Intratumoral STING Activation with T-cell Checkpoint ... · Research Article Intratumoral STING...
10
Research Article Intratumoral STING Activation with T-cell Checkpoint Modulation Generates Systemic Antitumor Immunity Casey R. Ager 1,2 , Matthew J. Reilley 3 , Courtney Nicholas 2 , Todd Bartkowiak 1,2 , Ashvin R. Jaiswal 1,2 , and Michael A. Curran 1,2 Abstract Coordinated manipulation of independent immune regulatory pathways in the tumor microenvironment—including blockade of T-cell checkpoint receptors and reversal of suppressive myeloid programs—can render aggressive cancers susceptible to immune rejection. Elevated toxicity associated with combination immu- notherapy, however, prevents translation of the most efficacious regimens. We evaluated T-cell checkpoint–modulating antibodies targeting CTLA-4, PD-1, and 4-1BB together with myeloid agonists targeting either STING or Flt3 in the TRAMP-C2 model of prostate cancer to determine whether low-dose intra- tumoral delivery of these agents could elicit systemic control of multifocal disease. Intratumoral administration of the STING agonist cyclic di-GMP (CDG) or Flt3 Ligand (Flt3L) augmented the therapeutic effect of systemic triple checkpoint modulation and promoted the cure of 75% of mice with bilateral TRAMP-C2; however, when all agents were administered locally, only CDG mobilized abscopal immunity. Combination efficacy correlated with globally enhanced ratios of CD8 þ T cells to regulatory T cells (Treg), macrophages, and myeloid-derived suppressor cells, and downregulation of the M2 marker CD206 on tumor-associated macrophages. Flt3L improved CD8 þ T-cell and dendritic cell infiltration of tumors, but was diminished in efficacy by concom- itant Treg expansion. Although intratumoral CDG/checkpoint therapy invokes substantial ulceration at the injection site, reduced CDG dosing can preserve tissue integrity without sacrificing therapeutic benefit. For high-order combinations of T-cell checkpoint antibodies and local myeloid agonists, systemic antibody administration provides the greatest efficacy; however, local administration of CDG and antibody provides substantial systemic benefit while minimizing the potential for immune-related adverse events. Cancer Immunol Res; 5(8); 676–84. Ó2017 AACR. Introduction Therapeutic blockade of T-cell coinhibitory receptors CTL- associated antigen 4 (CTLA-4) and programmed death 1 (PD-1) is sufficient to promote durable immune-mediated tumor regres- sion across multiple cancers in mouse and man. Neither ipilimu- mab (anti–CTLA-4) nor nivolumab (anti–PD-1), however, pro- vide clinical benefit in the setting of castration-resistant prostate cancer (CRPC; refs. 1, 2). Prostate cancer is the second leading cause of cancer-related death in men, and patients with CRPC have a median overall survival of 14 months, highlighting the urgent need for alternative immunotherapeutic approaches for this disease (3). Preclinical models of prostate cancer, including the transgenic adenocarcinoma of the mouse prostate (TRAMP) mouse and its derivative TRAMP-C2 implantable cell line (4), reveal two major barriers to antitumor immunity in CRPC: (i) poor CD8 þ T-cell infiltration into the prostate tumor microenvi- ronment (TME) and (ii) robust infiltration of immunosuppres- sive myeloid populations including tumor-associated macro- phages (TAM) and myeloid-derived suppressor cells (MDSC). Given the well-described means by which TAM and MDSC impede T-cell infiltration and effector function independent of the CTLA-4/PD-1 axes (5), therapies which deplete or biologically reprogram TAM and MDSC may render the prostate TME ame- nable to T-cell activity. Absent these barriers to T-cell infiltration and function, we hypothesize that CRPC patients would be likely to experience durable benefit from T-cell checkpoint blockade. In this study, we pursued a rational approach to design and evaluate multimodal therapies for CRPC consisting of antagonis- tic antibodies targeting T-cell coinhibitory receptors CTLA-4 and PD-1, agonistic antibodies targeting the T-cell costimulatory receptor 4-1BB, and agonistic molecules targeting myeloid acti- vation pathways including stimulator of interferon induced genes (STING) or FMS-like tyrosine kinase 3 (Flt3). Our lab previously established synergistic relationships between anti–CTLA-4 and anti–PD-1 antibodies, owing to their nonredundant roles in regulating central T-cell priming and peripheral effector function (6). These data preceded successful phase III trials and subsequent FDA approval of this combination in patients with metastatic melanoma (7, 8). In addition, we described complimentary effects of CTLA-4 blockade with concomitant ligation of the stimulatory receptor 4-1BB, which promotes CD8 þ T-cell survival, proliferation, and TH1 cytokine production (9). In each setting, 1 Immunology Program, University of Texas Graduate School of Biomedical Sciences at Houston, Houston, Texas. 2 Department of Immunology, University of Texas MD Anderson Cancer Center, Houston, Texas. 3 Division of Cancer Medicine, University of Texas MD Anderson Cancer Center, Houston, Texas. Note: Supplementary data for this article are available at Cancer Immunology Research Online (http://cancerimmunolres.aacrjournals.org/). Corresponding Author: Michael A. Curran, The University of Texas MD Anderson Cancer Center, 1515 Holcombe Blvd, Unit 0901, Houston, TX 77030. Phone: 713- 563-3286; Fax: 713-563-3276; E-mail: [email protected] doi: 10.1158/2326-6066.CIR-17-0049 Ó2017 American Association for Cancer Research. Cancer Immunology Research Cancer Immunol Res; 5(8) August 2017 676 on April 1, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from Published OnlineFirst July 3, 2017; DOI: 10.1158/2326-6066.CIR-17-0049
Transcript of Intratumoral STING Activation with T-cell Checkpoint ... · Research Article Intratumoral STING...

