Infarcted fibroadenoma of the breast: report of two new cases with
Upload
jonathan-caseyCategory
view
221download
1
Introduction to the Management of Breast Cancer
Statistics
• 192,370 new cases and 40,170 deaths estimated for 2009 in the US – 62,280 cases in situ breast cancer
• Lifetime risk of developing breast cancer is 12-13%, or ~1 in 8 women– Highest incidence
• Lifetime risk of dying is approximately 3.0% (1 in 33 women)– Second cancer mortality (after lung ca)
CA Cancer J Clin 2009; 59:225-249
Copyright ©2009 American Cancer Society
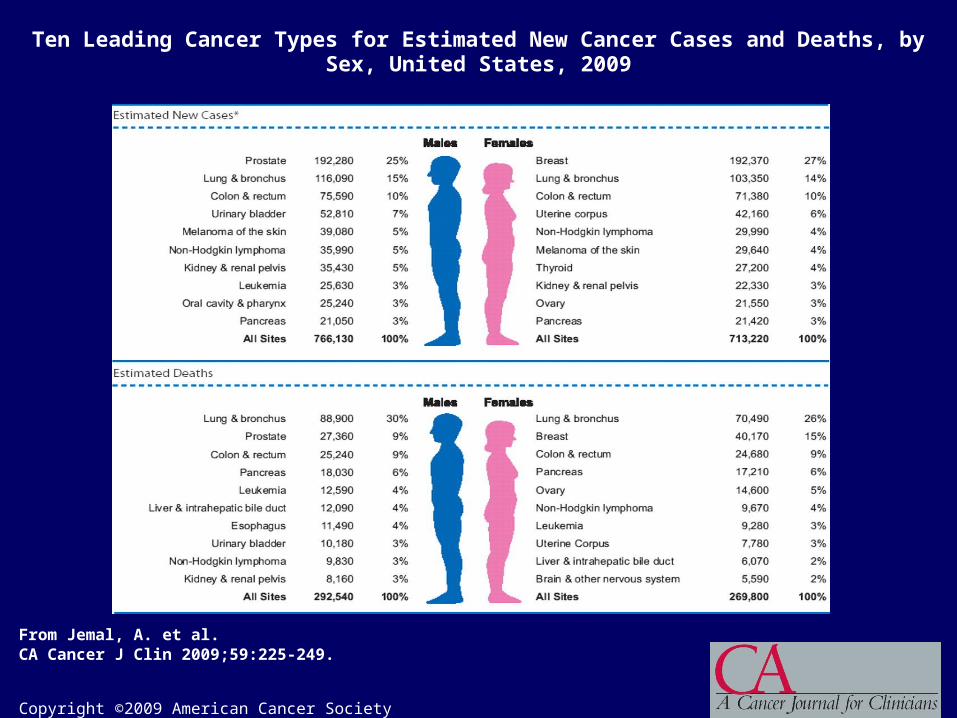
From Jemal, A. et al. CA Cancer J Clin 2009;59:225-249.
Ten Leading Cancer Types for Estimated New Cancer Cases and Deaths, by Sex, United States, 2009
Copyright ©2009 American Cancer Society
From Jemal, A. et al. CA Cancer J Clin 2009;59:225-249.
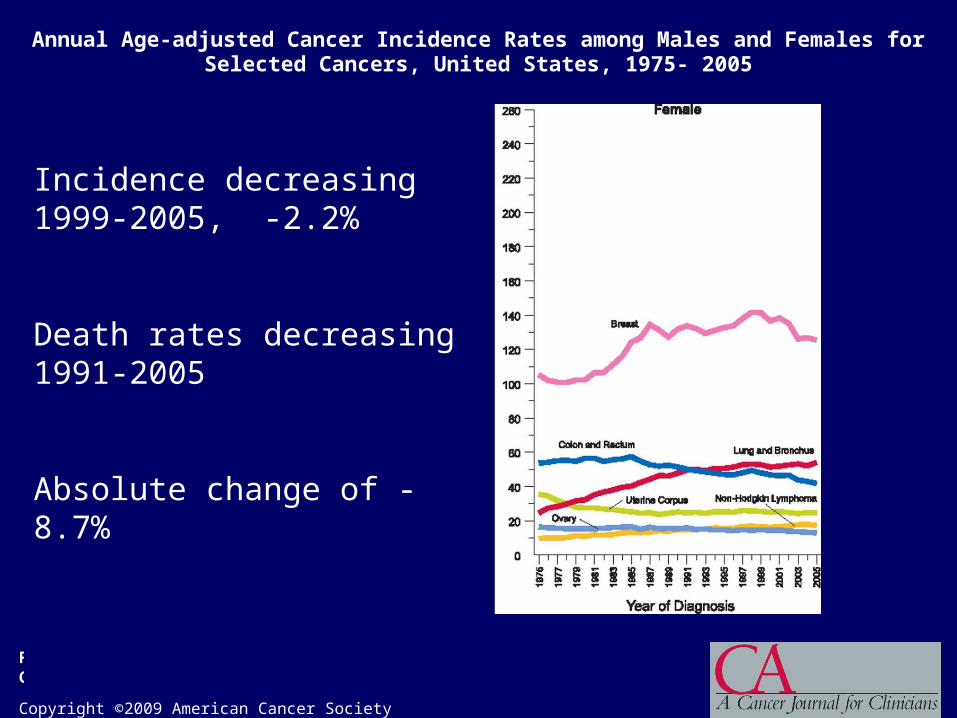
Annual Age-adjusted Cancer Incidence Rates among Males and Females for Selected Cancers, United States, 1975- 2005
Incidence decreasing 1999-2005, -2.2%
Death rates decreasing 1991-2005
Absolute change of -8.7%
Incidence and Mortality
• Incidence – Increased screening (mammography)– Environmental factors? – 2003 7% decline in incidence (> in ER+)
• Decrease in use of hormone replacement therapy
• Mortality decreasing– 2.3 percent per year from 1990 to 2002– Early detection– Better adjuvant therapy
Ravdin, SABCS 2006Berry et al NEJM 2005 353:1784
Breast Cancer Risk Factors• Age• Prior breast biopsies with proliferative breast disease
• Atypical hyperplasia• Lobular carcinoma in-situ
• Family History• Thoracic radiation• Endogenous hormones
– Early menarche– Late menopause– Nulliparity or older age at birth of first child
• Exogenous hormones• Mammographic density• Lifestyle Factors (alcohol, obesity, diet, exercise)

