
Invasive Bi-level Positive Airway Pressure (BiPAP): An ...
40
April 29, 2020 Invasive Bi-level Positive Airway Pressure (BiPAP): An Innovative Alternative to Ventilatory Management for COVID-19 Patients Keith Robinson, MD, MS, FCCP Pulmonary and Critical Care Medicine, Syneos Health Hugh Cassiere, MD, FCCP, FACP Chief, Critical Care Medicine North Shore University Hospital, Northwell Health Jhaymie Cappiello, MS RRT-ACCS RCP Educator-Respiratory Care Services Duke University Hospital Prepared for
Transcript of Invasive Bi-level Positive Airway Pressure (BiPAP): An ...

April 29, 2020
Invasive Bi-level Positive Airway Pressure (BiPAP):
An Innovative Alternative to Ventilatory
Management for COVID-19 Patients
Keith Robinson, MD, MS, FCCP
Pulmonary and Critical Care Medicine, Syneos Health
Hugh Cassiere, MD, FCCP, FACP
Chief, Critical Care Medicine
North Shore University Hospital, Northwell Health
Jhaymie Cappiello, MS RRT-ACCS RCP
Educator-Respiratory Care Services
Duke University Hospital
Prepared
for

2© 2020 All rights reserved | Confidential | For Syneos Health® use only
Faculty
Keith Robinson, MD, MS, FCCPPulmonary and Critical Care Medicine
Syneos Health
Hugh Cassiere, MD, FCCP, FACPChief, Critical Care Medicine
North Shore University Hospital
Northwell Health
Jhaymie Cappiello, MS RRT-ACCS RCPEducator-Respiratory Care Services
Duke University Hospital

3© 2020 All rights reserved | Confidential | For Syneos Health® use only
Audience response
Which of the following devices can be adapted to meet
the need for emergency invasive ventilation?1
Hospital BiPAP
Home-use BiPAP
CPAP
Reference: 1. Branson RC, Hess DR, Kallet R, et al. American Association for Respiratory Care: SARS-CoV-2 Guidance Document. American Association for Respiratory
Care, 9425 N. MacArthur Blvd., Ste 100, Irving TX 75063 T: 972.243.2272 W: www.aarc.org. Accessed April 19, 2020.

4© 2020 All rights reserved | Confidential | For Syneos Health® use only
Pulmonary features of COVID-19 associated ARDS
• COVID-19 associated acute respiratory distress syndrome (ARDS) is hypoxic respiratory failure that
results from inflammatory pulmonary responses to the SARS-CoV-2 virus1
– inflamed, dysfunctional alveolar epithelium
– impaired surfactant function
– reduced alveolar fluid clearance; alveoli collapse or fill, resulting in ventilation/perfusion (V/Q) mismatch
• Patients show varying degrees of hypoxemia1
• Unlike typical ARDS, however, respiratory system compliance is often near normal2
References: 1. Luks AM, Freer L, Grissom CK, et al. High Alt Med Biol. 2020 Apr 13. 2. Gattinoni L, Coppola S, Cressoni M, et al. AJRCCM Articles in Press. Published March 30, 2020.

