INTRACRANIAL SUPPURATION
7
POSTGRAD. MED. j. (I96I), 37, 534 INTRACRANIAL SUPPURATION LESLIE OLIVER, M.B.(LOND.), F.R.C.S., F.A.C.S. Neurosurgeon, Charing Cross Hospital, West London Hospital and Royal Northern Hospital, London ALTHOUGH the introduction of the sulphonamides and the antibiotics has reduced the incidence of intracranial suppuration, it can still cause con- siderable anxiety to the medical practitioner. Extradural Abscess An abscess may form between the skull and the dura mater as a complication of mastoiditis, osteomyelitis of the skull or fracture of the skull (open to the exterior, or into an infected mastoid process or nasal sinus). The dura mater forming the inner wall of the abscess is inflamed and usually covered with granulations corresponding to the extent of the abscess. there is severe toxemia and pyrexia. Localizing neurological signs are sometimes found and depend on the site of the abscess. Rarely, osteomyelitis, blood- borne or arising from an overlying carbuncle, affects the suboccipital region causing an extra- dural abscess with cerebellar signs. The cerebro- spinal fluid shows a moderate increase in white cells but contains no organisms; its pressure may be raised. When an extradural abscess is caused by osteo- myelitis or mastoiditis, the operation appropriate to these diseases establishes the necessary drainage. When, however, an extradural abscess follows fracture of the skull, a burr-hole is made over the site of the abscess and a drain inserted. Appropriate antibiotics are administered. Subdural Suppuration (The synonym purulent pachymeningitis is a bad term, for it equally well applies to extradural abscess which is associated with pachymeningitis secondary to overlying osteomyelitis.) Subdural empyema means a widespread collection of pus between the dura and arachnoid mater. It is an uncommon but serious condition which before the days of antibiotics was invariably fatal. The commonest cause is osteomyelitis of the skull following an acute exacerbation of inflammation of the nasal air sinuses. Such an exacerbation may be brought about by operative interference in sinusitis. Subdural infection may also be caused by blood-borne osteomyelitis of the skull, mastoiditis, or frac-tures of the skull which open to the exterior or into septic nasal sinuses or mastoid cells. Infected subdural effusions not infrequently complicate the convalescence in cases of acute purulent meningitis, especially in child- hood (Hankinson and Amador, 1956). There are severe toxemia and pyrexia, with signs of raised intracranial pressure (headache, vomiting and papilledema). The infection spreads widely in the subdural space producing contralateral hemi- paresis, cortical sensory loss and hemianopia. If the dominant cerebral hemisphere is affected, dysphasia or aphasia may be found. Patients sometimes present with grand mal or Jacksonian epilepsy. Subdural empyemas sometimes occur bilaterally. A subdural abscess is a localized collection- of pus; it may form during the treatment of sub- dural empyema, or the infection may be localized from the beginning. Subdural abscesses tend to form along the falx or between the occipital lobe and tentorium. A subdural abscess produces a localized neurological effect. Thus an abscess on the medial aspect of the hemisphere involving the motor cortex causes paralysis of the contra- lateral leg with sparing of the arm and face. Lumbar puncture in subdural infection shows raised pressure, and the cerebrospinal fluid con- tains an increased number of white cells (ioo to 300 per cu. mm.) but no organisms. Although a variety of organisms may be grown from the primary focus, the commonest one found in subdural pus is the non-h2emolytic streptococcus. Burr holes are made to confirm the diagnosis and to enable drainage to be carried out. In subdural empyema small rubber catheters are insinuated between the dura and arachnoid for the instillation of penicillin, to which the organisms of subdural infection are usually sensitive (Schiller, Cairns and Russell, 1948). The strength of penicillin employed is 500 units per ml. of isotonic saline. Although systemic penicillin passes into the subdural space, the greater concentration of the drug obtained by the catheter method is desirable. Subdural abscesses are located with the aid of a brain cannula which is passed unhesitatingly through relatively silent parts of the brain, but it is particularly important to avoid the motor cortex
Transcript of INTRACRANIAL SUPPURATION

POSTGRAD. MED. j. (I96I), 37, 534
INTRACRANIAL SUPPURATIONLESLIE OLIVER, M.B.(LOND.), F.R.C.S., F.A.C.S.
