
Introduction The paramyxoviruses include the most important agents of respiratory infections of...
40
-
Upload
meryl-french -
Category
Documents
-
view
214 -
download
0
Transcript of Introduction The paramyxoviruses include the most important agents of respiratory infections of...


Introduction
The paramyxoviruses include the most important agents of respiratory infections of under 5 years of age.(respiratory
syncytial virus and the parainfluenza viruses)
They are causative agents of two of the most common contagious diseases of childhood.(mumps and measles)

All initiating infection via the respiratory tract
Replication of the respiratory pathogens is limited to the respiratory epithelia, whereas measles and mumps become
disseminated throughout the body and produce generalized disease.

aZoonotic paramyxoviruses.bHemolysin activity carried by F glycoprotein.cHemagglutination and neuraminidase activities carried by HN glycoprotein of respiroviruses and rubulaviruses; H glycoprotein of morbilliviruses lacks neuraminidase activity; G glycoprotein of other paramyxoviruses lacks both activities.dC, cytoplasm; N, nucleus.

Classification
• Paramyxoviridae
• The Paramyxoviridae family is divided into two subfamilies (and) and seven genera, six of which contain human pathogens (Respirovirus, Rubulavirus, Morbillivirus, Henipavirusa, Pneumovirus, Metapneumovirus)
Paramyxovirinae
Pneumovirinae

Properties of Paramyxoviruses
Virion:Spherical,pleomorphic,150nm or more in diameter (helical nucleocapsid, 13–18 nm)
Composition: RNA (1%), protein (73%), lipid (20%), carbohydrate (6%) Genome: Single-stranded RNA, linear, nonsegmented, negative-sense,
noninfectious, about 15 kb
Proteins: Six to eight structural proteins Envelope: Contains viral glycoprotein (G, H, or HN) (which sometimes carries
hemagglutinin or neuraminidase activity) and fusion (F) glycoprotein; very fragile
Replication: Cytoplasm; particles bud from plasma membrane Outstanding characteristics:
Antigenically stableParticles are labile yet highly infectious

PARAINFLUENZA VIRUS INFECTIONS
Parainfluenza viruses cause common respiratory illnesses in persons of all ages.
They are major pathogens of severe respiratory tract disease in infants and young children
Involving only the nose and throat, resulting in a harmless "common cold" syndrome.
Infecting the larynx (حنجره) and upper trachea, resulting in croup (laryngotracheobronchitis)
Characterizing Croup by respiratory obstruction due to swelling of the larynx and related structures.

Types 1 and 2, may involve the larynx and upper trachea, resulting in croup
The infection may spread deeper to the lower trachea and bronchi, resulting in pneumonia or bronchiolitis, especially with type 3, but at a much lower frequency than that observed with RSV
Reinfections with parainfluenza viruses are common.
The severe illness associated with type 3 occurs mainly in infants under the age of 6 months. croup or laryngotracheobronchitis is more likely
to occur in older children, between ages 6 months and 18 months.
Pathogenesis & Pathology

Factors involving in severity
both viral and host properties Susceptibility of the protein to cleavage by different proteases, Production of an appropriate protease by host cells, Immune status of the patient Airway hyperreactivity.
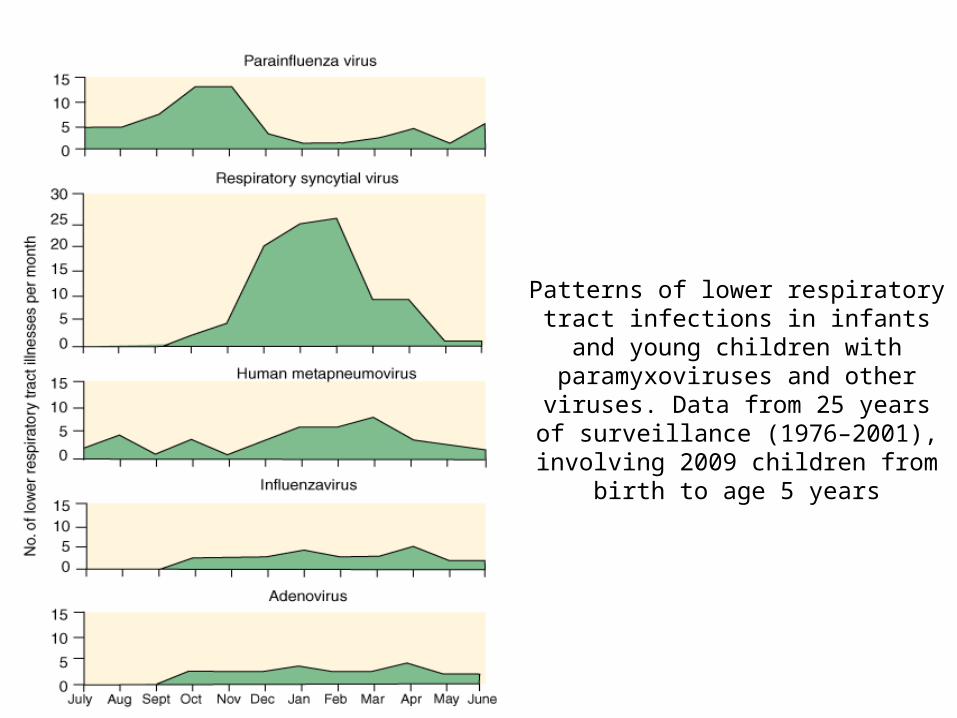
Patterns of lower respiratory tract infections in infants and young children with paramyxoviruses and other viruses.
Data from 25 years of surveillance (1976–2001), involving 2009 children from birth
to age 5 years