5© 2020 All rights reserved | Confidential | For Syneos Health® use only
Formal guidelines for ARDS careStandard of ARDS care is a low tidal volume (TV) strategy on ventilator support (6 cc/kg ideal weight)1
Reference: 1. Papazian L, Aubron C, Brochard L, et al. Formal guidelines: management of acute respiratory distress syndrome. Ann. Intensive Care 9, 69 (2019). https://doi.org/10.1186/s13613-019-0540-9.
6© 2020 All rights reserved | Confidential | For Syneos Health® use only
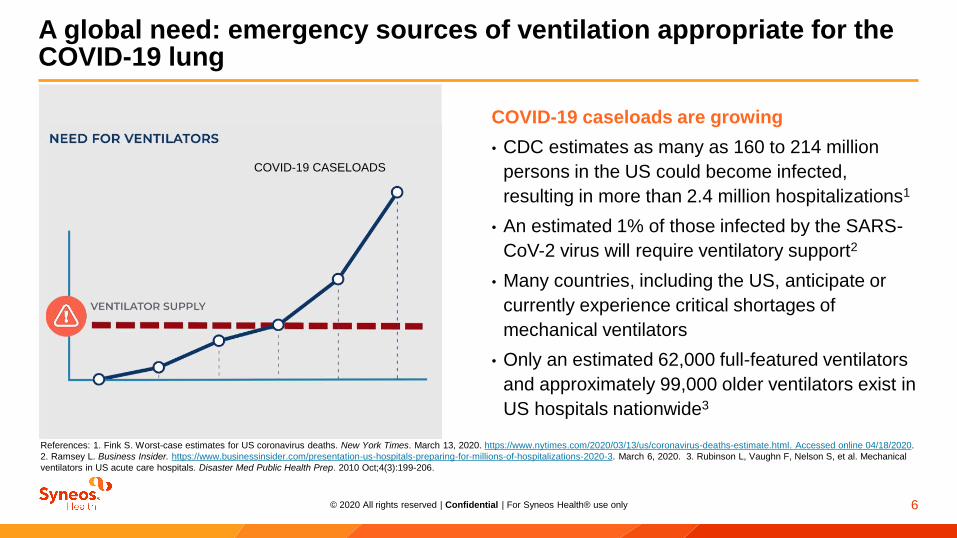
COVID-19 caseloads are growing
• CDC estimates as many as 160 to 214 million
persons in the US could become infected,
resulting in more than 2.4 million hospitalizations1
• An estimated 1% of those infected by the SARS-
CoV-2 virus will require ventilatory support2
• Many countries, including the US, anticipate or
currently experience critical shortages of
mechanical ventilators
• Only an estimated 62,000 full-featured ventilators
and approximately 99,000 older ventilators exist in
US hospitals nationwide3
A global need: emergency sources of ventilation appropriate for the COVID-19 lung
References: 1. Fink S. Worst-case estimates for US coronavirus deaths. New York Times. March 13, 2020. https://www.nytimes.com/2020/03/13/us/coronavirus-deaths-estimate.html. Accessed online 04/18/2020.
2. Ramsey L. Business Insider. https://www.businessinsider.com/presentation-us-hospitals-preparing-for-millions-of-hospitalizations-2020-3. March 6, 2020. 3. Rubinson L, Vaughn F, Nelson S, et al. Mechanical
ventilators in US acute care hospitals. Disaster Med Public Health Prep. 2010 Oct;4(3):199-206.
COVID-19 CASELOADS

7© 2020 All rights reserved | Confidential | For Syneos Health® use only
• Bi-level Positive Airway Pressure (BiPAP) machines
are widely available hospital and at-home devices
providing bi-level positive airway pressure
• Use of BiPAP on an emergency basis for ventilation
in appropriate COVID-19 patients may conserve
ICU beds and delay or reduce the hospital’s need
for mechanical ventilation equipment
– Can meet need for low tidal volume ventilation
– Caution: using BiPAP without intubation may disperse
aerosolized virus into the treatment environment
An emergency solution: adapt BiPAP for invasive use to delay or remove need for mechanical ventilation

8© 2020 All rights reserved | Confidential | For Syneos Health® use only
• Adaptors, filters, and use of appropriate device settings
can enable BiPAP to be used with endotracheal tubes
– The U.S. Food and Drug Administration is temporarily waiving
objections to such device modifications when they do not
create an undue risk1
• Among hospitals adapting BiPAP devices for use in
COVID-19 are:
– Northwell Health, NY
– Massachusetts General Hospital, MA
– Emory Health, GA
– Broward Health Medical, FL
• Do not confuse with CPAP devices for obstructive sleep
apnea, which cannot be used for ventilation and provide
no ventilatory support
What is invasive BiPAP?
CPAP BiPAP
References: 1. U.S. Food and Drug Administration. Enforcement policy for ventilators and accessories and other respiratory devices during the coronavirus disease 2019 (COVID-19) public health emergency:
guidance for industry and Food and Drug Administration Staff. March 2020. www.fda.gov/regulatory-information/search-fda-guidance-documents/enforcement-policy-ventilators-and-accessories-and-other-
respiratory-devices-during-coronavirus. Accessed March 20, 2020.

