Introduction to aortic surgery
28
Introduction to Aortic Surgery By Staff Members of Dept. of Cardiothoracic Surgery
-
Upload
mohammed-nabil-abd-al-jawad -
Category
Health & Medicine
-
view
26 -
download
0
Transcript of Introduction to aortic surgery

Introduction to Aortic Surgery
ByStaff Members of Dept. of Cardiothoracic Surgery
Disclosures

Learning Objectives
At the end of this lecture you should understand:1. Anatomy of different segments of the Aorta2. Different pathologies affecting the Aorta3. Strategy in management of different pathologies4. Surgical procedures for Aorta
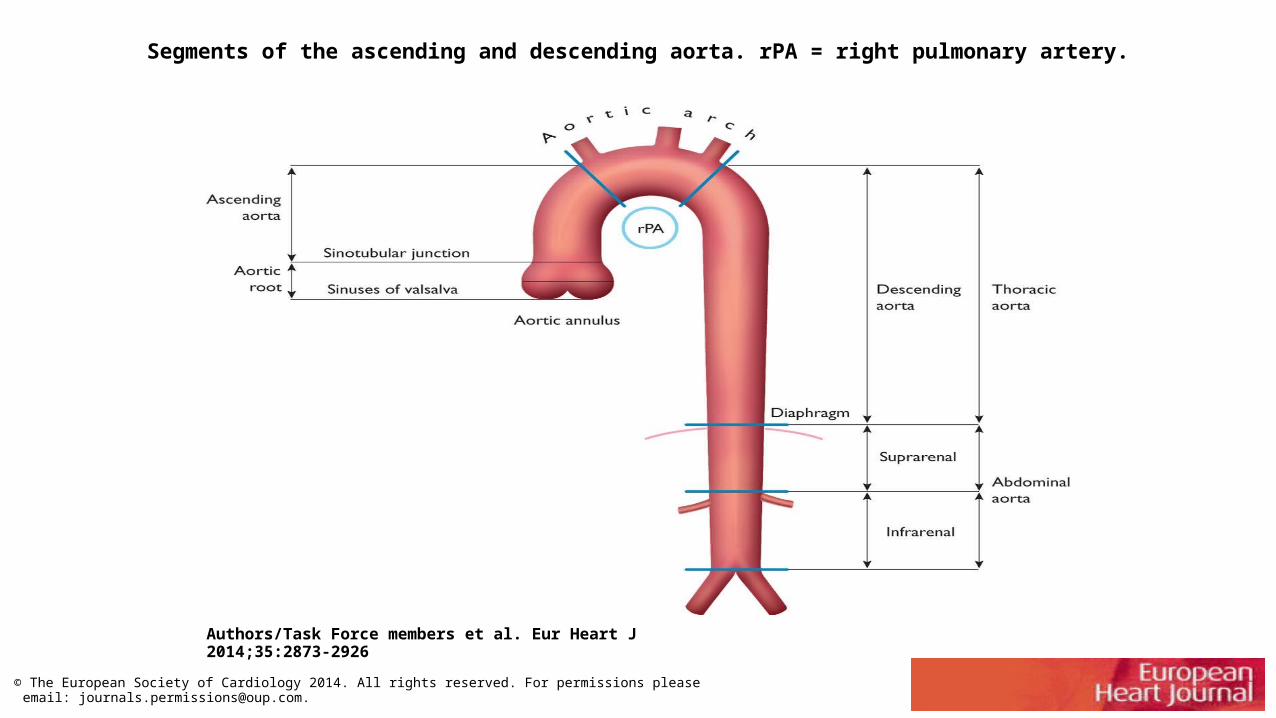
Segments of the ascending and descending aorta. rPA = right pulmonary artery.
Authors/Task Force members et al. Eur Heart J 2014;35:2873-2926
© The European Society of Cardiology 2014. All rights reserved. For permissions please email: [email protected].

