Cervical Spine Stenosis - Lieberman's eRadiology Learning Sites
Eric Swart MS3Gillian Lieberman, MD
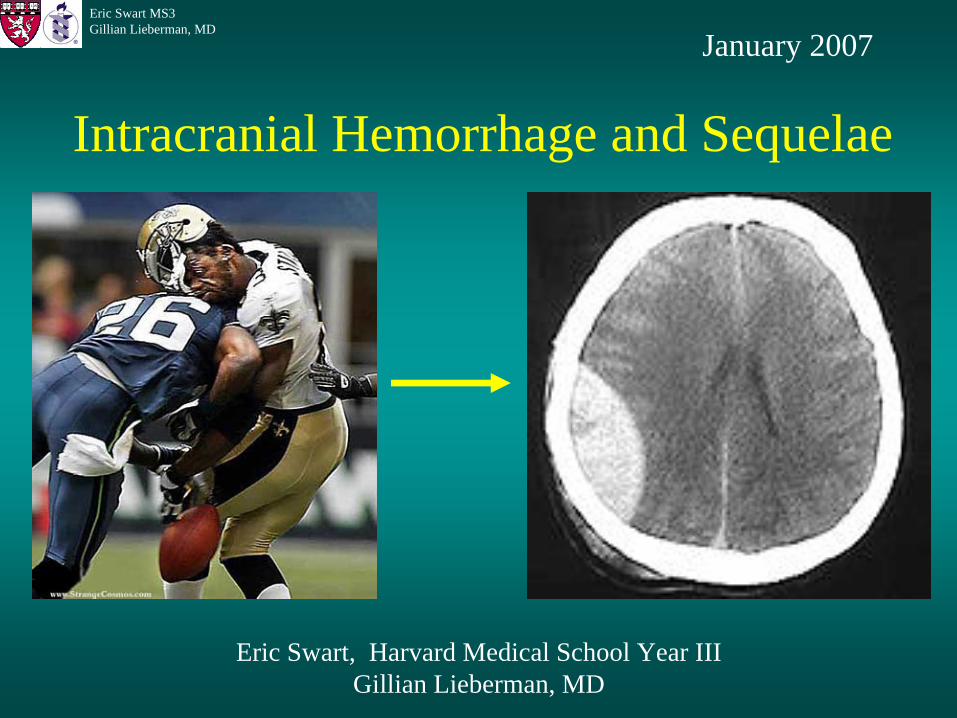
Intracranial Hemorrhage and Sequelae
Eric Swart, Harvard Medical School Year III Gillian Lieberman, MD
January 2007
2
Eric Swart MS3Gillian Lieberman, MD
Agenda
• Patient Presentation
• Brief review of neuroanatomy
• Causes of hemorrhage and radiologic appearance
• Imaging principles of blood
• Physiology and consequences of hemorrhage
3
Eric Swart MS3Gillian Lieberman, MD
Patient 1• 83 y/o M with IDDM, CAD, and CRI presents
s/p fall in home with RU extremity redness.
• Further history reveals multiple minor falls over past month associated with dizziness and minor head trauma.
• Current medications include ASA
• Any imaging?
4
Eric Swart MS3Gillian Lieberman, MD
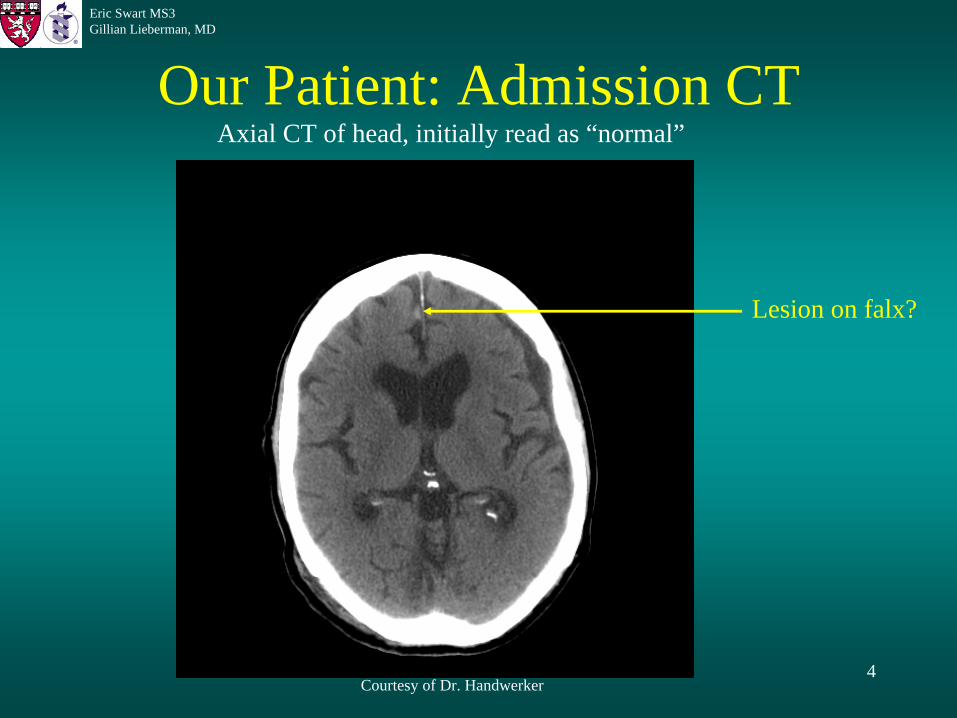
Our Patient: Admission CT
Courtesy of Dr. Handwerker
Axial CT of head, initially read as “normal”
Lesion on falx?