9© 2020 All rights reserved | Confidential | For Syneos Health® use only
• Non-invasive ventilation (NIV) should only be used in
selected patients with hypoxemic respiratory failure1
• Patients treated with either high-flow nasal oxygen or NIV
should be closely monitored for clinical deterioration1
• Clinicians may consider use of helmet interface or face
mask with BiPAP to support respiratory status1
• Risks include delayed intubation, large tidal volumes, and
injurious transpulmonary pressures1
• To reduce risk to healthcare providers:
– Use local best practices for non-invasive ventilation
– Bag valve masks (BVMs) and other ventilator equipment
should be equipped with HEPA filtration to filter expired air and
minimize aerosolization2
• If the patient isn’t stabilized in a monitored setting within 60
minutes after non-invasive BiPAP, clinicians may elect to
intubate1 and continue use with the BiPAP machine
• This can provide a means to ventilate/oxygenate patients
until a standard ventilator and ICU bed become available,
or in lieu of these resources
if they are not available
Non-invasive or invasive: which BiPAP modality to use?
References: 1. WHO Interim Guidance. Reference number: WHO/2019-nCoV/Clinical/2020.4
2. Centers for Disease Control and Prevention. www.cdc.gov/coronavirus/ 2019-ncov/hcp/guidance-for-ems.html. Accessed March 20, 2020.
Non-invasive BiPAP:
Early in the course of care
Invasive BiPAP:
If the patient isn’t stabilized quickly

10© 2020 All rights reserved | Confidential | For Syneos Health® use only
How to adapt BiPAP for invasive ventilation support*
• Replace mask with adaptor/coupler that enables
connection to endotracheal tube
• Provide humidification (active HME or with filter [HMEF])
– COVID-19 patients (especially those with underlying
respiratory conditions and/or bacterial infections) have been
reported to have difficulty adequately humidifying the airways
and patients develop tenacious, thick secretions that are
occluding their endotracheal tubes
• A leak port must be open to allow expiratory outflow
– HEPA filter on the leak port to prevent virus-containing
aerosols from contaminating room
– Contact manufacturer to obtain appropriate filter
• Program BiPAP device settings for invasive ventilation
If an HME or HMEF is used, it must be fitted between the leak
port and the endotracheal tube1 (AARC)
BiPAP
Pressure
source/controller
Single limb passive circuitLeak port
Filter
Humidifier
*Note: This is general guidance and they should contact the manufacturers for any specific modification questions as each BiPAP is likely different.
Reference: 1. American Association for Respiratory Care. Bilevel Devices Converted to Ventilators. https//www.aarc.org/clinical-resources/bilevel-devices-converted-to-ventilators/.
Accessed April 19, 2020.

