Intravenous thrombolysis with rt pa for acute ischemic stroke within 24 hrs of a ait
6
Intravenous thrombolysis with rt-PA for acute ischemic stroke within 24 h of a transient ischemic attack Piotr Sobolewski a, ⁎, Waldemar Brola b , Małgorzata Wiszniewska c , Wiktor Szczuchniak a , Małgorzata Fudala b , Mariusz Domagalski c , Monika Śledzińska-Dźwigał a a Department of Neurology and Stroke Unit, Holy Spirit Specialist Hospital in Sandomierz, Sandomierz, Poland b Department of Neurology and Stroke Unit, Saint Luke's Hospital in Końskie, Końskie, Poland c Department of Neurology and Stroke Unit, Hospital in Piła, Piła, Poland abstract article info Article history: Received 2 December 2013 Received in revised form 19 January 2014 Accepted 20 February 2014 Available online 26 February 2014 Keywords: Transient ischemic attack Acute ischemic stroke rt-PA iv-thrombolysis Safety Efficacy Background: Intravenous thrombolysis (iv-thrombolysis) with the use of rt-PA in patients after recent transient ischemic attack (TIA) is an important clinical problem. The aim of the study was to assess the impact of TIA within 24 h preceding acute ischemic stroke (AIS) on the safety and efficacy of iv-thrombolysis. Methods: We retrospectively evaluated the clinical and demographic data of 400 patients with AIS who were consecutively treated with iv-thrombolysis from September 2006 to May 2011 in three stroke centers. Results: At three-month follow-up, 58.0% of patients were independent (modified Rankin scale; mRS 0–2), 17.8% had died, 17.0% suffered hemorrhagic transformation (HT) and 4.3% experienced symptom- atic intracerebral hemorrhage (SICH). There were 29 patients (7.3%) who had a previous ipsilateral TIA within 24 h before established stroke. In the TIA subgroup, there was no significant higher percentage of favorable outcome (p = 0.07) and higher SICH rate (p = 0.15). Multivariate analysis showed the impact of prior TIA within 24 h before stroke onset in the presence of SICH (p = 0.01), no impact of TIA on unfavorable outcomes after three months (p = 0.25) and on the mortality rate within three months (p = 0.41). Conclusion: TIA within 24 h prior to ischemic stroke can portend severe intracerebral bleeding in patients qualified to iv-thrombolysis with the use of rt-PA. © 2014 The Authors. Published by Elsevier B.V. 1. Introduction Transient ischemic attacks (TIAs) are brief episodes of neurological dysfunction resulting from cerebral ischemia not associated with permanent cerebral infarction. The traditional definition of TIA on the basis of a temporal criterion needs revision since almost one-third of patients with transitory symptoms within the 24 h threshold have had a new related infarction, as assessed by diffusion-weighted magnetic resonance imaging (DW-MRI) [1,2]. As endorsed by 2009 guidelines from the American Heart Association and American Stroke Association (AHA/ASA), transient ischemic attack (TIA) is defined as a transient episode of neurologic dysfunction caused by focal brain, spinal cord, or retinal ischemia, without acute infarction [3]. Precise estimates of the incidence and prevalence of TIAs are difficult to determine, mainly be- cause of the varying criteria used in epidemiological studies to identify TIA. TIAs have been shown to be a strong predictor of subsequent stroke and death [4]. The risk of stroke after a TIA has been estimated at 14.6% within three months of observation, and the risk of TIA/stroke/death is 25.2% [5]. The history of an established TIA within the previous three months is not a formal contraindication for intravenous thrombolysis. However, TIA could influence outcome after iv-thrombolysis, because some patients may have, invisible in the CT scans, ischemic lesions and intra- cerebral microbleeds. Only a few studies have assessed the impact of prior TIA on the long- term outcome and safety of iv-thrombolysis in patients with acute ischemic stroke. Limitations of these studies are: the relatively small groups of patients with a history of TIA and performing only computed tomography (CT) imagings as a rule [6,7]. This also applies to our study. We also had to base our analysis on data from an interview from patients or their guardians, and only in some cases were we able to observe a TIA in our stroke units. The objective of the present study was to assess the impact of TIA within 24 h preceding an acute ischemic stroke (AIS) on the safety and efficacy of intravenous thrombolytic therapy. Journal of the Neurological Sciences 340 (2014) 44–49 ⁎ Corresponding author at: Department of Neurology and Stroke Unit, Holy Spirit Specialist Hospital in Sandomierz, 13 Schinzla Str., 27-600 Sandomierz, Poland. Tel.: +48 608510991, +48 158330650; fax: +48 158330593. E-mail address: [email protected] (P. Sobolewski). http://dx.doi.org/10.1016/j.jns.2014.02.022 0022-510X © 2014 The Authors. Published by Elsevier B.V. Contents lists available at ScienceDirect Journal of the Neurological Sciences journal homepage: www.elsevier.com/locate/jns Open access under CC BY-NC-ND license. Open access under CC BY-NC-ND license.
