
Intracranial revascularization in Acute Stroke: Data and · PDF fileIntracranial...
78
Intracranial revascularization in Acute Stroke: Data and Trials Session 4: Target Stroke S. Mangiafico Interventistica Neurovascolare AOUCareggi Firenze
Transcript of Intracranial revascularization in Acute Stroke: Data and · PDF fileIntracranial...

Intracranial
revascularization in Acute
Stroke: Data and Trials
Session 4: Target Stroke
S. Mangiafico
Interventistica Neurovascolare
AOUCareggi
Firenze

disclosure
• Codaman Neurovascular

Recanalization is an independent predictor of favorable clinical outcome


NEJM, March 2013
5

SYNTHESIS exp (1 feb. 2008-16 apr.2012)
362 pts with ischemic stroke onset within 4.5 h. Randomization 1:1
181 Endovasc.
Median onset-to-groin 3.45 h
Interquartile (3:14-4.20)
181 i.v.
Median onset-to-needle 2.75 h
Interquartile (2:20-3:20) P<0.01
mRS 0-1 (3 m)
30.4%
mRS 0-1 (3 m)
34.8% OR (adjusted for age, sex, stroke severity, AF) 0.71 (CI 95% 0.44-1.14) P=0.16
Fatal or non Fatal symptomatic hemorrhage in 6% in both groups

Synthesis Analisi per sottogruppi

SYNTHESIS: CRITICAL POINTS
Low recanazatin rate due to Old devices ( only in 15% )
• Uselected vascular occlusion, unselcted perfusion patterns
• No bridging no rescue
Delayed Groin puncture after 1 h vs iv tpa administaration
•

IMS III Phase III, randomized, open-label trial
iv t-PA vs iv t-PA associated with Endovascular treatment
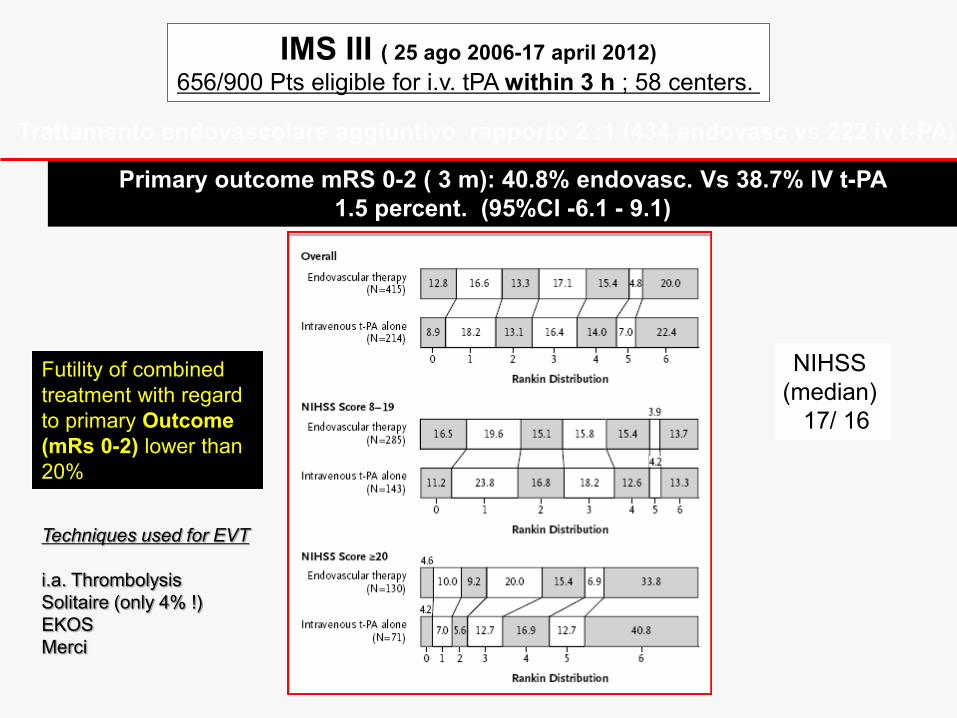
IMS III ( 25 ago 2006-17 april 2012)
656/900 Pts eligible for i.v. tPA within 3 h ; 58 centers.
Trattamento endovascolare aggiuntivo rapporto 2 :1 (434 endovasc vs 222 iv t-PA)
Primary outcome mRS 0-2 ( 3 m): 40.8% endovasc. Vs 38.7% IV t-PA
1.5 percent. (95%CI -6.1 - 9.1)
Futility of combined
treatment with regard
to primary Outcome
(mRs 0-2) lower than
20%
NIHSS
(median)
17/ 16
Techniques used for EVT
i.a. Thrombolysis
Solitaire (only 4% !)
EKOS
Merci