Neurosurgeon, Charing Cross Hospital, West London Hospital and Royal Northern Hospital, London
ALTHOUGH the introduction of the sulphonamidesand the antibiotics has reduced the incidence ofintracranial suppuration, it can still cause con-siderable anxiety to the medical practitioner.
Extradural AbscessAn abscess may form between the skull and
the dura mater as a complication of mastoiditis,osteomyelitis of the skull or fracture of the skull(open to the exterior, or into an infected mastoidprocess or nasal sinus). The dura mater formingthe inner wall of the abscess is inflamed andusually covered with granulations correspondingto the extent of the abscess. there is severetoxemia and pyrexia. Localizing neurologicalsigns are sometimes found and depend on thesite of the abscess. Rarely, osteomyelitis, blood-borne or arising from an overlying carbuncle,affects the suboccipital region causing an extra-dural abscess with cerebellar signs. The cerebro-spinal fluid shows a moderate increase in whitecells but contains no organisms; its pressure maybe raised.When an extradural abscess is caused by osteo-
myelitis or mastoiditis, the operation appropriateto these diseases establishes the necessary drainage.When, however, an extradural abscess followsfracture of the skull, a burr-hole is made overthe site of the abscess and a drain inserted.Appropriate antibiotics are administered.
Subdural Suppuration(The synonym purulent pachymeningitis is a
bad term, for it equally well applies to extraduralabscess which is associated with pachymeningitissecondary to overlying osteomyelitis.) Subduralempyema means a widespread collection of pusbetween the dura and arachnoid mater. It is anuncommon but serious condition which beforethe days of antibiotics was invariably fatal. Thecommonest cause is osteomyelitis of the skullfollowing an acute exacerbation of inflammationof the nasal air sinuses. Such an exacerbationmay be brought about by operative interferencein sinusitis. Subdural infection may also becaused by blood-borne osteomyelitis of the skull,mastoiditis, or frac-tures of the skull which open
to the exterior or into septic nasal sinuses ormastoid cells. Infected subdural effusions notinfrequently complicate the convalescence in casesof acute purulent meningitis, especially in child-hood (Hankinson and Amador, 1956). There aresevere toxemia and pyrexia, with signs of raisedintracranial pressure (headache, vomiting andpapilledema). The infection spreads widely inthe subdural space producing contralateral hemi-paresis, cortical sensory loss and hemianopia. Ifthe dominant cerebral hemisphere is affected,dysphasia or aphasia may be found. Patientssometimes present with grand mal or Jacksonianepilepsy. Subdural empyemas sometimes occurbilaterally.A subdural abscess is a localized collection- of
pus; it may form during the treatment of sub-dural empyema, or the infection may be localizedfrom the beginning. Subdural abscesses tend toform along the falx or between the occipital lobeand tentorium. A subdural abscess produces alocalized neurological effect. Thus an abscess onthe medial aspect of the hemisphere involvingthe motor cortex causes paralysis of the contra-lateral leg with sparing of the arm and face.Lumbar puncture in subdural infection shows
raised pressure, and the cerebrospinal fluid con-tains an increased number of white cells (ioo to300 per cu. mm.) but no organisms. Althougha variety of organisms may be grown from theprimary focus, the commonest one found insubdural pus is the non-h2emolytic streptococcus.
Burr holes are made to confirm the diagnosisand to enable drainage to be carried out. Insubdural empyema small rubber catheters areinsinuated between the dura and arachnoid forthe instillation of penicillin, to which the organismsof subdural infection are usually sensitive (Schiller,Cairns and Russell, 1948). The strength ofpenicillin employed is 500 units per ml. of isotonicsaline. Although systemic penicillin passes intothe subdural space, the greater concentration of thedrug obtained by the catheter method is desirable.Subdural abscesses are located with the aid ofa brain cannula which is passed unhesitatinglythrough relatively silent parts of the brain, but itis particularly important to avoid the motor cortex

OLIVER: Intracranial Suppuration
and the speech zones. Diodone is injected intothe'subdural empyema or abscess cavity to demon-strate its extent radiologically. A subduralabscess, unlike a brain abscess, is shown to besuperficial to the brain. Ventriculography orangiography may be required to localize it. Anti-biotics are given from the beginning, and whenpenicillin is indicated, 20,000 units in 5 ml. of-isotonic saline are given by lumbar puncture toprevent meningitis arising after needling the brain,for systemic penicillin does not reach the cerebro-spinal fluid in sufficient concentration to beeffective. Subdural abscess is treated by inter-mittent aspiration and usually the instillation ofpenicillin.