Most Breast Cancer is NOT Hereditary
SporadicSporadic
Family Family clustersclusters
HereditaryHereditary
Ovarian CancerOvarian CancerBreast CancerBreast Cancer
5%–10%5%–10% ~10%~10%
15%-15%-20% 20%
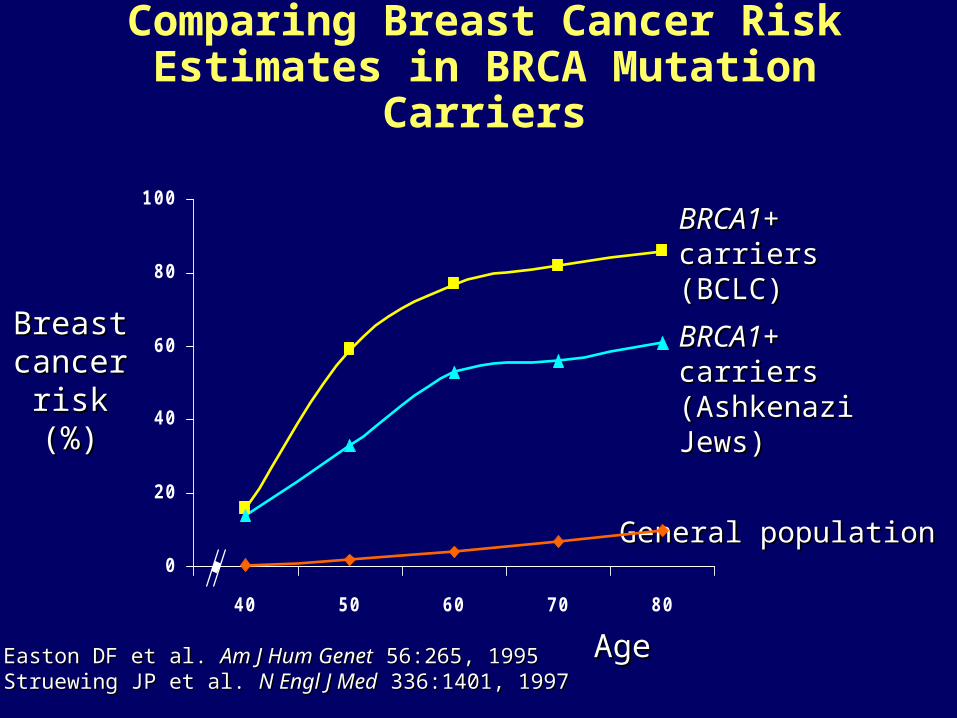
Comparing Breast Cancer Risk Estimates in BRCA Mutation Carriers
Breast Breast cancer cancer
risk (%)risk (%)
General populationGeneral population
BRCA1BRCA1+ carriers+ carriers(BCLC)(BCLC)
BRCA1BRCA1+ carriers+ carriers(Ashkenazi Jews)(Ashkenazi Jews)
AgeAgeEaston DF et al. Easton DF et al. Am J Hum GenetAm J Hum Genet 56:265, 1995 56:265, 1995Struewing JP et al. Struewing JP et al. N Engl J MedN Engl J Med 336:1401, 1997 336:1401, 1997
0
20
40
60
80
100
40 50 60 70 80
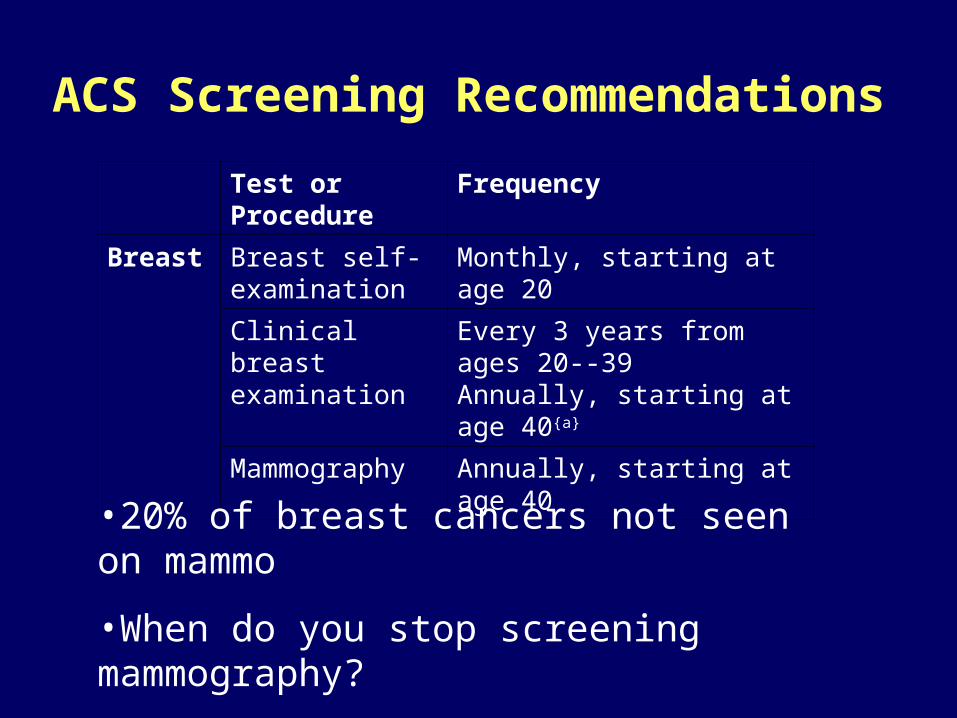
ACS Screening Recommendations
Test or Procedure
Frequency
Breast Breast self-examination
Monthly, starting at age 20
Clinical breast examination
Every 3 years from ages 20--39Annually, starting at age 40{a}
Mammography Annually, starting at age 40
•20% of breast cancers not seen on mammo
•When do you stop screening mammography?