IMS 3: very low recanalization rates
correlation TICI-outcome (mRS 0-2)
TICI 0 : 12.7%
TICI 1: 27.6%
TICI 2a : 34.3%
TICI 2b : 47.9%
TICI 3: 71.4%
(P<0.001)
Broderick JP et al. N Engl J Med 2013;368:893-903
Reperfusion rates, TICI 2b -3 (end of the procedure DSA)
38% ICA
44% complete M1,
44% single M2 occlusion,
23% for multiple M2 occlusions

But…

Better outcome
Stroke onset –IV
tPA < 120 min
Better outcome
In severe stroke
NIHSS> 20
Better outcome
If stroke onset-
IV treatment
Within 2 h
NIHSS > 20

182 pts of IMS3
Recanalizatione within 7h
Average Time-to-reperfusion 325’

7
With CTA-confirmed occlusion at baseline, representative of current practice, IMS III has a positive outcome for endovascular therapy.
IMS III: Considering patients with documented occlusion through CT-Angiography, the
endovascular treatment seems to be effective
Endovascular
confers a real
benefit across the
spectrum of mRS
A. Demchuk, IMS III: Comparison of
Outcomes between IV and IV/IA
Treatment in Baseline CTA Confirmed
ICA, M1, M2 and Basilar Occlusions,
slide 20, Presented at ISC 2013,
Honolulu, Hawaii

MR RESCUE
phase 2b, randomized, controlled,open-label (blinded outcome), multicenter trial
conducted at 22 sites in North America
study within 8 hours after the onset of large vessel,anterior-circulation strokes
Mechanical Embolectomy (MerciRetriever or Penumbra System) vs Standard Care.
Randomization was stratified according to whether the patient had a favorable
penumbral pattern (substantial salvageable tissue and small infarct core) or a non
penumbral pattern (large core or small or absent penumbra).
Outcomes 90-day modified Rankin scale,
MR RESCUE

In summary, patients between the
ages of 18 and 85 years, NIHSS
scores of 6 to 29 who had a large-
vessel, anterior-circulation ischemic
stroke were randomly assigned within
8 hours after the onset of symptoms
to undergo either mechanical
embolectomy (Merci Retriever or
Penumbra System)
or standard medical care.
Patients who were treated with
intravenous t-PA without successful
recanalization were eligible if
magnetic resonance angiography or
CT angiography after the treatment
showed a persistent target occlusion
A favorable penumbral pattern was
defined as a predicted infarct core of
90 ml or less and a proportion of
predicted infarct tissue within the at-
risk region of 70% or less.
•Outcome : mRS 0-2
•Outcome : On 7-day CT or MRI perfusion
imaging,
•Successful reperfusion was defined as a
reduction of 90% or more in the volume of the
perfusion lesion from baseline with the time
until the peak of the residue function of more
than 6 seconds.
118 patients who met the full eligibility criteria.
Overall, 68 of 118 patients (58%) had a
favorable penumbral pattern on final core
laboratory review.
Misure di Outcome

MR RESCUE

Conclusions
study did not confirm hypothesis that penumbral imaging would identify
patients who would differentially benefit from endovascular therapy for
acute ischemic stroke within 8 hours after symptom onset
regardless of penumbral-imaging pattern on study entry, no significant
differences were noted in clinical and imaging outcomes for patients undergoing
embolectomy,as compared with those receiving standard medical care.

