Cardiovascular Anatomy, Physiology and Pharmacology BS913 Lecture 10: Pharmacology cont., …
Upload
ankush-chourasiaCategory
view
22download
2description

Introductory Lecture PharmacologyTerm comes from Greek words
•Pharmakon - drug or medicine & •Logos - the truth about or a rational discussion …………Truth about medicine.
Pharmacology is the study of how drugs exert their effects on living systems.
• More specifically it is the study of the interactions between a living organism and drugs that alter normal biochemical function.
Drug Any substance that can affect biological system. OR
Single active chemical entity present in medicine used for prevention, diagnosis or treatment.
Pharmacokinetics investigates the effects of the biological system on drugs (absorption, distribution, elimination…)
Pharmacodynamics describes the fundamental action of a drug on a physiological, biochemical or molecular level
Toxicology studies the undesirable effects of chemicals on living systems (includes poisons, antidotes and unwanted side effects of drugs)
Pharmacy is the art of preparing, compounding and dispensing chemicals for medicinal use.
Clinical Pharmacology is the branch of pharmacology concerned with the pharmacology of therapeutic agents in the prevention, treatment, and control of disease in humans.
Prophylactic refers to a drug or procedure aimed to prevent disease
Palliative refers to a drug or procedure aimed to relieve symptoms
Therapeutic refers to a drug or procedure aimed to cure disease
Tolerance is the increased resistance to the usual effects of an established dose of a particular drug
Effective dose (ED50) is the concentration at which 50% of the subject show a predefined response
Efficacy refers to the inherent capability of a drug to produce a desired effect
Potency compares the relative effectiveness of drugs to produce a desired effect
e.g. Drug A requires fewer milligrams than Drug B to achieve the same pharmacological response --> Drug A has the higher potency, yet, both drugs have the same efficacy.
Chemical Name Generic Name Trade Name
Page 1 of 14

Adverse Drug Reaction is any noxious unintended and undesired effects of a drug that occur at doses used for prevention, diagnosis or treatment
Type A: Predictable, common and related to Pharmacological action of the drug eg diarrhea due to antibiotics use (About 80%)
Type B: Unpredictable, uncommon, usually not related to the pharmacological actions of the drug eg. Intolerance. Anaphylaxis or Idiosyncratic reaction (Independent of dose and generally unrelated to pharmacological action of drug)
Type C: Associated with long-term therapy BZD dependence or nephropathy due to analgesic use
Type D: Carcinogenic/teratogenic effects. Delayed in onset, rare (because drug studies are conducted to ensure)
Drug dependence means that a person needs a drug to function normally. Abruptly stopping the drug leads to withdrawal symptoms. Drug addiction is the compulsive use of a substance, despite its negative or dangerous effects.
Drug abuse is the use of illegal drugs, or the misuse of prescription or over-the-counter drugs for at least a year with negative consequences.
OTC & Controlled Substance
Placebo
What do you need to remember: Classification, MOA, Important pharmacokinetic parameters, therapeutics uses, Life threatening/unique ADRs
Page 2 of 14

What do you need to remember: Classification, MOA, Important pharmacokinetic parameters, therapeutics uses, Life threatening/unique ADRs
PharmacokineticsAbsorption: is the rate at which and the extent to which a drug moves from its site of administration
Transport from GIT (also movement into the cells during distribution)
Passive Diffusion: Higher to lower conc. No carrier. Energy-independent. Non-saturable
Facilitated Diffusion: Higher to lower conc. Carrier required. Energy-independent. Non-saturable
Active Transport: Against Gradient. Carrier required. Energy-dependent. Saturable.
Endo Exocytosis. For large drug molecules. Invagination of cell membrane. Eg. Vit B12.
Rate and efficiency of absorption depends upon
a. Route of administration (iv)b. Blood flow (high vascularization eg small intestine)c. Surface area availabled. Solubilitye. Drug-drug interactions (when given in combination)f. Chemical instability (insulin in GIT)g. Nature of drug formulationh. pH
Effect of pH and pKa
Drugs are either weak acids or bases (HA ↔H+ + A-) OR (BH+↔ B + H+)
Only uncharged drug will pass through the membrane, which depends upon the pH and pKa.
Bioavailability is the fraction of administered drug that gains access to its site of action or a biologic fluid that allows access to its site
Factors affecting bioavailablity: 1st pass metabolism & all the factors that affect absorption
1 st pass metabolism is the biotransformation that occurs before the drug reaches its site of action. It most commonly occurs in liver. Eg nitroglycerine and morphine
Routes of Drug AdministrationDetermined by the properties of drug, therapeutic objective (onset, duration, restriction to local sites)
Enteral & parenteral
Page 3 of 14

