Intrafractional Prostatic Fossa Motion in Biochemically Relapsed Prostate Cancer using a Rectal...
2
2879 Predicting Isocenter Shift due to Prostate Motion and Selecting Patient Specific Posterior Margin for IGRT in the External Beam Treatment of Prostate Cancer C. Cheng 1 , J. R. Wong 1 , S. Merrick 1 , B. Langley 2 , J. Z. Gao 1 1 Morristown Memorial Hospital, Morristown, NJ, 2 Stevens Institute of Technology, Hoboken, NJ Purpose/Objective(s): The motion of the prostate gland manifested as an isocenter shift (isoshift) in the left-right (LR), superior- inferior (SI) and anterio-posterior (AP) directions is a well known problem in prostate irradiation. Due to the apparent random na- ture of the motion, predicting the isoshift may seem to be futile. Thus IGRT of prostate cancer is generally performed for the whole treatment course, requiring significant resources. In this study, we present our clinical data to demonstrate the predictive nature of the isoshift, based on which a patient specific treatment margin can be determined with 95% confidence limit for more than 90% of the patients. Materials/Methods: A total of 2,670 isoshifts from 1,350 CT scans for 100 consecutive patients are reviewed and analyzed. IGRT for prostate irradiation is performed with a Siemens Primatom by image fusion of the Primatom CT images with the planning CT. In the first phase of treatment, each patient received 10-15 IGRT fractions. The isoshift is reviewed every 5 fractions and an ‘average’ isoshift is determined for patient setup for the next 5 IGRT fractions. After all 10-15 IGRT fractions had been delivered, a final isoshift and a patient specific posterior margin are determined for the second phase of irradiation. The accuracy of the isoshift is verified weekly by a CT scan (isocheck). To show the effect of the patient adjustment as a result of IGRT, the shift data for each patient is ‘un-shifted’ relative to the initial treatment isocenter. The frequency distributions (FD) of the ‘un-shifted’ and shifted data sets in the LR and AP directions are compared. The shift data from isochecks is also compared. Results: The FD of the un-shifted data in the LR and AP directions follow that of a normal distribution, indicating the random nature of the prostate motion. The normalized FD of the un-shifted data in the AP direction (mean = 0.18 mm, SD = 5.1 mm). The 2SD width (10 mm) coincides with the posterior margin traditionally used in 3D planning. The shifted data superimposed on the un-shifted curve also shows a normal distribution (mean = -0.12 mm, SD = 4.1 mm), validating an improvement in setup accuracy. Further improvement in setup accuracy is demonstrated in the isochecks (AP: mean = 0.28 mm, SD = 3.4 mm). The AP margin in the second phase of treatment is in the range 5-8 mm for 90% of patients. Conclusions: Despite the apparent random nature of prostate motion, we have used a simple method to predict the iso-shift and determine a specific margin to account for the prostate motion. The patient subgroup that lies outside of the 2SD range may indicate that a daily IGRT is needed for these patients. Author Disclosure: C. Cheng, None; J.R. Wong, None; S. Merrick, None; B. Langley, None; J.Z. Gao, None. 2880 IMRT Dose Reconstruction using Cone-beam CT and EPID-measured Leaf Sequence Files L. Xing, L. Lee, W. Mao Stanford University School of Medicine, Stanford, CA Purpose/Objective(s): Most of the dose reconstructions performed on cone-beam CT (CBCT) are based on planned fluence maps, tacitly assuming that they can be faithfully realized by the MLC delivery. This assumption might not be necessarily valid. For in- stance, in IMRT using step-and-shoot mode, the delivery is associated with intrinsic errors in the MLC kinematics and beam control communication resulting in overshoot, undershoot segmental monitor units, dropped segments, and leaf position deviations. There- fore, the use of delivered fluence maps in IMRT dose reconstruction warrants a more accurate evaluation of the delivered dose to a patient. The purpose of this work is to study the feasibility of retrospectively reconstructing the IMRT dose delivered to a prostate patient on the basis of on-treatment CBCT and fluence maps derived from the MLC segments captured by an amorphous silicon electronic portal imaging device (aSi-EPID) during the treatment. Materials/Methods: CBCT was performed on a pelvic phantom and a typical IMRT prostate plan was delivered to the phantom; EPID images at 6.7 frames per second were acquired for each