MR Rescue, Comments • Low recanalization rates (obsolete devices)
• Therapeutic window too wide (late treatments, futile recanalizations)
• Wide latency between imaging and endovascular treatment
• i.v. t-PA used in 37% of patients • • Heterogeneity of perfusional imaging (CT, MR)
• It might be possible that patients with a favorable panumbral pattern
could have a good clinical outcome independently from type of treatment (collaterals)

The trials lesson
• SYNTHESIS expansion and IMSIII ( t-PA vs i.a. thrombolysis IA/ i.v. r-tPA vs i.v. r-tPA + endovascular treatment) : the missed favorable result for i.a. treatment dependend on the inappropriate selection of patients (no documented occlusions) and on the missed used of stent-retrievers (low recanalization rates) although the time to groin was respectively of 225 and 196 mins
• MR rescue - ( within6 h) ( tPA vs TPA+ thrombectomy): too long time-to-treatment, low recanalization rates

New devices

The TREVO 2 study
Trevo versus Merci retrievers for thrombectomy revascularisation of large vessel
occlusions in acute ischaemic stroke (TREVO 2): a randomised trial (trevo vs
merci) Raul G Nogueira et al. for the TREVO 2 Trialists Lancet 2012; 380: 1231–40

SWIFT (Solitaire FR with the Intention for Thrombectomy) Study Solitaire flow restoration device versus the Merci Retriever in
patients with acute ischaemic stroke (SWIFT): a randomised,
parallel-group, non-inferiority trial
Jeffrey L Saver, et al. for the SWIFT Trialists Lancet 2012; 380: 1241–49
3 months mRS
Patients included in the trial
may be ineligible for or have
failed IV tPA within an 8-hour
window

New trials
• New device
• Documented major intracranial vascular
occlusion
• Perfusional Imaging of volume of infarction

26
Courtesy of Dr. Castaño
Stents: immediate flow restoration
Retrievers: removed after thrombectomy
Distal and within the occlusion
SolitaireTM, TREVO® , REVIVE, PRESET, EMBO-TRAP
Castaño C et al. Stroke 2010
Rohde S et al.Stroke 2011
San Román L et al. Stroke 2012
New neuroendovascular thrombectomy devices

27
Schellinger et al. Stroke 2008
Lansberg MG et al. Stroke 2008
TCDx - Angio-CT/ASPECTS Angio-MR/DWI
Mismatch
Neuroimaging tools to identify salvageable brain

Ottobre 2014
Febbraio 2015
Aprile 2015

29
OTR: median time from onset to randomisation; OTG: median time
from onset to groin puncture; mRS, modified Rankin scale; BMT:
Best medical therapy (includes IV alteplase if eligible); RCT,
randomised controlled trial; EVT, endovascular therapy; ICA, internal
carotid artery; CTP, computer tomography perfusion
* MRI or CTP mismatch >1.8 in the first 71 patients
Clinical trial
Control
Time
window
OTR time
(randomisatio)
Trial end Proven
occlusion
Ischaemic
penumbra
IV alteplase
(%)
OTG time Stent-
riever
Outcome
variable
MR CLEAN
(n=500)
IV alteplase
6.0h
204 min
Ended ICA, M1, M2,
A1, A2
NA rt-PA
failure
89%
260 min 81% mRS at 90d
(shift)
ESCAPE
(n=316)
BMT
12.0h
169 min
Halted ICA, M1 ASPECT 6-10
Good collaterals
Bridging
75%
185 min 86% mRS at 90d
(shift)
EXTEND IA
(n= 70)
IV alteplase
4.5h
157 min
Halted ICA, M1, M2 CTP or MRI
Tmax 6sec
Core <70mL
Bridging
100%
210 min 100% 24h
reperfusion
3 days NIHSS
SWIFT
PRIME
(n=196)
Iv alteplase
6h
188 min
Halted ICA, M1 ASPECT 6-10*
Bridging
100%
224 min 100% mRS at 90d
(shift)
REVASCAT
(n=206)
BMT
8.0h
223 min
Halted
after 1st
interim
ICA, M1 ASPECT 6-10 rt-PA failure
(30’) 73%
269 min 100% mRS at 90d
(shift)
Design of recently published RCT on EVT
1 - Berkhemer OA et al. N Engl J Med 2015;372:11-20.
2 - Goyal M et al. N Engl J Med 2015; ePub February 11
3 - Campbell BCV et al. N Engl J Med 2015; ePub February 11
4 - Saver J et al. N Engl J Med 2015, ePub April 17
5 – Jovin T et al. N Engl J Med 2015, ePub April 17

