Introducing the Pharma 2020 Series July 2011

of 16
Transcript of Introducing the Pharma 2020 Series July 2011
-
8/10/2019 Introducing the Pharma 2020 Series July 2011
1/16
These reports lookinto the future of the Pharmaceuticals and LifeSciences value chain. Andthey include an analysis ofthe strategies available tocompanies.
www.pwc.com/pharma
Introducing the Pharma 2020
Series
-
8/10/2019 Introducing the Pharma 2020 Series July 2011
2/16PwC2
Pharma2020: Thevision #
Pharma 2020: The visionWhich path will you take?*
Pharmaceuticals
*connectedthinking
Pharma 2020: Taxing times aheadWhich path will you take?
Pharmaceuticals and LifeSciences
Pharma 2020: Challenging business modelsWhich path will you take?
Pharmaceuticals and LifeSciences
Pharma2020: VirtualR&D 1
Pharma 2020: Virtual R&DWhich path will you take?
Pharmaceuticals and LifeSciences This report, published in June2008, explores opportunitiesto improve the R&D process. Itproposes that new technologies will enable the adoption of virtual R&D; and by operatingin a more connected world theindustry, in collaboration withresearchers, governments,healthcare payers andproviders, can address thechanging needs of society moreeffectively.
Published in June 2007, thispaper highlights a number ofissues that will have a majorbearing on the industry by2020. The publication outlinesthe changes we believe willbest help pharmaceuticalcompanies realise the potentialthe future holds to enhance the value they provide toshareholders and society alike.
The fth report in our series,published in December 2009,focuses on the opportunitiesand challenges from a taxperspective. It discusses howthe political, economic,scienti c and social trendscurrently shaping thecommercial environment,together with the developmentof new, more collaborativebusiness models, will exertincreasing pressure on effectivetax rates within the industry. Italso shows how companies canadapt their tax strategies tosupport the provision ofoutcomes-based healthcare andremain competitive.
Fourth in the Pharma 2020series and published in April2009, this report highlightshow Pharmas fully integratedbusiness models may not bethe best option for the pharmaindustry in 2020; morecreative collaboration modelsmay be more attractive. Thispaper also evaluates theadvantages and disadvantagesof the alternative businessmodels and how each stands
up against the challengesfacing the industry.
All these publicat ions are available to download at: www.pwc.com/pharma2020
Pharma 2020: Marketing the futureWhich path will you take?
Pharmaceuticals andLife Sciences Published in February 2009,this paper discusses the keyforces reshaping thepharmaceutical marketplace,including the growing powerof healthcare payers, providersand patients, and the changesrequired to create a marketingand sales model that is t forthe 21st century. Thesechanges will enable theindustry to market and sell its
products more cost-effectively,to create new opportunitiesand to generate greatercustomer loyalty across thehealthcare spectrum.
Publications in this series include:
In our sixth release of theseries, published in February2011, PwC discusses howpharma companies mustdevelop different supply chainmodels, learn to use supplychains as a marketdifferentiator and revenuegenerator, and recognise howinformation will drive thedownstream ow of productsand services.
-
8/10/2019 Introducing the Pharma 2020 Series July 2011
3/16PwC 3
Pharma 2020: Executive summary
The global market formedicines is growingbut the industry musttransform to capitaliseopportunities
Pharmas strategy of placing big betson a few molecules, promoting themheavily and turning them intoblockbusters worked well for many years, but its R&D productivity hasnow plummeted and theenvironments changing. PwC 1 believes that seven major trends arereshaping the marketplace:
the burden of chronic disease issoaring placing even greaterpressure on already stretched
healthcare budgetshealthcare policy-makers andpayers are increasingly mandating what doctors can prescribe
a growing number of healthcarepayers are measuring thepharmacoeconomic performance ofdifferent medicines. A widespreaduse of electronic medical records will give them the data they need toinsist on outcomes-based pricing
the boundaries between differentforms of healthcare are blurring, asclinical advances render previouslyfatal diseases chronic and theself-medication sector expands
demand for medicines is growingmore rapidly in the emergingeconomies than the industrialisedeconomies
governments everywhere are beginning to focus on preventionrather than treatment, althoughthey have not yet invested verymuch in pre-emptive measures; and
the regulators are becoming morecautious about approving trulyinnovative medicines.