ACS guidelines for Breast MRI
CA Cancer J Clin 2007; 57; 75-89

Diagnosis of Breast Cancer
• Fine needle aspiration – Cytologic diagnosis, cannot distinguish DCIS from invasive
disease– Negative aspiration does not rule out cancer
• Core-needle biopsy – Preferred method for diagnosis; preserves architecture
• Excisional biopsy – Useful to determine tumor size– Precludes primary chemotherapy
• Needle localization– Nonpalpable lesions, multiple lesions
• Stereotactic biopsy– Image-guided FNA or core biopsy

Breast Cancer Pathology
• Invasive carcinoma
– Infiltrating ductal (75% of breast cancers)
– Infiltrating lobular (5-10% of breast cancers)
• “Indian file” histology, less distinct mass
• More often metastasizes to: pleura, peritoneum, meninges
– Medullary (5-7%)
• Lymphocytic and plasma cell infiltrate, well circumscribed
– Good prognosis
• Mucinous/Colloid (3%,)
• Papillary (1-2%)• Tubular (5 %)
Breast Cancer Pathology
• Non-invasive tumors
– Ductal carcinoma in situ (DCIS)
• Comedo (poorly differentiated)
• Noncomedo (well differentiated, low-grade)
– Papillary, micropapillary, cribiform, solid
– Lobular carcinoma in situ (LCIS)
• Uncommon tumors
– Inflammatory carcinoma
– Paget’s disease
– Phyllodes tumor (cystosarcoma phyllodes)
Breast Cancer Classification
• Staging (TNM)
• Histologic evaluation– Tumor grade– Hormone receptors– HER2 expression– Molecular subtypes

Prognostic Factors
• Patient age (menopausal status)• Tumor size• # of Lymph nodes• Histologic tumor type • Tumor grade (% tubule formation, nuclear
pleomorphism, mitotic count)• Hormone receptor status• Her2/neu status• Oncotype DX score/ Recurrence score

Copyright © American Society of Clinical Oncology
Chia, S. K. et al. J Clin Oncol; 22:1630-1637 2004
Fig 1. (A) Relapse free survival (RFS) based on size for entire cohort 1 (0.1 to 1.0 cm, top); entire cohort 2 (1.1 to 2.0 cm, middle); and entire cohort 3 (2.1 to 5.0
cm, bottom)
82%
75%
66%
Natural History

Histology
DuctalLobularMucinousMedullaryTubularPapillary
Survival (%)
58.7 67 65.3 55.2 81.5 62.8
HR 995% CI)
1.00 (reference)0.89 (0.86-0.91)0.80 (0.76-0.85)0.82 (0.78-0.87)0.66 (0.60-0.73)0.81 (0.73-0.90)
Li, et al Arch Int Med 163:2149-53, 2003
Risks of Mortality by Tumor Type in Women aged 50-79 yrsSEER 1974-1998 (164,958 pts)
Tumor Grading• Tumor grade is a system used to classify
cancer cells in terms of how abnormal they look under a microscope and how quickly the tumor is likely to grow and spread

Hormone receptor status
• Estrogen and progesterone receptors are nuclear transcription factors
• Determined by immunohistochemistry
• Scored as a percentage of cells staining
• 1% or greater is considered positive
Her2/neu status
• Membrane-associated tyrosine kinase receptor (aka erbB2)– Expressed in breast cancers, DCIS, and some
other tissues such as heart
• Worse prognosis with HER2 gene amplification– Prognosis changing with use of trastuzumab
Her2/neu status
• Measured by immunohistochemistry (IHC) and/or FISH
• FISH more accurate• IHC: Graded 0, 1+, 2+, or 3+
– Based on characteristics of staining– 0-1 = negative– 2 = in determinant, should be followed with
FISH (fluorescent in situ hybridization) to determine status (amplified/not amplified)
– 3 = positive

Press, M et al. J Clin Oncol 15:2894-904, 1997
Prognosis: Tumors 1 cm, HER2 gene amplification, Node-negative

The HER Family of Receptors
HER1EGFR
HER2 HER3
HER4
Tumor CellTumor Cell
•Trastuzumab (Herceptin)Trastuzumab (Herceptin)•Pertuzumab (Omnitarg)Pertuzumab (Omnitarg)
•LapatinibLapatinib

Her2 therapy
• Trastuzumab (Herceptin) – Monoclonal antibody directed towards
Her2/neu receptor– cardotoxicty
• Lapatinib (Tykerb)– Small molecule tyrosine kinase inhibitor
blocking HER2 and EGFR1 (HER1)– Diarrhea, rash– Cardiotoxicity?
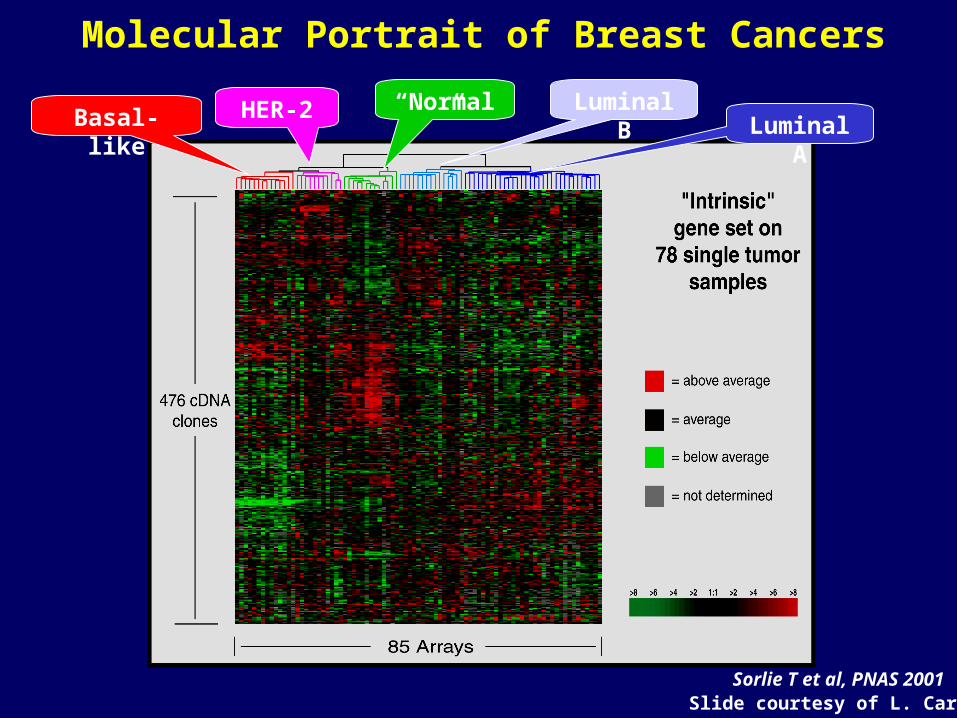
Molecular Portrait of Breast Cancers
HER-2Basal-like Luminal ALuminal B“Normal”
Sorlie T et al, PNAS 2001Slide courtesy of L. Carey