30
OTR: median time from onset to randomisation; OTG: median time
from onset to groin puncture; mRS, modified Rankin scale; BMT:
Best medical therapy (includes IV alteplase if eligible); RCT,
randomised controlled trial; EVT, endovascular therapy; ICA, internal
carotid artery; CTP, computer tomography perfusion
* MRI or CTP mismatch >1.8 in the first 71 patients
Clinical trial
Control
Time
window
OTR time
(randomisatio)
Trial end Proven
occlusion
Ischaemic
penumbra
IV alteplase
(%)
OTG time Stent-
riever
Outcome
variable
MR CLEAN
(n=500)
IV alteplase
6.0h
204 min
Ended ICA, M1, M2,
A1, A2
NA rt-PA
failure
89%
260 min 81% mRS at 90d
(shift)
ESCAPE
(n=316)
BMT
12.0h
169 min
Halted ICA, M1 ASPECT 6-10
Good collaterals
Bridging
75%
185 min 86% mRS at 90d
(shift)
EXTEND IA
(n= 70)
IV alteplase
4.5h
157 min
Halted ICA, M1, M2 CTP or MRI
Tmax 6sec
Core <70mL
Bridging
100%
210 min 100% 24h
reperfusion
3 days NIHSS
SWIFT
PRIME
(n=196)
Iv alteplase
6h
188 min
Halted ICA, M1 ASPECT 6-10*
Bridging
100%
224 min 100% mRS at 90d
(shift)
REVASCAT
(n=206)
BMT
8.0h
223 min
Halted
after 1st
interim
ICA, M1 ASPECT 6-10 rt-PA failure
(30’) 73%
269 min 100% mRS at 90d
(shift)
Design of recently published RCT on EVT
1 - Berkhemer OA et al. N Engl J Med 2015;372:11-20.
2 - Goyal M et al. N Engl J Med 2015; ePub February 11
3 - Campbell BCV et al. N Engl J Med 2015; ePub February 11
4 - Saver J et al. N Engl J Med 2015, ePub April 17
5 – Jovin T et al. N Engl J Med 2015, ePub April 17

31
OTR: median time from onset to randomisation; OTG: median time
from onset to groin puncture; mRS, modified Rankin scale; BMT:
Best medical therapy (includes IV alteplase if eligible); RCT,
randomised controlled trial; EVT, endovascular therapy; ICA, internal
carotid artery; CTP, computer tomography perfusion
* MRI or CTP mismatch >1.8 in the first 71 patients
Clinical trial
Control
Time
window
OTR time
(randomisatio)
Trial end Proven
occlusion
Ischaemic
penumbra
IV alteplase
(%)
OTG time Stent-
riever
Outcome
variable
MR CLEAN
(n=500)
IV alteplase
6.0h
204 min
Ended ICA, M1, M2,
A1, A2
NA rt-PA
failure
89%
260 min 81% mRS at 90d
(shift)
ESCAPE
(n=316)
BMT
12.0h
169 min
Halted ICA, M1 ASPECT 6-10
Good collaterals
Bridging
75%
185 min 86% mRS at 90d
(shift)
EXTEND IA
(n= 70)
IV alteplase
4.5h
157 min
Halted ICA, M1, M2 CTP or MRI
Tmax 6sec
Core <70mL
Bridging
100%
210 min 100% 24h
reperfusion
3 days NIHSS
SWIFT
PRIME
(n=196)
Iv alteplase
6h
188 min
Halted ICA, M1 ASPECT 6-10*
Bridging
100%
224 min 100% mRS at 90d
(shift)
REVASCAT
(n=206)
BMT
8.0h
223 min
Halted
after 1st
interim
ICA, M1 ASPECT 6-10 rt-PA failure
(30’) 73%
269 min 100% mRS at 90d
(shift)
Design of recently published RCT on EVT
1 - Berkhemer OA et al. N Engl J Med 2015;372:11-20.
2 - Goyal M et al. N Engl J Med 2015; ePub February 11
3 - Campbell BCV et al. N Engl J Med 2015; ePub February 11
4 - Saver J et al. N Engl J Med 2015, ePub April 17
5 – Jovin T et al. N Engl J Med 2015, ePub April 17