-
Upload
javier-pacheco-paternina -
Category
Health & Medicine
-
view
68 -
download
3
Transcript of Intravenous thrombolysis with rt pa for acute ischemic stroke within 24 hrs of a ait

Journal of the Neurological Sciences 340 (2014) 44–49
Contents lists available at ScienceDirect
Journal of the Neurological Sciences
j ourna l homepage: www.e lsev ie r .com/ locate / jns
Intravenous thrombolysis with rt-PA for acute ischemic stroke within 24h of a transient ischemic attack
Piotr Sobolewski a,⁎, Waldemar Brola b, Małgorzata Wiszniewska c, Wiktor Szczuchniak a, Małgorzata Fudala b,Mariusz Domagalski c, Monika Śledzińska-Dźwigał aa Department of Neurology and Stroke Unit, Holy Spirit Specialist Hospital in Sandomierz, Sandomierz, Polandb Department of Neurology and Stroke Unit, Saint Luke's Hospital in Końskie, Końskie, Polandc Department of Neurology and Stroke Unit, Hospital in Piła, Piła, Poland
⁎ Corresponding author at: Department of NeurologSpecialist Hospital in Sandomierz, 13 Schinzla Str.,Tel.: +48 608510991, +48 158330650; fax: +48 15
E-mail address: [email protected] (P. So
http://dx.doi.org/10.1016/j.jns.2014.02.0220022-510X © 2014 The Authors. Published by Elsevier B.V
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 2 December 2013Received in revised form 19 January 2014Accepted 20 February 2014Available online 26 February 2014Keywords:Transient ischemic attackAcute ischemic strokert-PAiv-thrombolysisSafetyEfficacy
Background: Intravenous thrombolysis (iv-thrombolysis) with the use of rt-PA in patients after recent transientischemic attack (TIA) is an important clinical problem. The aimof the studywas to assess the impact of TIAwithin24 h preceding acute ischemic stroke (AIS) on the safety and efficacy of iv-thrombolysis.Methods:We retrospectively evaluated the clinical and demographic data of 400 patients with AIS whowereconsecutively treated with iv-thrombolysis from September 2006 to May 2011 in three stroke centers.Results: At three-month follow-up, 58.0% of patients were independent (modified Rankin scale; mRS0–2), 17.8% had died, 17.0% suffered hemorrhagic transformation (HT) and 4.3% experienced symptom-atic intracerebral hemorrhage (SICH). There were 29 patients (7.3%) who had a previous ipsilateral TIAwithin 24 h before established stroke. In the TIA subgroup, there was no significant higher percentageof favorable outcome (p = 0.07) and higher SICH rate (p = 0.15). Multivariate analysis showed theimpact of prior TIA within 24 h before stroke onset in the presence of SICH (p = 0.01), no impact ofTIA on unfavorable outcomes after three months (p = 0.25) and on the mortality rate within three months
(p = 0.41).Conclusion: TIA within 24 h prior to ischemic stroke can portend severe intracerebral bleeding in patientsqualified to iv-thrombolysis with the use of rt-PA.© 2014 The Authors. Published by Elsevier B.V. Open access under CC BY-NC-ND license.
1. Introduction
Transient ischemic attacks (TIAs) are brief episodes of neurologicaldysfunction resulting from cerebral ischemia not associated withpermanent cerebral infarction. The traditional definition of TIA on thebasis of a temporal criterion needs revision since almost one-third ofpatients with transitory symptoms within the 24 h threshold have hada new related infarction, as assessed by diffusion-weighted magneticresonance imaging (DW-MRI) [1,2]. As endorsed by 2009 guidelinesfrom the American Heart Association and American Stroke Association(AHA/ASA), transient ischemic attack (TIA) is defined as a transientepisode of neurologic dysfunction caused by focal brain, spinal cord, orretinal ischemia, without acute infarction [3]. Precise estimates of theincidence and prevalence of TIAs are difficult to determine, mainly be-cause of the varying criteria used in epidemiological studies to identify
y and Stroke Unit, Holy Spirit27-600 Sandomierz, Poland.8330593.bolewski).
. Open access under CC BY-NC-ND lic
TIA. TIAs have been shown to be a strong predictor of subsequent strokeand death [4]. The risk of stroke after a TIA has been estimated at 14.6%within three months of observation, and the risk of TIA/stroke/death is25.2% [5].