These trends will compound thechallenges Pharma already faces, buttheyll also provide some majoropportunities. So what must theindustry do to capitalise on them? Wethink that itll have to improve itsunderstanding of disease, reduce itsR&D costs signi cantly and spread itsbets to improve its productivity. Itllalso have to tap the potential of theemerging economies and switch fromselling medicines to managingoutcomes. However, few, if any,companies will be able to performthese activities alone.
1 PwC refers to the network of member rms of PricewaterhouseCoopers International Limited (PwCIL), or, as the context requires, individual member rms of thePwC network.
-
8/10/2019 Introducing the Pharma 2020 Series July 2011
4/16PwC 4
Target IDDesign &
initial testingof treatment
Synthesis oftreatment
Testing oftreatment
in vivo
Initial testingin man
Further testingof treatment
in vitro
Mixed computer/labLab work
Testing in man
In silico
Source: PwC
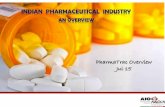
Figure 1: What the research process might look like in 2020
Taking R&D to the virtual levelLets begin with R&D. If Pharmas todevelop safe, ef cacious newmedicines more economically, itllhave to learn much more about howthe human body functions at themolecular level and thepathophysiological changes diseasecauses. Only then will it be able to
develop a better understanding of howto modify or reverse these changes.This is a huge task but one thatseveral emerging technologies canhelp to facilitate.
Semantic technologies will, forexample, make it much easier toidentify the links between a particulardisease and the biological pathways itaffects, or the links between aparticular molecule and its impact onthe human body. Similarly, computer-
aided molecule design will giveresearchers a much better startingpoint in the search for potentmolecules.
Various academic institutes andbioinformatics rms are also buildingcomputer models of different organsand cells, with the ultimate aim ofcreating a virtual man. Developing
such a model will require a massivecollaborative effort far exceeding thatneeded to complete the HumanGenome Project. Nevertheless,predictive biosimulations alreadyplaying a growing role in the R&Dprocess and we anticipate that, by2020, virtual cells, organs and animals will be widely employed inpharmaceutical research (see Figure 1 ).
Of course, even the most robustlymodelled molecules will still have tobe tested in real human beings. Buthere too, we expect some dramaticchanges. When biomarkers fordiagnosing and treating patients moreaccurately are more widely available,for example, the industry will be ableto stratify patients with different butrelated conditions and test newmedicines only in patients who sufferfrom a speci c disease subtype. That will allow the industry to reduce the
number and size of the clinical studiesrequired to prove ef cacy. Semantictechnologies will also play a major rolein improving the development process, while pervasive monitoring will helpPharma track patients on a real-timebasis wherever they are.
-
8/10/2019 Introducing the Pharma 2020 Series July 2011
5/16PwC 5
We think that these scienti c andtechnological advances will ultimatelyrender the current model ofdevelopment, with its four distinctphases of clinical testing, defunct. Acompany will start by administering atreatment to a single patient who hasbeen screened to ensure that he or shehas the right medical pro le. Oncetheres evidence that the treatmentdoesnt cause any immediate adverse
events, itll be sequentiallyadministered to other patients fromas few as 20 to as many as 100. Thedata they generate will be compared todata from the modelling that precededthe study and subjected to techniqueslike Bayesian analysis to adapt thecourse of the study, but the study itself will be conducted in a single,continuous phase (see Figure 2 ).
The development process will alsobecome much more iterative, with
data on a molecule for one diseasesubtype getting fed back into thedevelopment of new molecules forother disease subtypes in the samecluster of related diseases. And thecurrent system of conducting trials atmultiple sites will be replaced with asystem based on independentlymanaged clinical supercentres.