32
OTR: median time from onset to randomisation; OTG: median time
from onset to groin puncture; mRS, modified Rankin scale; BMT:
Best medical therapy (includes IV alteplase if eligible); RCT,
randomised controlled trial; EVT, endovascular therapy; ICA, internal
carotid artery; CTP, computer tomography perfusion
* MRI or CTP mismatch >1.8 in the first 71 patients
Clinical trial
Control
Time
window
OTR time
(randomisatio)
Trial end Proven
occlusion
Ischaemic
penumbra
IV alteplase
(%)
OTG time Stent-
riever
Outcome
variable
MR CLEAN
(n=500)
IV alteplase
6.0h
204 min
Ended ICA, M1, M2,
A1, A2
NA rt-PA
failure
89%
260 min 81% mRS at 90d
(shift)
ESCAPE
(n=316)
BMT
12.0h
169 min
Halted ICA, M1 ASPECT 6-10
Good collaterals
Bridging
75%
185 min 86% mRS at 90d
(shift)
EXTEND IA
(n= 70)
IV alteplase
4.5h
157 min
Halted ICA, M1, M2 CTP or MRI
Tmax 6sec
Core <70mL
Bridging
100%
210 min 100% 24h
reperfusion
3 days NIHSS
SWIFT
PRIME
(n=196)
Iv alteplase
6h
188 min
Halted ICA, M1 ASPECT 6-10*
Bridging
100%
224 min 100% mRS at 90d
(shift)
REVASCAT
(n=206)
BMT
8.0h
223 min
Halted
after 1st
interim
ICA, M1 ASPECT 6-10 rt-PA failure
(30’) 73%
269 min 100% mRS at 90d
(shift)
Design of recently published RCT on EVT
1 - Berkhemer OA et al. N Engl J Med 2015;372:11-20.
2 - Goyal M et al. N Engl J Med 2015; ePub February 11
3 - Campbell BCV et al. N Engl J Med 2015; ePub February 11
4 - Saver J et al. N Engl J Med 2015, ePub April 17
5 – Jovin T et al. N Engl J Med 2015, ePub April 17
<

33
OTR: median time from onset to randomisation; OTG: median time
from onset to groin puncture; mRS, modified Rankin scale; BMT:
Best medical therapy (includes IV alteplase if eligible); RCT,
randomised controlled trial; EVT, endovascular therapy; ICA, internal
carotid artery; CTP, computer tomography perfusion
* MRI or CTP mismatch >1.8 in the first 71 patients
Clinical trial
Control
Time
window
OTR time
(randomisatio)
Trial end Proven
occlusion
Ischaemic
penumbra
IV alteplase
(%)
OTG time Stent-
riever
Outcome
variable
MR CLEAN
(n=500)
IV alteplase
6.0h
204 min
Ended ICA, M1, M2,
A1, A2
NA rt-PA
failure
89%
260 min 81% mRS at 90d
(shift)
ESCAPE
(n=316)
BMT
12.0h
169 min
Halted ICA, M1 ASPECT 6-10
Good collaterals
Bridging
75%
185 min 86% mRS at 90d
(shift)
EXTEND IA
(n= 70)
IV alteplase
4.5h
157 min
Halted ICA, M1, M2 CTP or MRI
Tmax 6sec
Core <70mL
Bridging
100%
210 min 100% 24h
reperfusion
3 days NIHSS
SWIFT
PRIME
(n=196)
Iv alteplase
6h
188 min
Halted ICA, M1 ASPECT 6-10*
Bridging
100%
224 min 100% mRS at 90d
(shift)
REVASCAT
(n=206)
BMT
8.0h
223 min
Halted
after 1st
interim
ICA, M1 ASPECT 6-10 rt-PA failure
(30’) 73%
269 min 100% mRS at 90d
(shift)
Design of recently published RCT on EVT
1 - Berkhemer OA et al. N Engl J Med 2015;372:11-20.
2 - Goyal M et al. N Engl J Med 2015; ePub February 11
3 - Campbell BCV et al. N Engl J Med 2015; ePub February 11
4 - Saver J et al. N Engl J Med 2015, ePub April 17
5 – Jovin T et al. N Engl J Med 2015, ePub April 17