field. An in-house program was developed to identify the different segmental images captured for each field and calculate, from the segmental image, the leaf end positions using a maximum gradient algorithm. For each segment, the corresponding fractional monitor unit (fMU) data was intercepted from the MLC workstation. Finally, for each field, a leaf sequence (LS) file was re-constituted using the segmental leaf positions and their associated fMU based on the sequence the segments were delivered. The EPID-measured LS files were loaded back to the treatment planning system to derive the delivered fluence maps. Dose reconstructions on the CBCT using the delivered and planned fluence maps, respectively, were performed and the dose distributions were compared. The geometric status of the EPDI, including the sag, tilt, and offsets for various gantry angles were established by a geometrical QA phantom, and the necessary corrections were incorporated in the cal- culation of the leaf end positions. Results: The feasibility of using EPID-measured LS files for dose reconstruction on CBCT has been studied. The dose distributions based on the delivered and planned fluence maps were slightly different in the high dose region; the maximum dose from the former distribution was 2.5% lower than that from the latter. Conclusions: IMRT dose reconstruction can be accomplished on the basis of (1) on-treatment CBCT that depicts the inter-frac- tional anatomic changes and (2) delivered fluence maps that include the delivery errors. This affords a valuable platform to imple- ment adaptive therapy, which requires the knowledge of actual delivered dose to targets and normal tissues, in the future. Author Disclosure: L. Xing, None; L. Lee, None; W. Mao, None. 2881 Intrafractional Prostatic Fossa Motion in Biochemically Relapsed Prostate Cancer using a Rectal Balloon J. A. Fortney, J. M. Watkins, D. T. Marshall Medical University of South Carolina, Charleston, SC Purpose/Objective(s): To describe intrafractional target motion in post-prostatectomy patients using a rectal balloon. Materials/Methods: Beginning in 2007, post-prostatectomy patients to receive salvage or adjuvant radiotherapy at the Medical University of South Carolina have been simulated with a rectal balloon filled with 60 cc of air. Early patients were evaluated using Proceedings of the 50th Annual ASTRO Meeting S563
Transcript of Intrafractional Prostatic Fossa Motion in Biochemically Relapsed Prostate Cancer using a Rectal...

Proceedings of the 50th Annual ASTRO Meeting S563
2879 Predicting Isocenter Shift due to Prostate Motion and Selecting Patient Specific Posterior Margin for IGRT
in the External Beam Treatment of Prostate CancerC. Cheng1, J. R. Wong1, S. Merrick1, B. Langley2, J. Z. Gao1
1Morristown Memorial Hospital, Morristown, NJ, 2Stevens Institute of Technology, Hoboken, NJ
Purpose/Objective(s): The motion of the prostate gland manifested as an isocenter shift (isoshift) in the left-right (LR), superior-inferior (SI) and anterio-posterior (AP) directions is a well known problem in prostate irradiation. Due to the apparent random na-ture of the motion, predicting the isoshift may seem to be futile. Thus IGRT of prostate cancer is generally performed for the wholetreatment course, requiring significant resources. In this study, we present our clinical data to demonstrate the predictive nature ofthe isoshift, based on which a patient specific treatment margin can be determined with 95% confidence limit for more than 90% ofthe patients.
Materials/Methods: A total of 2,670 isoshifts from 1,350 CT scans for 100 consecutive patients are reviewed and analyzed. IGRTfor prostate irradiation is performed with a Siemens Primatom by image fusion of the Primatom CT images with the planning CT. Inthe first phase of treatment, each patient received 10-15 IGRT fractions. The isoshift is reviewed every 5 fractions and an ‘average’isoshift is determined for patient setup for the next 5 IGRT fractions. After all 10-15 IGRT fractions had been delivered, a finalisoshift and a patient specific posterior margin are determined for the second phase of irradiation. The accuracy of the isoshiftis verified weekly by a CT scan (isocheck). To show the effect of the patient adjustment as a result of IGRT, the shift data foreach patient is ‘un-shifted’ relative to the initial treatment isocenter. The frequency distributions (FD) of the ‘un-shifted’ and shifteddata sets in the LR and AP directions are compared. The shift data from isochecks is also compared.