The regulatory process will changeequally substantially over the nextdecade. First, therell be a commonregulatory regime for all healthcareproducts and services, rather thanseparate regimes for pharmaceuticals,medical devices, diagnostics and thelike. Indeed, there may even be asingle global system, administered bynational or federal agenciesresponsible for ensuring that new
treatments meet the needs of patients within their respective domains,although we think the latter is lesslikely.
Second, the current all-or-nothingapproach to the approval of newmedicines will be replaced by acumulative process, based on thegradual accretion of data. In other words, all newly approved therapies will receive live licences conditionalon further in-life testing to
substantiate their safety and ef cacyin larger populations, differentpopulations or the treatment of otherconditions.
But, if they are to capitalise on the newtechnologies now emerging and thecreation of a nimbler, morecollaborative regulatory regime, manycompanies will have to make
Companies will use virtual R&D to increaseinnovation and reduce commercial de cit
Confidence in mechanismfrom research work
Epidemiological data
Disease knowledge
Knowledge / Data from clinicalusage or similar products
Proof of value requirementsCIE
CIS
Launch
1 year
1.5 years
0.5 year
First into man(adaptive design) 20-100 pts
Limitedclinical use
Clinical data / Knowledge incorporated into studieson future indications/populations
Automatedsubmission/approvals
Figure 2: What the development process might look like in 2020
Source: PwC
signi cant organisational andbehavioural changes. Theyll, forexample, have to decide whether they want to focus on mass-marketmedicines or speciality therapies, and whether they want to outsource most oftheir research or keep it in-house.Those that regard R&D as an integralpart of their activities may also need toreview the way they manage their R&Dand remunerate their scienti c staff.
-
8/10/2019 Introducing the Pharma 2020 Series July 2011
6/16
-
8/10/2019 Introducing the Pharma 2020 Series July 2011
7/16PwC 7
We believe that timely access to various emerging technologies willhelp to increase the ef ciency of themanufacturing and distributionfunctions. It will also rede ne theinterface with the patient bringingpharma companies even closer topatients.
Additionally, more collaborationbetween the parties involved inhealthcare provision will contribute tomake the industry more ef cient. Thesupply chains for designing,manufacturing and distr ibutingpharmaceuticals and medical devicesplus those providing healthcareservices wil l integrate. The aim is thatall partners can see the full pictureand can plan ahead more accuratelyand cost-effectively.
The successful pharmaceuticalcompanies of the future will be thosethat integrate all these opportunitiesand build supply chains with newmanufacturing, distribution andservice-management techniques. Weoutline four potential scenarios.Depending on their product andchannel portfolio, most companies will have to manage more than onescenario simultaneously.
Companies that concentrate onspecialist therapies might exit frommanufacturing altogether and, instead,become a virtual manufacturer. Theylloutsource the entire supply fromproduction of the earliest clinicalbatches to full-scale manufacturing,packaging and distribution through anetwork of integrated supply partners(see Figure 6 ).
Alternatively, they might positionthemselves as service innovators,building supply chains that arecapable of manufacturing anddistributing complex treatments as well as managing multiple suppliers ofintegrated, valued-added healthmanagement services.
Mass-market manufacturers, such asthe makers of generics, might positionthemselves as high-volume, low-costproviders, borrowing lessons in leanmanufacturing, strategic pricing andinventory management from theconsumer products industry. Anotheroption for mass mass-marketmanufacturers is to turn their supplychains into pro t centres that combineeconomic manufacturing anddistribution of satellite services, such asdirect-to-patient delivery, secondarypackaging or distribution to hospitalsand pharmacies. Theyll then franchise
those pro t centres as a stand-aloneoffering for both internal and externalcustomers.