Sigmoid Sinus ThrombosisSince the introduction of sulphonamides and
antibiotics, the incidence of this condition hasbeen greatly reduced and the clinical picturemodified. Now it is more often a complicationof chronic than of acute suppurative otitis mediaand, whereas in the past, septicemia was thecommon presentation, today the manifestationsof the disease are due to spreading thrombosisinto other venous sinuses and the cerebral veins.Formerly, the common -syndrome consisted ofheadache, rigors, swinging temperature, positiveblood culture, and metastatic abscesses in thelungs and elsewhere; at the present time, themore usual features are headache, vomiting andpapilledema caused by thrombosis spreading intothe other venous sinuses; if it spreads into corticalveins, focal effects may be produced such asepilepsy or hemiparesis. If thrombosis spreadsinto the petrosal sinuses the fifth and sixth cranialnerves may be affected producing paralysis of theexternal rectus muscle and pain in the face(Gradenigo's syndrome). Extension of throm-bosis into the internal jugular vein produces atender swelling in the neck.
Opinion is divided about the extent of surgicaltreatment that is necessary in these days of,abundant antibiotics. There is a tendency to becontent with mastoidectomy and wide exposureof the sigmoid sinus, but some otologists stilladvocate the classical triad of mastoidectomy,evacuation of the clot from the sinus and ligationof the internal jugular vein (Reading and Schurr,I956).
Cavernous Sinus Throm6osisSeptic thrombosis of the cavernous sinus may
arise from: (a) Boils or carbuncles of the nose orupper lip, especially after suigical interference;(b) erysipelas; (c) dental sepsis in the upper jaw,especially after extractions; or (d) middle-earinfection. In (a), (b) and (c) infection spreads to
the sinus through the angular and ophthalmicveins; in (d)' it spreads through the superiofpetrosal sinus. The onset occurs with headache,rigors and a remittent temperature. The eyelidsbecome swollen, the conjunctivae (edematous, theeyes fixed and proptosed, and the pupils dilatedand inactive. If the cornea is clear, retinalhamorrhages and papilloedema' may be observed.
Septic sinus thrombosis is rare in countrieswhere sulphonamides and antibiotics are freelyavailable for the treatment of the causal lesions.Formerly, the condition was fatal; patients diedfrom septicammia and metastatic infection of thelungs, or from meningitis; nowadays the dis5aseis usually cured with antibiotics. Nevertheless;septic lesions of the nose or upper lip-the'"danger area "-should not be squeezed 6rincised. There 'is nowadays no indication forligation o'f the angular veins in cavernous sinusinfection when the primary lesion is in the dangerarea.
MeningitisUnless otherwise stated, the term meningitis'
refers to leptomeningitis (i.e. inflammation of thearachnoid and pia mater). Infection may reachthe meninges directly from the exterior: (a) byerosion of the skin over a cranial or spinal con-genital defect (e.g. meningocele); (b) as the resultof open injuries of the head or spine; (c) followingcranial or spinal operations 'or lumbar puncturewhen aseptic technique has been defective.-Infection may also reach the meninges from thefollowing adjacent inflammatory diseases: (a)otitis media; (b) osteomyelitis of the skull; (c)'infected dermoid sinus of the occiput or spine(Logue and Till, I952); (d) cerebral abscess, byrupturing into the ventricles or subarachndid space.Lastly, infection may occur through the blood'stream; tuberculous and meningococcal menin-gitis arise in this way whereas pneumococcalmeningitis can occur either as a blood-borneinfection from pneumonia, or directly from otitismedia (by far the commonest cause) or nasalsinusitis. In many cases of pneumococcalmeningitis the source of infection cannot be traced.The symptoms of meningitis are frontal or
occipital headache, vomiting and in some casesphotophobia. Retention of urine may occur.The physical signs are neck stiffness, positiveKernig's sign and sometimes a positive Brud-zinski's sign (flexion of the hips and knees occurswhen the patient's head is flexed). These signsof meningeal irritation are accompanied bypyrexia and toxwemia. With the onset of coma,the signs of meningeal irritation may disappear,and in infants and young children they may beinconspicuous or absent from the beginning.' In-
Sept0mber I196 I 535

POSTGRADUATE MEDICAL JOURNAL
meningococcal meningitis, which may occursporadically or in epidemics, a petechial rash maybe present on the trunk (' spotted fever '). Intuberculous meningitis, the syndrome of menin-geal irritation may be absent, and thus the ' diag-nosis ' of pyrexia of unknown origin may be made.