The history of an established TIAwithin the previous threemonths isnot a formal contraindication for intravenous thrombolysis. However,TIA could influence outcome after iv-thrombolysis, because somepatients may have, invisible in the CT scans, ischemic lesions and intra-cerebral microbleeds.
Only a few studies have assessed the impact of prior TIA on the long-term outcome and safety of iv-thrombolysis in patients with acuteischemic stroke. Limitations of these studies are: the relatively smallgroups of patients with a history of TIA and performing only computedtomography (CT) imagings as a rule [6,7]. This also applies to our study.We also had to base our analysis on data from an interview frompatients or their guardians, and only in some cases were we able toobserve a TIA in our stroke units.
The objective of the present study was to assess the impact of TIAwithin 24 h preceding an acute ischemic stroke (AIS) on the safetyand efficacy of intravenous thrombolytic therapy.
ense.

45P. Sobolewski et al. / Journal of the Neurological Sciences 340 (2014) 44–49
2. Material and methods
2.1. Patient population
We retrospectively evaluated the clinical and epidemiological dataof 400 Caucasian patients with acute ischemic strokewhowere consec-utively treated with iv-thrombolysis from September 2006 to May2011 in three experienced stroke centers in Poland (the Departmentof Neurology and the Stroke Unit of the Hospital in Sandomierz, theDepartment of Neurology and Stroke Unit of the Hospital in Końskieand the Department of Neurology and the Stroke Unit of the Hospitalin Piła). These study centers are recognized as stroke units accordingto the Polish national criteria and are equipped with the proper moni-toring and diagnostic facilities [8] and provided a 24-hour stroke service7 days a week.
2.2. Protocol
Participating stroke units share common, periodically updatedprotocols for the management of acute ischemic stroke and secondaryprevention, according to international recommendations [9]. To collectthe data a pre-specified database was used. All patients were examinedat the time of admission by a stroke physician, and the severity of strokesymptoms was assessed using the National Institutes of Health StrokeScale (NIHSS) [10]. Stroke onset was defined as the last occasionon which the patient was known to be without neurological deficit.Exams to evaluate the coagulation status in all the patients were per-formed. CT scans were performed upon admission to hospital in orderto establish the indication for treatment, between 22 and 36 h and onthe seventh day after iv-thrombolysis. Intravenous rt-PA was appliedaccording to the recommendations for thrombolytic treatment. Sincethe publication of the European Cooperative Acute Stroke Study(ECASS) III trial and data from the Safe Implementation of Thrombolysisin Stroke (SITS) registry, patients have been treatedwithin the 4.5-hourtimewindow [11–13]. In patients, to evaluate the etiology of stroke andto determine secondary prevention transcranial Doppler (TCD), carotidduplex ultrasonography, Holter electrocardiography (Holter ECG),transthoracic echocardiography (TTE) and in the case of some patientstransesophageal echocardiography (TEE) was performed.
The 90-day stroke outcomes were measured using the modifiedRankin scale (mRS) [14]. A favorable outcome was defined as an mRSscore ≤2 points, while an unfavorable outcome was defined as an mRSscore of 3–6 points. The 90 daymRSwas obtained by clinic or home visits.Hemorrhagic transformation (HT) and symptomatic intra-cerebral hem-orrhage (SICH) rates were assessed according to the European Coopera-tive Acute Stroke Study (ECASS) II criteria. Radiographically, in ECASS IIprotocol HT was classified into hemorrhagic infarction (petechial in-farction without space occupying effect) and parenchymal hematoma(hemorrhage with mass effect); clinically, SICH was defined as an intra-cranial hemorrhage if the patient had clinical deterioration causing anincrease in the NIHSS score by 4 points, and if the hemorrhage was likelyto be the cause of the clinical deterioration [15].
All included patients were specifically interviewed by a neurologistfor symptoms of TIA suffered within 24 h prior to recruitment, or weobserved incidents of TIA during hospitalization in our stroke unitsprior to thrombolytic therapy. When patients were not able to givethe sought-after information, the relatives or medical records providedthe data. TIA was defined on a clinical basis as a documented transientfocal neurological deficit lasting b24 h. Due to the limited availabilityofMRI in routine practice, only patientswith performedCTwere includ-ed in this study. All patients had complete resolution of the neurologicsymptoms of TIA before the acute ischemic stroke. Clinical symptoms,number of TIA events suffered, the time from TIA to definite symptomonset and duration of episodes were recorded. Only cases in whichpatients had a documented normal neurological examination afterepisode of TIA were included. Patients who qualified for thrombolytic
therapy had symptoms for at least 30 min without a significant im-provement before treatment. In patients whowere admitted to the hos-pital due to TIA antiplatelet or anticoagulant therapy was implementedor continued according to the indications.
All patients treated with iv-thrombolysis in our stroke units werereported to the SITS registry.