11© 2020 All rights reserved | Confidential | For Syneos Health® use only
Invasive BiPAP experience has been positive in resource-poor settings or when mechanical ventilators have been unavailable
Pakistan
In comatose COPD patient responders, invasive BiPAP
significantly (P<0.01) improved coma scale scores, pH,
and PaCO21
India
In comatose COPD patient responders, invasive BiPAP
significantly improved (P≤0.001) coma scales scores, pH,
PaCO2, respiratory rate, and SOFA score2
There are reports of invasive BiPAP use in COVID-19
from Washington State, China3, Italy, France
References: 1. Akhter N, Rizvi NA. Pak J Med Sci. 2017;33(6):1444-1448. doi: https://doi.org/10.12669/pjms.336.13972. 2. Rawat J, Sindhwani G, Biswas D, et al. International Journal of COPD. 2012:7 321–325.
3. Boxue H, Lei S, Guifeng Z, et al. Poster, CHEST. October 2019, 156(4) suppl:A996. doi: https://doi.org/10.1016/j.chest.2019.08.921.
12© 2020 All rights reserved | Confidential | For Syneos Health® use only
Virus containment
considerations
13© 2020 All rights reserved | Confidential | For Syneos Health® use only
Audience response
Which of these can transmit SARS-CoV-2?1
Droplets
Aerosols
Steel
Copper
Aluminum
Wood
Paper
Glass
Latex Gloves
Reference: 1. Kampf G, Todt D, Pfaender S, Steinmann E. Persistence of coronaviruses on inanimate surfaces and its inactivation with biocidal agents. J Hospit Infect. 2020:246-251.
14© 2020 All rights reserved | Confidential | For Syneos Health® use only
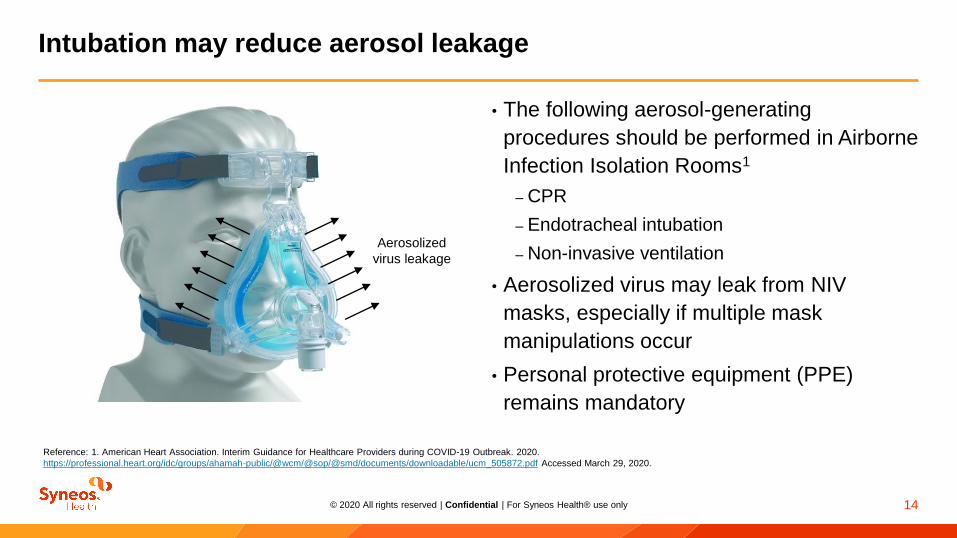
• The following aerosol-generating
procedures should be performed in Airborne
Infection Isolation Rooms1
– CPR
– Endotracheal intubation
– Non-invasive ventilation
• Aerosolized virus may leak from NIV
masks, especially if multiple mask
manipulations occur
• Personal protective equipment (PPE)
remains mandatory
Intubation may reduce aerosol leakage
Reference: 1. American Heart Association. Interim Guidance for Healthcare Providers during COVID-19 Outbreak. 2020.
https://professional.heart.org/idc/groups/ahamah-public/@wcm/@sop/@smd/documents/downloadable/ucm_505872.pdf Accessed March 29, 2020.
Aerosolized
virus leakage

15© 2020 All rights reserved | Confidential | For Syneos Health® use only
Each mask manipulation creates an aerosol risk equivalent to a one-time intubation
Risk of SARS Transmission to HCWs Exposed and Not Exposed to Aerosol-Generating Procedures, and
Aerosol Generating Procedures as Risk Factors for SARS Transmission1
References: 1. Tran K, Cimon K, Svern M, Pessoa-Silva CL, Conly J. (2012). PLoS ONE 7(4): e35797. doi:10.1371/journal.pone.0035797.
Aerosol Generating Procedures Odds ratio (95% CI)
Point estimate Pooled estimate; I2
Manipulation of oxygen mask
(2 cohort studies)
17.0 (1.8, 165.0)4.6 (0.6, 32.5); 64.8%
2.2 (0.9, 4.9)
Tracheal intubation
(4 cohort studies)
3.0 (1.4, 6.7)
6.6 (2.3, 18.9); 39.6%22.8 (3.9, 131.1)
13.8 (1.2, 161.7)
5.5 (0.6, 49.5)
Non-invasive ventilation
(2 cohort studies)2.6 (0.2, 34.5)
3.1 (1.4, 6.8); 0%3.2 (1.4, 7.2)
Mechanical ventilation
(1 cohort study)
0.9 (0.4, 2.0)N/A

16© 2020 All rights reserved | Confidential | For Syneos Health® use only
When to intubate?