In all forms of leptomeningitis, the cerebro-spinal fluid pressure is raised. In pyogenicmeningitis the fluid is opalescent because of thepresence of a large number of polymorphs (i,oooto io,ooo per cu. mm.). The protein is increased(Ioo to 500 mg. per ioo ml.), while the sugar isreduced below 40 mg. per ioo ml. The chloridesare moderately reduced.
In tuberculous meningitis, the cerebrospinalfluid appears clear or slightly hazy and, afterstanding a few hours, a fine web-like fibrin clotforms. The cell count is increased. In themajority of cases there are between 50 and 500cells per cu. mm. Lymphocytes and mono-nuclears predominate. The protein level is raisedwith an average of 200 mg. per ioo ml. If intuberculous meningitis the protein exceeds 500mg. per I00 ml. there is likely to be a subarachnoidblock. The sugar content is lowered but not tothe same extent as in pyogenic meningitis. Thechloride is usually reduced below 650 mg. perI00 ml. Although formerly thought to be areliable test for the presence or absence of tuber-culous meningitis, the chloride test is now regardedas significant only when positive. Under themicroscope, tubercle bacilli may be seen in thefluid or can be cultured from it.
Treatment of MeningitisIn pyogenic meningitis, the organism should be
identified as soon as possible and its antibioticsensitivity determined. In the meantime, a widespectrum antibiotic should be given. If theorganism is sensitive to penicillin, the drug shouldbe given intrathecally as well as intramuscularly,for an effective concentration of penicillin doesnot pass into the cerebrospinal fluid from theblood stream. The dose injected into the cerebro-spinal fluid must not exceed 20,000 units dailyand it should be dissolved in not less than 5 ml.of isotonic saline. Cases are on record in which500,000 units were given in error and the patientsdeveloped generalized convulsions and died within24 hours. Pneumococcal meningitis is usuallytreated with penicillin and a sulphonamide,whereas meningococcal meningitis requires onlya sulphonamide in the majority of cases. Hcemo-philus influenza meningitis usually responds tochloramphenicol alone, although there is a ten-dency to give it with sulphadiazine. In pyogenicmeningitis, the focus of origin of the infection maybe known and can be treated surgically, e.g.
mastoiditis and osteomyelitis of the skull. Intuberculous meningitis, a course of streptomycinis given lasting several months. The drug is givenintramuscularly and intrathecally. Burr holesmay be needed for injection of the drug into thelateral ventricles when adhesions have produceda spinal block (the intrathecal or intraventriculardose of streptomycin is So to ioo mg. in S ml.isotonic saline). Burr holes may also be requiredin pneumococcal meningitis when a spinal blockoccurs. When satisfactory progress is not beingmade by a patient suffering from pyogenicmeningitis, the possibility of a coexistent brainabscess, subdural abscess or subdural hygromashould be considered.