Proxies for Gene Signature “Subtypes”
Triple Negative
ER/PR+HER2+ ER/PR-
Basal-like 75% 9% 0%
Luminal 12% 76% 14%
“HER2” 9% 5% 85%Courtesy of L Carey
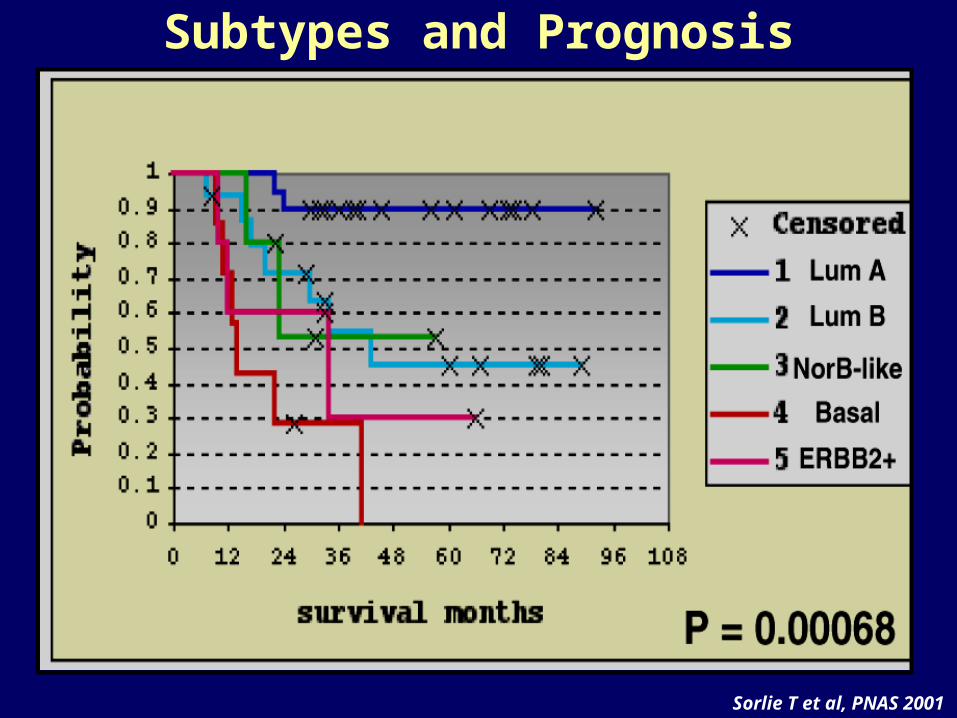
Subtypes and Prognosis
Sorlie T et al, PNAS 2001

2003 AJCC: Primary Tumor (T)
• T1: 2 cm– T1mic
microinvasion 0.1 cm
– T1a >0.1 - 0.5 cm– T1b 0.6 – 1 cm– T1c 1.1 – 2 cm
• T2: 2.1- 5 cm• T3: > 5 cm
• T4a: Extension to chest wall, not including pectoralis
• T4b: Edema, ulceration, satellite skin nodules
• T4c: both T4a and T4b• T4d: inflammatory ca

AJCC 2003: Stage GroupingStage 0 Tis N0 M0
Stage I T1 N0 M0
Stage IIA T0 N1 M0
T1 N1 M0
T2 N0 M0
Stage IIB T2 N1 M0
T3 N0 M0
Stage IIIA T0-3 N2 M0
T3 N1 M0
Stage IIIB T4 N0-2 M0
Stage IIIC Any T N3 M0
Stage IV Any T Any N M1

Staging Classification of Breast Tumour

Therapy of Breast Cancer
• Local: – Surgery
• Mastectomy • Breast Conserving Therapy• SLND/ALND
– Radiation therapy• Systemic:
– Endocrine/hormonal therapy – Chemotherapy– Biologic therapy

Breast Cancer Local Treatment
• Modified radical mastectomy with axillary lymph node dissection
• Breast-conserving therapy – lumpectomy with axillary lymph node dissection followed by radiation
• Equivalence established by NSABP B-06• Original report (Fisher, et al., NEJM 1985)• 12 year follow up (Fisher, et al., NEJM 1995)• NCI audit (Christian, et al., NEJM 1995)
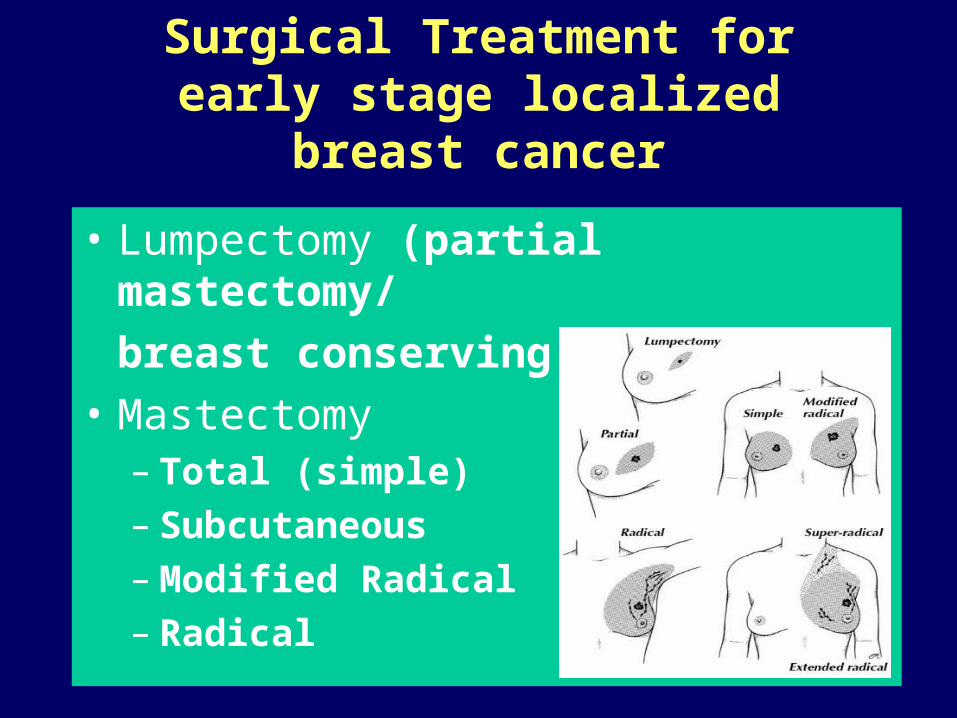
Surgical Treatment for early stage localized breast cancer
• Lumpectomy (partial mastectomy/
breast conserving therapy)
• Mastectomy– Total (simple) – Subcutaneous– Modified Radical – Radical
Contraindications to BCT
• Pregnancy
• Previous breast or mantle RT
• Diffuse malignant microcalcifications
• Collagen vascular disease (SLE, scleroderma)
• Multicentric disease
Indications for Post-Mastectomy Radiation
• 4 or more positive axillary lymph nodes• Tumor 5 cm or greater• Tumor invading the skin or adjacent
musculature• Positive surgical margins
• Note: Role in patients with 1 – 3 positive nodes is controversial (balanced discussion)
• ASCO guidelines for postmastectomy XRT• Recht, et al., JCO 19:1539, 2001.
• Can eliminate hidden, microscopic metastases
•Decreases local recurrence in patients treated with breast conservation •Includes:
• Hormone therapy• Chemotherapy• Target therapy (ie Herceptin)
Adjuvant systemic therapy
Who should receive adjuvant therapy?
• Consensus statements:– Early Breast Cancer Trialists’ Collaborative
Group (EBCTCG, aka Oxford Overview) last published 2005
– 7th International Conference on Adjuvant Therapy of Primary Breast Cancer (St. Gallen, 2009)
– NCI Consensus Conference (Nov 2000)– NCCN guidelines
Indications for Adjuvant Chemotherapy
• All lymph node-positive • Her2/neu positive tumors• Triple negative tumors• Invasive, lymph node-negative
- invasive ductal/lobular, > 1 cm (NIH)
- invasive ductal/lobular, > 2 cm (St. Gallen’s)
- invasive, favorable histology, > 3 cm