Enteral
By mouthAdvantages: Easily administered (convenient and economical), less chance of infection and toxicity (overcome), large area for absorption (stomach, duodenum)
Disadvantages: GIT environmental stress, 1st pass effect (Nitroglycerin 90%)~ adjust dose, food/drugs administration alongwith may influence (Penicillin, prolonged emptying due to food ~ destruction
Buccal/SublingualSublingual →Under tongue ~ diffusion to capillary bed
Buccal → Between gums and cheeks
Advantages: rapid absorption, convenience of administration, low incidence of infection, avoidance of the harsh GI environment, and avoidance of first-pass metabolism.
Disadv: Not all drugs good candidates. Taste. Dose
Parenteral:Directly into systemic circulation/vascular tissue.
Advantages: Good for drugs with poor abs. orally/ or unstable. Rapid onset. Unconscious. Bypass GI
Disadvantages: Irreversible, pain, fear, infection, inconvenience.
I.V. Fast onset, no 1st pass. No control, systemic infection, ADR’s like phlebitis, hemolysis, local irritation
I.M.Aqueous solution/depot in non aq. Like PEG. Different rates of absorption.
S.C.Lesser rate of abs. and less risk compared to iv.
Others
Inhalational:Rapid absorption across mucous membranes of the respiratory tract and pulmonary epithelium (mimics iv). For gases/nebulized products for local effect.
Itranasal:Nasal decongestants like ephedrine
Itrathecal/IntraventricularDirectly into CSF (Amph B for cryptococcal meningitis)
Page 4 of 14

TopicalLocal effect. Clotrimazole for dermatophytosis
TransdermalPatches (nitroglycerin, scopolamine)
RectalWhen oral not desirable (children, vomiting, unconscious), less chances of biotransformation
Erratic and incompletes absorption, irritation
Bioequivalent drugs have the same bioavailablity.
Therapeutic equivalents drugs have the same effect in treatment of a disease or condition.
Drug DistributionProcess by which a drug reversibly leaves the bloodstream and enters the interstitium (extracellular fluid) and/or the cells of the tissues. Depends upon blood flow, capillary permeability, the degree of binding of the drug to plasma and tissue proteins, and the relative hydrophobicity of the drug.
A. Blood Flow: Differential depending upon COP. Eg Blood flow to the brain, liver, and kidney is greater than that to the skeletal muscles; adipose tissue has a still lower rate of blood flow. Thiopental
B. Capillary permeability: Structure, BBB (endothelial cells of the capillaries of the CNS, prostate --- liver, spleen→wide spaces)/Placental (small MW, Chemical Nature of drug.
C. PPB: Reversible binding to plasma proteins sequesters drugs in a nondiffusible form and slows their transfer out of the vascular compartment. Plasma albumin is the major drug-binding protein and may
Page 5 of 14
act as a drug reservoir; that is, as the concentration of the free drug decreases due to elimination by metabolism or excretion, the bound drug dissociates from the protein. This maintains the free-drug concentration as a constant fraction of the total drug in the plasma. Different drugs have different affinity with albumin, and therefore different capacity of albumin to offer. Albumin has the strongest affinities for anionic drugs (weak acids) and hydrophobic drugs. Most hydrophilic drugs and neutral drugs do not bind to albumin. Competition for binding between drugs: divided into two Class I (Low dose/capacity ratio: Warfarin) and Class II (High dose/capacity ratio: Sulfonamide antibiotic) ~ Free very small percentage→displaced → 100% free
D. Drug Structure: Small non-polar more easy distribution that large polar ones
Volume of Distribution. (Vd): The volume of distribution is a proportionality factor that relates the amount of drug in the body to the concentration of drug measured in a biological fluid. The larger the volume of distribution, the more likely that the drug is found in the tissues of the body. The smaller the volume of distribution, the more likely that the drug is confined to the circulatory system.
Redistribution: Lipid-soluble drugs can get redistributed before elimination. So drugs acting on CNS, the duration of action of an initial dose may depend more on redist rather than on half life. So second dose has a longer duration of action because redist is less.
Drug MetabolismLipophilic→polar. Liver major site but kidney and intestine too for some drugs. Pro→active.
Types of Rxns:Phase I: Modification of the drug molecule via oxidation, reduction or hydrolysis.
Microsomal metabolism.
(Microsome: A small particle in the cytoplasm of a cell, typically consisting of fragmented endoplasmic reticulum to which ribosomes are attached.)
Page 6 of 14