Research Article
Intratumoral STING Activation with T-cellCheckpoint Modulation Generates SystemicAntitumor ImmunityCasey R. Ager1,2, Matthew J. Reilley3, Courtney Nicholas2, Todd Bartkowiak1,2,Ashvin R. Jaiswal1,2, and Michael A. Curran1,2
Abstract
Coordinatedmanipulationof independent immune regulatorypathways in the tumor microenvironment—including blockadeof T-cell checkpoint receptors and reversal of suppressivemyeloidprograms—can render aggressive cancers susceptible to immunerejection. Elevated toxicity associated with combination immu-notherapy, however, prevents translation of the most efficaciousregimens.We evaluated T-cell checkpoint–modulating antibodiestargeting CTLA-4, PD-1, and 4-1BB together with myeloidagonists targeting either STING or Flt3 in the TRAMP-C2model of prostate cancer to determine whether low-dose intra-tumoral delivery of these agents could elicit systemic control ofmultifocal disease. Intratumoral administration of the STINGagonist cyclic di-GMP (CDG) or Flt3 Ligand (Flt3L) augmentedthe therapeutic effect of systemic triple checkpoint modulationand promoted the cure of 75% of mice with bilateral TRAMP-C2;however, when all agents were administered locally, only CDG
mobilized abscopal immunity. Combination efficacy correlatedwith globally enhanced ratios of CD8þ T cells to regulatory T cells(Treg), macrophages, and myeloid-derived suppressor cells, anddownregulation of the M2 marker CD206 on tumor-associatedmacrophages. Flt3L improved CD8þ T-cell and dendritic cellinfiltration of tumors, but was diminished in efficacy by concom-itant Treg expansion. Although intratumoral CDG/checkpointtherapy invokes substantial ulceration at the injection site,reduced CDG dosing can preserve tissue integrity withoutsacrificing therapeutic benefit. For high-order combinationsof T-cell checkpoint antibodies and local myeloid agonists,systemic antibody administration provides the greatestefficacy; however, local administration of CDG and antibodyprovides substantial systemic benefit while minimizing thepotential for immune-related adverse events. Cancer Immunol Res;5(8); 676–84. �2017 AACR.
IntroductionTherapeutic blockade of T-cell coinhibitory receptors CTL-
associated antigen 4 (CTLA-4) and programmed death 1 (PD-1)is sufficient to promote durable immune-mediated tumor regres-sion across multiple cancers in mouse and man. Neither ipilimu-mab (anti–CTLA-4) nor nivolumab (anti–PD-1), however, pro-vide clinical benefit in the setting of castration-resistant prostatecancer (CRPC; refs. 1, 2). Prostate cancer is the second leadingcause of cancer-related death in men, and patients with CRPChave a median overall survival of 14 months, highlighting theurgent need for alternative immunotherapeutic approaches forthis disease (3). Preclinical models of prostate cancer, includingthe transgenic adenocarcinoma of the mouse prostate (TRAMP)mouse and its derivative TRAMP-C2 implantable cell line (4),
reveal two major barriers to antitumor immunity in CRPC: (i)poor CD8þ T-cell infiltration into the prostate tumor microenvi-ronment (TME) and (ii) robust infiltration of immunosuppres-sive myeloid populations including tumor-associated macro-phages (TAM) and myeloid-derived suppressor cells (MDSC).Given the well-described means by which TAM and MDSCimpede T-cell infiltration and effector function independent ofthe CTLA-4/PD-1 axes (5), therapies which deplete or biologicallyreprogram TAM and MDSC may render the prostate TME ame-nable to T-cell activity. Absent these barriers to T-cell infiltrationand function, we hypothesize that CRPC patients would be likelyto experience durable benefit from T-cell checkpoint blockade.
In this study, we pursued a rational approach to design andevaluate multimodal therapies for CRPC consisting of antagonis-tic antibodies targeting T-cell coinhibitory receptors CTLA-4 andPD-1, agonistic antibodies targeting the T-cell costimulatoryreceptor 4-1BB, and agonistic molecules targeting myeloid acti-vation pathways including stimulator of interferon induced genes(STING) or FMS-like tyrosine kinase 3 (Flt3). Our lab previouslyestablished synergistic relationships between anti–CTLA-4 andanti–PD-1 antibodies, owing to their nonredundant roles inregulating central T-cell priming and peripheral effector function(6). These data preceded successful phase III trials and subsequentFDA approval of this combination in patients with metastaticmelanoma (7, 8). In addition, we described complimentaryeffects of CTLA-4 blockade with concomitant ligation of thestimulatory receptor 4-1BB,which promotes CD8þ T-cell survival,proliferation, and TH1 cytokine production (9). In each setting,
1Immunology Program, University of Texas Graduate School of BiomedicalSciences at Houston, Houston, Texas. 2Department of Immunology, Universityof Texas MD Anderson Cancer Center, Houston, Texas. 3Division of CancerMedicine, University of Texas MD Anderson Cancer Center, Houston, Texas.
Note: Supplementary data for this article are available at Cancer ImmunologyResearch Online (http://cancerimmunolres.aacrjournals.org/).
CorrespondingAuthor:Michael A. Curran, TheUniversity of TexasMDAndersonCancer Center, 1515 Holcombe Blvd, Unit 0901, Houston, TX 77030. Phone: 713-563-3286; Fax: 713-563-3276; E-mail: [email protected]
doi: 10.1158/2326-6066.CIR-17-0049
�2017 American Association for Cancer Research.
CancerImmunologyResearch
Cancer Immunol Res; 5(8) August 2017676
on April 1, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst July 3, 2017; DOI: 10.1158/2326-6066.CIR-17-0049

combination therapies were maximally effective in the context ofan irradiated cellular vaccine secreting Flt3-ligand (Flt3L). Knownfor its classical role in promoting survival, proliferation, anddifferentiation of hematopoietic progenitors, Flt3L can inducedendritic cell (DC) chemotaxis and conversion to aCD8aþCD103þ phenotype associated with cross-presentationand robust T-cell priming potential (10, 11). In contrast, Flt3Lalso promotes differentiation of plasmacytoid DCs, which canexert tolerogenic effects in cancer through induction of regulatoryT cells (Treg) and limit the efficacy of Flt3L as a cancer immuno-therapy (12).
The cytosolic nucleic acid sensor STING acts to promote tumor-specific T-cell responses by activating interferon secretion andcostimulatory ligand expression by myeloid cells after uptake oftumor cell–derived DNA and is indispensable for spontaneousrejection of immunogenic cancers (13). Cyclic dinucleotide ago-nists of STING activate macrophages and DC in vitro and havedemonstrated therapeutic utility alone and in combination withcheckpoint blockade across multiple tumor models (14, 15).