By 2020, the most successful companies will be those that seize theinitiative and start building agile, ef cient supply chains which bringthem closer to the patient
-
8/10/2019 Introducing the Pharma 2020 Series July 2011
8/16PwC8
Figure 4: Four options exist for restructuring the pharmaceutical supply chain
In all four cases, the supply chain ofthe future will need to be much morepatient-focused. In a world whereoutcomes count for everything, its notmolecules that create value but,
rather, the ability to integrate data,products and services in a coherentcare package. Understanding this shif tof emphasis from products to patientoutcomes is key. Those organisationsthat recognise the shift will be able todeliver signi cant bene ts to everystakeholder in the healthcare valuechain: payers, providers, patients andshareholders.
Operations strategy
Virtual manufacturer
Create a virtual networkof integrated supplypartners
Build a service-orientedsupply chain to enhancebrands and differentiate
company from itscompetitors
Build a reliable, no-frillssupply chain to deliverproducts as
economically aspossible
Combine agile,economic manufacturingand distribution with the
provision of satelliteservice to generateprots
Service innovator Low-cost provider Prot centre
Specialist Therapies Mass-market medicines
Source: PwC
-
8/10/2019 Introducing the Pharma 2020 Series July 2011
9/16PwC 9
A new approach tomarketing and salesThe industrys marketing and salesmodel will likewise have to undergomajor alterations, as pay-for-performance becomes the norm inmany countries and the opportunitiesfor generating value from pureproduct offerings diminish. Manycompanies will have to analyse their
own value chains to identifyopportunities for working moreclosely with healthcare payers andproviders. They will, for instance,have to consult payers, providers andpatients when deciding whichcompounds to progress through theirpipelines. Some companies now lookat whether the products theyredeveloping are more effective thanother existing therapies. Very fewfocus on understanding the payersperspective. We believe that allcompanies should extend the conceptof de-risking from the clinical to thecommercial sphere to ensure thattheyre making medicines the marketreally wants to buy (see Figure 5 ).
Similarly, many companies will haveto supplement the therapies theydevelop with a wide range of health
management services. Mosttreatments perform much better inclinical trials than they do in everydaylife, partly because the level ofcompliance is much higher. Anypharmaceutical company that wantsto command premium prices for itstherapies will have to provide a rangeof products and services from whichpatients can choose all but the coreprescription. They will need to help
patients manage their health.This route has several signi cantadvantages. Itll enable companies togenerate new sources of revenue,differentiate their offerings moreeffectively and protect the value of themedicines they make. But itll alsoentail the formation of numerousalliances with local service providersand even rival manufacturers; thedevelopment of a secure, interoperabletechnological infrastructure; the
management of new intellectual rightsissues; the creation of much strongerbrands; and the rede nition of theindustrys role. Instead of trying tostimulate prescription sales, its task will be to help patients manage thedisease lifecycle.
The shift to performance-basedpricing will dictate other changes, too,
Smaller, refocused salesforces will enablepharma companies tocreate greater value forpatients
Percentage of spending in each phase of R&D. 11.3% of spending uncategorised
Preclinical Phase I Phase II Phase III Regulatory Phase IV25.7 5.8 11.7 25.5 6.9 13.3
Point at which
pharmaceuticalcompaniesshould be
thinking aboutpricing to de-risk
their portfolios
Point at which
pharmaceuticalcompanies
typically start
thinking aboutpricing
Figure 5: Pharma needs to use a price de-risking strategy in early development
Source: PwC
-
8/10/2019 Introducing the Pharma 2020 Series July 2011
10/16PwC10
including the need for a more exibleapproach to pricing. The introductionof live licences and increasingimportance of the emerging markets will reinforce this trend. Any companythat launches a new healthcarepackage will have to negotiate pricerises in line with the extension of theterms on which that package can bemarketed. And if it wants to establish astronger footing in the emerging
world, itll have to use differentialpricing both within and betweencountries.
Increasing payer pressure on pricingand outcomes is forcing companies toincrease its efforts to improve patientcompliance. Improved patientcompliance provides numerousbene ts, not least, individual healthoutcomes, but it also helps to drivehealthcare cost and improved revenuesfor companies. With performance
based pricing becoming morecommon, a focus on patientcompliance through education andtechnology will be a necessity.