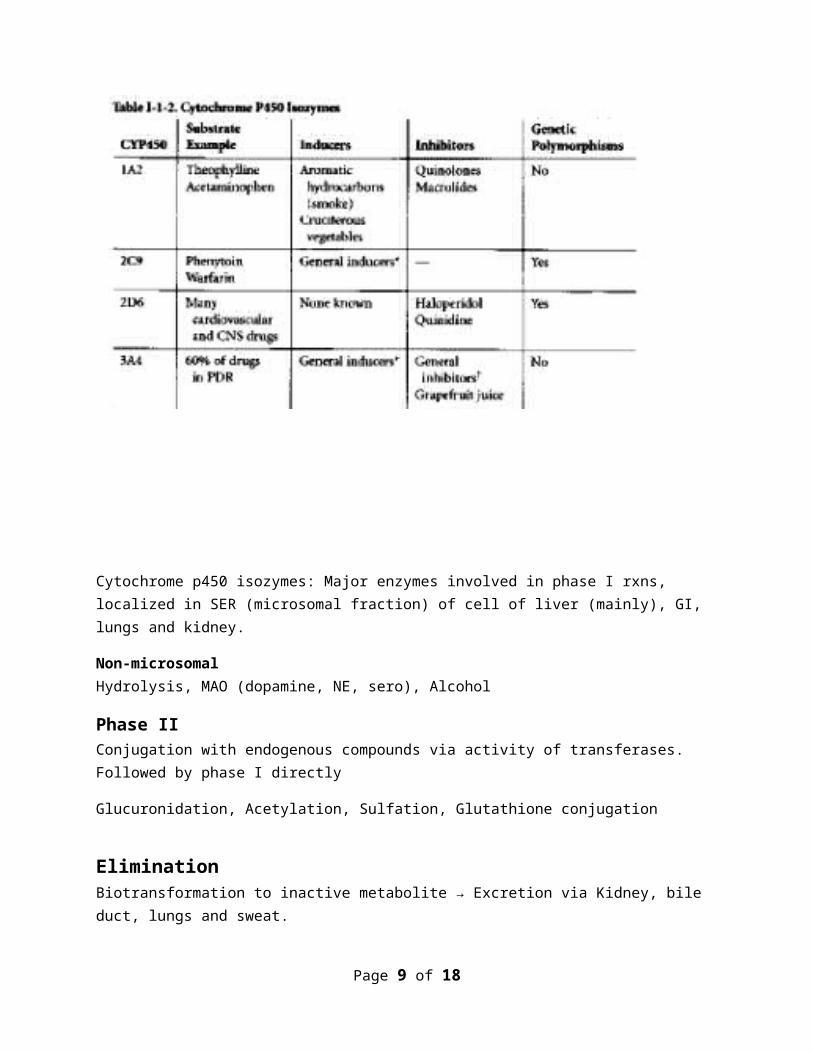
Cytochrome p450 isozymes: Major enzymes involved in phase I rxns, localized in SER (microsomal fraction) of cell of liver (mainly), GI, lungs and kidney.
Non-microsomalHydrolysis, MAO (dopamine, NE, sero), Alcohol
Phase IIConjugation with endogenous compounds via activity of transferases. Followed by phase I directly
Glucuronidation, Acetylation, Sulfation, Glutathione conjugation
EliminationBiotransformation to inactive metabolite → Excretion via Kidney, bile duct, lungs and sweat.
Renal elimination of drug1. Glomerular filtration : free drug is filtered ~ lipid solubility/pH has no effect2. PCT Secretion : Drugs not filtered leave thru efferent may get actively secreted thru acid/base
sec mech. Competition and neonates.
Page 7 of 14

3. Distal tubular reabsorption : High luminal conc ~ uncharged drug may diffuse back into systemic circulation. Increase pH for acids (ion trapping) Phenobarbital/bicarbonate. Amphetamine/NH4Cl. Better metabolism
Clearance by other routesIntestines, the bile, the lungs, and milk in nursing mothers.
1. Fecal : Unabsorbed drugs orally ingested drugs through feces or drugs secreted into intestine directly or in bile.
2. Lungs : Inhalational anesthetic agents (halothane/iso) 3. Milk : Important for infants4. Misc : Excretion of most drugs into sweat, saliva, tears, hair, and skin occurs only to a small
extent.
Kinetics of Elimination
Zero-order Elimination rateA constant amount of drug is eliminated per unit time. Rate is independent of plasma conc. Drugs following zero order have no fixed t1/2. E.g. ethanol, phenytoin, salicylate
1st – order Constant fraction of drug is eliminated per unit time. Rate dependent on plasma conc. Fixed t1/2.
Renal EliminationRate of elimination= GFR+ active secretion – reabsorption (active/passive)
Clearance = volume of blood cleared of drug per unit of time. Cl=GFR (no reabsorption/secretion)
Steady state: rate in = rate out
Plateau principle
Time needed to reach steady state is dependent upon t1/2 and independent of dose size or frequency
Page 8 of 14
Pharmacodynamics:
Pharmacodynamics is related with the binding of the drugs to the receptors and their effects.
Describes the actions of a drug on the body and includes the principles of receptor interations, mechanisms of therapeutic and toxic action, and dose-response relationship
Receptor: A chemical group or molecule (as a protein) on the cell surface or in the cell interior that has an affinity for a specific chemical group, molecule, or virus OR
Receptors are protein molecules, embedded in either the plasma membrane (cell surface receptors) or the cytoplasm or nucleus (nuclear receptors) of a cell, to which one or more specific kinds of signaling molecules may attach.
A molecule which binds (attaches) to a receptor is called a ligand, and may be a peptide (short protein) or other small molecule, such as a neurotransmitter, a hormone, a pharmaceutical drug, or a toxin.
Agonist: Binding to a receptor results in response. Salbutamol β2 agonist
Antagonist: Binding to a receptor = no response. Drug can block the agonist from binding to its receptor. Propranolol β antagonist.
Affinity: Ability of a drug to bind to a receptor.
Potency: Measure of activity of the drug expressed in terms of amount required to produce an effect of given magnitude. Morphine is small doses, aspirin in large doses. OR
Shows relative doses of two or more agonists to produce the same magnitude of effect.
Efficacy: Degree of effectiveness of a drug. OR
relationship between receptor occupancy and the ability to initiate a response at the molecular, cellular, tissue or system level.
Dose-response curve: A dose-response curve describes the relationship between responseto drug treatment and drug dose or concentration. Sensitivity to a drug acting at a specific, saturable receptor typically spans a large concentration range, so dose-response curves are usually semi-logarithmic, i.e., the amountof drug is plotted as the log of drug concentration, giving them their familiar sigmoidal shape.
Page 9 of 14