MR CLEAN october 2014

ESCAPE february 2015

EXTEND-IA february 2015

april 2015


REVASCAT april 2015

Clinical trial Median NIHSS
improvement at
24h
mRS 0-2
T vs C
Adj. OR, 95%CI
24h Complete
recanalisation
T vs C
Infarct volume
median (IQR)
T vs C
MR CLEAN
(n=500)
IV alteplase
-2.6 33% vs 19%
2.2 (1.4, 3.4)
75% vs 34% 49 (22,96)
vs
79 (34-125)
ESCAPE
(n=316)
BMT
-4.0 53% vs 29% NA NA
EXTEND IA
(n= 70)
IV alteplase
80% vs 37% 71% vs 40%
4.2 (1.4, 12)
94% vs 43% 11 (0, 24)
vs 35 (6, 73)
SWIFT PRIME
(n=196)
Iv alteplase
-4.6 60% vs 35%
2.7 (1.5, 4.9)
83% vs 40%* NA
REVASCAT
(n=206)
BMT
58% vs 20% 44% vs 28%
2.1 (1.1, 4.0)
NA 16 (8, 58)
vs
39 (12, 87)
T, thrombectomy; C, control; IQR, interquartile range; mRS, modified
Rankin score; BMT, best medical therapy; OR, odds ratio
* Successful reperfusion (>90%) on CTP or MRI
I farct growth
Decrease of 8 or ore poi ts i NIHSS score or score = 0-2
Clinical outcomes NIHSS improvement at 24 h
mRS 0-2 ( 3 m)
1 - Berkhemer OA et al. N Engl J Med 2015;372:11-20.
2 - Goyal M et al. N Engl J Med 2015; ePub February 11
3 - Campbell BCV et al. N Engl J Med 2015; ePub February 11
4 - Saver J et al. N Engl J Med 2015, ePub April 17
5 – Jovin T et al. N Engl J Med 2015, ePub April 17

Clinical trial
Control
Death at 90 days
Thrombectomy
vs Control
SICH (PH2)
Thrombectomy
vs Control
Malignant
oedema
Thrombectomy
vs Control
SAH
Thrombectomy
vs Control
Progressing
stroke
Thrombectomy
vs Control
MR CLEAN
(n=500)
IV alteplase
21% vs 22% 6% vs 5.2% NA 0.9% vs 0% 20% vs18%
ESCAPE
(n=316)
BMT
10% vs 19% 3.6% vs 2.7% 5% vs 11% 0.6% vs 0% NA
EXTEND IA
(n= 70)
IV alteplase
9% vs 20% 0% vs 6% NA 1% vs 0% NA
SWIFT PRIME
(n=196)
IV alteplase
9% vs 12% 0% vs 3.1% NA 4% vs 1% NA
REVASCAT
(n=206)
BMT
18%/ vs 15% 1.9% vs 1.9% 11% vs 10% 4.9% vs 1.9% 15% vs 13%
BMT: Best medical therapy (includes IV alteplase if eligible); SICH,
symptomatic intracerebral haemorrhage; SAH, subarachnoid
haemorrhage
Alteplase (rt-PA) does not have marketing approval in Europe
for treatment >4.5 hours after stroke onset.
Safety variables
1 - Berkhemer OA et al. N Engl J Med 2015;372:11-20.
2 - Goyal M et al. N Engl J Med 2015; ePub February 11
3 - Campbell BCV et al. N Engl J Med 2015; ePub February 11
4 - Saver J et al. N Engl J Med 2015, ePub April 17
5 – Jovin T et al. N Engl J Med 2015, ePub April 17