The ethics committee approved all data analyses (Ethics Committeeof Świętokrzyska Medical Chamber). Each patient, or in case of his/herinability, two physicians, signed the standardized consent form in re-spect of the Ethical Principles for Medical Research involving humansubjects approved in Helsinki in 1964 by World Medical Association.
2.3. Statistical analysis
This study was based on a retrospective data analysis. Data gath-ering and characteristics and univariate analysis were performedusing Microsoft Excel 2010. Logistic regression was performed withSTATISTICA v. 9.1. All continuous variables were tested for a normaldistribution and equality of variances. Because of the non-normality ofthe variables, non-parametricMann–Whitney U tests were used to per-form the univariate analysis of the continuous variables. Categoricaldatawere compared using chi square tests. p values b0.05were consid-ered statistically significant. The multivariate analysis was performedusing multiple logistic regression. Factors identified on univariate anal-ysis with a p value b0.1 were then examined using a multivariatemodel. In the analysis, age and sex were also included. The results ofthe logistic regression models were presented as odds ratios (ORs)and the corresponding 95% confidence intervals (CIs).
3. Results
In the analyzed group, there were 400 patients with acute ischemicstroke treatedwith iv-thrombolysis (54.5%male; aged 41–92;mean age69.6 ± 11.8). Median onset to treatment time was 160 min (range135–180 min). After three months of follow-up, 58.0% of patientswere independent (mRS 0–2), 17.8% had died, 17.0% had suffered HTand 4.3% had experienced SICH according to the ECASS II definition.Baseline characteristics, onset to treatment time, stroke severity, thedistributions of risk factors, previous treatments, laboratory findings,and radiological findings in CT scans at baseline and functional out-comes after the months in TIA and non-TIA patients are shown inTable 1.
There were 29 patients (7.3%) who had a previous ipsilateral TIAwithin 24 h before established stroke. Most of the patients (n = 22;75.9%) had a single episode of TIA, while seven patients (24.1%) hadmore than one episode. The time interval between the first TIA episodeand the time of stroke onset ranged from 60 to 1320minwith amedianduration of 369 min (range 160–720). The median duration of TIA was45 min (range 4–300). All patients had ipsilateral TIA compared to thestroke signs.
The groups of patients with prior TIAwithin 24 h before stroke onsetand without TIA did not differ according to the presence of most vascu-lar risk factors, onset to treatment time, laboratory and radiologicalfindings at baseline. Coronary heart disease and the use of pre-strokeantiplatelet drugs were more frequent in the group of patients withoutprior TIA. Median arterial pressure (MAP), diastolic and systolic bloodpressure at the time of admission were higher in group of patientswith prior TIA. The NIHSS score at the time of admission was lowerin patients with prior TIA (p = 0.04). 41% of patients with history ofTIA prior to iv-thrombolysis were treated with antiplatelet agents and24% — with anticoagulants (all patients had INR b1.7).
In the TIA subgroup, there was no significant higher percentage offavorable outcome (p = 0.07) and higher SICH rate according to theECASS definition (p = 0.15) (Table 1).
Multivariate analysis showed the impact of prior TIA within 24 hbefore stroke onset in the presence of SICH (p = 0.01), no impact of

Table 1The clinical characteristics of the subgroups of thrombolytic patients without and with history of TIA within 24 h before stroke onset.
No prior TIA Prior TIA within 24 h p value
n (%) 371 (92.8) 29 (7.2) –
Demographic dataMean age (±SD) 69.7 ± 11.9 67.7 ± 10.2 0.26Male gender, n (%) 202 (54.5) 16 (55.2) 0.55
Risk factors, n (%)Hypertension 244 (65.8) 20 (69.0) 0.73Coronary heart disease 190 (51.2) 9 (31.0) 0.04Atrial fibrillation 132 (35.6) 7 (24.1) 0.21Diabetes mellitus 55 (14.8) 8 (27.6) 0.12Dyslipidemia 255 (68.7) 24 (82.8) 0.11Smoking 79 (21.3) 9 (31.0) 0.22Pre-stroke antiplatelets 224 (60.4) 12 (41.4) 0.045Pre-stroke anticoagulants 45 (12.1) 7 (24.1) 0.06