Laboratory Diagnosis
a) ANTIGEN DETECTION (direct or indirect immunoflorescence)b) ISOLATION & IDENTIFICATION OF VIRUS (Nasal washes)
c) NUCLEIC ACID DETECTIONd) SEROLOGY

Epidemiology Parainfluenza viruses are a major cause of lower respiratory tract disease
in young children
Type 3 is most prevalent parinfluenza, cause endemics during spring
1 and 2 tend to cause epidemics during the fall or winter
Parainfluenza viruses are transmitted by direct person-to-person contact or by large-droplet aerosols
Parainfluenza viruses are troublesome causes of nosocomial infection in pediatric wards in hospitals.

Treatment & Prevention
Contact isolation precautions gowning and hand washing by medical personnel.
Ribavirin has been used with some benefit in treatment of immunocompromised patients with lower respiratory tract disease
No vaccine

RESPIRATORY SYNCYTIAL VIRUS (RSV) INFECTIONS
RSV is the most important cause of lower respiratory tract illness in infants and young children
Replication occurs initially in epithelial cells of the nasopharynx.
Virus may spread into the lower respiratory tract and cause bronchiolitis and pneumonia.
Bronchiolitis is the distinct clinical syndrome associated with this virus
Respiratory syncytial virus is an important cause of otitis media

Epidemiology
Respiratory syncytial virus is distributed worldwide and is recognized as the major pediatric respiratory tract pathogen
RSV is the most common cause of viral pneumonia in children under age 5 years but may also cause pneumonia in the elderly or in immunocompromised persons.
Spread by large droplets and direct contact

Laboratory Diagnosis
a) ANTIGEN DETECTIONb) ISOLATION & IDENTIFICATION OF VIRUSc) NUCLEIC ACID DETECTIONd) SEROLOGY

Treatment
Depends primarily on supportive care.Ribavirin administered in an aerosol for 3–6
days

Mumps is an acute contagious disease characterized by nonsuppurative enlargement of one or both salivary glands (90% are both).
Mumps virus mostly causes a mild childhood disease, but in adults complications including meningitis and orchitis are fairly common.
More than one-third of all mumps infections are asymptomatic.
Mumps Virus Infections

Pathogenesis & Pathology
Humans are the only natural hosts for mumps virus.
Primary replication occurs in nasal or upper respiratory tract epithelial cells.
Viremia then disseminates the virus to the salivary glands and other major organ systems.
Clinical Findings
Majority of infections in children under 2 years of age.
The most characteristic feature of symptomatic cases is swelling of the salivary glands (Parotitis, 20-70%)
The incubation period may range from 2 to 4 weeks but is typically about 14–18 days.
Symptoms:
Nonspecific prodrome of low-grade fever, headache, malaise, myalgias
Lower respiratory tract illness, especially preschool-aged children

Mumps Complications:Unvaccinated Persons
• Common• Meningitis – 5-15% of cases• Orchitis – 20%-30% of cases in post-pubertal males
(rarely sterility)
• Uncommon• Pancreatitis • Encephalitis• Deafness • Death

Mumps Epidemiology
• Transmission– Route: person-to-person (respiratory secretions, e.g. saliva),
respiratory droplets, fomites– Closer contact is necessary for transmission of mumps than
for transmission of measles or varicella.
• Risk of disease: > 50% reported cases 5-9 yrs but shift to younger children with child care
• Seasonality: Peak late winter and spring

Mumps Diagnosis• Laboratory (validation)
• Isolation• PCR• Serologic
– IgG– IgM

Measles highly infectious disease characterized by fever, respiratory
symptoms, and a maculopapular rash.
Measles (Rubeola) Virus Infections

.
Humans are the only natural hosts
Viral replication begins in the respiratory epithelium
Multinucleated giant cells with intranuclear inclusions are seen in lymphoid tissues throughout the body (lymph nodes, tonsils).
The virus-specific immune response is detectable when the rash appears.
The rash develops as a result of interaction of immune T cells with virus-infected cells in the small blood vessels and lasts about 1 week.
Involvement of the central nervous system is common in measles.
progressive measles inclusion body encephalitis may develop in patients with defective cell-mediated immunity.
Pathogenesis & Pathology