Using mice bearing bilaterally implanted TRAMP-C2 tumors,we found that intratumoral STING activation with the dinucle-otide cyclic di-GMP (CDG) mediates regression of injectedtumors, but fails to elicit systemic "abscopal" immunity targetingdistal lesions. Triple checkpoint modulation with anti–CTLA-4,anti–PD-1, and anti–4-1BB, however, converts intratumoral CDGinto a potentiator of systemic immunity capable of rejectingdistal, uninjected lesions. In contrast, intratumoral Flt3L aug-ments the benefit of triple checkpointmodulation, but onlywhenadministered locally at each lesion. Given the potential toxicity ofanti–CTLA-4, anti–PD-1, and anti–4-1BB combination therapy,we investigated whether intratumoral administration of thiscombination at low doses could serve as a safer alternative tosystemic antibody therapy. These studies demonstrate that cura-tive abscopal immunity can be generated against multifocalTRAMP-C2 when local triple checkpoint modulation is used incombination with intratumoral CDG. This therapeutic synergy isassociated with infiltration of tumor-specific T cells and enhancedratios of CD8þ T cells to Treg, MDSC, and TAM, as well aspronounced downregulation of the M2 macrophage markerCD206 on TAM. Alternatively, Flt3L failed to mobilize abscopalimmunity in combination with triple checkpoint modulation,likely due its expansion of CD4þ Teff and Treg populations withsimilar potency to CD8þ T cells at local and distal lesions. Weobserved dose-dependent skin pathology in mice receiving intra-tumoral CDG in combination with triple checkpoint blockade,although the therapeutic benefit of this combination appearsmodestly (but not significantly) dose-dependent. These datasupport the development of combinatorial strategies targetingadaptive and innate immune populations in prostate cancer, andinform the design of dosing strategies for STING agonists andcheckpoint modulators to maximize clinical benefit while min-imizing undue toxicity.
Materials and MethodsMice
Male C57BL/6 mice were obtained from The Jackson Labora-tory andwere housed according to the Association for Assessmentand Accreditation of Laboratory Animal Care and NIH standards.All experiments were conducted according to protocols approvedby the University of Texas MD Anderson Cancer Center Institu-
tional Animal Care andUseCommittee.Micewere approximately8 weeks old at the time of tumor implantation.
AntibodiesThe following therapeutic antibodies were obtained fromBio X
Cell and used in vivo at the indicated concentrations: anti–CTLA-4(9H10; 100 mg i.p. 50 mg i.t.), anti–PD-1 (RMP1-14; 250 mg i.p.50 mg i.t.), anti–4-1BB (3H3; 150 mg i.p. 50 mg i.t.). Antibodiesused for flow cytometry were obtained from Biolegend, BDBiosciences, eBioscience, and Fisher Scientific and are describedin Supplementary Table S1.
Myeloid agonistsSTING agonist c-di-GMP (CDG; Invivogen) was administered
i.t. at 25 mg per mouse. Flt3L-Ig (Flt3L; Bio X Cell) was admin-istered i.t. at 50 mg per mouse or 200 mg per mouse wheredescribed.
Cell linesThe TRAMP-C2 tumor cell line was provided by Dr. Norman
Greenberg, and all experiments in this article were performedusing passage 21-22 tumor cells. TRAMP-C2 cells were main-tained as previously described (4).
TRAMP-C2 implantation and treatmentAll mice were implanted at day 0 on both flanks with 1 � 106
TRAMP-C2 cells. For survival analysis experiments, mice weretreated on days 14, 18, and 22 i.p. (100 mL volume) and/or i.t.(50–100 mL volume) with the indicated antibodies and myeloidagonists. Tumor volumes were measured with calipers to definethe largest length (a), width (b), and height (c), and volumes werecalculated as (a x b x c).
Flow cytometry analysis of tumor immune infiltrateTRAMP-C2 cells (1 � 106) were mixed with 30% collagen
matrix (Matrigel, BD) and implanted at day 0 on both flanks.Mice received treatment when tumors reached approximately200 mm3 volume, on days 31, 35, and 39. On day 42, mice weresacrificed, tumors excised, and digested with collagenase H(Sigma) and DNAse (Roche), then live infiltrating immune cellswere purified by ficoll gradient centrifugation (Sigma; 1119density). Cells were then fixed and permeabilized (eBioscienceFoxP3 Fix/Perm kit), stained with fluorescently labeled antibo-dies, and analyzed by 18-color flow cytometry on a BD LSRII flowcytometer.
ResultsIntratumoral CDG potentiates systemic checkpointmodulation in TRAMP-C2
In both clinical and preclinical settings, prostate cancer remainsrefractory to checkpoint blockade therapy targeting CTLA-4 orPD-1. To identify combinatorial strategies capable of sensitizingprostate tumors to immunotherapy, we augmented our check-point blockade cocktail of antagonistic anti–CTLA-4 andanti–PD-1 antibodies with an agonistic antibody targeting 4-1BB,a costimulatory receptor of the Tumor Necrosis Factor Receptor(TNFR) superfamily which promotes CD8þ T-cell survival andcytotoxic effector function (16). We next investigated whetherintratumoral STING activation using the STING agonist c-di-GMP(CDG) can potentiate checkpoint modulation by promoting
Mobilizing Abscopal Immunity in Prostate Cancer
www.aacrjournals.org Cancer Immunol Res; 5(8) August 2017 677
on April 1, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst July 3, 2017; DOI: 10.1158/2326-6066.CIR-17-0049

in situ vaccine-like augmentation of T-cell priming and proin-flammatory reprogramming of the murine prostate tumor mye-loid compartment.Micewere challengedwith 1� 106 TRAMP-C2cells on both flanks, and received three doses of therapy every 4days beginning when tumors were palpable on day 14. Tumorgrowth and survival were monitored until tumors reached 1,000mm3 (Fig. 1A).We found that as a single agent, intratumoral CDGmediated rejection of essentially all locally injected tumors;however, CDG failed to elicit a systemic immune response capa-
ble of clearing distal, uninjected lesions (Fig. 1B–C; Supplemen-tary Fig. S2). Although systemic triple checkpoint modulationwith anti–CTLA-4, anti–PD-1, and anti–4-1BB demonstratedefficacy in this model, curing both bilateral tumors in 40% ofmice, we found that concurrent administration of CDG andimmunotherapeutic antibodies, even at a single lesion, inducedcomplete bilateral tumor rejection in approximately 75% ofmice(Fig. 1D). This revealed a therapeutic synergy between CDG andour antibody cocktail and demonstrated the abscopal potential of
Figure 1.
Local CDG potentiates i.p. checkpointmodulation against bilateral TRAMP-C2.A, Five to 8-week-old C57BL/6micewere challengedwith 1� 106 TRAMP-C2cells on both flanks andwere treated ondays 14, 18, and 22 after implantationwith i.p. checkpoint modulators and/orintratumoral (IT) CDG at either the right(R) or both right and left flank tumors (Rand L). B, Percentage of mice tumorfree at each flank, (C) tumor growthkinetics, and (D) overall survival overthe treatment period are shown. Micewere deemed moribund when tumorvolume reached 1,000 mm3. Data arecumulative of n ¼ 3 experiments with5 mice per group. Statisticalsignificance for survival was calculatedusing the Gehan–Breslow–Wilcoxontest. Ns, not significant; �, P < 0.05;�� , P < 0.01; ��� , P < 0.001;���� , P < 0.0001.
Figure 2.