Brain AbscessOtitis media and mastoiditis may give rise to
an abscess in either the temporal lobe or thecerebellum. Abscess of the brain is much morelikely to be caused by chronic than acute infectionof the middle ear. Inflammatory diseases of thelungs, especially following their surgical treatment,are liable to cause metastatic brain abscesses;single abscesses occur much more frequently thanmultiple ones. Degeneration of a secondarycarcinoma, especially when there is no evidentprimary growth, may cause confusion in diagnosiswhen the lesion in the brain is aspirated. Nasalsinusitis, with or without spreading osteomyelitis,may cause a frontal lobe abscess. Open fracturesof the skull, when the dura mater has been openedand the brain penetrated, have a strong tendencyto cause intracranial suppuration (Fig. i). Abrain abscess is almost certain to form if frag-ments of bone, hair or hat material have beenleft in the brain. Fractures into the nasal airsinuses, with or without cerebrospinal fluidrhinorrhca, frequently cause meningitis and some-times a cerebral abscess. The presence of amissile is much less likely to cause an abscess.Osteomyelitis of the skull, caused either byinfection of the nasal air sinuses or by blood-borneorganisms, is liable to cause a brain abscess.Occasionally an inflammatory lesion of the scalpproduces a cerebral abscess without evidence ofosteomyelitis. Rarely, infection of an operationwound causes an abscess of the brain. Peripheralsepsis is responsible for an occasional brainabscess. Examples of such causal lesions arecarbuncle, whitlow, to9sillitis, infected dental root(especially after extraction), septic wounds andosteomyelitis. Sometimes an abscess occurswithout an evident focus of infection and maythus be encountered unexpectedly. Cryptogenicbrain abscess is particularly liable to occur in thepresence of congenital heart disease, especiallywhen there is cyanosis (Campbell, 1957). More
536 6September i9 I

OLIVER: Intracranial Suppuration
G. 2.-A carod a ig shoing te c c-...... ..:...........teristic upwad swp ..t...c
.5''5'5'...n ....& .. ....... -
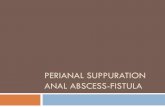
FIG. 2.-A carotid arteriogram showing the charac-teristic upward sweep of the middle cerebralartery and the opening up of the carotid ' syphon'produced by a space-occupying lesion in the tem-poral lobe, in this case an abscess.
.... .....
FIG. i.-Inflammation of the right upper lid at the siteof entry of a pencil through the root of the orbit.The pencil entered the brain and caused an abscessin the frontal lobe. The abscess was successfullytreated by the aspiration method.
than 5o% of such abscesses have been found inassociation with Fallot's tetralogy and some havefollowed operations for cardiac lesions. They arenot necessarily caused by paradoxical emboli, forthe shunt is not always from right to left.
Bacteriology. Organisms isolated from abscessesof the brain include Staphylococcus aureus or albus;Streptococcus pyogenes, viridans or pneumonia?Pseudonomas pyocyanea; Proteus vulgaris; actino-myces; diphtheroids; Haemophilus influenza? andoccasionally Entamcba histolytica. Not in-frequently a mixed growth of organisms isobtained. The nature of the responsible organismsand their sensitivity to the various antibiotics isascertained. Often, however, no organism isdemonstrated in the pus although the infectionmay still be active in the abscess capsule.
Diagnosis. An abscess of the brain behaveslike a tumour, giving rise to increased intracranialpressure and localizing signs. Thus there areheadache, vomiting and, frequently, but notalways, a mild degree of papilledema. A meta-static abscess may begin with epileptic attackswhich, if of the Jacksonian type, are of localizingvalue. When the infection arises in the skull orits air-containing cavities, the cerebral abscess is
usually immediately subjacent to the primarylesion, but occasionally it may be well away fromthe area of osteomyelitis. A careful neurologicalexamination is therefore necessary. The com-monest site for osteomyelitis is in the frontalregion, although no part of the skull is exempt.Of particular importance in temporal lobeabscesses is examination of the visual fieldswhichcommonly show an upper quadrantic homonymousdefect or, if the abscess is extensive, a completehemianopia. Cerebellar abscesses produce mini-mal or moderate cerebellar signs (unilateralhypotonia; incoordination of the upper ex-tremity of the same side; nystagmus, which ismore marked and of greater excursion when thepatient fixes his gaze towards the side of theabscess; and a tendency for the patient to deviatetowards the side of the lesion when walking).A metastatic abscess may occur anywhere in thebrain. As much information as possible aboutits location is obtained from the history andneurological examination, as in the diagnosis ofintracranial tumnours, and help then obtainedfrom the investigations discussed below. Thetemperature is most likely to be slightly raised(990 to ioo0F.) or subnormal. A high temperatureis not found with an uncomplicated brain abscess.The pulse may show an increased rate or theclassical slowing of increased intracranial pressure.
