with slack rope. While the winch is underspooled and S1 is overspooled, the big

15
distance involved (25 metres) probably means that this is not an issue. However, a much
greater problem is the S bend between S1 and S2, where the fatigue/break occurred. Steel
rope which lifts its maximum load (14.4 + 3.5 tonnes) continuously is more exposed to
reduced service life in the event of an S bend than on equipment where the load varies from
zero to the maximum safe working load (SWL). See the report from W Giertsen Service AS.
The combination of rotation-resistant steel rope of high tensile strength, led over multiple
sheaves of a small diameter (18xD/d) and subject several times to S bends during each crane
operation, with a relatively high fleet angle between winch drum and upper sheave has
resulted in loads which have resulted in a short service life for the rope. No service life
calculations were carried out for it. The investigation found that the fatigue occurred in the
area subject to the largest number of passes over several sheaves during each work operation
by the crane.
Conversation with MH Wirth revealed that components in the hoisting arrangement were
largely chosen on the basis of the DNV GL 2.22 standard for certification of lifting appliances
and of products delivered earlier which involved rotation-resistant steel rope for winch and
hoisting arrangements. Where the choice of rope is concerned, DNV GL 2.22 specifies that
the manufacturer should be involved to ensure that a product with the right properties is used.
This was not done with the design for the HTV Eagle crane on GFB.
During its review of project documentation, including the FMECA, the team could not see
that the steel rope was identified or classified as a safety-critical component in the hoisting
arrangement. Nor were there any indications that service life calculations had been carried out
for components in the hoisting arrangement, including the rope.
4.2.2 Failure to follow up earlier incidents
On 1 January 2016, a birdcage was discovered on the steel rope for the HTV Eagle crane, and
broken strands were found on it. KCAD and MH Wirth concluded that the wrong rope type
had been installed, since right-hand lay rope was installed on a drum for left-hand lay. The
replacement was left-hand lay, but differed in tensile strength from the previous rope. No
assessment was made of whether this rope grade was correct for the crane arrangement, and
no particular inspection or maintenance of the rope was subsequently carried out.
The technical report subsequently published by MH Wirth does not reflect on other causes of
the incident than the rope having the wrong lay. A report from Kverneland Aqua AS to MH
Wirth states: “as installed, the rope will have S bends. Such bends could help to limit the
service life of the rope considerably – particularly with small rope-sheave dimensions.”
This did not result in any documented assessment of the rope’s service life. The report from
Kverneland Aqua AS also recommended a D/d ratio of 26, but this was again not taken into
account by MH Wirth nor communicated to Statoil or KCAD.
On 30 July 2016, the roller bearing in S1 on the HTV Eagle crane failed. Synergi contains the
following observation: “The winch is installed in such a way that the drum is at right-angles
to the rope sheave. In other words, the fleet angle of the steel rope across the winch drum
imposes transverse forces on the sheave/bearing. The preventive measure here is to replace
the sheave every six months.”

16
Neither KCAD nor Statoil assessed the possible consequences of this arrangement for the
rope.
These incidents ought to have initiated new follow-up routines and better methods for
inspection and maintenance of components in the hoisting arrangement. This would probably
also have identified that the design was deficient.
4.2.3 Insufficient knowledge of and expertise on steel rope
Statoil, Aibel, MH Wirth and KCAD all failed to assess the steel rope as a safety critical
component, even though it is solely responsible for supporting the weight of the boom and
load.
The boom weighs about 14.4 tonnes without load and can lift 3.5 tonnes. This means the rope
will be under a continuous load of at least 14 tonnes when the crane is not parked on the pipe
deck.
The rope used was a rotation-resistant type with high tensile strength, so that a rope with a
relatively small diameter can cope with a high load. The disadvantage is that high tensile
strength makes the rope stiff and unsuitable for a sheave diameter of 18xD/d.
In addition, checking a rotation-resistant steel rope for fatigue is very difficult. Fatigue caused
by large bending loads over small sheaves will cause strand fractures in the core which are not
detectable by visual checks. After the incident, KCAD incorporated visual checks of the steel
rope as a corrective measure in the maintenance system. However, this form of inspection has
its limits for detecting internal wear, broken strands and fatigue because they occur in the rope
core. This was demonstrated when the rope was taken out in January 2017 in order to install a
new sheave. Following a visual inspection, it was reinstalled despite having almost certainly
already reached the end of its fatigue life and being unacceptable for reinstallation.
4.2.4 Monitoring/inspection of steel rope
KCAD had only established visual checks of the rope, even though it is almost impossible to
detect fatigue in rotation-resistant steel rope in this way. Only external damage or wear would
be identified visually.
No system or routines were established to monitor the service life of or the number of load
cycles for the rope, even though the system is designed to be able to register the number of
lifting and lowering cycles for the boom. Only a replacement interval of 1.5 to two years is
described. Nor was provision made for assessing the type of rope (rotation-resistant) or its
sheave arrangement, or the pattern of use and operating time for the crane.
The PSA was told in interviews that the lists issued for short-term maintenance/lubrication
routines were so extensive that completing them within the allotted time was challenging. In
addition, the language in maintenance and inspection routines was too generalised to ensure
consistent implementation. The daily routine for the crane, for example, was described as
“Carry out a pre-use check of the lifting equipment”, and “Check the rope for damage and
deformation before use and during operation”. Nothing was said about particular wear sites or
vulnerable areas which called for special attention. Nor was provision made for access to the
most vulnerable areas.