OCSP classification, n (%)TACI (Total Anterior Circulation Infarct) 116(31.3) 10(34.5) 0.72PACI (Partial Anterior Circulation Infarct) 183(49.3) 10(34.5) 0.12LACI (Lacunar Infarct) 68(18.3) 7(24.1) 0.44POCI (Posterior Circulation Infarct) 4(1.1) 2(6.9) 0.09
Etiological classification, n (%)Large vessel disease 132 (35.6) 14 (48.3) 0.17Cardioembolism 125(33.7) 9(24.1) 0.29Lacunar stroke 43(11.6) 5(17.2) 0.55Undetermined etiology 72(19.4) 3(10.3) 0.23
Stroke severity, median NIHSS (pts.) (IQR) 11.0 (8.0–16.0) 8.0 (6.0–14.0) 0.04Onset to treatment time (min) (IQR) 160(135.0–180.0) 160.0 (135.0–190.0) 0.93Median arterial blood pressure before thrombolysis (mm Hg) (IQR)MAP 108.0 (99.7–117.7) 113.3 (104.7–123.7) 0.02Diastolic 85.0 (80.0–95.0) 90.0 (85.0–100.0) 0.01Systolic 155.0 (140.0–170.0) 165.0 (150.0–175.0) 0.04
Laboratory findings before thrombolysisMedian INR (IQR) 1,05 (1.0–1.1) 1.03 (1.0–1.1) 0.36Median glucose level, mmol/l (IQR) 6.4 (5.6–7.6) 6.2 (5.6–8.4) 0.77Median creatinine level, μmol/l (IQR) 88.4 (73.4–101.7) 86.1 (69.8–97.0) 0.68
Radiological findings in CT scans at baseline, n (%)Old ischemic changes 132 (36.1) 12 (41.4) 0.57Early ischemic changes 89 (24.0) 10 (34.5) 0.21
mRS 0–2 at three months, n (%) 211 (56.9) 21 (72.5) 0.07Hemorrhagic transformation (HT)a, n (%) 63 (17.0) 5 (17.2) 0.63SICHa, n (%) 13 (3.5) 4 (13.8) 0.15Mortality, n (%) 67 (18.1) 4 (13.8) 0.56
mRS—modifiedRankin scale,MAP—median arterial pressure, NIHSS—National Institutes of Health Stroke Scale, ECASS— European Cooperative Acute Stroke Study, SICH— symptomaticintracerebral hemorrhage, SD— standard deviation, IQR — interquartile range (Q1–Q3), CT— computed tomography, OCSP — Oxford Community Stroke Project, and pts.— points.
a According to the ECASS II criteria.
46 P. Sobolewski et al. / Journal of the Neurological Sciences 340 (2014) 44–49
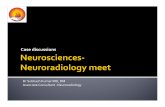
TIA on unfavorable outcomes after three months (p = 0.25) and onthe mortality rate within three months (p = 0.41). In the multivariateregression, lower NIHSS scores were associated with good out-comes (p b 0.0001) and higher NIHSS scores were associated withSICH (p = 0.02) and mortality (p b 0.0001). The analysis did notshow the impact of prior to stroke treatment with antiplatelet agentsor anticoagulants on the incidence of SICH in the TIA subgroup(Fig. 1).
4. Discussion
Our analyses showed the impact of prior TIA within 24 h beforestroke onset in the presence of SICH, no impact of TIA on unfavorableoutcomes after three months and on the mortality rate within threemonths in a population-based cohort of 400 Caucasian patients withAIS.
The reported prevalence of prior TIA in patients presenting withAIS ranges from 7% to 40% [3,16,17]. The effectiveness and safety ofsystemic cerebral thrombolysis in patients with previous TIA have notbeen clearly determined to date. Some studies have previously broughtup the safety and efficacy of thrombolytic therapy in such patients. We
Fig. 1.Multivariate logistic regression analysis. Odds ratio (OR) and95% CI for (a) independence, (ipsilateral TIA.
did notfind any study that assessed the impact of TIAwithin 24 h beforestroke on the efficacy of intravenous thrombolytic therapy.
de Leciñana et al. conducted an observational study from a prospec-tive registry of all AIS patients treated between 2003 and 2009 in Spain.There were 60 patients (6.8%)who had a previous ipsilateral TIAwithinonemonth prior to the current stroke; 71.6% of the patients had a singleepisode of TIA before an established stroke, while 28.4% had two ormore than two episodes. 65% of TIA episodes occurred during the pre-ceding 24 h [6].
Patients with previous TIA in our sample were older but fewer wereseverely affected at onset than those reported in the series in the obser-vational study by de Leciñana et al. We also included patients N80 yearsof age in our series. Both in the group of patients from Spain aswell as inour group, there were no statistically significant differences betweenthe subgroups of patients with a history of TIA and without TIA regard-ing long-term outcomes and mortality.