Local Flt3L potentiates i.p. checkpointmodulation against bilateral TRAMP-C2. A, Five to eight-week-old C57BL/6mice were challenged with 1 � 106
TRAMP-C2 cells on both flanks andwere treated on days 14, 18, and 22 afterimplantation with i.p. checkpointmodulators and/or intratumoral (IT)Flt3L at either the right (R) or both rightand left flank tumors (R and L). B,Percentage of mice tumor free at eachflank, (C) tumor growth kinetics, and(D) overall survival over the treatmentperiod are shown. Mice were deemedmoribund when tumor volume reached1,000mm3.Data are cumulative of n¼ 3experiments with 5 mice per group.Statistical significance for survival wascalculated using the Gehan–Breslow–
Wilcoxon test. ns, not significant;� , P < 0.05; �� , P < 0.01; ��� , P < 0.001;���� , P < 0.0001.
Ager et al.
Cancer Immunol Res; 5(8) August 2017 Cancer Immunology Research678
on April 1, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst July 3, 2017; DOI: 10.1158/2326-6066.CIR-17-0049

CDG when combined with systemic checkpoint-modulatingtherapies.
Intratumoral Flt3L at each lesion potentiates systemiccheckpoint modulation in TRAMP-C2
Given our previous work combining checkpoint blockade withirradiated cellular vaccines secreting Flt3L (17), and the potentialfor Flt3L to act as a chemotactic and differentiation factor for DCs,we also chose to evaluate the capacity of intratumoral Flt3L topotentiate triple checkpoint modulation in our bilateral TRAMP-C2 model (Fig. 2A). In contrast to CDG, intratumoral Flt3Lexhibited modest local efficacy as a single agent, yet achievedcurative responses in approximately 15% of mice (Fig. 2B–D).Similar to CDG, Flt3L synergized with triple checkpoint modu-lation to cure 75% of mice in this model; however, this maximalresponse required intratumoral administration of Flt3L at eachtumor (Fig. 2D). Therefore, in optimal conditions, Flt3L andCDGwere capable of potentiating triple checkpoint modulation withsimilar efficacy, curing up to 75% of mice with multifocal, poorlyimmunogenic TRAMP-C2 tumors.When combinedwith systemiccheckpoint modulators, however, only the STING agonist mobi-lized abscopal immunity.
Intratumoral checkpoint modulation and CDG mobilizesabscopal immunity
In the clinic, individual checkpoint modulators can triggersevere, dose-limiting immune-related adverse events in manypatients (18). Colitis, pruritus, fatigue, and rash are toxicitiesassociatedwith anti–CTLA-4 and anti–PD-1. Agonistic antibodiestargeting 4-1BB are associated with rare instances of fatal hepa-totoxicity (19–21). Therefore, combinatorial strategies to targetCTLA-4, PD-1, and 4-1BBmust be suboptimally dosed or admin-istered in a manner that limits systemic toxicity while preservingtherapeutic potency. Based on a number of studies investigatingintratumoral administration of checkpoint modulators includinganti–CTLA-4 (22, 23), we asked whether intratumoral adminis-
tration of low-dose combination checkpoint modulation withanti–CTLA-4, anti–PD-1, and anti–4-1BB could prime local andsystemic immunity against bilateral TRAMP-C2, and whetherconcomitant local STING activation with CDG could furtherpotentiate these effects.
Mice bearing 14-day established bilateral TRAMP-C2 tumorsreceived three intratumoral injections of therapy only at the rightflank tumor 4 days apart (Fig. 3A). In this setting, intratumorallow-dose anti–CTLA-4, anti–PD-1, and anti–4-1BB mediatedregression of approximately 50% of injected tumors, but failedto engender systemic immunity against distal lesions (Fig. 3B–D;Supplementary Fig. S3). Concurrent administration of CDG aug-mented the abscopal potential of local checkpoint modulation,however, promoting abscopal regression of distal lesions andbilateral tumor rejection in up to 52% of mice. In this setting, wedid not observe a statistically significant dose-dependent increasein efficacy with additional CDG doses in potentiating localcheckpoint modulation (Fig. 3D). Thus, we conclude that oneormoredoses ofCDGcanenhance the curative abscopal potentialof intratumoral anti–CTLA-4, anti–PD-1, and anti–4-1BB againstbilateral TRAMP-C2.
Intratumoral combination therapy with CDG elicits skinpathology
In the course of the experiments described above, we observedan inflammatory reaction provoked at the injection site in micereceiving intratumoral administration of CDG togetherwith anti–CTLA-4, anti–PD-1, and anti–4-1BB. Within 2 days of the finaltherapeutic injection, we observed accumulation of dark, bloodyfluid in and around the tumor site that yielded to ulceration,scabbing, and eventual resolution after 2 to 3 weeks. This pathol-ogy required concomitant local administration of CDG andcheckpointmodulators, as no ulceration occurred followingCDGor checkpoint modulation therapy alone. This effect was dose-dependent with respect to the number of CDG doses, with mildinflammation and no ulceration observed in mice that received
Figure 3.
Intratumoral combination CDG andcheckpoint modulation mobilizesabscopal responses against distalTRAMP-C2. A, Five to 8-week-oldC57BL/6mice were challenged with 1�106 TRAMP-C2 cells on both flanks, andwere treated on days 14, 18, and 22 afterimplantation with intratumoral CDGand/or checkpoint modulators at theright flank tumor only. B, Percentage ofmice tumor free at each flank, (C) tumorgrowth kinetics, and (D) overall survivalover the treatment period areshown. Mice were deemed moribundwhen tumor volume reached 1,000mm3. Data are cumulative of n ¼ 3to 4 experiments with 5 to 10 mice pergroup. Statistical significance forsurvival was calculated using theGehan–Breslow–Wilcoxon test.Ns, not significant; � , P < 0.05;�� , P < 0.01; ��� , P < 0.001;���� , P < 0.0001.
Mobilizing Abscopal Immunity in Prostate Cancer
www.aacrjournals.org Cancer Immunol Res; 5(8) August 2017 679
on April 1, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst July 3, 2017; DOI: 10.1158/2326-6066.CIR-17-0049

one or twoCDGdoses (Fig. 4A). Tumor size at the time of therapymay also play a role in determining the extent of ulceration, asinjection of larger, 28-day established TRAMP-C2 tumors resultedin reduced ulceration generally localized to the tumor core and
not evident in the surrounding skin (Fig. 4B). Given that threeconcurrent doses of CDG with intratumoral anti–CTLA-4,anti–PD-1, and anti–4-1BB were associated with ulcerativepathology at the injection site yet delivered little survival benefit
Figure 4.