17© 2020 All rights reserved | Confidential | For Syneos Health® use only
Audience response
Which of these are potential benefits of earlier intubation?
Reduces negative pressure
that could worsen pulmonary
edema and lower oxygenation
Improves patient comfort
via ventilation support
Airway protection allows
sedation and lowers
aspiration risk
Removes dead space of
trachea from ventilation and
oxygenation considerations
Avoids high risk of
NIV failure and need for
rush intubation
18© 2020 All rights reserved | Confidential | For Syneos Health® use only
Sedation may offer advantages
Sedation options:
All are available options and can be provided to a patient with airway protected

19© 2020 All rights reserved | Confidential | For Syneos Health® use only
Algorithms and device settings

20© 2020 All rights reserved | Confidential | For Syneos Health® use only
Ventilation considerations relevant to COVID-19 ARDS
In patients using excessive inspiratory effort, intubation is high priority
– Avoids excessive negative intrathoracic pressures and self-inflicted lung injury1
Reference: 1. Gattinoni L, Coppola S, Cressoni M, et al. AJRCCM Articles in Press. Published March 30, 2020 as 10.1164/rccm.202003-0817LE. 2. Siegel MD, Hyzy RC. UpToDate. November 26, 2019.
www.uptodate.com/contents/ventilator-management-strategies-for-adults-with-acute-respiratory-distress-syndrome. Accessed March 22, 2020.
PaO2
>55 mm
Hg>88% 7.35 to
7.45
SaO2 Blood pH
Treatment targets

21© 2020 All rights reserved | Confidential | For Syneos Health® use only
Mean SOFA ≤2
COVID-19 (+) or pending status
Those considered for use of NIV with face mask
Moderate ARDS (P/F ratio of 100–200)
Hemodynamically stable
Those with any chronic illness not in exacerbation during ICU stay
Which patients are candidates for emergency invasive BiPAP?
• In general, if patients have lung failure and not more than 2 organ systems in failure,
BiPAP devices may support them adequately
– Caveat: An endotracheal tube with BiPAP has not been evaluated in COVID-19 patients, nor
are there formal recommendations from critical care societies or associations
• Bedside clinicians should consider the severity of failure in multiple organs or other
symptoms of worsening ARDS

22© 2020 All rights reserved | Confidential | For Syneos Health® use only
1
Available for download at
www.covid-bipapinfo.com
Algorithms:
Smart BiPAP

23© 2020 All rights reserved | Confidential | For Syneos Health® use only
1
Available for download at
www.covid-bipapinfo.com
Algorithms:
Standard BiPAP

24© 2020 All rights reserved | Confidential | For Syneos Health® use only
THE FOLLOWING PROTOCOL HAS BEEN DEVELOPED BY NORTHWELL HEALTH FOR EMERGENCY
SITUATIONS ARISING OUT OF THE COVID-19 PUBLIC HEALTH EMERGENCY ONLY.
NORTHWELL IS SHARING THIS PROTOCOL WITH YOU, AT YOUR REQUEST, FOR INFORMATION
PURPOSES ONLY.
YOU SHOULD REVIEW AND ANALYZE THE PROTOCOL FOR YOUR OWN SPECIFIC
EMERGENCY USE PURPOSES AND MAKE YOUR OWN DETERMINATION AS TO WHETHER
AND WHEN DEPLOYMENT OF THIS PROTOCOL IS NECESSARY.
Emergency protocol for using Philips Respironics V60 ventilator with pressure control ventilation
(PCV) option as a pressure-controlled ventilator using a conventional bipap circuit
Authored by Hugh Cassiere, MD, Stanley John RT, Todd Goldstein, PhD
You may use the conventional exhalation valve and/or circuit sold by Philips Respironics
**In situations where the manufacturer’s connection is unavailable, Northwell Health has
successfully replicated and tested a 3D printed solution that is autoclavable and reusable. As the 3D
printed solution should only be used in an emergency situation, it is recommended that the bacterial
or viral filter be placed between the ET tube and the 3D printed adapter. (Photo at end of document.)