17
Inspection and maintenance routines are vague and do not describe how the work is to be
done. As a result, inspection and maintenance of the steel rope can become dependent on the
person concerned and ambiguous. The work description for the rope in the maintenance
procedure for crane inspection, which is to be carried out every second, sixth and 12th month,
states: “inspect the rope for damage and wear in accordance with the applicable
requirements”. However, what requirements have been set by KCAD for inspecting the rope
are not specified in more detail.
No dimensional measurements of the rope were made on installation, nor when it was taken
off and inspected in January 2017. This would not have had an effect on the installed rope, but
maintenance requirements must be tailored to the equipment.
5 Potential of the incident
5.1 Actual consequence
The actual consequence of the crane boom falling onto the pipe deck was substantial material
damage to the crane and to the cable tray for the traverse crane on this deck. In addition, the
incident caused a halt to activity. Statoil has estimated the total financial cost at NOK 66
million.
Figure 10 The crane with bent crane arm and broken gripper arrangement.
Figure 10 shows the outer boom segment of the crane after it fell to the pipe deck. The
segment (striped red and yellow) has been bent by 90 degrees. The cable tray for the traverse
crane is deformed, while the gripper arrangement for loads hangs over the edge of the deck.
The railing broke off and fell towards the BOP deck, where it landed in the safety net. Figures
11–13 show other material damage.
Figure 11 The outer jib with the broken and detached gripper arrangement.
The gripper arrangement has been fractured.
One of the grippers is detached and lying on
the other side of the outer jig.
The crane with a bent outer boom segment.
The detached gripper arrangement
after it broke in two.

18
Figure 12 Photograph taken from below, under the pipe deck. Damage after the crane boom hit the deck.
Figure 13 The railing was broken off and fell towards the BOP deck, where it landed in the safety net.
5.2 Potential consequence
Under slightly different circumstances, the incident could have caused serious personal
injuries with the potential for a fatal outcome. A few minutes earlier, two people had
unhooked a load and adjusted the grippers on the gripper yoke for 3 ½-inch drill pipe. The
deck under the crane had been washed earlier the same day.
Had the derrick been positioned on a well slot further from the pipe deck, the boom could
have fallen straight down to the hatch/BOP deck and caused substantial material damage,
including to the well control equipment.
6 Observations
The PSA’s observations fall into two principal categories.
Nonconformities: observations where the PSA establishes a breach of/failure to comply
with the regulations.
Improvement points: observations where the PSA believes a breach of/failure to comply
with the regulations has occurred, but lacks sufficient information to establish this.
Damage to the underside of the
pipe deck after the crane boom fell.
Railing caught by the safety net over
the BOP deck.