Results: The FD of the un-shifted data in the LR and AP directions follow that of a normal distribution, indicating the randomnature of the prostate motion. The normalized FD of the un-shifted data in the AP direction (mean = 0.18 mm, SD = 5.1 mm).The 2SD width (10 mm) coincides with the posterior margin traditionally used in 3D planning. The shifted data superimposedon the un-shifted curve also shows a normal distribution (mean = -0.12 mm, SD = 4.1 mm), validating an improvement in setupaccuracy. Further improvement in setup accuracy is demonstrated in the isochecks (AP: mean = 0.28 mm, SD = 3.4 mm). The APmargin in the second phase of treatment is in the range 5-8 mm for 90% of patients.
Conclusions: Despite the apparent random nature of prostate motion, we have used a simple method to predict the iso-shift anddetermine a specific margin to account for the prostate motion. The patient subgroup that lies outside of the 2SD range may indicatethat a daily IGRT is needed for these patients.
Author Disclosure: C. Cheng, None; J.R. Wong, None; S. Merrick, None; B. Langley, None; J.Z. Gao, None.
2880 IMRT Dose Reconstruction using Cone-beam CT and EPID-measured Leaf Sequence Files
L. Xing, L. Lee, W. Mao
Stanford University School of Medicine, Stanford, CA
Purpose/Objective(s): Most of the dose reconstructions performed on cone-beam CT (CBCT) are based on planned fluence maps,tacitly assuming that they can be faithfully realized by the MLC delivery. This assumption might not be necessarily valid. For in-stance, in IMRT using step-and-shoot mode, the delivery is associated with intrinsic errors in the MLC kinematics and beam controlcommunication resulting in overshoot, undershoot segmental monitor units, dropped segments, and leaf position deviations. There-fore, the use of delivered fluence maps in IMRT dose reconstruction warrants a more accurate evaluation of the delivered dose toa patient. The purpose of this work is to study the feasibility of retrospectively reconstructing the IMRT dose delivered to a prostatepatient on the basis of on-treatment CBCT and fluence maps derived from the MLC segments captured by an amorphous siliconelectronic portal imaging device (aSi-EPID) during the treatment.
Materials/Methods: CBCT was performed on a pelvic phantom and a typical IMRT prostate plan was delivered to the phantom;EPID images at 6.7 frames per second were acquired for each field. An in-house program was developed to identify the differentsegmental images captured for each field and calculate, from the segmental image, the leaf end positions using a maximum gradientalgorithm. For each segment, the corresponding fractional monitor unit (fMU) data was intercepted from the MLC workstation.Finally, for each field, a leaf sequence (LS) file was re-constituted using the segmental leaf positions and their associated fMU basedon the sequence the segments were delivered. The EPID-measured LS files were loaded back to the treatment planning system toderive the delivered fluence maps. Dose reconstructions on the CBCT using the delivered and planned fluence maps, respectively,were performed and the dose distributions were compared. The geometric status of the EPDI, including the sag, tilt, and offsets forvarious gantry angles were established by a geometrical QA phantom, and the necessary corrections were incorporated in the cal-culation of the leaf end positions.
Results: The feasibility of using EPID-measured LS files for dose reconstruction on CBCT has been studied. The dose distributionsbased on the delivered and planned fluence maps were slightly different in the high dose region; the maximum dose from the formerdistribution was 2.5% lower than that from the latter.
Conclusions: IMRT dose reconstruction can be accomplished on the basis of (1) on-treatment CBCT that depicts the inter-frac-tional anatomic changes and (2) delivered fluence maps that include the delivery errors. This affords a valuable platform to imple-ment adaptive therapy, which requires the knowledge of actual delivered dose to targets and normal tissues, in the future.