25© 2020 All rights reserved | Confidential | For Syneos Health® use only
Preliminary
results

26© 2020 All rights reserved | Confidential | For Syneos Health® use only
First experience was on
patients with non-COVID-19
respiratory failure
• Allowed us to free up FDA-
approved invasive ventilators
• Over the course of 3 weeks we
invasively ventilated 50–60 such
patients
• As of last week we continued to
ventilate 12–15 patients
Second experience was on
“surge” COVID-19 patients
• On occasion, sites were
depleted of ventilators due to
surges of COVID-19 patients
being intubated
• Providers used the protocol and
adapters were set up to rescue
these patients while awaiting
ventilator resupply
Third experience was upfront
use on COVID-19 ARDS
respiratory failure patients
• At peak of our pandemic up to
80 patients were invasively
ventilated using the V60 BiPAP
Northwell Health Experience – Philips Respironics V60 BiPAP
Started using the Philips Respironics V60 BiPAP March 2020

27© 2020 All rights reserved | Confidential | For Syneos Health® use only
Add 2 HEPA filters, one
immediately connected to the
V60 main gas port outlet and the
second HEPA gets connected to
the exhalation valve port closer
to the ET/Trach
We recommend that the HEPA
filter on the exhalation valve
port be connected to a blind
reservoir
*In order to connect to an ETT tube
you need to use the Philips
Respironics conventional exhalation
valve and/or circuit kit

28© 2020 All rights reserved | Confidential | For Syneos Health® use only
147525 v.2
Turn on machine and hit the Menu
tab. Please ensure the patient is not
connected to the V60 machine
Under the Menu tab select the
option for Mask/Port
Select →ET/Trach option
(extreme left)
Hit Accept
Then choose type of exhalation port
Select →Other
Hit Accept

29© 2020 All rights reserved | Confidential | For Syneos Health® use only
Perform exhalation port test
Keep circuit open
The machine will detect the open
circuit and ask you to occlude the
outlet port that connects to the
patient end of the circuit
Now occlude the outlet keeping the
exhalation valve port open
Hit Start Test
Test takes 4-5 seconds; when you
see the green bar the test was
completed successfully, or you
passed the test

30© 2020 All rights reserved | Confidential | For Syneos Health® use only
Select mode–Batch PCV
Place patient on the appropriate
pressure settings parameters prior
to activating mode as follows:
The EPAP will be the same as
the PEEP
For IPAP use the plateau
pressure measured on the
conventional ventilator as a
baseline
The Fi02 would be the same
The ramp should be turned off
The rise time can be adjusted
based on patients demand. We
recommend a rise time of 3

31© 2020 All rights reserved | Confidential | For Syneos Health® use only
Now activate the batch change by hitting Select (Active Batch Change)

32© 2020 All rights reserved | Confidential | For Syneos Health® use only
3D printing protocol
There are many different types of 3D
printing modalities that can be used for this
adapter. Please ensure that the STL is
printed with a biocompatible material.
*HEPA Filter placed after the adapter.
147525 v.2

33© 2020 All rights reserved | Confidential | For Syneos Health® use only
Equipment useful at bedside during invasive BiPAP
Use of BiPAP with intubation may require equipment normally used for patients on
mechanical ventilation:Suction device
to remove pulmonary secretions
Pulse oximeter
to measure saturation of oxygen in blood
BVM (often referred to as an Ambu® bag)
to provide positive pressure ventilation
Telemetry system
to measure vital signs (e.g., heart rate, breathing, blood pressure)
Capnography
to monitor CO2, if available