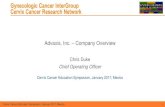
Intratumoral CDG with checkpoint modulationinvokes dose-dependent and tumor size-dependentulcerative pathology at the tumor site. A,Photographs of representative mice treated asdescribed in Fig. 3 were taken 6 days following finalintratumoral injection (day 28), when ulceration ismost intense, and 2 weeks later during the resolutionphase (day 42). B, Mice bearing either 14-day or 28-day established TRAMP-C2 tumors were given threeintratumoral injections of CDG with anti–CTLA-4,anti–PD-1, and anti–4-1BB every 4 days for a total ofthree injections, according to normal protocol.Photographs of ulceration were taken 2 (day 24) and6 (day 28) days following final intratumoral injection.
Figure 5.
Intratumoral combination Flt3L andcheckpoint modulation does notmobilize abscopal responses againstdistal TRAMP-C2. A, Five to 8-week-oldC57BL/6mice were challenged with 1�106 TRAMP-C2 cells on both flanks, andwere treated on days 14, 18, and 22 afterimplantation with intratumoral Flt3Land/or checkpoint modulators in theright flank only. B, Percent of micetumor free at each flank, (C) tumorgrowth kinetics, and (D) overall survivalover the treatment period are shown.Mice were deemed moribund whentumor volume reached 1,000mm3.Dataare cumulative of n ¼ 3 to 4experiments with 5 mice per group.Statistical significance for survivalwas calculated using the Gehan–Breslow–Wilcoxon test. ns, notsignificant; � , P < 0.05; �� , P < 0.01;��� , P < 0.001; ���� , P < 0.0001.
Ager et al.
Cancer Immunol Res; 5(8) August 2017 Cancer Immunology Research680
on April 1, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst July 3, 2017; DOI: 10.1158/2326-6066.CIR-17-0049

over one or two concurrent CDG doses (Fig. 3D), it may beprudent to limit STING agonist dosing in the combination settingin order to maximize therapeutic benefit while minimizingadverse event frequency and severity.
Flt3L with checkpoint modulation failed to generate abscopalimmunity
Using the treatment schedule described in Figure 5A, we eval-uated whether local Flt3L could mobilize abscopal immunityagainst TRAMP-C2 when combined with intratumoral triplecheckpoint modulation. In contrast to CDG, we found that Flt3Lfailed to synergizewith local checkpointmodulation inmediatingsystemic tumor immunity, delivering no survival benefit overanti–CTLA-4, anti–PD-1, and anti–4-1BB alone (Fig. 5B–D).Given the possibility that the therapeutic potency of our humanFlt3L-Ig protein could be limited by sub-optimal receptor bindingaffinity and generation of neutralizing antibodies, we tested asaturating dose of 200 mg per injection (Fig. 5B–D; Flt3L 3x"HIGH") and found that although local efficacy against theinjected tumor was increased, abscopal immunity failed toimprove. Of all mice treated, we noted that the incidence ofrelapse was higher in groups that received intratumoral Flt3Lcompared with groups treated with CDG, although the resultswere not statistically significant, and time to relapse was notdisparate between these groups (Supplementary Fig. S4).Although these data suggest that in situ vaccination with Flt3Lwas inferior to CDG in the context of checkpoint modulation, wewished to further confirm that this discrepancy was a generaliz-able phenomenon andnot dependent on tumor size at the timeofinjection. To address this, we asymmetrically implantedmicewithTRAMP-C2 to obtain 28-day established tumors (�200mm3) onthe right flank and 14-day established tumors (�20 mm3) on theleft flank before beginning local treatment (Supplementary Fig.S5A). Though the long engraftment period led to variability inboth tumor size at the right flank and engraftment efficiency ofdistal tumors by the time of treatment, we were able to observemore effective local control of large TRAMP-C2 tumors followingin situ delivery of combination checkpoint modulation and CDGin comparison to local checkpoint antibodies and Flt3L. Despitethe inferior regression of the injected lesion, Flt3L did show anequivalent capacity to 3xCDG to promote abscopal responsestargeting the smaller, uninjected tumor on the opposite flank(Supplementary Fig. S5B). Together, we conclude that CDG issuperior to Flt3L in potentiating local checkpoint modulation toinduce both local control and tomobilize abscopal effects againstTRAMP-C2 tumors.
STING/checkpoint therapy increased T-cell infiltration andreduced suppressive myeloid polarization
To further understand the biological mechanisms drivingresponse to intratumoral therapy at both injected and distalTRAMP-C2 tumors, as well as the differential capacity of CDGand Flt3L to potentiate local checkpoint modulation, we uti-lized 18-color flow cytometry to phenotype and functionallycharacterize the immune composition of bilateral TRAMP-C2tumors following intratumoral therapy. As local CDG injectionof 14-day established TRAMP-C2 mediates rapid, completeregression leaving minimal tumor tissue for analysis, weallowed tumors to establish for 31 days before initiatingtherapy, performing intratumoral injections on right flank
tumors on days 31, 35, and 39, and harvesting all tumors onday 42 (Supplementary Fig. S4).
At baseline, TRAMP-C2 tumors are dominated by a densemyeloid infiltrate consisting of CD11bþF4/80þGr-1� TAM andCD11bþGr-1þ MDSCs (Fig. 6B). T cells constitute only 5% of allCD45þ cells and are composed of roughly even proportions ofCD8þ cytolytic T lymphocytes (CTL), CD4þFoxP3� effector Tlymphocytes (Teff), and CD4þFoxP3þ Treg (Fig. 6C). Intratu-moral CDG administration enhanced CD8þ T-cell infiltrationof injected tumors and caused local accumulation ofCD11bþGr-1þF4/80neg granulocytes, likely indicating neutrophilinfiltration (Fig. 6D; Supplementary Fig. S7). In contrast, intra-tumoral Flt3L elicits increased CD11cþCD11b� DC accumula-tion, yet triggered expansion of Treg in both injected and unin-jected tumors (Fig. 6B and C). Intratumoral checkpoint modu-lation enhanced the proportion of T cells infiltrating TRAMP-C2tumors and diminished the Treg pool, likely through antibody-dependent cellular cytotoxic depletion of aCTLA-4–coated Treg(24). Concurrent administration of CDG and checkpoint-mod-ulating antibodies further enhanced CD8þ T-cell accumulation ateach tumor, resulting in favorable CD8:Treg ratios that weresuperior to those seen in response to combination therapy withFlt3L (Fig. 6E). Using tetramer staining to track the knownimmunodominant SPAS-1 neoepitope expressed in TRAMP-C2(25),we found that combination therapywithCDGenhanced thedensity of SPAS-reactive CD8þ T cells at the injected tumor andexhibited a trending capacity to mobilize these cells to the distaltumor, which was not observed in mice receiving Flt3L therapy(Fig. 6F). Local CDG synergized with checkpoint modulation toreduce the percentage of SPAS-specific T cells within the total poolof infiltrating CD8þ T cells, suggesting that this therapeuticapproach may diversify the T-cell receptor repertoire to moreeffectively target subdominant epitopes in addition to SPAS-1compared with checkpoint modulation alone or combinationtherapy with Flt3L (Fig. 6G). These data indicate a mechanisticbasis underlying the discrepancy in efficacy between local com-bination therapy incorporating CDG and Flt3L wherein CDGelicits numerous and diverse CD8þ T-cell responses againstinjected and uninjected tumors, whereas the efficacy of Flt3L islimited by the tendency to promote CD4þ T-cell responses.