The most feared complication in acute ischemic stroke is symptom-atic HT [18]. Blood–brain barrier (BBB) breakdown resulting from ische-mia before reperfusion therapy is hypothesized to contribute to HTin AIS patients [19]. Following an acute ischemic stroke the integrityof the BBB may be compromised by the ischemic insult to the vascular
b)mortality, and (c) symptomatic intracranial hemorrhage (SICH) associatedwith previous

47P. Sobolewski et al. / Journal of the Neurological Sciences 340 (2014) 44–49

48 P. Sobolewski et al. / Journal of the Neurological Sciences 340 (2014) 44–49
endothelium, multiple signaling molecules and mediators have beenidentified with respect to how rt-PA treatment may lead from BBBbreakdown to HT. Even a relatively short period of ischemia will resultin markedly increased vascular permeability [20–22]. Some studiesshowed, that the risk of bleeding complications increased in patientswith more protracted symptoms duration and DWI lesion volume[2,3,23,24], but there have not been any prospective studies of thisproblem.
We found a SICH rate of 13.8% (according to the ECASS definition) inpatients with TIA preceding acute ischemic stroke who were treatedwith thrombolysis. The SICH rate was higher and the mortality ratewas similar to that reported in previous clinical trials of thrombolysisfor acute ischemic stroke [11,15,25] and a thrombolytic therapy registry[26,27]. The impact of prior TIA within 24 h before stroke onset in thepresence of SICHwas confirmed inmultivariate analysis. Increased inci-dence of intracerebral bleeding complication in our study sample can beexplained in two ways. First of all, our patients with a history of TIAwere older (mean age 68) than in similar studies (63) [6,7]. Older agehas been shown to be an important risk factor for SICH in some studies[15,28–31]. In addition, in these patients we found significantly higherdiastolic and systolic blood pressure, which also could increase the inci-dence of SICH [32].
McKinney et al. analyzed 23 patientswith acute ischemic strokewhoreceived thrombolytic therapy within seven days of a documented TIAand monitored the incidence of SICH. However, the group of patientswas not homogeneous. The authors also included in the analysispatients treated with intra-arterial thrombolysis (IA-thrombolysis) andcombination therapy: thrombolysis and mechanical thrombectomy.They found a SICH rate (according to the NINDS definition) of 8.6% ofpatients with TIA preceding AIS who were treated with thrombolysis.In patients who received IA-thrombolysis or mechanical therapy, therewere higher rates of SICH than in patients treated with iv-thrombolysisalone [7].
Although data collection was done in a prospective fashion, the ret-rospective nature of our data may be considered as a limitation of ourstudy, which has, therefore, inferior value than prospective and ran-domized trial. Also, the small number of patients with TIA before strokeand performing only CT imagings as a rule could be considered a limita-tion of our study.
Imaging studies have challenged the simplistic assumption thatbecause clinical TIA symptoms are resolved, significant ischemic tissueinjury does not occur. Several studies have shown that many patientsmeeting the clinical criteria for TIA demonstrate neuroanatomicallyrelevant infarcts on neuroimaging, which contributed to a change inthe definition of TIA. MRI has the potential to improve the accuracy ofTIA diagnosis. The pooled analysis of 808 patients from 10 centers dem-onstrated that restricted diffusion lesions were present in 33% [33]. Thecombination of early DW-MR and perfusion-weighted MRI (PW-MR)can document the presence of a cerebral ischemic lesion in approxi-mately half of all patients who present with a suspected hemispherictransient ischemic attack (TIA). This refers mostly to patients withneurological dysfunction that lasted more than 15 min. Hence, someconcernsmight exist regarding the risk of bleeding as a result of throm-bolytic therapy in these patients [34]. The risk of secondary SICHmay beincreased after thrombolytic therapy in AIS patients who have cerebralmicrobleeds on T2*-weighted magnetic resonance imaging [35]. There-fore, MRI is becoming the standard in diagnosis of patients with TIA andin making decision on the thrombolytic therapy in these patients.
In conclusion, our data suggest that iv-thrombolysis with the use ofrt-PA in patientswith AIS after recent TIA does not appear to havemajorinfluence on long-term outcomes. In patients with TIAwithin 24 h priorto a stroke, severe intracerebral bleeding may occur more frequently.However, our pre-stroke TIA group of patients had significantly lowerbaseline stroke severity and the frequency of pre-stroke anticoagulationwas higher in the prior TIA group. We believe that our findings providecertain values to the assessment of the safety and efficacy of treatment
with rt-PA in this group of patients. In the future, a prospective con-trolled study with the use of DW-MR would determine this importantclinical problem.
Disclosure of conflicts of interest
The authors declare that they have no conflicts of interest.
References
[1] Albers GW, Caplan LR, Easton JD, Fayad PB,Mohr JP, Saver JL, et al. Transient ischemicattack— proposal for a new definition. N Engl J Med 2002;347:1713–6.
[2] Lamy C, Oppenheim C, Calvet D, Domigo V, Naggara O, Méder JL, et al. Diffusion-weighted MR imaging in transient ischaemic attacks. Eur Radiol 2006;16:1090–5.