19
6.1 Nonconformities
6.1.1 Risk assessment of equipment
Nonconformity Inadequate identification of risk.
Grounds The responsible party must choose technical, operational and organisational solutions which
reduce the probability that damage, faults, hazards or accidents will occur.
It emerged from the document review and conversations that neither Statoil nor MH Wirth
had assessed the steel rope as a safety-critical component, even though it alone bears the
whole weight of the crane boom and load. A single failure, such as the rope breaking, can
accordingly have big consequences.
Statoil defined the HTV Eagle cranes as a lifting facility with a low risk level, since it was
regarded as well-proven technology. Its certification is based on a low-level verification level
as defined in DNV-OSS-308, despite a number of design changes from the HTV Eagle crane
on Gullfaks C.
The FMECA did not identify and classify the steel rope as a safety-critical component in the
system, even though activities conducted on the drill floor and pipe deck meant that personnel
had to work beneath and close to the crane – when hooking loads on and off, for example, and
adjusting the gripper yoke. Nothing prevents the crane falling down if a single failure occurs
with load-carrying components during these activities. Nor is it possible to stop the crane
falling down when it is parked in the derrick.
Requirements
Section 4 of the management regulations on risk reduction
Section 17 of the management regulations on risk analyses and emergency preparedness
assessments
Section 5 of the facilities regulations on design of facilities
6.1.2 Investigation of and improvement measures following earlier incidents
Nonconformity Inadequate identification, investigation and follow-up of previous hazards and accidents.
Grounds The responsible party must ensure that hazards and accidents which could or have caused
acute pollution or other damage are registered and investigated to prevent repetition.
Earlier incidents with this crane where that had not been done emerged during the
investigation.
On 1 January 2016, a birdcage was discovered on the steel rope for the HTV Eagle crane, and
broken strands were found on it. KCAD and MH Wirth concluded that the wrong rope type
had been installed, since right-hand lay rope was installed on a drum for left-hand lay. The
replacement was left-hand lay, but differed in tensile strength from the previous rope. No

20
assessment was made of whether this rope grade was correct for the crane arrangement, and
no particular inspection or maintenance of the rope was subsequently carried out.
The technical report subsequently published by MH Wirth does not reflect on other causes of
the incident than the rope having the wrong lay. A report from Kverneland Aqua AS to MH
Wirth states: “as installed, the rope will have S bends. Such bends could help to limit the
service life of the rope considerably – particularly with small rope-sheave dimensions.”
This did not result in any documented assessment of the rope’s service life. The report from
Kverneland Aqua AS also recommended a D/d ratio of 26, but this was again not taken into
account by MH Wirth nor communicated to Statoil or KCAD.
On 30 July 2016, the roller bearing in S1 on the HTV Eagle crane failed. Synergi contains the
following observation: “The winch is installed in such a way that the drum is at right-angles
to the rope sheave. In other words, the fleet angle of the steel rope across the winch drum
imposes transverse forces on the sheave/bearing. The preventive measure here is to replace
the sheave every six months.”
Neither KCAD nor Statoil assessed the possible consequences of this arrangement for the
rope.
KCAD asked MH Wirth to verify that the sheave would cope with the oblique pull. This was
assessed and confirmed, but MH Wirth did not evaluate the possible consequences of the
arrangement for the steel rope.
Crane and lifting specialists in Statoil and at KCAD had expressed concern over the fleet
angle and wear on the sheave which could affect the rope, but these comments were not
followed up in a systematic manner.
In other words, the incidents with the rope and the failure of the roller bearing in the sheave
were not adequately investigated to prevent recurrence. Only minor changes were made to the
maintenance programme by expanding the visual inspection, but this cannot identify fatigue
in rotation-resistant steel rope
Requirements
Section 20, paragraph 1 of the management regulations on registration, review and
investigation of hazard and accident situations
Section 19, paragraph 1, litera e of the management regulations on collection, processing and
use of data
6.1.3 Utilisation of expertise
Nonconformity Insufficient use of crane and lifting expertise when specifying crane requirements.
Grounds Before decisions are taken, the responsible party must ensure that issues related to health,
safety and the environment have been comprehensively and adequately spelt out. That was
not the case here with regard to the HTV Eagle crane (Statoil’s specifications).

21
Users of the HTV Eagle crane on Gullfaks C were involved in order to benefit from their
experience. One result was the requirement that the rope should be protected by incorporating
it in the crane’s H beams in order to reduce the threat of damage when lifting equipment to
the drill floor with the deck crane. That led in turn to a reduction in sheave diameter from
26xD/d on Gullfaks C to 18xD/d on GFB, without any assessment of what effect these
changes would have on the rope’s service life. This should have been identified by involving
relevant crane and lifting expertise in the project.
Requirements
Section 11 of the management regulations on the basis for making decisions and decision
criteria
See section 8 of the management regulations on internal requirements
Section 14 of the management regulations on manning and competence
6.1.4 Responsibility for taking delivery and operation of equipment
Nonconformity Inadequate follow-up and checks when taking delivery of and operating machinery and
equipment.
Grounds The operator must ensure that everyone who does work for it complies with the requirements
specified in the health, safety and environmental legislation.
Taking delivery
When taking delivery and before starting to use the machine/crane, Statoil’s responsibilities
include seeing to it that the machinery regulations have been complied with, and that
necessary documentation and documents – such as spare part lists, maintenance routines and
instruction manuals – have been provided. One finding from the investigation team’s
document review is that the spare parts list was deficient and that the maintenance routines
were incomplete and unsuitable for the steel rope in question. The operation manual, for
example, had specified a rope replacement interval of 1.5 to two years, but this was not based
on service life calculations. No service life calculations were made for the rope.
Operation
Statoil has a responsibility for following up the drilling contractor’s work on the facility,
where its enterprise of competence in turn has a responsibility for following up the
maintenance and checking of offshore lifting equipment. A number of incidents with the HTV
Eagle crane were handled by KCAD through improvements implemented in collaboration
with MH Wirth. These incidents were treated by KCAD as remedial work for MH Wirth.
KCAD and Statoil’s rig representative failed to appreciate that the relevant incidents with the
crane should have prompted extraordinary checks and follow-up by the enterprise of
competence (see Statoil doc OM 209). According to information from interviews, Statoil’s
enterprise of competence was not involved in preparing or implementing the measures taken.
The investigation team takes the view that Statoil, including its enterprise of competence, has
failed to comply with its own requirements for taking delivery and for follow-up of control
and maintenance of crane and lifting equipment on GFB.