Case#1
• 68 y.o. postmenopausal female noted to have abnormality in left breast on screening mammogram– approx 1 cm abnormality noted in upper
outer quadrant
• No sig PMH or FH
• Negative ROS

• Left core biopsy-infiltrating ductal carcinoma, grade 1, ER 90%, PR 95%, Her2/neu negative
• Left lumpectomy and SLNB-1.1cm IDC, 0/2LN+
• What adjuvant therapy should she receive?

• Hormonal treatment first choice
• Could consider chemotherapy– Oncotype DX
Indications for Adjuvant Hormonal Therapy
• Indicated for almost all patients with ER or PR expression > 1%
• Sequential preferred over concurrent chemo-hormonal therapy
• Tamoxifen and/or AI – No AI in premenopausal women
Albain, K. St Gallen Conf 2003

Hormonal (Endocrine) Therapies:Mechanisms of Action
• Decrease ligand• Aromatase inhibitors• Oophorectomy• Goserelin, Leuprolide
• Block receptor• SERM (selective
estrogen receptor modulators)
• SERD (selective estrogen receptor downregulator)

Diff hormonal agents
• Tamoxifen– Blood clots, uterine cancer, increased LFTs,
cataracts, hot flashes– Improves BMD in postmenopausal, improves
lipid profile• Aromatase Inhibitors (anastrozole, letrozole,
exemestane)– Myalgias/arthralgias, decrease in BMD– Elevate BP, elevate lipids, CV risk?

Adjuvant TherapyGuiding Principles: Hormones
EBCTCG Lancet. 365(9472):1687-717 2005
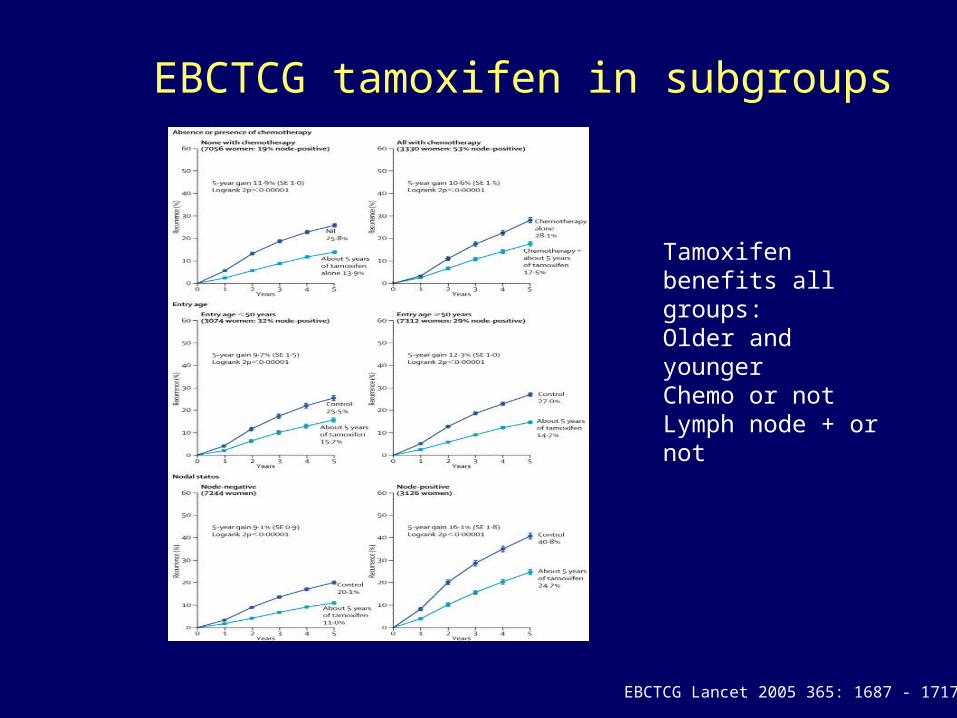
EBCTCG tamoxifen in subgroups
Tamoxifen benefits all groups:Older and youngerChemo or notLymph node + or not
EBCTCG Lancet 2005 365: 1687 - 1717

Trials of AIs in the adjuvant setting
ATAC
BIG I-98
IES
ABCSG 8ARNO 95
MA-17
TAMOXIFEN x 5
ANASTROZOLE x 5
TAM + ANAST x 5
TAMOXIFEN x 5
LETROZOLE x 5
TAM x 2
LET x 2
LET x 3
TAM x 3
TAM x 2-3
EXEMESTANE x 2-3TAM x 2-3
TAM x 2-3
Anastozole x 2-3TAM x 2-3
TAMOXIFEN x 5LETROZOLE x 5
PLACEBO x 5
ITA

0.4 0.6 0.8 1.0 1.2
BIG I-98 0.81 (0.70, 0.93)
ABSCG/ARNO
0.60 (0.44, 0.81)
ATAC 0.83 (0.73, 0.94)
MA.17 0.58 (0.45, 0.76)
IES 0.76 (0.66, 0.88)
Summary of Results from Large Adjuvant Aromatase Inhibitor Trials

Length of Hormonal Tx
• Atleast 5 years
• Up to 10 years
• Maybe more?

Endocrine Rx:What you need to know
• Use in anyone with ER+ and/or PR+– Sequence after chemotherapy
• Tamoxifen reduces the risk of recurrence and improves overall survival across the board
• AIs reduce risk of recurrence compared with tamoxifen. NO increased OS yet. – Try to use AIs in all postmenopausal women
• SERM and AI side effect profiles differ, keep in mind when assessing individual patients
• Ovarian suppression is an option for premenopausal women (added benefit with hormonal tx?)