[3] Easton JD, Saver JL, Albers GW, Alberts MJ, Chaturvedi S, Feldmann E, et al. Definitionand evaluation of transient ischemic attack: a scientific statement for healthcareprofessionals from the American Heart Association/American Stroke AssociationStroke Council; Council on Cardiovascular Surgery and Anesthesia; Council onCardiovascular Radiology and Intervention; Council on Cardiovascular Nursing;and the Interdisciplinary Council on Peripheral Vascular Disease. The AmericanAcademy of Neurology affirms the value of this statement as an educational toolfor neurologists. Stroke 2009;40:2276–93.
[4] Hill MD, Yiannakoulias N, Jeerakathil T, Tu JV, Svenson LW, Schopflocher DP. Thehigh risk of stroke immediately after transient ischemic attack: a population-basedstudy. Neurology 2004;62:2015–20.
[5] Kleindorfer D, Panagos P, Pancioli A, Khoury J, Kissela B, Woo D, et al. Incidence andshort-term prognosis of transient ischemic attack in a population-based study.Stroke 2005;36:720–3.
[6] de LeciñanaMA, Fuentes B,Masjuan J, Simal P, Díaz-Otero F, Reig G, et al. Thrombolytictherapy for acute ischemic stroke after recent transient ischemic attack. Int J Stroke2012;7:213–8.
[7] McKinney JS,Masjuan J, Purroy F, Calvet D, AyH, Cucchiara BL. Safety of thrombolytictherapy for acute ischemic stroke after recent transient ischemic attack. J StrokeCerebrovasc Dis 2012;21:551–4.
[8] Członkowska A, Sarzynska-Długosz I, Niewada M, Kobayashi A. Eligibility of strokeunits in Poland for administration of intravenous thrombolysis. Eur J Neurol2006;13:220–4.
[9] Adams HP, del Zoppo G, Alberts MJ, Bhatt DL, Brass L, Furlan A, et al. Guidelines forthe early management of adults with ischemic stroke: a guideline from theAmerican Heart Association/American Stroke Association Stroke Council, ClinicalCardiology Council, Cardiovascular Radiology and Intervention Council, and theAtherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes inResearch Interdisciplinary Working Groups: the American Academy of Neurologyaffirms the value of this guideline as an educational tool for neurologists. Circulation2007;38:1655–711.
[10] Lyden P, Brott T, Tilley B,Welch KM, Mascha EJ, Levine S, et al. Improved reliability ofthe NIH Stroke Scale using video training. NINDS TPA Stroke Study Group. Stroke1994;25:2220–6.
[11] HackeW, Kaste M, Bluhmki E, BrozmanM, Dávalos A, Guidetti D, et al. Thrombolysiswith alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 2008;359:1317–29.
[12] Wahlgren N, Ahmed N, Dávalos A, Hacke W, Millán M, Muir K, et al. Thrombolysiswith alteplase 3–4.5 h after acute ischaemic stroke (SITS-ISTR): an observationalstudy. Lancet 2008;372:1303–9.
[13] Del Zoppo GJ, Saver JL, Jauch EC, Adams HP. Expansion of the time window fortreatment of acute ischemic stroke with intravenous tissue plasminogen activator:a science advisory from the American Heart Association/American Stroke Association.Stroke 2009;40:2945-8.
[14] Bonita R, Beaglehole R. Recovery of motor function after stroke. Stroke 1988;19:1497–500.
[15] Hacke W, Kaste M, Fieschi C, von Kummer R, Davalos A, Meier D, et al. Randomiseddouble-blind placebo-controlled trial of thrombolytic therapy with intravenousalteplase in acute ischaemic stroke (ECASS II). Second European–AustralasianAcute Stroke Study Investigators. Lancet 1998;352:1245–51.
[16] Sitzer M, Foerch C, Neumann-Haefelin T, Steinmetz H, Misselwitz B, Kugler C, et al.Transient ischaemic attack preceding anterior circulation infarction is independentlyassociated with favourable outcome. J Neurol Neurosurg Psychiatry 2004;75:659–60.
[17] Wegener S, Gottschalk B, Jovanovic V, Knab R, Fiebach JB, Schellinger PD, et al.Transient ischemic attacks before ischemic stroke: preconditioning the humanbrain? A multicenter magnetic resonance imaging study. Stroke 2004;35:616–21.
[18] Berger C, Fiorelli M, Steiner T, Schäbitz W-R, Bozzao L, Bluhmki E, et al. Hemorrhagictransformation of ischemic brain tissue: asymptomatic or symptomatic? Stroke2001;32:1330–5.
[19] Lin K, Kazmi KS, Law M, Babb J, Peccerelli N, Pramanik BK. Measuring elevatedmicrovascular permeability and predicting hemorrhagic transformation in acuteischemic stroke using first-pass dynamic perfusion CT imaging. Am J Neuroradiol2007;28:1292–8.