34© 2020 All rights reserved | Confidential | For Syneos Health® use only
Monitor:
• Tidal volume; Target tidal volume to 6 mL/kg
predicted tidal volume
• SpO2: target 88%–95%
• Arterial blood gases
• Capnography is not necessary unless needed as
a disconnect alarm
• Also important to set alarms – particularly the
disconnect alarm
• Titration
• Physical assessment – LOC
• RR comfort therapy
• Observations: accessory muscles, pulse oximetry,
HR, vitals
• Secondary driver or device back-up
• Review of analyzing blood gas (TcCO2 or EtCO2?)
• Safety considerations
• Ongoing management – potential clinical
complications (pneumothorax, gastric distention);
and potential mechanical complications
(inadequate ventilation)
Patient monitoring and intervention considerations
Reference: 1. American Association for Respiratory Care. Bilevel Devices Converted to Ventilators. https://www.aarc.org/resources/clinical-resources/bilevel-devices-converted-to-ventilators/.
Accessed April 19, 2020.
Other considerationsAARC Recommendations1

35© 2020 All rights reserved | Confidential | For Syneos Health® use only
• Prolonged stay in ICU bed shortage vs. short term
• Signs of treatment failure
• Need to prone patient due to refractory hypoxia
• Need for paralytics due to refractory hypoxia
• Multiple organs in failure
• SOFA mean score 3 or more
• Hemodynamic instability
When to progress to mechanical ventilation
ICUED to ICU

36© 2020 All rights reserved | Confidential | For Syneos Health® use only
Conclusion

37© 2020 All rights reserved | Confidential | For Syneos Health® use only
Conclusion
BiPAP machines are widely available devices providing
bi-level positive airway pressure
Use of BiPAP on an emergency basis for ventilation in appropriate
COVID-19 patients may conserve ICU beds and delay or reduce
the hospital’s need for mechanical ventilation equipment
Invasive BiPAP minimizes healthcare worker exposure to aerosols• PPE must be worn and standard precautions taken at all times

38© 2020 All rights reserved | Confidential | For Syneos Health® use only
More information about invasive BiPAP
AARC Guidance
https://www.aarc.org/wp-
content/uploads/2020/03/guidance-document-SARS-
COVID19.pdf
Additional training:
https://www.aarc.org/resources/clinical-resources/bilevel-
devices-converted-to-ventilators/
FDA Guidance
https://www.fda.gov/regulatory-information/search-fda-
guidance-documents/enforcement-policy-ventilators-and-
accessories-and-other-respiratory-devices-during-
coronavirus
HHS Guidance
https://www.hhs.gov/sites/default/files/optimizing-
ventilator-use-during-covid19-pandemic.pdf
NIH Treatment Guidelines
https://covid19treatmentguidelines.nih.gov/critical-care/
Northwell Health
Coronavirus Digital Resource Center:
https://www.northwell.edu/coronavirus-covid-19
3D design and innovation:
https://www.northwell.edu/3d-design-innovation
Syneos Health
www.COVID-BiPAPinfo.com