The dense myeloid infiltrate characteristic of TRAMP-C2tumors poses a barrier to the function of infiltrating cytolytic Tcells. Even in this context, we found that local priming with3XCDG promoted improved CD8:TAM ratios relative to theuntreated animals (Fig. 6H). This was also evident for 1xCDGvs. Flt3L forCD8:MDSC ratios; however, these data for the 3xCDGgroup were confounded by the large neutrophil infiltration inresponse to the skin inflammation shown in Figure 4, and ourinability to distinguish these neutrophils from PMN-MDSC usingthe antibodies in our panel (Supplementary Fig. S7A). Overallthough, few, if any, tumors reached ratios at which CD8þ T cellsare expected to fully escape myeloid suppression. Therefore, wehypothesize that intratumoral delivery of myeloid agonists canreprogram tumor myeloid populations to reduce their immuno-suppressive activity, creating a microenvironment that is amena-ble to T-cell effector function despite unfavorable relative cellularratios. Supporting this hypothesis, we observed downregulationof theM2macrophagemarkerCD206onTAMin tumors receivingCDGconcurrentlywith all three doses of anti–CTLA-4, anti–PD-1,and anti–4-1BB, potentially indicating repolarization of TAM inresponse to CDG combined with checkpoint modulation
Mobilizing Abscopal Immunity in Prostate Cancer
www.aacrjournals.org Cancer Immunol Res; 5(8) August 2017 681
on April 1, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst July 3, 2017; DOI: 10.1158/2326-6066.CIR-17-0049

Figure 6.
Analysis of the TRAMP-C2 immune infiltrate at local and distal tumors following intratumoral therapy at a single lesion. A, To obtain cell numbers sufficient for flowanalysis, TRAMP-C2 tumors were established for 31 days, exposed to three doses of intratumoral therapy at the right flank, then were harvested for multiparameterflow cytometry as described in Materials and Methods. See Supplementary Materials for antibodies used and gating strategy. B, Relative proportions ofunique cell subsets within the CD45þ immune infiltrate, normalized to the total number of gated cells. C, Relative proportions of T-cell subsets within theCD3þ lymphocyte infiltrate, normalized to the total number of gated T cells. D, Relative proportions of MDSC subsets within the CD11bþGr-1þ immune infiltrate.E, Calculated ratios of CD8þ T cells to Treg, (F) density of SPAS-1 tetramerþ CD8þ T cells, (G) percentage of SPAS-1 reactive T cells within all infiltrating CD8 T cells,and ratio of CD8þ T cells to (H) macrophages are shown. I, Percentage of macrophages expressing the M2 macrophage marker CD206. Data are cumulativeof 2 independent experiments with 5 mice per group. Statistical significance was calculated using the Student t test. ns, not significant; � , P < 0.05; �� , P < 0.01;��� , P < 0.001; ���� , P < 0.0001.
Ager et al.
Cancer Immunol Res; 5(8) August 2017 Cancer Immunology Research682
on April 1, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst July 3, 2017; DOI: 10.1158/2326-6066.CIR-17-0049

(Fig. 6I). Although combination therapywith Flt3L promotedDCexpansion and a reduction in MDSC populations, Flt3L failed toinduce CD206 downregulation on TAM, suggesting this effect isspecific to CDG. We conclude, therefore, that relative to Flt3L,CDG better potentiates intratumoral anti–CTLA-4, anti–PD-1,and anti–4-1BB activity by increasing infiltration and diversifica-tion of tumor-specific CD8þ T cells at local and distal tumors,enhancing CD8:Treg ratios, and by reprogramming suppressiveTAM to a proinflammatory phenotype.
DiscussionSimultaneous manipulation of multiple, nonredundant
immune regulatory systems can activate potent antitumorimmune responses in mouse and man. Translation of thisapproach, however, has been limited by cumulative inflamma-tory side effects, which limit the tolerability of high-order com-bination therapies in patients. At the time of this writing, the onlycombination immunotherapy with FDA approval consists ofipilimumab (Yervoy; anti–CTLA-4) and nivolumab (Opdivo;anti–PD-1) for patients with Braf V600 wild-type unresectableor metastatic melanoma. Though effective and tolerable in thisindication, a number of solid tumors, including CRPC, remainresistant to these therapies. We report that an optimized cocktailof immunomodulators engaging both innate and adaptiveimmunity mediates efficient rejection of poorly immunogenicmurine prostate cancer. Although local stimulation of the STINGor Flt3 pathways can complement checkpoint-modulating anti-bodies targeting CTLA-4, PD-1, and 4-1BB to delay tumor growthand enhance survival of mice withmultifocal TRAMP-C2, we findthat the STING agonist CDGmobilizes abscopal immunity moreefficiently than Flt3L. In an effort to mitigate the toxicity of thesehigh-order combinations, we report that intratumoral injection oflow-dose checkpoint modulators together with CDG, but notFlt3L, is sufficient to induce curative abscopal immunity inapproximately 50% of mice. We identify a potential mechanisticbasis for the discrepancy in synergy between checkpoint mod-ulators and CDG vs. Flt3L, as CDG promotes CD8 skewing,infiltration of tumor-specific T cells, and enhanced intratumoralratios of CD8þ T cells to Treg, TAM, and MDSC, whereas Flt3Lfacilitates expansion of CD4 T cells, including Treg, in both localand distal tumors. Combination therapy with CDG may reducethe suppressive capacity of TAM in TRAMP-C2 tumors, as weobserve downregulation of theM2macrophagemarker CD206 inresponse to this therapy. These data suggest that STING-mediatedmyeloid programming can potentiate intratumoral T-cell check-pointmodulation to rendermultifocal prostate cancer sensitive toimmunotherapy.