Lastly, the industry leaders will haveto develop comprehensive strategiesfor marketing and selling specialisthealthcare packages, a process that will require the development of newskills and routes to market; and theyl lhave to revolutionise their marketingand sales functions. By 2020, the role
of the traditional sales representative will be largely obsolete. Conversely,the industry will have a much greaterneed of people with the expertise tobuild brands; manage a network ofexternal al liances; negotiate withgovernments and health insurers;
liaise with secondary-care specialists;and communicate with patients.
The need for newbusiness modelsThe changes weve outlined above willall necessitate the development ofmultinational, multi-disciplinarynetworks drawing on a much widerrange of skills than Pharma alone canprovide. Most companies will therefore need to adopt new business models.
We believe that two principal models federated and fully diversi ed willemerge. The federated modelcomprises a network of separateorganisations linked by a sharedpurpose and infrastructure. The fullydiversi ed model comprises a networkof entities owned by a single parentcompany. Weve also identi ed two variants of the federated model. In the virtual version, a company outsourcesmost or all of its activities; in the venture version, it manages a portfolioof investments (see Figure 6 ).
These models are not mutuallyexclusive. A fully diversi ed companymight choose to use a federated modelfor certain aspects of its business, and vice versa. But we think that thefederated model will ultimatelydominate, primarily because itsquicker and more economic to
implement.The transition will not be easy,because collaborative business modelsare far more complex than theintegrated model thats previouslyprevailed.
-
8/10/2019 Introducing the Pharma 2020 Series July 2011
11/16PwC 11
Disrupting the existing order can alsohave a major impact on a companysshort-term performance. We anticipatethat many companies which choosethe federated model will adopt aprogressive approach. Theyll star t with opportunistic alliances; use themost successful alliances as buildingblocks to create more strategic,longer-lasting coalitions; and, nally,use the most successful coalitions to
create a fully federated network oflong-term partners.
The prospects for any pharmaceuticalcompany that can make the switch are very promising. To date, Pharma hasfocused on the pro ts it can earn fromthe estimated 10-15% of the healthbudget that goes on medicines.
Yet there are many opportunities togenerate revenues by improving the way in which the remaining 85-90% isspent. Its these opportunities theindustry will need to address in thebrave new world of 2020.
Figure 6: The different business models
Challenging times require bold movesif pharma companies are to survive the immediate storm
Virtual variant Venture variant
Owned: Fully Diversified modelCollaborative: Federated model
Network of separate entities
Based on shared goals and infrastructure
Draws on in-house and/or external assets
Combines size with flexibility
Network of contractors
Activities coordinated by one companyacting as hub
Operates on project-by-project basis
Fee-for-service financial structure
Portfolio of investments
Based on sharing of intellectual property/ capital growth
Stimulates entrepreneurialism and innovation
Spreads risk across portfolio
Network of entities owned by oneparent company
Based on provision of internally integratedproduct-service mix
Spreads risk across business units
Source: PwC
-
8/10/2019 Introducing the Pharma 2020 Series July 2011
12/16PwC12
A heavier tax burdenThe collaborative business models willenable Pharma to deliver healthcarepackages that comprise medicines andsupporting services supplied locally(such as drug administration training,home delivery, physiotherapy, healthscreening and exercise facilities). Thisnew way of doing business, combined with the political and economic trends
already shaping the general commercialenvironment, will have major taxrepercussions. We anticipate that theindustrys corporate tax burden will risesigni cantly over the next 10 years unless it undertakes variousstrategies to mitigate the impact.
Governments of the industrialised world will st ruggle to repair public
nances damaged by debts accrued inmanaging the global recession. Theylldecrease the opportunities that have
allowed the industry to reducecorporate taxes by moving pro ts fromhigher-tax to lower-tax territories.
Along with imposing more stringenttax regulations, the major powerscould place trading restrictions ontraditional tax havens that refuse tocooperate. The tax authorities in mostcountries will work more closely withtheir counterparties in otherterritories to control multinationalstax-reducing practices.