Case #2
• 48 y.o. perimenopausal female notes a 1.5 cm mass in her right breast on self exam
• Mammogram shows no abnormalities
• Biopsy-IDC, grade 3, ER 30%, PR 10%, Her2/neu negative

• Lumpectomy and SLNB-2cm IDC, grade 3, 1/2 LN+
• What should she receive as adjuvant therapy?

Lymph Node Positive Breast Cancer• ER negative
– chemotherapy
(pre-menopausal or post-menopausal)
• ER positive– premenopausal: chemotherapy + tamoxifen**– postmenopausal: tamoxifen/AI +
chemotherapy
- age > 70: tamoxifen (+ chemotherapy?)
** ovarian ablation/GnRH analog may be considered
Adjuvant!
• Computer program to determine breast cancer prognosis by adjuvant therapy
– http://www.adjuvantonline.com
• Recurrence rates based on Oxford Overview data
• Overall survival based on SEER data
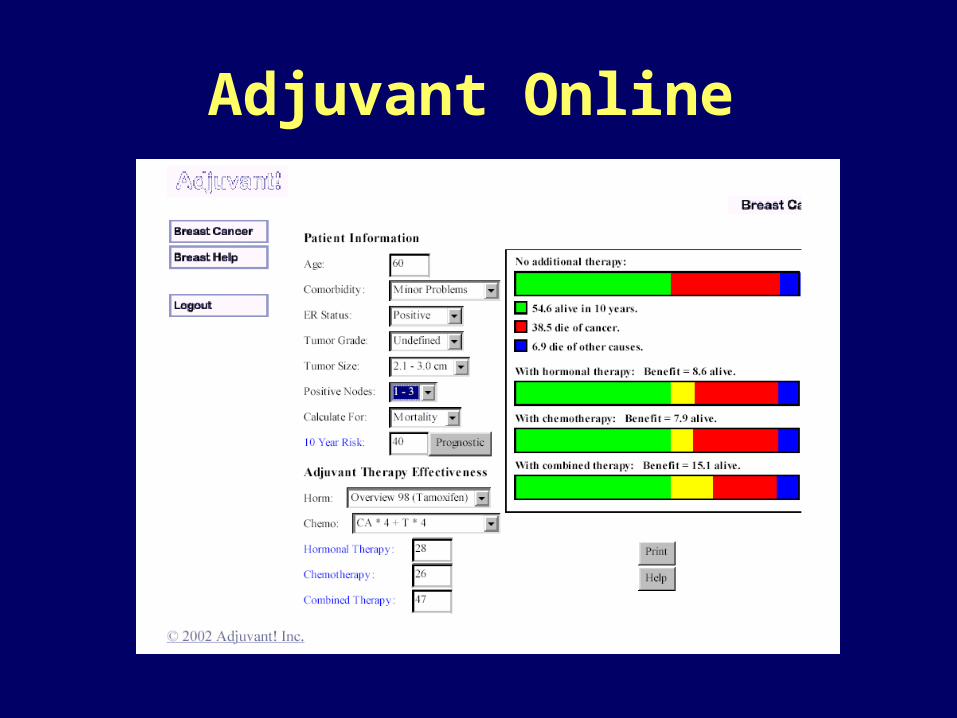
Adjuvant Online
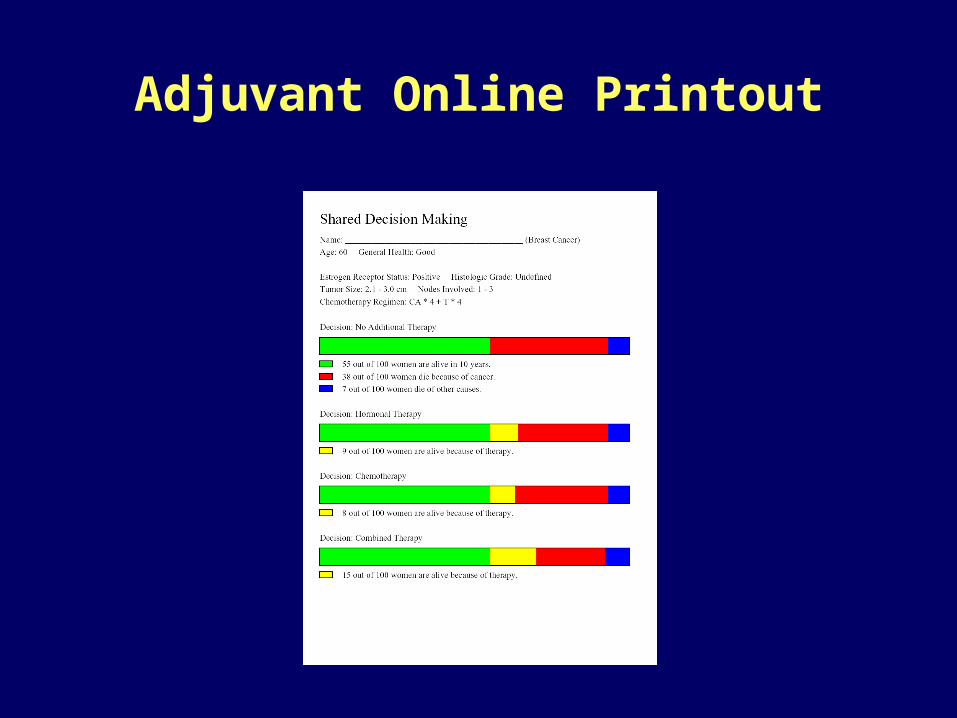
Adjuvant Online Printout
Genomic Health 21 Gene Panel Predicts Benefit from Chemotherapy
- Results from NSABP B-14 and B-20
Soonmyung Paik1, Steven Shak2, Gong Tang1, Chungyeul Kim1, Joffre Baker2, Maureen Cronin2, Rick Baehner2, Drew Watson2, John Bryant1, Joseph Costantino1, William Hiller1, and Norman Wolmark1
From 1. Division of Pathology, Operation Center, and Biostatistics Center, NSABP, Pittsburgh, PA2. Genomic Health, Inc., Redwood City, CA
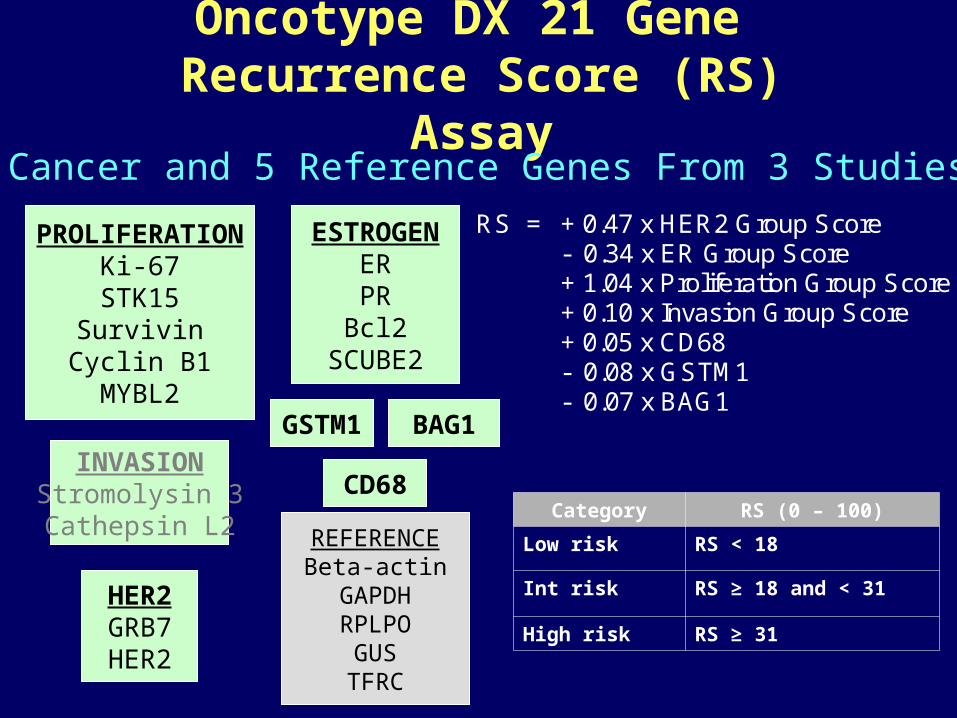
RS = + 0.47 x HER2 Group Score
- 0.34 x ER Group Score + 1.04 x Proliferation Group Score + 0.10 x Invasion Group Score + 0.05 x CD68 - 0.08 x GSTM1 - 0.07 x BAG1
Oncotype DX 21 Gene Recurrence Score (RS) Assay
PROLIFERATIONKi-67
STK15Survivin
Cyclin B1MYBL2
ESTROGENERPR
Bcl2SCUBE2
INVASIONStromolysin 3Cathepsin L2
HER2GRB7HER2
BAG1GSTM1
REFERENCEBeta-actinGAPDHRPLPO
GUSTFRC
CD68
16 Cancer and 5 Reference Genes From 3 Studies
Category RS (0 – 100)
Low risk RS < 18
Int risk RS ≥ 18 and < 31
High risk RS ≥ 31