[20] Bisdas S, Hartel M, Cheong LH, Koht S. Detection of early vessel leakiness in acuteischemic stroke using computed tomography perfusion may indicate hemorrhagictransformation. Acta Radiol 2007;48:341–4.

49P. Sobolewski et al. / Journal of the Neurological Sciences 340 (2014) 44–49
[21] Lampl Y, Shmuilovich O, Lockman J, SadehM, LorberboymM. Prognostic significanceof blood brain barrier permeability in acute hemorrhagic stroke. Cerebrovasc Dis2005;20:433–7.
[22] Ewing JR, Knight RA, Nagaraja TN, Yee J, Nagesh V, Whitton P, et al. Patlak plots ofGd-DTPA MRI data yield blood–brain Transfer constants concordant with those of14C-sucrose in areas of blood–brain opening. Magn Reson Med 2003;50:283–92.
[23] Coutts SB, Simon JE, EliasziwM, Sohn CH, Hill MD, Barber PA, et al. Triaging transientischemic attack and minor stroke patients using acute magnetic resonance imaging.Ann Neurol 2005;57:848–54.
[24] Selim M, Fink JN, Kumar S, Caplan LR, Horkan C, Chen Y, et al. Predictors of hemor-rhagic transformation after intravenous recombinant tissue plasminogen activator:prognostic value of the initial apparent diffusion coefficient and diffusion-weightedlesion volume. Stroke 2002;33:2047–52.
[25] The National Institute of Neurological Disorders and Stroke rt-PA Stroke StudyGroup. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med1995;333:1581–7.
[26] Strbian D, Sairanen T, Meretoja A, Pitkäniemi J, Putaala J, Salonen O, et al. Patientoutcomes from symptomatic intracerebral hemorrhage after stroke thrombolysis.Neurology 2011;77:341–8.
[27] Wahlgren N, Ahmed N, Dávalos A, Ford GA, Grond M, Hacke W, et al. Thrombolysiswith alteplase for acute ischaemic stroke in the Safe Implementation of Thrombolysisin Stroke-Monitoring Study (SITS-MOST): an observational study. Lancet 2007;369:275–82.
[28] Fiorelli M, Bastianello S, von Kummer R, del Zoppo GJ, Larrue V, Lesaffre E, et al.Hemorrhagic transformation within 36 hours of a cerebral infarct: relationshipswith early clinical deterioration and 3-month outcome in the European CooperativeAcute Stroke Study I (ECASS I) cohort. Stroke 1999;30:2280–4.
[29] Thomalla G, Sobesky J, Kohrmann M, Fiebach JB, Fiehler J, Zaro Weber O, et al. Twotales: hemorrhagic transformation but not parenchymal hemorrhage after throm-bolysis is related to severity and duration of ischemia: MRI study of acute strokepatients treated with intravenous tissue plasminogen activator within 6 hours.Stroke 2007;38:313–8.
[30] Bluhmki E, Chamorro A, Dávalos A, Machnig T, Sauce C, Wahlgren N, et al. Stroketreatment with alteplase given 3.0–4.5 h after onset of acute ischaemic stroke(ECASS III): additional outcomes and subgroup analysis of a randomised controlledtrial. Lancet Neurol 2009;12:1095–102.
[31] Wahlgren N, Ahmed N, Errikson N, Aichner F, Bluhmki E, Dávalos A, et al. Multivar-iable analysis of outcome predictors and adjustment of main outcome results tobaseline data profile in randomized controlled trials: Safe Implementation of Throm-bolysis in Stroke-Monitoring Study (SITS-MOST). Stroke 2008;39:3316–22.
[32] Engelter ST, Reichhart M, Sekoranja L, Georgiadis D, Baumann A, Weder B, et al.Thrombolysis in stroke patients aged 80 years and older: Swiss survey of IV throm-bolysis. Neurology 2005;65:1795–8.
[33] Shah SH, Saver JL, Kidwell CS, Lansberg MG, Eyngorn I, Kemp S, et al. A multicenterpooled, patient-level data analysis of diffusion-weighted MRI in TIA patients. Stroke2007;38:463.
[34] Mlynash M, Olivot JM, Tong DC, Derex L, Gass A, Hjort N, et al. Yield of combinedperfusion and diffusion MR imaging in hemispheric TIA. Neurology 2009;72:1127–33.
[35] Fiehler J, Albers GW, Boulanger JM, Derex L, Gass A, Hjort N, et al. Bleeding riskanalysis in stroke imaging before thrombolysis (BRASIL): pooled analysis ofT2*-weighted magnetic resonance imaging data from 570 patients. Stroke 2007;38:2738–44.