Pathology
• Aortic dissection• Aortic aneurysm• Traumatic aortic transection
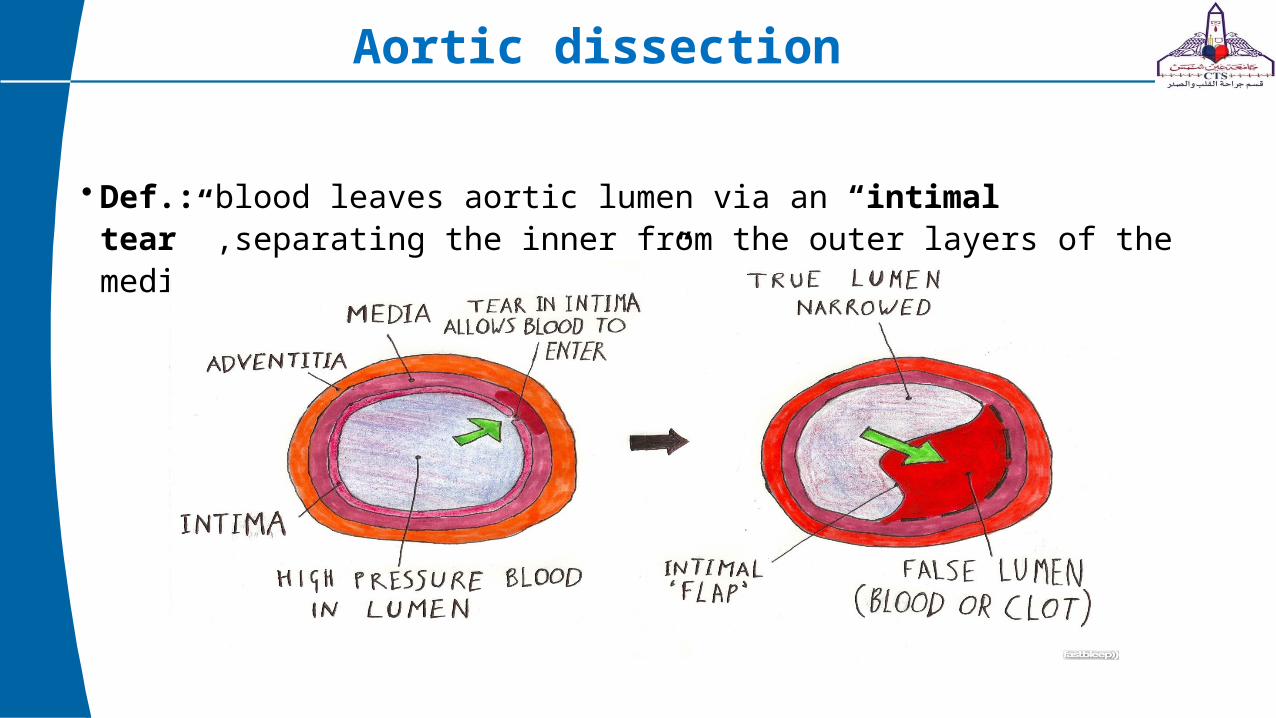
Aortic dissection
• Def.: blood leaves aortic lumen via an “intimal tear” ,separating the inner from the outer layers of the media creating a “false lumen”

Pathology

Classification
• Time of presentation:• Acute: within 14 days• Chronic: after 2 months• Subacute: between 14 days and 2 months
• Site:• Stanford classification• Debakey classification
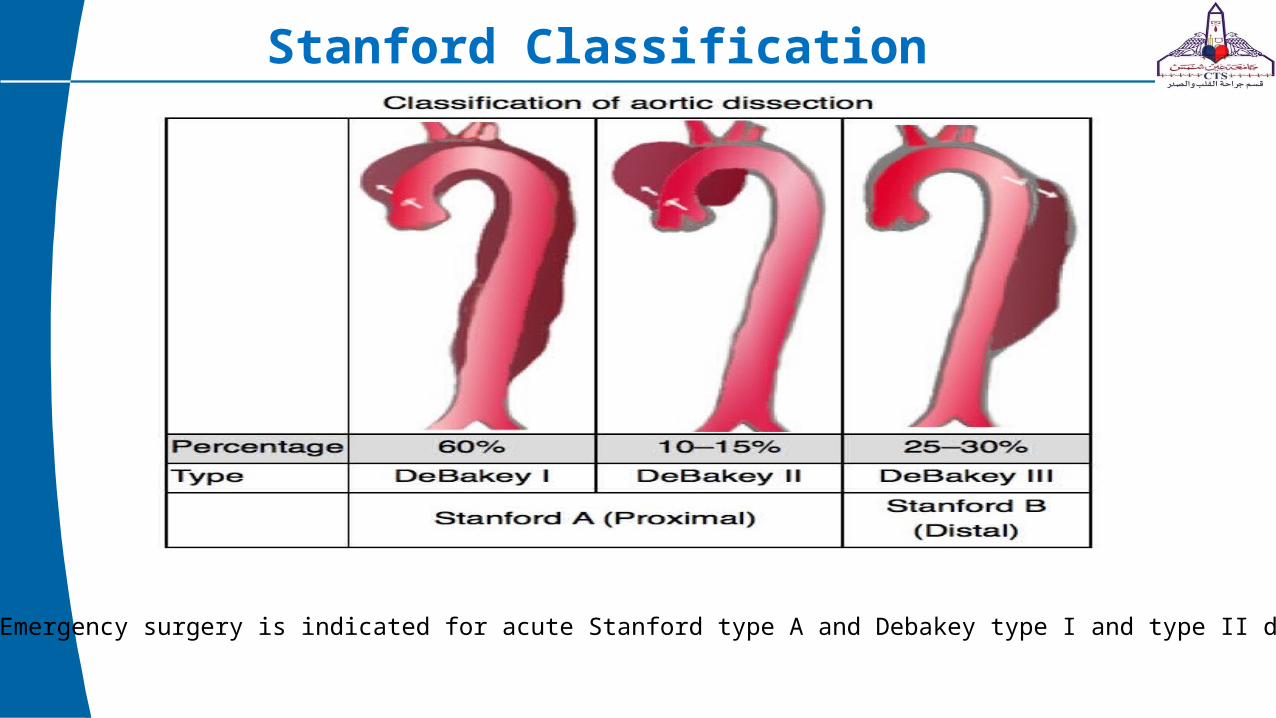
Stanford Classification
Emergency surgery is indicated for acute Stanford type A and Debakey type I and type II dissections