Tamoxifen treated patients from NSABP B-14 (N=668)
Performance exceeded standard measures of patient age, tumor size
Validation Study of Oncotype DX
0%
5%
10%
15%
20%
25%
30%
35%
40%
0 5 10 15 20 25 30 35 40 45 50
Recurrence Score
Dis
tan
t R
ec
urr
en
ce
at
10
Ye
ars
Low Risk Group High Risk Group Intermediate Risk Group
0 2 4 6 8 10 12 14 16
Years
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
DR
FS
Low Risk (RS <18) Intermediate Risk (RS 18 - 30) High Risk (RS 31)
338 pts149 pts181 pts

OncotypeDX Results
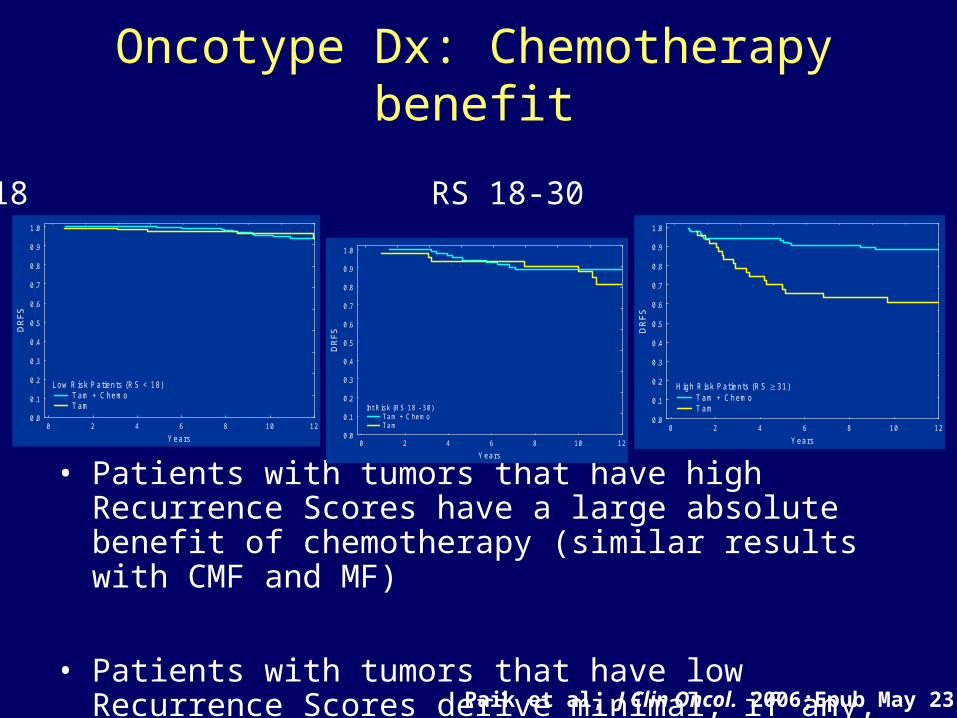
Oncotype Dx: Chemotherapy benefit
• Patients with tumors that have high Recurrence Scores have a large absolute benefit of chemotherapy (similar results with CMF and MF)
• Patients with tumors that have low Recurrence Scores derive minimal, if any, benefit from chemotherapy
RS < 18 RS 18-30 RS ≥ 31
0 2 4 6 8 10 12
Years
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
DR
FS
Low R isk Patients (R S < 18) T am + C hemo T am
0 2 4 6 8 10 12
Years
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
DR
FS
Int Risk (RS 18 - 30) Tam + C hemo Tam 0 2 4 6 8 10 12
Years
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
DR
FS
H igh R isk Patients (R S 31) T am + C hemo T am
Paik et al, J Clin Oncol. 2006;Epub May 23.
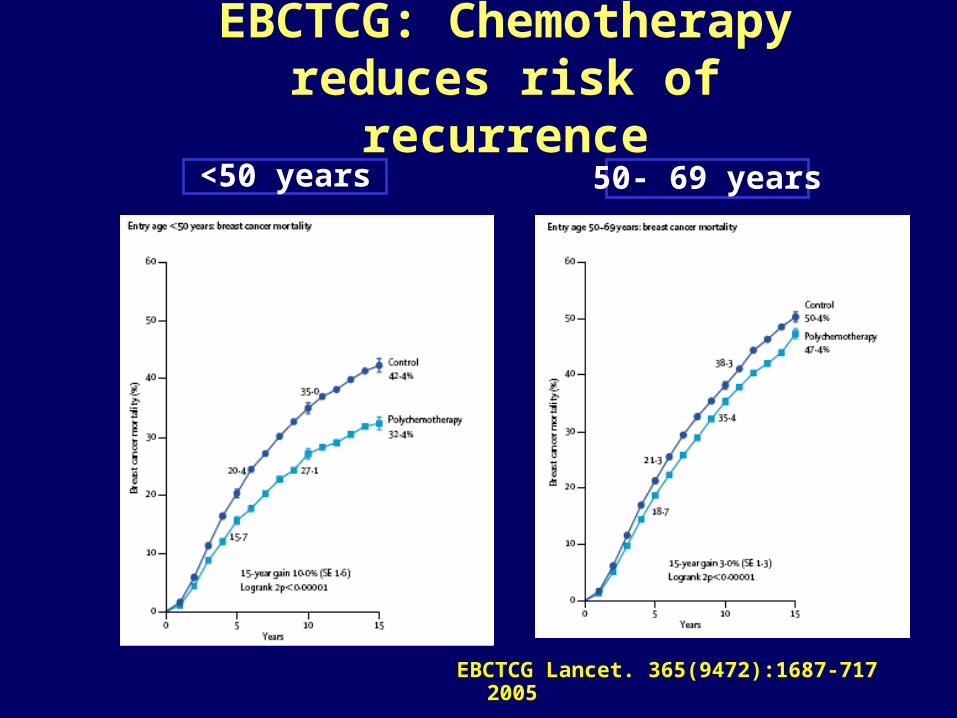
EBCTCG: Chemotherapy reduces risk of recurrence<50 years 50- 69 years
EBCTCG Lancet. 365(9472):1687-717 2005