As Big Pharma moves toward theprovision of integrated healthcarepackages, the proportion of incomegenerated in the industrys end markets
will increase. Demand for such servicesinitially is likely to be greatest in theindustrialised world, where corporateincome tax rates are often higher. That will make it more dif cult forcompanies to assign pro ts legitimatelyfrom high- to low-tax jurisdictions.
Undertaking or managing morebusiness activities in end markets willalso make it harder to prove that acompany has not created a permanentbusiness establishment in countries where services are delivered. This mayincrease the risk of failing to obtaindouble tax relief, as allowed underinternational tax treaties, and of beingtaxed on the same earnings in thehome country and the country wherethe services have been delivered.
The provision of direct-to-patientservices wil l additionally make it evenmore dif cult for the industry tonegotiate its way through the maze of withholding tax regulations. Countr ieshave traditionally adopted a morediverse approach to the application of withholding taxes to payments forservices than they have for goods.These variations can produce morematerial for tax disputes.
-
8/10/2019 Introducing the Pharma 2020 Series July 2011
13/16PwC 13
The provision of services also mayaffect the way the income ofcontrolled foreign corporations (CFCs)is taxed. In many developed countries,tax laws provide that CFC pro ts maybe attributed to the holding companyand taxed immediately, rather thanbeing taxed only when (and if) theyare repatriated. However, CFClegislation often distinguishesbetween passive income (i.e.,
interest, dividends, annuities, rentsand royalties), which is taxed, andactive income (i.e., income fromcommercial activities), which is nottaxed. Some of the new healthcareservices pharmaceuticalmultinationals will provide may fallinto the taxable category.
Providing integrated packages alsocould increase compliance costs andrisks associated with indirect taxes,such as value-added tax (VAT). Some
VAT regimes may apply theappropriate rate of VAT to eachcomponent of a package, while othersmay treat the package as a compositeand apply the rate of the principalelement to the entire bundle.
The increasing importance ofemerging markets, an evolving supplychain, and a shift to services couldalso have a major bearing on customs
duties and other trade-related tariffspharmaceutical companies incur.Some countries levy signi cant importduties on key active pharmaceuticalingredients and nished products, andthe valuation of combined product-service offerings for customs purposescould prove complicated.
Finally, because of more complexsupply chains, it may become moredif cult to use transfer pricing i.e.,the allocation of income amongrelated business entities via thepricing of intellectual property,tangible goods, services, and loans orother nancial transactions toavoid double taxation. Many taxauthorities already are clamping downon abusive transfer pricing practices,such as shifting pro ts arti cially froma high- to a low-tax jurisdiction, bymaximising expenses in the formerand income in the latter.
To deal with these multiple pressures,companies will need to rethink theirtax strategies. The choice of legalentity and structure of commercialarrangements, for example, will havea signi cant impact on taxation. Onesolution for multinationals might be tolocate more business activities, such asR&D, manufacturing, and marketing,in regional hubs in low-tax countries.
Some might choose to move theirentire operations to a low-tax location.
On the positive side, the competitionto attract companies engaging in R&D will intensify. Some countries willoffer generous tax incentives andcredits and several will be newcompetitors keen to build knowledge-based economies. Tax departments will need to keep abreast of theseincentives so they can adviseleadership on how to take advantageof tax-reduction opportunities.
Tax departments will also have tobuild much closer relationships withthe operational parts of the businessand acquire a much more detailedunderstanding of the complexities ofsupply chain arrangements. Those taxdepartments that combine a stronggrasp of long-term strategy andeffective lobbying with a detailedtactical understanding of the way in which products are distributed and value is created will be best placed tohelp pilot their companies along thepath to future prosperity.
