Investigating allergic effects on environmental exposure ... Allergy - Antonella Muraro.pdf ·...
31
Antonella Muraro Referral Centre for Food Allergy Diagnosis and Treatment Department of Pediatrics , University of Padua Padua , Italy [email protected] ALLERGY SCHOOL Investigating allergic effects on environmental exposure BRINDISI ( Italy) July 2 - 5 th , 2014 Food A ller gy
Transcript of Investigating allergic effects on environmental exposure ... Allergy - Antonella Muraro.pdf ·...

Antonella Muraro
Referral Centre for Food Allergy Diagnosis and Treatment
Department of Pediatrics, University of Padua
Padua, Italy
ALLERGY SCHOOL
Investigating allergic effects on environmental exposure
BRINDISI ( Italy)July 2-5 th, 2014
Food Allergy

FOOD ALLERGY
ADVERSE HEALTH EFFECT ARISING FROM
A SPECIFIC IMMUNE RESPONSE THAT OCCURS REPRODUCIBLY
ON EXPOSURE TO A GIVEN FOOD
NIH-NIAID Food Allergy Guidelines JACI 2011

2 MAIN GROUPS ACCORDING TO THE
MECHANISMS
- IMMUNOLOGICAL (IgE/non IgE) =FOOD ALLERGY
- NON IMMUNOLOGICAL = INTOLERANCE
enzimatic (lactose intolerance)
toxic ( sgombroid syndrome)
pharmacologic
ADVERSE REACTIONS TO FOODS

Outline
Epidemiology
Patient’s diversity : phenotypes
Pollen Food Allergy
Need for individualized therapy
Burden of Food Allergy

• Prevalence:– 3 million school age children (3.9%)
– 18% increase since 1997
Branum 2009 Pediatrics. 124:1549-55
• 7 most common food allergens in Western countries.– Milk, egg, peanut, tree nuts, shellfish, soy, wheat
• Peanut allergy– Prevalence ~1%
– Most common cause of anaphylaxis in children presenting to the ED
– Most common cause of fatal food anaphylaxis
• Standard of care– Avoidance of only foods appropriately diagnosed
– Self-injectable epinephrine/antihistamines
Vander Leek, J Peds 2000
Bock, J Allergy Clin Immunol 2007
EAACI GUIDELIINES 2014
Burden of Food Allergy
Epidemiology (i)

Burden of Food Allergy
Epidemiology (ii)
• Reported increase in severe allergic
reactions from food
– Food-induced anaphylaxis is a leading cause
of outpatient anaphylaxis
– Food-related anaphylaxis increased 13% per
year in a 12-year period
– Food-induced anaphylaxis admissions have
increased in the UK (1990-2004)
– in Australia (1993-2003)
1Webb Ann Allergy 2006, 2Sampson Pediatrics 2003, 3Novembre Pediatrics 1998, 4Bock JACI 2001, 5Mehl Allergy 2005, 6Poulos JACI 2007, 7Gupta Thorax 2007

Patients diversity

SKINGUTRESPIRATORY TRACT
SINGLE OR ASSOCIATED MANIFESTATIONS
SYSTEMIC MANIFESTATIONS
- Urticaria/angioedema- Atopic Dermatitis- Gastroenteropathies- Rhinitis- Asthma
Anaphylaxis
FOOD ALLERGYClinical manifestations

EAACI Task Force on Nomenclature
FOOD HYPERSENSITIVITY
FOOD ALLERGYNON ALLERGIC
HYPERSENSITIVITY
IgE-MEDIATED FOOD ALLERGY
NON IgE-MEDIATED FOOD ALLERGY
FOOD ALLERGY
Allergy, 2001; 56: 813J Allergy Clin Immunol 2004 113;832-6
MixedIgE & nonIgE

IgE Non-IgE
Immediate vomiting, diarrhea, urticaria, respiratory symptomsOral allergy syndrome
Eosinophilic Allergic Esophagitis
Eosinophilic Allergic Gastritis
Eosinophilic Allergic Gastroenterocolitis
Atopic Dermatitis
Food Enterocolitis
Food Proctitis
Food Enteropathy
Atopic dermatitis
Heiner Syndrome
Celiac disease
Sampson HA, et al J Pediatr Gastroenterol Nutrit 2000; 30: 587-594
FOOD ALLERGY CLINICAL MANIFESTATIONS

Does one size fit all?
FOOD ALLERGY Phenotypes

Early v’s late DiseaseSensitization v’s Clinical reactivity
Mild v’s Severe
Persistent v’s Transient
Food Allergy Phenotypes
Early v’s late onset
Pollen Food Allergy

Patient’s diversity (i)Symptoms:
Coexistence of immediate IgE mediated with late non IgE mediated.
Severity:Mild v’s Severe
Cow’s milk: baked-milk tolerant children have milder symptoms than non tolerant
Egg: Baked-egg tolerant children had a low incidence of severe reactions and low egg specific IgE levels
Peanut: tolerant patients had smaller size and lower specific IgE values

•TIMING IN ONSET OF SENSITIZATION
EARLY v’s LATE
•TIMING IN ACHIEVING TOLERANCE
Transient v’s Persistent
Patient’s diversity (ii)

Patients’ diversity (iii)
1
2
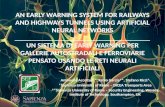
Heating
MI
IM
K
LLI
M
KM
I KL
L
K
Effect of Heating on Milk Proteins
LLI
M
KM
I
Nowak-Wegrzyn A: EAACI Food Allergy and Anaphylaxis Meeting- FAAM 2011
Majority of children outgrow milk or egg within first 6 years of life
- children who “outgrow” milk / egg allergy have IgE directed primarily at conformational epitopes