Timing of neurologic complications of measles. PIE, postinfectious encephalomyelitis (also called acute disseminated encephalomyelitis); MIBE, measles inclusion body encephalitis; SSPE, subacute sclerosing panencephalitis. Encephalitis occurs in about one out of every 1000 cases of measles, whereas SSPE is a rare late complication that develops in about one out of 300,000 cases.
SSPE( subacute sclerosing panencephalitis ) A rare late complication of measles This fatal disease is caused by virus that remains in the body after acute measles infection

The prodromal phase is characterized by fever, sneezing, coughing, running nose, redness of the eyes, Koplik spots, and lymphopenia
The rash starts on the head and then spreads progressively to the chest, the trunk, and down the limbs
The most common complication of measles is otitis media (5–9% of cases)
Pneumonia is the most common life-threatening complication of measles, caused by secondary bacterial infections
Pulmonary complications account for more than 90% of measles-related deaths
Clinical Findings

.
There is only one antigenic type of measles virus
Infection confers lifelong immunity
Measles immune responses are involved in disease pathogenesis
Local inflammation causes the prodromal symptoms, and specific cell-mediated immunity plays a role in development of the rash
Immunity

.
Natural history of measles infection. Viral replication begins in the respiratory epithelium and spreads to monocyte-macrophages, endothelial cells, and epithelial cells in the blood, spleen, lymph nodes, lung, thymus, liver, and skin and to the mucosal surfaces of the gastrointestinal, respiratory, and genitourinary tracts. The virus-specific immune response is detectable when the rash appears. Clearance of virus is approximately coincident with fading of the rash.

Antigen & Nucleic Acid DetectionMeasles antigens can be detected directly in epithelial cells from respiratory secretions, the nasopharynx, conjunctiva, and urine. Antibodies to the nucleoprotein are useful because that is the most abundant viral protein in infected cells.Detection of viral RNA by RT-PCR is a sensitive method that can be applied to a variety of clinical samples for measles diagnosis
Isolation & Identification of VirusNasopharyngeal and conjunctival swabs, blood samples, respiratory secretions, and urine collected from a patient during the febrile period are appropriate sources for viral isolation.
Serologic confirmation of measles infection
Laboratory Diagnosis

The virus is highly contagious, there is a single serotype, there is no animal reservoir , and inapparent infections are rare.
Transmission occurs predominantly via the respiratory route .
Measles is endemic throughout the world.
Epidemiology
.
Vitamin A decreasing the mortality and morbidity
Ribavirin,
A highly effective and safe attenuated live measles virus vaccine a (monovalent form) Measles vaccine is available in and in combination with live attenuated rubella vaccine (MR) live attenuated rubella and mumps vaccines (MMR), and live attenuated varicella vaccine (MMRV)
Treatment, Prevention, & Control

Rubella (German Measles) Virus
Rubella (German measles; 3-day measles) is an acute febrile illness with rash and lymphadenopathy
Affects children and young adults
It is the mildest of common viral exanthems
Infection during early pregnancy may result congenital malformations and mental retardation
Electron micrograph of rubella

Classification
A member of the Togaviridae family
The sole member of the genus Rubivirus
Classified into two clinical groups
Postnatal Rubella Congenital Rubella Syndrome

Neonatal, childhood, and adult infections occur through the mucosa of the upper respiratory tract
In 20–50% of cases, primary infection is subclinical.

Clinical Findings
Rubella usually begins with malaise, low-grade fever, and a morbilliform rash appearing on the same day
The rash starts on the face, extends over the trunk and extremities, and rarely lasts more than 3 days
Transient arthralgia and arthritis are commonly seen in adults, especially women
Rare complications include thrombocytopenic purpura and encephalitis.

Maternal viremia during pregnancy may result in infection of the placenta and fetus
the earlier in pregnancy infection occurs, the greater the damage to the fetus
Inapparent maternal infections can also result in fetal death and spontaneous abortion
Symptomes: cataracts, cardiac abnormalities, and deafness, microcephaly, rash, hepatosplenomegaly, jaundice, and meningoencephalitis

Laboratory Diagnosis
specific laboratory studies
Isolation & Identification of Virus
Nucleic Acid Detection
Serology
Nasopharyngeal or throat swabs taken 6 days before and after onset of rash are a good source of rubella virus

Epidemiology
a peak incidence in the spring
Epidemics occur every 6–10 years, with explosive pandemics every 20–25 years
Infection is transmitted by the respiratory route
rubella is not as contagious as measles

Treatment, Prevention, & Control Rubella is a mild, self-limited illness, and no specific treatment is indicated
It can be prevented by :
The vaccine is available as a single antigen or combined with measles and mumps vaccine
The primary purpose of rubella vaccination is to prevent congenital rubella infections
Immune globulin intravenous (IGIV) injected into the mother does not protect the fetus against rubella infection


