Progress in Adjuvant Chemotherapy
of Breast Cancer
Before Anthracyclines• CMF, CMFVP
With Anthracyclines• Combination: AC, FAC, FEC, CEF• Sequence and Alternating• Dose intensity, dose density, HDCT
Taxanes (Paclitaxel/Docetaxel)• Sequential: A → T → C or AC → T• Combination: TA, TAC
Biologic Modifiers
1970s
1980s
1990s
2000sVogel CL, ASCO 2003

Adjuvant Chemotherapy Regimens
• Low risk/lymph node negative– ACx4– CMFx6– CAFx6– TCx4
• High risk/lymph node positive– dd ACx4paclitaxel x4 (q2 week)– TACx6– FEC-100 or CAFx6 if taxane not tolerated– TC 4-6 cycles if anthracycline not tolerated
• Her2+– Herceptin based regimen

Neoadjuvant Therapy• Indications
– Inoperable tumors– Inflammatory breast cancer– May consider to increase chance for BCS– In operable breast cancer where chemotherapy is
recommended, neoadjuvant therapy can be considered
• No difference in DFS or OS between neoadjuvant and adjuvant Rx
• Patients with pCR after neoadjuvant Rx have > 90% OS (reported rates range of pCR 4-65%)
• The optimal approach to staging the axilla in patients getting neoadjuvant Rx is not known– This impacts surgery and radiation therapy

Surveillance
• History and physical every 4-6 months for 5 years, then annually
• Mammogram annually (and at 6 months after treatment with XRT and breast conserving surgery)
• Pelvic exam annually for women with intact uterus on tamoxifen
• Other imaging only as indicated by history and physical exam
Case #3
• 56 y.o. female with newly diagnosed stage III right breast cancer (IDC, gr 2, ER+, PR-, Her2/neu-)
• On staging studies found to have multiple bony lesions on bone scan and suspicious liver lesions on CT
• Liver bx-consistent with metastatic breast cancer
• What do you do?

Disease Recurrence
ER, PR, HER2/neu status
ER+ ER-HER2/neu+
Hormonal therapy
2nd line/3rd line hormonal
therapy
Chemotherapy
Chemotherapy
Biopsy
ER+ ER-
Hormonal Therapy +/- Trastuzumab
Chemotherapy + Trastuzumab
Chemotherapy + Trastuzumab
Metastatic disease: General principles
• Hormonal therapy for indolent disease• Trastuzumab-based therapy for HER2/neu
positive disease• Single agent chemotherapy for
aggressive/symptomatic disease or disease not responsive to hormonal therapy
• Consider tx with bevacizumab• Polyagent chemotherapy for visceral crisis or
disease requiring rapid response

History of Drug Approvals for Breast Cancer
• General approvals– Methotrexate Dec 1953– Cyclophosphamide Nov 1959– Doxorubicin Aug 1974
• 1st Breast Cancer Approval– Paclitaxel Apr 1994– Docetaxel July 1994– Capecitabine Mar 1998– Pamidronate Sept 1998– Trastuzumab Sept 1998– Epirubicin Sept 1999– Abraxane Jan 2005– Bevacizumab Feb 2008
• Hormonal– Tamoxifen Dec 1977– Anastrozole Dec 1995– Goserelin Dec 1995– Toremifene May 1997– Letrozole July 1997– Exemestane Oct 1999– Fulvestrant Apr 2002
Metastatic Breast Cancer
• Not curable
• 1st recurrence should be biopsied!!
• 1st goal is to maintain good QOL – consider it a chronic disease
• Bisphosphonates for bone metastases

Metastatic disease
• Tumor markers not shown to be helpful in making clinical decisions
• Restaging studies every 3 to 6 months to determine progression, sooner if symptomatic, clinically warranted
• Clinical trials!
High Dose Chemotherapy with Stem Cell Rescue
• Toxicities are substantial, including a 5-8% mortality in past, 1-2% at present
• Overall survival benefit has not been demonstrated; relapse-free benefit is controversial in high risk patients
• No proven benefit in metastatic disease• Should be done only on clinical trials

Conclusions
• Many effective treatment regimens• Efforts now focused on defining subtypes to
individualize treatment and avoid overtreatment

• Questions???