22
Requirements
Section 20 of the activities regulations on start-up and operation of facilities
Section 7 of the framework regulations on responsibilities pursuant to these regulations
See section 18 of the framework regulations on qualification and follow-up of other
participants
6.1.5 Maintenance
Nonconformity Deficiencies in the maintenance programme for the steel rope.
Grounds Failure modes which could present health, safety or environmental risk must be
systematically prevented with the aid of a maintenance programme.
It emerged from conversations with personnel on GFB and the documentation review that the
maintenance programme for steel rope does not specify the methodology and tolerance
requirements when inspecting the rope.
The inspection scope in KCAD’s maintenance programme is limited to a visual check of the
rope, and no physical method is specified.
When the sheave was disassembled and replaced, the whole rope was inspected and approved
on GFB. What the inspection comprised is not recorded in the maintenance programme.
MH Wirth’s operational description (Doc 880015-HA-022) proposes a measurement for the
work done by the steel rope in section 10.3.2 (“Winch rope monitoring. In order to plan
maintenance more easily, the control system will log the hours in mode and metres run. These
values are shown in the service display for the HTV Eagle”). However, KCAD did not make
this part of the maintenance routines.
Requirement
Section 47 of the activities regulations on maintenance programme
7 Other comments
Poor visibility from crane cabin It was observed during the investigation that the window pane in the HTV Eagle crane cabin
was broken, and that visibility from the cabin was thereby sharply reduced. The pane was of
toughened glass, but had not fallen to the deck because it was laminated.
KCAD explained that the pane was registered as broken on 25 October 2016 (Synergi
1488683), but that the damage had not been repaired in 133 days. The crane had been used
without special restrictions over a long period.
8 Barrier assessment
A brief assessment has been made of the barriers which functioned and failed to function.

23
The barriers are assessed in relation to the technical, organisational and operational barrier
elements.
Non-functioning
barriers
Functioning
barriers
Technical
elements
Organisational
elements
Operational
elements
Technical Individual
faults can lead
to failure and
fault modes on
the HTV Eagle
crane.
No system
exists for
parking and
disengaging
the steel rope
when the crane
is parked in the
derrick.
Inadequate
knowledge of
steel rope.
Inaccurate
description of
maintenance
intervals in the
user manual.
Maintenance
system
Unclear
description of
inspection
routines and
maintenance
tasks.
Maintenance Inadequate
knowledge of
maintenance
requirements for
steel rope.
Follow-up/
learning from
earlier incidents
Responsibility for
the equipment
and for following
up incidents was
spread between
several companies
and people, and
became less clear.
Procedure for
cordoning off
the area under
the HTV
Eagle crane.
In accordance
with operational
routines.
9 Discussion of uncertainties
We have not identified any uncertainties with regard to the course of events or causes.

24
10 Statoil’s investigation report
The incident has been investigated by Statoil’s internal audit function (COA INV), and the
PSA received its report on 8 June.
This report’s description of the course of events and causes by and large coincides with the
investigation team’s findings and assessments.
A number of the recommended measures in the report are rather vague. Measures are phrased
in such a way as “secure that ...”, for example, without describing how this should be done or
what activities are to be performed. Nothing is said about a systematic review of similar crane
and lifting equipment with rotation-resistant rope.
Statoil has sent the damaged steel rope and sheave to W Giertsen Service AS for assessment
and investigation. The investigation team has taken note of the assessments of the actual and
potential consequences and the material technology investigation and analysis
11 Appendix
A: List of documents taken into account in the investigation.
B: Overview of personnel interviewed.