Author Disclosure: L. Xing, None; L. Lee, None; W. Mao, None.
2881 Intrafractional Prostatic Fossa Motion in Biochemically Relapsed Prostate Cancer using a Rectal Balloon
J. A. Fortney, J. M. Watkins, D. T. Marshall
Medical University of South Carolina, Charleston, SC
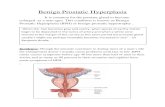
Purpose/Objective(s): To describe intrafractional target motion in post-prostatectomy patients using a rectal balloon.
Materials/Methods: Beginning in 2007, post-prostatectomy patients to receive salvage or adjuvant radiotherapy at the MedicalUniversity of South Carolina have been simulated with a rectal balloon filled with 60 cc of air. Early patients were evaluated using

S564 I. J. Radiation Oncology d Biology d Physics Volume 72, Number 1, Supplement, 2008
fluoroscopic imaging of surgical clips in order to measure maximum excursion in the anterior to posterior (A-P), superior to inferior(S-I) and lateral (L-R) dimensions. More recently, full breath-cycle 4D-CT is used to determine the maximum extent of motion ofsurgical clips in the prostatectomy bed. These measurements were used to create a patient-specific internal target volume (ITV)expansion for each patient. The initial two patients were simulated prone, while all patients since have been simulated supine.Data was prospectively recorded in a quality assurance database, from which the present analysis is being conducted after IRBapproval.
Results: Twenty-one patients were identified for inclusion in the present analysis and two patients were excluded due to lack ofmotion data. Two patients (10%) were simulated prone and 17 (90%) were simulated supine. Motion was measured using fluoros-copy on eleven patients (58%) and 4D-CT on eight (42%). The mean maximum excursion in the A-P dimension was 1.3 mm(range, 0-4, standard dev 1.16, 68% #1 mm), 1.4 mm in S-I (range, 0-4, std dev 1.21, 68% #1 mm), and 0.6 mm in L-R (range,0-2, std dev 0.61, 95% #1 mm). The two patients treated prone both showed A-P, S-I, and L-R motion of 4mm, 4mm, and 1mm,respectively. For supine patients, the mean A-P motion was 1.0mm (range, 0-2, std dev 0.71, 76% #1 mm), 1.1 mm S-I (range, 0-3,std dev 0.83, 76% #1 mm), and 0.5 mm L-R (range, 0-2, std dev 0.62, 94% #1 mm).
Conclusions: Potential advantages of a rectal balloon during radiotherapy for prostate cancer have been thoroughly described forpatients undergoing definitive radiotherapy, including improved reproducibility of daily set-up, positioning the posterior rectal walloutside of the high-dose field, dosimetric advantages of an air-tissue interface, and decreased target motion. For post-prostatectomypatients requiring adjuvant or salvage radiotherapy, intrafractional motion of the prostatic fossa during radiotherapy is minimalusing a rectal balloon with the patient in the supine position (#1 mm in A-P, S-I, and L-R dimensions in 76%, 76%, and 94%of patients, respectively).
Author Disclosure: J.A. Fortney, None; J.M. Watkins, None; D.T. Marshall, None.
2882 A Study of Daily Localization with 3D Ultrasound, Cone Beam CT and Implanted Fiducial Markers for
Patients undergoing IGRT for Prostate CancerT. Neicu, T. Nurushev, R. Hammoud, F. Martin, D. Pradhan, H. Stricker, B. Movsas, I. Chetty, M. Elshaikh
Henry Ford Health System, Detroit, MI
Purpose/Objective(s): To evaluate the use of three image-guided radiation therapy (IGRT) methods (3D ultrasound [U/S], conebeam CT [CBCT] and implanted markers) for prostate cancer patients being treated on a prospective IRB-approved protocol.