Abscopal effects are the holy grail of intratumoral therapy.Although published reports describe regression of uninjectedlesions in response to local delivery of STING-activating cyclicdinucleotides (CDN), we find that single-agent CDG fails toelicit abscopal immunity against distal TRAMP-C2 tumors (15).This discrepancy may be related to the type of CDN used, asCDG binds with low affinity to STING yet can engage theinflammasome to promote IL1b production, unlike syntheticCDNs used in other studies (26). Furthermore, this may be aproduct of the TRAMP-C2 model resulting from genomic DNAbeing leaked into the cytoplasm to trigger low levels of chronicSTING signaling by this cell line (27). This, in turn, maypromote interferon-induced expression of PD-L1 and indolea-
mine 2,3-dioxygenase in the microenvironment that can act asbarriers to immune responses generated at distant sites. Ourresults suggest that the capacity for STING agonists alone toelicit abscopal effects is limited in certain indications. Never-theless, even in this context, we demonstrate that abscopalimmunity can be effectively mobilized when CDNs are admin-istered in combination with checkpoint modulation.
Although intratumoral therapy carries the benefit of minimiz-ing off-target toxicities common in patients receiving systemicimmunotherapy, overt inflammation at the injection site cancomplicate dosing strategies of locally administered agents. Weobserve an ulcerative response to intratumoral therapy in micereceiving combination CDG and anti–CTLA-4, anti–PD-1, andanti–4-1BB; delivery of CDG or checkpoint modulators alonedoes not elicit this pathology. Baird and colleagues have alsoreported intratumoral hemorrhagic necrosis in anumber of tumormodels upon local delivery of Rp, Rp dithio-CDG (RR-CDG) withradiotherapy, involving swelling and leakage of neovascularendothelium and stromally derived TNFa release (28). Weobserve accumulation of CD11bþGr-1þF4/80� granulocytes inthese tumors, suggesting inflammatory neutrophils may be con-tributing to ulceration, possibly through production of TNFa.Ulcerative pathology appears less extensive in larger tumors,although it is unknown whether this is due to the presence oflarger numbers of suppressive TAM andMDSC, vascular constric-tion due to stromal desmoplasia in advanced TRAMP tumors, orreduced bystander activation of cells in surrounding healthy skin.By reducing the number of CDG doses administered concurrentlywith checkpoint modulators, we observe reduction in local ulcer-ation without sacrificing therapeutic power as measured by distaltumor growth or overall survival. Therefore, we conclude thatcombination therapies incorporating STING agonists with intra-tumoral checkpoint modulators can promote localized tissuepathology, and that an optimal therapeutic indexmay be reachedby restricting CDN dosing.
High-order combinations of immunotherapies that engageboth innate and adaptive immunity have the potential to regresspreclinical models of aggressive, poorly immunogenic cancer, butcumulative inflammatory toxicities can impede translation ofthese therapies into patients. We evaluated a cocktail of T-cellcheckpoint–modulating antibodies targeting CTLA-4, PD-1, and4-1BB together with intratumoral innate agonists engaging eitherSTING or Flt3 in a poorly immunogenic model of multifocalmurine prostate cancer. In the context of systemic checkpointmodulation, intratumoral CDG or Flt3L deliver curativeresponses in the majority of mice; however, CDG proves to bethe best choice to augment intratumoral low-dose combinationcheckpoint blockade. Although this intratumoral combinationtherapy can induce injection site ulcerative pathology, limitingCDGdosing can sustain tissue integritywithout foregoing survivalbenefit, illuminating an avenuebywhichhigh-order combinationimmunotherapy can be delivered for systemic control of poorlyimmunogenic prostate cancer with reduced local and systemictoxicity.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
DisclaimerThe content is solely the responsibility of the authors and does not neces-
sarily represent the official views of the NIH.
Mobilizing Abscopal Immunity in Prostate Cancer
www.aacrjournals.org Cancer Immunol Res; 5(8) August 2017 683
on April 1, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst July 3, 2017; DOI: 10.1158/2326-6066.CIR-17-0049

Authors' ContributionsConception and design: C.R. Ager, M.A. CurranDevelopment of methodology: C.R. Ager, M.A. CurranAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): C.R. Ager, M.J. Reilley, C. Nicholas, T. Bartkowiak,A.R. JaiswalAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): C.R. Ager, M.J. Reilley, T. Bartkowiak, A.R. Jaiswal,M.A. CurranWriting, review, and/or revision of the manuscript: C.R. Ager, M.J. Reilley,T. Bartkowiak, M.A. CurranAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): C.R. Ager, C. NicholasStudy supervision: M.A. Curran
AcknowledgmentsThe authors would like to acknowledge the National Center for Advancing
Translational Sciences of the National Institutes of Health (award numbers
TL1TR000369 and UL1TR000371) and the American Legion Auxiliary forsupport during the completion of this study.
Grant SupportResearch reported in this article was supported by the National Center for
Advancing Translational Sciences of the National Institutes of Health underAward Numbers TL1TR000369 and UL1TR000371. This research was alsosupported by the University Cancer Foundation via the InstitutionalResearch Grant program at the University of Texas MD Anderson CancerCenter.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received January 27, 2017; revised May 7, 2017; accepted June 23, 2017;published OnlineFirst July 3, 2017.
References1. Kwon ED, Drake CG, Scher HI, Fizazi K, Bossi A, van den Eertwegh
AJM, et al. Ipilimumab versus placebo after radiotherapy in patientswith metastatic castration-resistant prostate cancer that had pro-gressed after docetaxel chemotherapy (CA184-043): a multicentre,randomised, double-blind, phase 3 trial. Lancet Oncol 2014;15:700–12.
2. Topalian SL,Hodi FS, Brahmer JR,Gettinger SN, SmithDC,McDermottDF,et al. Safety, activity, and immune correlates of anti–PD-1 antibody incancer. N Eng J Med 2012;366:2443–54.
3. RitchCR, CooksonMS. Advances in themanagement of castration resistantprostate cancer. BMJ 2016;355:i4405.
4. Foster BA, Gingrich JR, Kwon ED, Madias C, Greenberg NM. Charac-terization of prostatic epithelial cell lines derived from transgenicadenocarcinoma of the mouse prostate (TRAMP) model. Cancer Res1997;57:3325–30.
5. Gabrilovich DI, Ostrand-Rosenberg S, Bronte V. Coordinated regulation ofmyeloid cells by tumours. Nat Rev Immunol 2012;12:253–68.
6. Curran MA, Montalvo W, Yagita H, Allison JP. PD-1 and CTLA-4 combi-nation blockade expands infiltrating T cells and reduces regulatory T andmyeloid cells within B16 melanoma tumors. Proc Nat Acad Sci U S A2010;107:4275–80.
7. Wolchok JD, Kluger H, Callahan MK, Postow MA, Rizvi NA, Lesokhin AM,et al. Nivolumab plus ipilimumab in advanced melanoma. N Engl J Med2013;369:122–33.
8. Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Cowey CL, Lao CD, et al.Combined nivolumab and ipilimumab or monotherapy in untreatedmelanoma. N Engl J Med 2015.
9. Curran MA, Kim M, Montalvo W, Al-Shamkhani A, Allison JP. Combina-tion CTLA-4 blockade and 4-1BB activation enhances tumor rejection byincreasing T-cell infiltration, proliferation, and cytokine production. PLoSOne 2011;6:e19499.
10. Maraskovsky E, Brasel K, Teepe M, Roux ER, Lyman SD, Shortman K, et al.Dramatic increase in the numbers of functionally mature dendritic cells inFlt3 ligand-treatedmice: multiple dendritic cell subpopulations identified.J Exp Med 1996;184:1953–62.
11. Salmon H, Idoyaga J, Rahman A, Leboeuf M, Remark R, Jordan S, et al.Expansion and Activation of CD103(þ) dendritic cell progenitors at thetumor site enhances tumor responses to therapeutic PD-L1 and BRAFinhibition. Immunity 2016;44:924–38.
12. KleinO, Ebert LM, Zanker D,Woods K, Tan BS, Fucikova J, et al. Flt3 ligandexpands CD4þ FoxP3þ regulatory T cells in human subjects. Eur JImmunol 2013;43:533–9.
13. Woo SR, Fuertes MB, Corrales L, Spranger S, Furdyna MJ, Leung MY, et al.STING-dependent cytosolic DNA sensing mediates innate immune recog-nition of immunogenic tumors. Immunity 2014;41:830–42.
14. Fu J, Kanne DB, Leong M, Glickman LH, McWhirter SM, Lemmens E, et al.STING agonist formulated cancer vaccines can cure established tumorsresistant to PD-1 blockade. Sci Transl Med 2015;7:283ra52.
15. Corrales L, Glickman LH,McWhirter SM, KanneDB, Sivick KE, KatibahGE,et al. Direct activation of STING in the tumor microenvironment leads topotent and systemic tumor regression and immunity. Cell Rep 2015;11:1018–30.
16. Bartkowiak T, Curran MA. 4-1BB agonists: multi-potent potentiators oftumor immunity. Front Oncol 2015;5:117.
17. Curran MA, Allison JP. Tumor vaccines expressing Flt3 ligand synergizewith CTLA-4 blockade to reject preimplanted tumors. Cancer Res 2009;69:7747–55.
18. Boutros C, Tarhini A, Routier E, LambotteO, Ladurie FL, Carbonnel F, et al.Safety profiles of anti-CTLA-4 and anti-PD-1 antibodies alone and incombination. Nat Rev Clin Oncol 2016;13:473–86.
19. Segal NH, Logan TF, Hodi FS, McDermott DF, Melero I, Hamid O,et al. Results from an integrated safety analysis of urelumab, anagonist anti-CD137 monoclonal antibody. Clin Cancer Res 2016;23:1929–36.
20. Hodi FS,O'Day SJ,McDermott DF,Weber RW, Sosman JA,Haanen JB, et al.Improved survival with ipilimumab in patientswithmetastaticmelanoma.N Eng J Med 2010;363:711–23.
21. TopalianSL,Hodi FS, Brahmer JR,Gettinger SN, SmithDC,McDermottDF,et al. Safety, activity, and immune correlates of anti-PD-1 antibody incancer. N Eng J Med 2012;366:2443–54.
22. Fransen MF, van der Sluis TC, Ossendorp F, Arens R, Melief CJ. Controlledlocal delivery of CTLA-4 blocking antibody induces CD8þ T-cell-depen-dent tumor eradication and decreases risk of toxic side effects. Clin CancerRes 2013;19:5381–9.
23. Marabelle A, Kohrt H, Sagiv-Barfi I, Ajami B, Axtell RC, Zhou G, et al.Depleting tumor-specific Tregs at a single site eradicates disseminatedtumors. J Clin Invest 2013;123:2447–63.
24. Simpson TR, Li F, Montalvo-Ortiz W, Sepulveda MA, Bergerhoff K, Arce F,et al. Fc-dependent depletion of tumor-infiltrating regulatory T cells co-defines the efficacy of anti-CTLA-4 therapy against melanoma. J Exp Med2013;210:1695–710.
25. Fasso M, Waitz R, Hou Y, Rim T, Greenberg NM, Shastri N, et al. SPAS-1(stimulator of prostatic adenocarcinoma-specific T cells)/SH3GLB2: Aprostate tumor antigen identified by CTLA-4 blockade. Proc Natl Acad SciUSA 2008;105:3509–14.
26. Abdul-Sater AA, Tattoli I, Jin L,Grajkowski A, Levi A, Koller BH, et al. Cyclic-di-GMP and cyclic-di-AMP activate the NLRP3 inflammasome. EMBO Rep2013;14:900–6.
27. Ho SS, ZhangWY, Tan NY, Khatoo M, Suter MA, Tripathi S, et al. The DNAstructure-specific endonuclease MUS81 mediates DNA sensor STING-dependent host rejection of prostate cancer cells. Immunity 2016;44:1177–89.
28. Baird JR, Friedman D, Cottam B, Dubensky TW Jr., Kanne DB, BambinaS, et al. Radiotherapy combined with novel STING-targeting oligonu-cleotides results in regression of established tumors. Cancer Res 2016;76:50–61.
Cancer Immunol Res; 5(8) August 2017 Cancer Immunology Research684
Ager et al.
on April 1, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst July 3, 2017; DOI: 10.1158/2326-6066.CIR-17-0049

2017;5:676-684. Published OnlineFirst July 3, 2017.Cancer Immunol Res Casey R. Ager, Matthew J. Reilley, Courtney Nicholas, et al. Generates Systemic Antitumor ImmunityIntratumoral STING Activation with T-cell Checkpoint Modulation
Updated version
10.1158/2326-6066.CIR-17-0049doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerimmunolres.aacrjournals.org/content/suppl/2017/07/01/2326-6066.CIR-17-0049.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerimmunolres.aacrjournals.org/content/5/8/676.full#ref-list-1
This article cites 27 articles, 11 of which you can access for free at:
Citing articles
http://cancerimmunolres.aacrjournals.org/content/5/8/676.full#related-urls
This article has been cited by 6 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerimmunolres.aacrjournals.org/content/5/8/676To request permission to re-use all or part of this article, use this link
on April 1, 2020. © 2017 American Association for Cancer Research. cancerimmunolres.aacrjournals.org Downloaded from
Published OnlineFirst July 3, 2017; DOI: 10.1158/2326-6066.CIR-17-0049