Patients’ diversity (iv)
Role of “informative” Epitopes
– Epitope recognition correlates with peanut allergy severity
– Patient with milk allergy and milk tolerance have different epitope recognition patterns
– Certain milk IgE epitopes can be used as candidate biomarkers to predict the development of tolerance to milk (epitope diversity)
Nowak-Wegrzyn A et al JACI 2008Wang J et al JACI 2010

IgE diversity corresponds to different phenotypes of milk allergy

IgE affinity correlates to different phenotypes of milk & egg allergy:
Role of Informative Epitopes

Patient Diversity (v)How to Identify groups of patients homogeneous
FOR:
• clinical symptoms
• reaction features
• Epitopes Recognition
How to define the Allergic Profile ?
FOR: • Risk of Severe Reactions
•Prognosis
•Tailored treatment

Role ofComponent-Resolved Diagnostics
(CRD)• CRD have been introduced in
order to increase the probabilityof
–True Food Allergy diagnosis
– Identify patients at high risk of reactions
– Identify patients more prone to persistent disease
Hansen et al. J Allergy Clin Immunol. 2009 May;123(5):1134-41, 1141.e1-3.

Suspicion of egg allergyIs it allergy? Risk for severe reactions?
Test with ImmunoCAP AllergenEgg White (f1) + Ovomucoid (f233)
Egg White: neg
Ovomucoid: neg
Egg White: posOvomucoid: neg
Egg White: pos
Ovomucoid: pos
Low risk for
Clinical Reactions
to eggAbsence of IgE antibodies to
ovomucoid indicates tolerance to ingestion of hard-boiled and egg
in baked cakes
Increase risk for
persistent egg
allergy
Mittag JACI 2004, Ballmer-Weber JACI 2007
Kleine-Tebbe JACI 2002, Treudler JInvACI2008
Van Zuuren Allergy 2010, Kosma Acta Pediatr 2011 Holzhauser JACI 2009
Risk for clinical
reactions to egg High risk for clinical
reactions to egg

Suspicion of soy allergyIs it allergy? Risk for severe reactions?
Test with ImmunoCAP AllergenSoybean (f14) + Gly m 4 + Gly m 5/Gly m 6
Soybean: neg
Gly m 4: neg
Gly m 5/Gly m 6: neg
Soybean: pos or
neg
Gly m 4: pos
Gly m 5/Gly m 6: neg
Soybean: pos
Gly m 4: pos or neg
Gly m 5/Gly m 6:
pos
Low risk for
reactions to soy
If patient is pollen-allergic:
Risk for reactions to soy
- predominantly OASbut sometimes severe
Risk for severe
reactions to soy
Mittag JACI 2004, Ballmer-Weber JACI 2007
Kleine-Tebbe JACI 2002, Treudler JInvACI2008
Van Zuuren Allergy 2010, Kosma Acta Pediatr 2011 Holzhauser JACI 2009

Pollen Food Allergy

Profilins
• Sensitisation observed in
pollen allergic patients
• BP<GP
• Monosensitised only in GP
• Pollen allergy preceeds the
fruit allergy
• OAS > 90%
20-75%
13-56% ms
13%
4% ms
19-50%
0-25% ms
15-74%
0-5% ms

PR-10 - Bet v 1 family
• Frequency related to BP
exposure
• BP allergy preceeds the
fruit allergy
• OAS > 90%
0-13%3%
0-91%
0% ms
0-67% ms
92-100%
26-86% ms

Lipid Transfer Protein –LTP
47-100%
44-100% ms
97%
84%ms
13-100%
0-3%

History suggestive of
pollen-food syndrome
Confirmed by SPT
with fresh
material and/or specific IgE
Not confirmed by SPT with fresh
material and/or specific IgE
Oral Challenge
Clinical Features Clinical Features
OAS Systemic Reactions
Both Labile and stable
allergens are suspect
IgE to Bet v 1Positive IgE to Bet v1- 2 Pos
Stable Allergen are suspect
IgE to LPT positiveIgE to seed storage
protein positive
Sensitization
To Bet v1-like
Allergens
Sensitization to both
Bet v1-like allergens and profilin
NO ORAL CHALLENGE NO ORAL CHALLENGE
NO ADRENALINENO ADRENALINE
Sensitization
To LTP (Pru p 3)
Evaluate for potential
cross-reactivities
NO ORAL CHALLENGE
CARRY ADRENALINE
Sensitization to
Storage Protein
Evaluate for potential
Cross-reactivities
NO ORAL CHALLENGE
CARRY ADRENALINE
POLLEN FOOD ALLERGY
Asero R. et al Int.Arch.Allergy Immunol 2005Bohle B, Allergy 2007

Need for
individualized therapy

Individualized treatment (i)
Age
Type and severity of symptoms
Type of allergen
Multiple food allergies
Level of food specific IgE , recombinant
allergens profile and epitope affinity
IS ESSENTIAL IN APPROPRIATE MANAGEMENT
IDENTIFYING the clinical profileof the food allergic patient with regard to:

Individualized Treatment (ii) Future Directions
• Identify environmental factors affecting the development of food allergy
• Develop biomarkers for identifying phenotypes mainly for severe reactors
• Develop diagnostic tests to correctly identify the phenotype of food allergy: transient-permanent to select patients for IT
•
• Molecular approach in order to optimize
opportunities to achieve hypoallergenicity of the extract