Materials/Methods: Patients are imaged using kV CBCT (Varian Medical Systems, Palo Alto CA), 3D U/S (Clarity, ResonantMedical Inc., Montreal, CN) and kV orthogonal images of implanted gold seed fiducial markers. The daily imaging protocol se-quence for each patient is as follows: CBCT, kV orthogonal X-rays, 3D U/S, perform patient shifts based on U/S (standard insti-tutional procedure), kV X-rays (post patient-shift), treat patient. Intramodality shifts are determined after performing rigid-bodyregistration of daily images and respective treatment planning (reference) images. Residual motion is assessed from differencesbetween kV images of marker positions performed prior to and after U/S-based shifts. On a weekly basis, an additional set ofCBCT, kV, and U/S images is acquired to evaluate prostate motion at another instance along the intra-fraction prostate motiontrajectory. To minimize variability in bladder and rectal filling, each patient is given a set of written instructions to ensure a fullbladder and an empty rectum during treatment. The intramodality shifts recorded were analyzed off-line. Prior to the start ofthe protocol, the entire localization procedure was validated with a custom-developed pelvic phantom which included implantedfiducial markers.
Results: For the phantom study, shifts determined by the 3 imaging modalities were found to be within 1 mm in all dimensions.Over a period of 13 fractions thus far, the prostate shifts (m ± s) are as follows:�8.9 ± 4.2 mm (A/P), 1.5 ± 2.4 mm (S/I) and�0.4 ±2.3 mm (L/R) for 3D U/S; -2.0 ± 1.2 mm (A/P), 2.1 ± 2.0 mm (S/I) and 1.5 ± 2.1 mm (L/R) for CBCT, and -5.1 ± 3.3 mm (A/P), 1.5± 2.0 mm (S/I) and 1.9 ± 2.1 mm (L/R) for kV images of marker positions. Residual motion of the prostate gland was found to be2.1 ± 6.0 mm (A/P), 0.5 ± 1.8 mm (S/I) and -0.1 ± 1.2 mm (L/R).
Conclusions: We have embarked on a prospective protocol to evaluate the use of CBCT, 3D U/S and kV images of implantedmarkers for IGRT-based treatment of prostate cancer. Uniquely, all 3 IGRT techniques are assessed within each individual patientundergoing daily localization of the prostate gland. A phantom study and preliminary patient results indicate that the protocol willbe beneficial in determining the tradeoffs of these different modalities and the underlying reasons for the differences observed. Theprotocol results, to be reported, will incorporate prospective data for a total of 30 patients, each treated over a course of 40 fractions.
(Supported in part by research funding from Resonant Medical Inc.)
Author Disclosure: T. Neicu, None; T. Nurushev, None; R. Hammoud, None; F. Martin, None; D. Pradhan, None; H. Stricker,None; B. Movsas, Resonant Medical Inc., B. Research Grant; I. Chetty, Resonant Medical Inc., B. Research Grant; M. Elshaikh,Resonant Medical Inc., B. Research Grant.
2883 4D CT Simulation for Prostate Cancer: Assessing Intrafraction Organ Motion for Image Guided IMRT
Treatment PlanningS. Sim1, J. Li1, M. Chan1, K. Schupak1, C. Burman1, B. Mueller2, D. M. Lovelock3, M. J. Zelefsky3
1Memorial Sloan-Kettering Cancer Center, Basking Ridge, NJ, 2Memorial Sloan-Kettering Cancer Center, Sleepy Hollow, NY,3Memorial Sloan-Kettering Cancer Center, New York, NY
Purpose/Objective(s): To utilize 4D CT simulation techniques to assess intrafraction organ motion for image-guided radiotherapy(IGRT) treatment planning in prostate cancer.
Materials/Methods: Twenty-six patients were simulated using a 4D approach (16 supine and 10 prone). Utilizing bellows on thechest to monitor respiratory cycle, 4D-CT simulation was performed. Patients were simulated with empty bladder and an evacuatedrectum. PTV was defined as an expansion of 1 cm throughout except posteriorly where a 6mm margin was utilized. All supinepatients had fiducial seed placement for purposes of IGRT. Respiratory motion was assessed in AP, sup-inf, and lateral directions