• Pathogenesis is not well understood, several theories might explain it• Cystic medial degeneration :oldest theory, only in minority of patients (lost ground)• Penetration of atherosclerotic ulcer (uncommon)• Intramural hematoma :from bleeding vasa vasorum into the media
• Risk factors include,• Age • Hypertension• CT disorders• Iatrogenic and trauma• High cardiac output status
• Clinical presentation may be in the form of severe “tearing pain” from chest through to the back, sudden death, asymptomatic or as a complicated dissection.
• Complications :• Arch vessel occlusion• Myocardial ischemia• Hemopericardium,hemothorax• Severe aortic valve incompetence• Upper,lower limb,mesenteric or renal ischemmia• CVS or paraplegia

Diagnosis of type A dissection
• History,clinical picture,ECG,CXR,ECHO ,etc……• Imaging
• The primary role is to differentiate between type A dissection (emergency)and type B
• As a rule centers planning to refer suspected acute type A dissection should use the imaging modality in which they have most expertise with minimum delay.
• MRI is the gold standard with a sensitivity and specificity of 98-100%• Aortography used to be the gold standard till recently• CT angiography 90% sensitivity and specificity

Chest X-Ray

CT chest
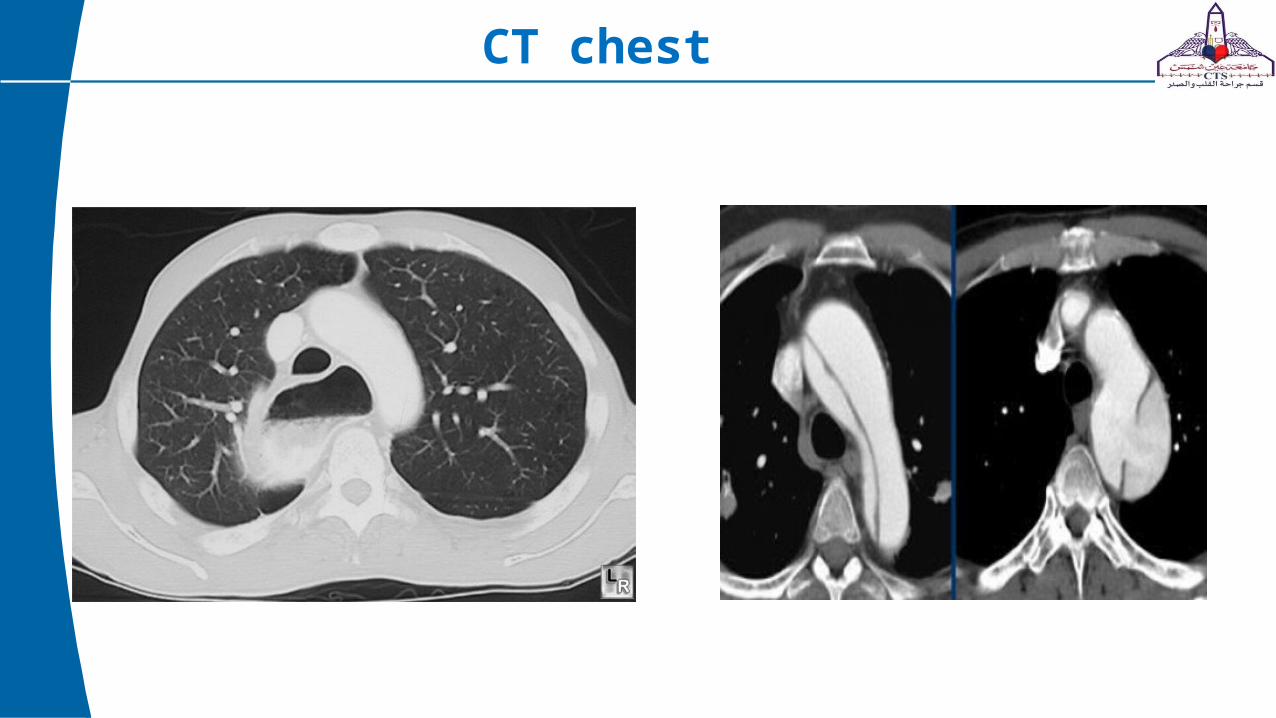
CT chest

MRI
Stanford type B
Management
• Medical treatment has no rule in acute type A dissection• In the acute setting it is usually safest to focus on treating the
immediately life-threatening complication• The main variable to think about are
1. Extent of the resection (root or arch replacement needed ??)2. Cannulation strategy3. Need for circulatory arrest4. Can aorta be clamped ?5. Myocardial protection ,cerebral and spinal protection ,use of DHCA 6. Venting



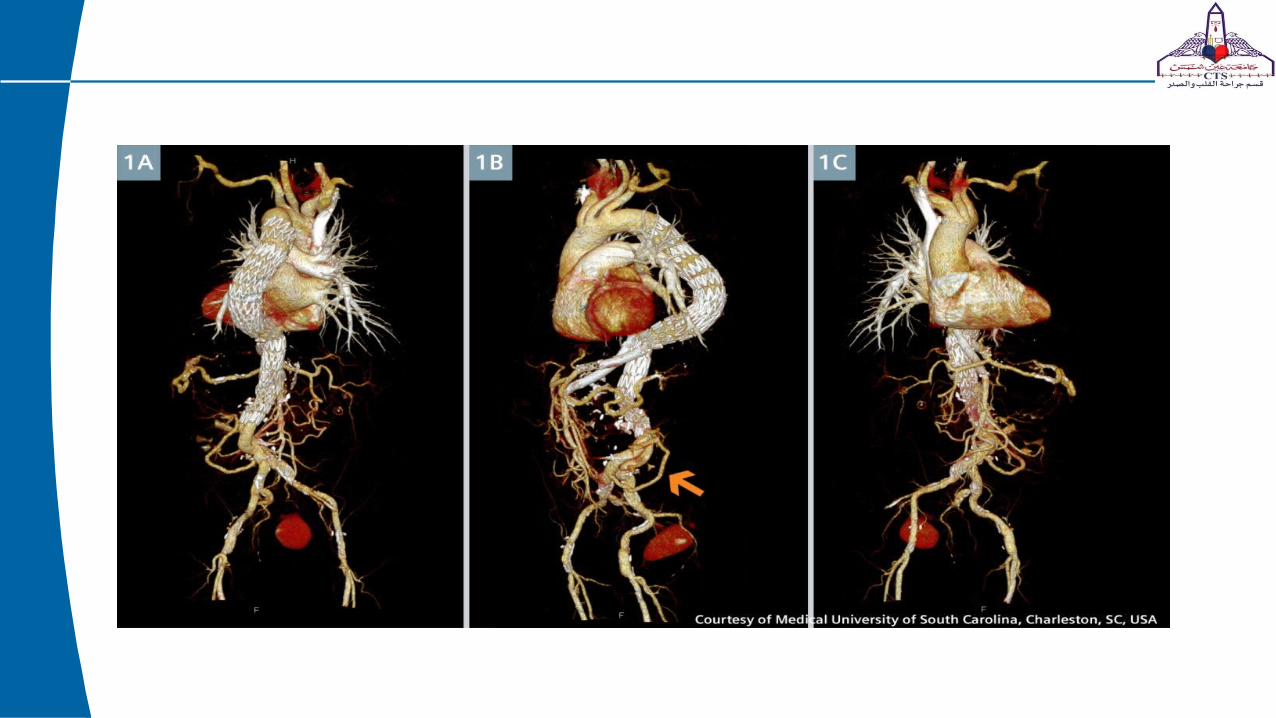
Arch repair Hybrid approach

Type B dissection
• Medical treatment is superior• Surgical approach is for complicated cases • Until recently,Endoluminal stenting




Permanent localized dilatation of an artery by at least 50% compared to normal

Thank you