Investigations. Lumbar puncture is avoidedwhen possible for fear of producing a cerebellarpressure cone. The cerebrospinal fluid is clearin uncomplicated cases, although there is usually
September I 96 I 537

POSTGRADUATE MEDICAL JOURNAL
FIG. 3.-A temporal lobe abscessvisualized radiologically by in-jection of 2 ml. diodone afteraspiration of pus.
a moderate increase in white cells. There shouldbe no organisms, either on direct examination ofthe fluid or after culture. When there is doubtabout the presence or location of an abscess,ventriculography or arteriography should becarried out. The latter investigation is particularlyuseful in demonstrating an abscess in the tem-poral lobe, because it may be difficult or impossibleto fill the temporal horn with air in such cases(Fig. 2). Electroencephalography is likely to showslow waves of marked amplitude, and phase-reversal in the region of a supratentorial abscess.When a brain abscess has been localized, itsextent can be demonstrated by positive contrastradiography. Diodone 2 to 3 ml. is injected intothe abscess cavity after some of the pus has beenaspirated (Oliver and Leese, I949). The skull isthen X-rayed (Fig. 3). Many neurosurgeonsrecommend Thorotrast (thorium dioxide), for ithas the advantage of remaining in situ and thusthe progress of the abscess can be followed radio-logically. But there is experimental evidence thatThorotrast, acting as a foreign body, stimulatescapsule formation (Falconer, McFarlan andRussell, 1943). Therefore, if resolution of theabscess is desired, the rapidly absorbable contrastmedium, diodone, should be employed. Further-more, it is a violation of surgical principles toleave an unabsorbable foreign body in a septicplace. The late Julian Taylor had strong feelingsabout this: ' I should like to point out that toinject a foreign body such as Thorotrast . . . into
a closed abscess cavity is asking for persistence ofinfection as plainly in the brain as it would beanywhere else in the body. There is no primaryreason to suppose that it may be any less provoca-tive of chronicity than is a sequestrum, or a knotof so-called absorbable catgut, in the depths ofa sinus. I cannot help thinking that the wide-spread habit of demonstrating the existence ofabscesses radicilogically by this means may bea cause of the need to excise them later' (Taylor,I950).
Treatment of Brain Abscess(a) Aspiration. A burr hole is made over the
site of the abscess, unless it is secondary toosteomyelitis of the skull when the dura mater isalready exposed by removal of infected bone.A small incision, a few millimetres long, is madein the dura mater. An avascular point on thesurface of the brain is punctured with a pointedtenotome, and a bluni-ended brain needle is'passed into the abscess cavity. The pus isaspirated and replaced by 2 to 3 ml. penicillinsolution (ioo,ooo units per ml.). This smallvolume of fluid is injected to avoid rupture of thecapsule which may be extremely thin. Sometimesan abscess heals after one penicillin replacement,but the procedure may have to be repeated severaltimes. The cannula (brain needle) is then passedthrough the original burr hole between thesutures. Considerable judgment is needed inspacing aspirations. Needling should be repeated
S--ebtember i 96 i538

OLIVER: Intracranial Suppuration ... 5,39
FiG. 4.-The probe indicates a largeopening from the interior wallof a temporal abscess throughwhich there was a free com-munication with the tympanicantrum. This type of abscessshould be totally excised.