a. Same mechanism, parallel slopes. b. Only drugs of same mechanism (interaction with same receptor) can be compared (1st figure) in
terms of affinity with the receptor.c. Potency can be compared in both
Full Agonists: Compounds that are able to elicit a maximal response following receptor occupation and activation.
Partial Agonists: Compounds that can activate receptors but are unable to elicit the maximal response of the receptor system. A partial agonist produces an effect if no full agonist is present, but acts as an antagonist in the presence of a full agonist. Concentration-effect curves of partial agonists resemble curves of full agonists in the presence of a noncompetitive antagonist.
Inverse agonist: an agent which binds to the same receptor binding-site as an agonist for that receptor and reverses constitutive activity of receptors. Inverse agonists exert the opposite pharmacological effect of a receptor agonist.
Page 10 of 14

Drug B is full agonist. A & C are partial agonists. Potency. Partial agonist can act as antagonist in the presence of a full agonist.
Antagonism & Potentiation
Potentiation: Parallel shift to right. Appearance of ↑ in potency.
Antagonism:
The joint effect of two or more drugs such that the combined effect is less than the sum of the effects produced by each agent separately
Page 11 of 14

Types: - a. Pharmacological Antagonism : -
i. Competitive (Reversible) ii. Non-competitive (Irreversible)
b. Chemical Antagonism.c. Physiological Antagonism .
Functional/Physiological antagonism. caused by agonist and antagonist acting at two independent sites and inducing independent OR
Histamine H1 bronchial constriction Epinephrine β 2 agonist relaxes smooth muscles of bronchi.
Chemical Antagonism: caused by combination of agonist with antagonist, with resulting inactivation of the agonist (dimercaprol and mercuric ion) OR
modifying or sequestering the agonist so that it is incapable of binding to and activating its receptor. Protamine sulfate (Negative/basic) binds to heparin (Positive/acidic)
Pharmacological:
Competitive: cause parallel shift to right in D-R curve for agonists. Can be reversed by ↑ing the dose of agonist. Appearance of ↓ in potency.
Non-competitive: Causes non- parallel shift to right. Can be rescued to some extent with the increase in the dose of the agonist (mostly irreversible). Appearance of ↓ in the efficacy of agonist.
ED50: The dose effective in 50% of population. Achieved thru plotting a cumulative (quantal) D-R curve.
Therapeutic Index: The therapeutic index of a drug is the ratio of the dose that produces toxicity to the dose that produces a clinically desired or effective response in a population of individuals.
Where
Page 12 of 14

Others
Signal Transduction:Drug = Signal Receptor = Signal Detector
Drug+Receptor→Complex→Response/Effect
Many types of drug responsive mechanism are known
I/C receptors:Cortisol ~ anti-inflammatory proteins
Eg. Thyroid, gonadal steroids, vit D ~ (Slow onset/Long Duration)
E/C receptors coupled to Ion-channelsEg. Nicotinic receptor in ANS, NMJ, CNS is coupled to Na/K ion channel. Drugs target this receptors include nicotine, ganglion blockers(hexamethonium), skeletal muscle relaxants (tubocurarine).
GABAA coupled to chloride channel. Target for barbiturates, BZD and anticonvulsants
Membrane receptors Types
Page 13 of 14

Receptors linked via coupling proteins to I/C effectors
Page 14 of 14