Tax strategy will be the crux, not anafterthought, of long-term business plans
-
8/10/2019 Introducing the Pharma 2020 Series July 2011
14/16
-
8/10/2019 Introducing the Pharma 2020 Series July 2011
15/16PwC 15
Luxembourg Laurent Probst[352] 0 494 848 2522
Malta Adrian Spiteri[356] 2564 7038
MexicoJorge Luis Hernndez Baptista[52] 55 5263 6106
Netherlands Arwin van der Linden[31] 20 5684712
Norway Fredrik Melle[47] 95 26 00 13
PeruFelix Horna[511] 211 6500
PhilippinesChe Javier[63] 2 845 2728
PolandMariusz Ignatowicz[48] 22 523 4795
Portugal Ana Lopes[351] 213 599 159
RomaniaMihaela Mitroi[40] 21 225 3717
Russia Alina Lavrentieva[7] 495 967 6250
Singapore Abhijit Ghosh[65] 6236 3888
SlovakiaRastislava Krajcovicova[421] 2 5935 06 16
South AfricaDenis von Hoesslin[27] 117 974 285
SpainRafael Rodrguez Alonso[34] 91 568 4287
SwedenMikael Scheja[46] 8 555 33 038
SwitzerlandClive Bellingham[41] 58 792 2822
TaiwanElliot Liao[886] 3 5780205 26217
ThailandZoya Vassilieva[66] 2 344 1115
Turkey Zeki Gunduz[90] 212 326 64 100
UkraineRon Barden[380] 44 490 6777
United Arab EmiratesSally Jeffery [971] 4 304 3154
United Kingdom Andrew Packman[44] 1895 522104
United StatesMichael Swanick [1] 267 330 6060
Uruguay Richard Moreira[598] 2916 0463
VenezuelaLuis Freites[58] 212 700 6966
-
8/10/2019 Introducing the Pharma 2020 Series July 2011
16/16
About Global Pharmaceuticals and Life Sciences Industry GroupPwC rms provide industry-focused assurance, tax and advisory services to enhance value for their clients. More than 161,000people in 154 countries in rms across the PwC network share their thinking, experience and solutions to develop freshperspectives and practical advice.
Our Global Pharmaceuticals and Life Sciences Industry Group has experience working with companies on industry-speci cstrategic, operational, and nancial issues. As well as assurance, tax and advisory services, we also have specialised capabilitiesin regulatory compliance, risk management, performance improvement and transaction support.
Simon Friend Partner, Global Pharmaceuticals and Life Sciences Industry Leader
[email protected][44] 20 7213 4875
Dr. Steve Arlington Partner, Global Pharmaceuticals and Life Sciences Advisory Services Leader
[email protected][44] 20 7804 3997
Michael Swanick Partner, Global Pharmaceuticals and Life SciencesTax Leader PwC (US)
[email protected][1] 267 330 6060
Attila Karacsony Director, US Pharmaceuticals and Life Sciences Marketing
[email protected][1] 973 236 5640
Marina Bello ValcarceGlobal Pharmaceuticals and Life Sciences Marketingand Knowledge Management
[email protected][44] 20 7212 8642
This publication has been prepared for general guidance o n matters of interest only, and does not constitute professional advice. You should not act upon theinformation contained in this publication without obtaining specic p rofessional advice. No representation or warranty (express or implied) is given as to theaccuracy or completeness of the information contained in this publication, and, to the extent permitted by law, PricewaterhouseCoopers does not accept or assumeany liability, responsibility or duty of care for any consequences of you or anyone else acting, or refraining to act, in reliance on the information contained in this
publication or for any decision based on it. 2011 PwC. All rights reserved. Not for further distribution without the permission of PwC. PwC refers to the network of member rms ofPricewaterhouseCoopers International Limited (PwCIL), or, as the context requires, individual member rms of the PwC network. E ach member rm is a separatelegal entity and does not act as agent of PwCIL or any other member rm. PwCIL does not provide any services to clients. PwCIL is not responsible or liable for theacts or omissions of any of its member rms nor can it control the exercise of their professional judgment or bind them in any way. No member rm is responsible orliable for the acts or omissions of any other member rm nor can it control the exercise of another member rms professional judgment or bind another memberrm or PwCIL in any way.
www.pwc.com/pharma