Clinical trial Median NIHSS
improvement at
24h
mRS 0-2
T vs C
Adj. OR, 95%CI
24h Complete
recanalisation
T vs C
Infarct volume
median (IQR)
T vs C
MR CLEAN
(n=500)
IV alteplase
-2.6 33% vs 19%
2.2 (1.4, 3.4)
75% vs 34% 49 (22,96)
vs
79 (34-125)
ESCAPE
(n=316)
BMT
-4.0 53% vs 29% NA NA
EXTEND IA
(n= 70)
IV alteplase
80% vs 37% 71% vs 40%
4.2 (1.4, 12)
94% vs 43% 11 (0, 24)
vs 35 (6, 73)
SWIFT PRIME
(n=196)
Iv alteplase
-4.6 60% vs 35%
2.7 (1.5, 4.9)
83% vs 40%* NA
REVASCAT
(n=206)
BMT
58% vs 20% 44% vs 28%
2.1 (1.1, 4.0)
NA 16 (8, 58)
vs
39 (12, 87)
T, thrombectomy; C, control; IQR, interquartile range; mRS, modified
Rankin score; BMT, best medical therapy; OR, odds ratio
* Successful reperfusion (>90%) on CTP or MRI
I farct growth
Decrease of 8 or ore poi ts i NIHSS score or score = 0-2
GROWTH INFARCTION
1 - Berkhemer OA et al. N Engl J Med 2015;372:11-20.
2 - Goyal M et al. N Engl J Med 2015; ePub February 11
3 - Campbell BCV et al. N Engl J Med 2015; ePub February 11
4 - Saver J et al. N Engl J Med 2015, ePub April 17
5 – Jovin T et al. N Engl J Med 2015, ePub April 17

Recanalization rate
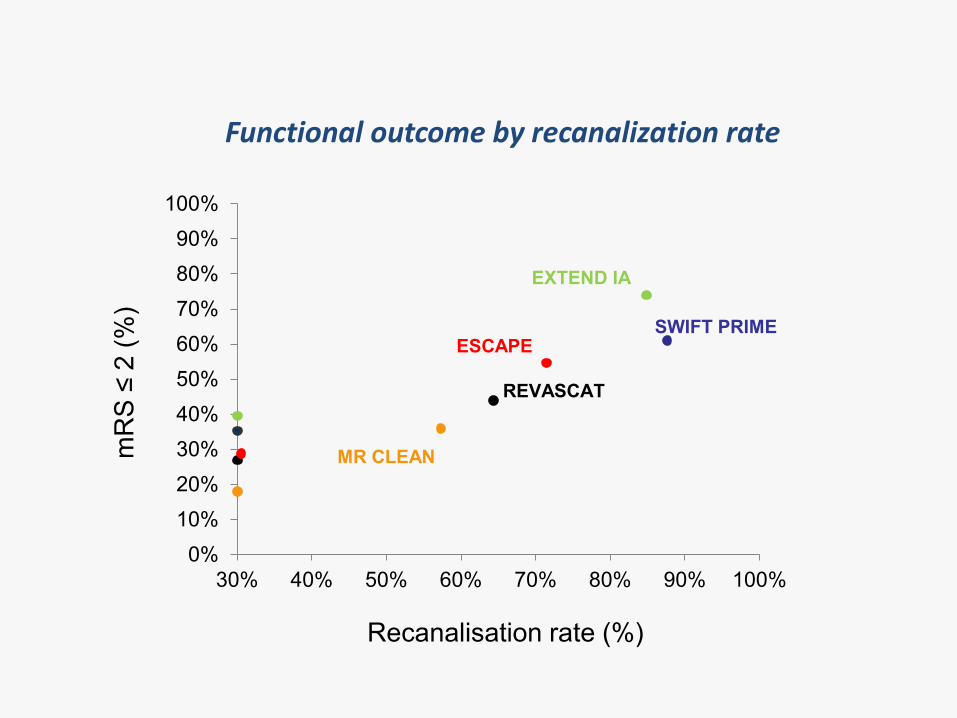
Functional outcome by recanalization rate
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
30% 40% 50% 60% 70% 80% 90% 100%
MR CLEAN
EXTEND IA
ESCAPE SWIFT PRIME
REVASCAT
mR
S ≤
2 (%
)
Recanalisation rate (%)

Reperfusion rate

Time to recanalization


time from last seen normal to groin puncture
STUDI
O
MR-
CLEAN
ESCAP
E
EXTEN
D-IA
SWIFT-
PRIME
REVAS
CAT