if the patient's general and neurological state donot improve; it should not be delayed untildeterioration occurs. At first, aspiration andpenicillin replacement may be needed at intervalsof 24 to 48 hours, but when progress is satisfactory,the intervals become longer and longer until nomore pus can be aspirated. Many abscesses canbe completely cured by this technique (Oliverand Leese, 1949) but if a patient's condition doesnot improve or deteriorates the possible causesare: (i) Persistent infection in the capsule asso-ciated with brain swelling. The abscess shouldthen be excised' (vide infra, method b) and decom-pression performed. The edema may also bereduced by intravenous injection of a solution ofurea. (2) Loculation, in which aspiration onlydrains part of the abscess. Other loculi may bedetected and drained by needling in new direc-tions. (3) The presence of multiple abscesseswhich may occur when the primary infection isin the lungs. Neurological examination alonemay not reveal the location of additional abscesses,but they may be demonstrated by ventriculo-graphy. (4) A sinus which has become establishedwith the tympanic antrum in an otogenic brainabscess (Fig. 4). Such an abscess will not healunless excised. (5) The presence of a foreign bodyin the abscess, e.g. bone fragments in post-traumatic cases. The aspiration technique isparticularly applicable to abscesses which involvethe motor cortex, the speech zones or the opticradiations when other methods would cause severeneurological deficits. Furthermore, aspiration
may be life-saving for patients who are too ill toundergo a major operation.
(b) Secondary Excision. Excision of the abscesscapsule is carried out when aspiration alone fails.Some neurosurgeons, however, excise the abscesscapsule as a routine as soon as aspiration isunproductive. After excision of the abscesscapsule, the wound is closed without drain-age.
(c) Primary Excision. This is another methodof treatment made possible by the discovery ofantibiotics (Le Beau, 1946). The advantage isthat the anxious period of observation requiredby the aspiration technique is'eliminated. Primaryexcision of the abscess is particularly indicatedwhen it is situated in a relatively silent part of thebrain, e.g. the frontal or cerebellar lobes wherea neurological deficit is unlikely to be caused byexcision. It is also the best method of treatingan abscess following an open head injury, for anyindriven fragments of bone or foreign bodies areautomatically removed and the infection is thusbrought to an end. A brain abscess occasionallyfollows a very slow course, and the onset ofincreased intracranial pressure and localizing signsare long delayed. Such an abscess develops intoa solid mass of fibrous tissue closely resemblinga tumour, although there may be a small quantityof pus in the centre. Primary excision is the onlypossible treatment in such a case.
In the management of cerebellar abscess, com-pression of the medulla oblongata by the increasingvolume of the abscess and the surrounding cedema
El
Se-btember i 96 i

540- POSTGRADUATE MEDICAL JOURNAL September I96I
of the cerebellum demands immediate decom-pression. A full exposure of the posterior fossais first carried out. The abscess is then aspiratedwith a brain cannula through a small puncturemade in the dura mater on the side of the abscess,and penicillin (ioo,ooo units dissolved in i ml. ofisotonic saline) is instilled into the cavity. The
dura mater is opened over both cerebellar lobes,and the abscess is removed. The wound isclosed without drainage, and 20,000 units ofpenicillin in 5 ml. of isotonic saline are given bylumbar puncture. If the patient is very ill, theabscess is aspirated and its removal carried outa few days later.
REFERENCESCAMPBELL, M. (1957): Cerebral Abscess in Cyanotic Congenital Heart Disease, Lancet, i, ixiI.FALCONER, M. A., McFARLAN, A. M., RUSSELL, D. S. (1943): Experimental Brain Abscesses in the Rabbit, Brit. 7.
Surg., 30, 245.HANKINSON, J., and AMADOR, L. V. (I956): Infected Subdural Effusions, Brit. med.J7. ii, I2z.LE BEAU, J. (1946): Radical Surgery and Penicillin in Brain Abscess, Y. Neurosurg., 3, 359.LOGUE, V., and TILL, K. (1952): Posterior Fossa Dermoid Cysts with Special Reference to Intracranial Infection,
J7. Neurol. Neurosurg. Psychiat., 15, I.OLIVER, L. C., and LEESE, W. L. B. (1949): Treatment of Brain Absces3 with Special Reference to a Conservative
Method, Lancet, ui, 828.READING, P. V., and SCHURR, P. H. (1956): Thrombosis of the Sigmoid Sinus, Ibid., ii, 473.SCHILLER, F., CAIRNs, H., and RUSSELL, D. S. (I948): The Treatment of Purulent Pachymeningitis and Subdural
Suppuration with Special Reference to Penicillin, 3. Neurol. Neurosurg. Psychiat., xi, New Series, 143.TAYLOR, J. (1950): Intracranial Suppuration, Proc. roy. Soc. Med., 43, 129.