39© 2020 All rights reserved | Confidential | For Syneos Health® use only
References
American Association for Respiratory Care. Bilevel Devices Converted to Ventilators.
https://www.aarc.org/resources/clinical-resources/bilevel-devices-converted-to-ventilators/.
Accessed April 19, 2020.
AHA (American Heart Association). Interim Guidance for Healthcare Providers during COVID-
19 Outbreak. 2020. https://professional.heart.org/idc/groups/ahamah-
public/@wcm/@sop/@smd/documents/downloadable/ucm_505872.pdf. Accessed March 29,
2020.
Akhter N, Rizvi NA. Application of BiPAP through Endotracheal Tube in Comatose Patients
with COPD Exacerbation. Pak J Med Sci. 2017;33(6):1444-1448. doi:
https://doi.org/10.12669/pjms.336.13972.
Aloud A. Average volume-assured pressure support. SW Respir Crit Care Chron. 2018;6:29-
37.
Boxue H, Lei S, Guifeng Z, et al. Advanced device with auto-titrating EPAP for ARDS patients.
Poster, CHEST. October 2019, 156(4) suppl:A996. doi:
https://doi.org/10.1016/j.chest.2019.08.921.
Branson RC, Hess DR, Kallet R, et al. American Association for Respiratory Care: SARS-
CoV-2 Guidance Document. American Association for Respiratory Care, 9425 N. MacArthur
Blvd., Ste 100, Irving TX 75063 T: 972.243.2272 W: www.aarc.org. Accessed April 19, 2020.
Centers for Disease Control and Prevention. Interim guidance for emergency medical services
(EMS) systems and 911 public safety answering points (PSAPs) for COVID-19 in the United
States. www.cdc.gov/coronavirus/ 2019-ncov/hcp/guidance-for-ems.html. Accessed March 20,
2020.
Fink S. Worst-case estimates for US coronavirus deaths. New York Times. March 13, 2020.
Gattinoni L, Coppola S, Cressoni M, et al. Covid-19 Does Not Lead to a “Typical” Acute
Respiratory Distress Syndrome. AJRCCM Articles in Press. Published March 30, 2020 as
10.1164/rccm.202003-0817LE.
Kampf G, Todt D, Pfaender S, Steinmann E. Persistence of coronaviruses on inanimate
surfaces and its inactivation with biocidal agents. J Hospit Infect. 2020:246-251.
Luks AM, Freer L, Grissom CK, et al. High Alt Med Biol. 2020 Apr 13. doi:
10.1089/ham.2020.0055. [Epub ahead of print].
Papazian L, Aubron C, Brochard L, et al. Formal guidelines: management of acute respiratory
distress syndrome. Ann. Intensive Care 9, 69 (2019). https://doi.org/10.1186/s13613-019-
0540-9.
Ramsey, L. 2020. Business Insider. March 6. https://www.businessinsider.com/presentation-
us-hospitals-preparing-for-millions-of-hospitalizations-2020-3.
Rawat J, Sindhwani G, Biswas D, et al. Role of BiPAP applied through endotracheal tube in
unconscious patients suffering from acute exacerbation of COPD: a pilot study. International
Journal of COPD 2012:7 321–325.
Rubinson L, Vaughn F, Nelson S, et al. Mechanical ventilators in US acute care hospitals.
Disaster Med Public Health Prep. 2010 Oct;4(3):199-206. doi: 10.1001/dmp.2010.18.
Siegel MD, Hyzy RC. UpToDate. November 26, 2019. www.uptodate.com/contents/ventilator-
management-strategies-for-adults-with-acute-respiratory-distress-syndrome. Accessed March
22, 2020.
Tran K, .Cimon K, Svern M, Pessoa-Silva CL, et al. (2012) Aerosol Generating Procedures
and Risk of Transmission of Acute Respiratory Infections to Healthcare Workers: A
Systematic Review. PLoS ONE 7(4): e35797. doi:10.1371/journal.pone.0035797.
U.S. Food & Drug Administration. Enforcement policy for ventilators and accessories and
other respiratory devices during the coronavirus disease 2019 (COVID-19) public health
emergency: guidance for industry and Food and Drug Administration Staff. March 2020.
www.fda.gov/regulatory-information/search-fda-guidance-documents/enforcement-policy-
ventilators-and-accessories-and-other-respiratory-devices-during-coronavirus. Accessed
March 20, 2020.
World Health Organization. Clinical management of severe acute-respiratory-infection when
novel coronavirus (nCoV) infection is suspected: interim guidance. March 13, 2020.
WHO/2019-nCoV/clinical/2020.4. https:// www.who.int/publications-detail/clinical-
management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is-
suspected. Accessed March 20, 2020.

40© 2020 All rights reserved | Confidential | For Syneos Health® use only
Questions?
Visit www.COVID-BiPAPinfo.com for free educational materials
More information:
AARC
FDA
HHS
NIH
Northwell Health


