Mazighi et al Circulation. 2013;127:1980-1985
Metanalysis of 7 studies on endovascular treatment
It confirms that the time
from the onset to
reperfusion influence the
mortality and the chance to
obtain a favorable outcome:
it should be considered the
main target during the
management of acute
ischemic stroke
The favorable clinical outcome (mRS score, 0–2) was significantly reduced when the
time to reperfusion increased, OR adjusted for increasing intervals of 30 minutes 0.79
(95% CI, 0.72–0.87; P<0.001)

Abilleira S et al. Stroke. 2014;45:1046-1052 Parameter: onset to groin puncture

Bridging or rescue

52
?
Probability of achieving a mRS 0-2 at 90 days with IV tPA
or mechanical thrombectomy by treatment delay
Emberson et al. Lancet 2014
Onset to IV tPA infusion or to reperfusion time in thrombectomy trials
* 2.0 hours corresponds to the theoretical shortest delay in local hospitals
IV tPA*
REVASCAT
MR CLEAN
SWIFT RIME
EXTEND – IA &
ESCAPE
4·2

Bridging or rescue
RCT OTG IV tPA Ischemic
penumbra
Outcome
Mrs 0-2 TvsC
MR CLEAN 260 min failure NA 33% vs 19%
ESCAPE 185 min bridging Aspect 6-10
good collaterals
53%vs 29%
EXTEND IA 250 min bridging Core < 70ml
(Tmax 6 sec
71% vs 40%
SWIFT PRIME 224mim bridging Aspect 6-10
(MRI-CTP)
60 vs 35%
REVASCAT 269 min failure Aspect 6-10 44 %vs 28 %

Patients selection

Imaging selection: outcome
MR Clean
ESCAPE
Goyal M et al. N Engl J Med 2015; ePub February 11
Berkhemer OA et al. N Engl J Med 2015;372:11-20
Saver J et al. N Engl J Med 2015, ePub April 17
Jovin T et al. N Engl J Med 2015, ePub April 17
SWIFT PRIME
REVASCAT

Collateral circulation

Collaterals at Angiography and Outcomes in the Interventional Management of Stroke (IMS) III Trial
Stroke Volume 45(3):759-764 February 24, 2014
RE-evaluation of IMS3 patients where the collateral circulation was assessed (83%)
The presence of good collaterals was significantly correlated to the recanalization
Significant predictor of favorable clinical outcome after 3 months

ESCAPE


Careggi Collateral Score
(CCS)
Semi-quantitative
Analysis (EXTENSION of
Collateral circulation)


Variability of the mismatch and extension of ischemic core in relation to
different grades of efficacy of collateral circulation
A B C c
E
p Ip
c c
I
p I
p
E
p E
p
CCS
0-1
CC
S2
CCS
3-5
C: core ;
Ip : Internal penumbra (savageable by recanalization);
Ep : External penumbra (savageable by collaterals)
Mangiafico S, Consoli A. CAPRI Study
Liebeskind, Stroke 2014

metanalysis

Balami et al., International Journal of Stroke 2015







data


Clinical Outcome for each recanalization grade and occlusion site
(Outcome Curves: mRS0-2 and mRS6 for each recanalization grade)
Anterior circulation Analysis of 22.02-16


Combined Treatment - only TM: Recanalization rates (TICI)
No significant differences in recanalization rate
Analisi del 22.02-16

Anterior circulation
TM
vs
tPA ev+TM
outcome / timing
time of end of the procedure
300 min
Analysis of 22.02-16

conclusions
• Trials and data collected from da studies and registries confirm that the favorable clinical outcome after thrombectomy depends on the recanalization grade, the time to reperfusion (better if within 240 min from the onset) and an appropriate patient selection (core extension and collateral circulation)
• In occlusions of the anterior circulation the endovascular treatment should be started withour waiting for a clinical improvement after IV tPA (bridging, no rescue)

Intracranial
revascularization in Acute
Stroke: Data and Trials
Session 4: Target Stroke




![Left Atrial Size and Function · congestive heart failure (CHF), stroke (cerebrovascular accident [CVA]), transient ischemic attack, acute myocar-dial infarction (AMI), coronary revascularization,](https://static.fdocuments.in/doc/165x107/5f0d41d97e708231d43972aa/left-atrial-size-and-function-congestive-heart-failure-chf-stroke-cerebrovascular.jpg)