5
Eric Swart MS3Gillian Lieberman, MD
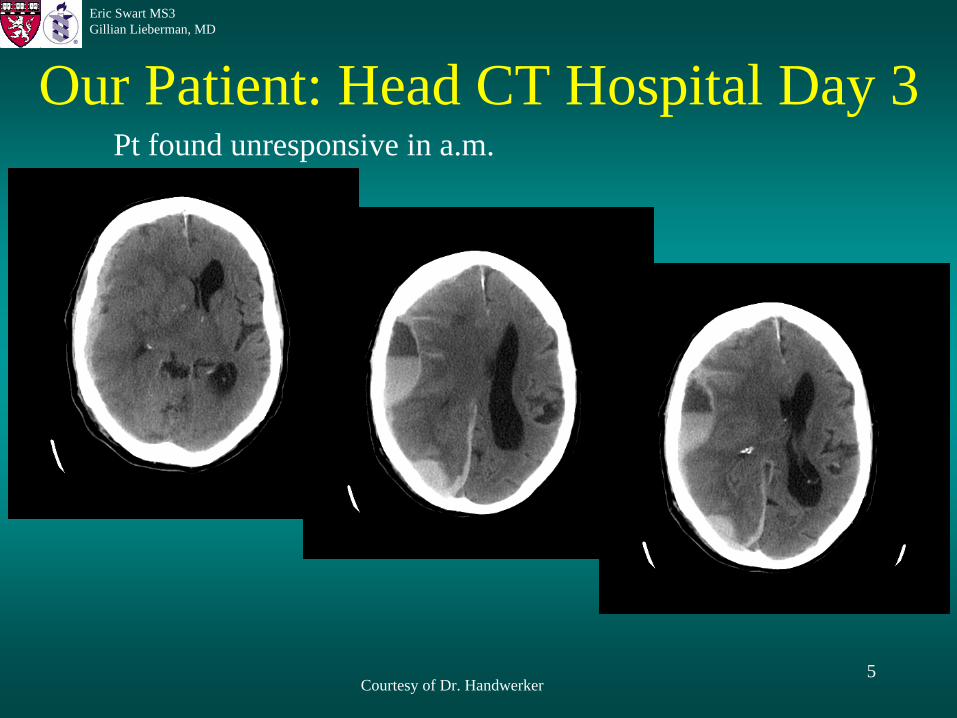
Our Patient: Head CT Hospital Day 3
Courtesy of Dr. Handwerker
Pt found unresponsive in a.m.

6
Eric Swart MS3Gillian Lieberman, MD
Our Patient: Subdural Hematoma
Layering Hemorrhage
Possible Subarachnoid Compression
of ventricles
Midline shift
Courtesy of Dr. Handwerker
7
Eric Swart MS3Gillian Lieberman, MD
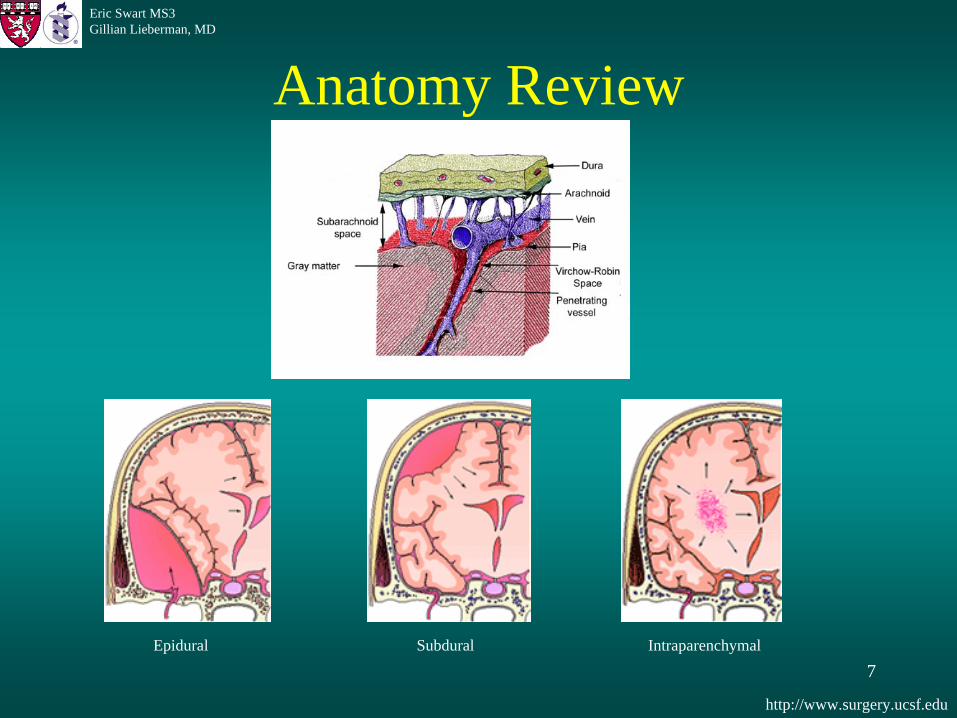
Anatomy Review
http://www.surgery.ucsf.edu
Epidural Subdural Intraparenchymal
8
Eric Swart MS3Gillian Lieberman, MD
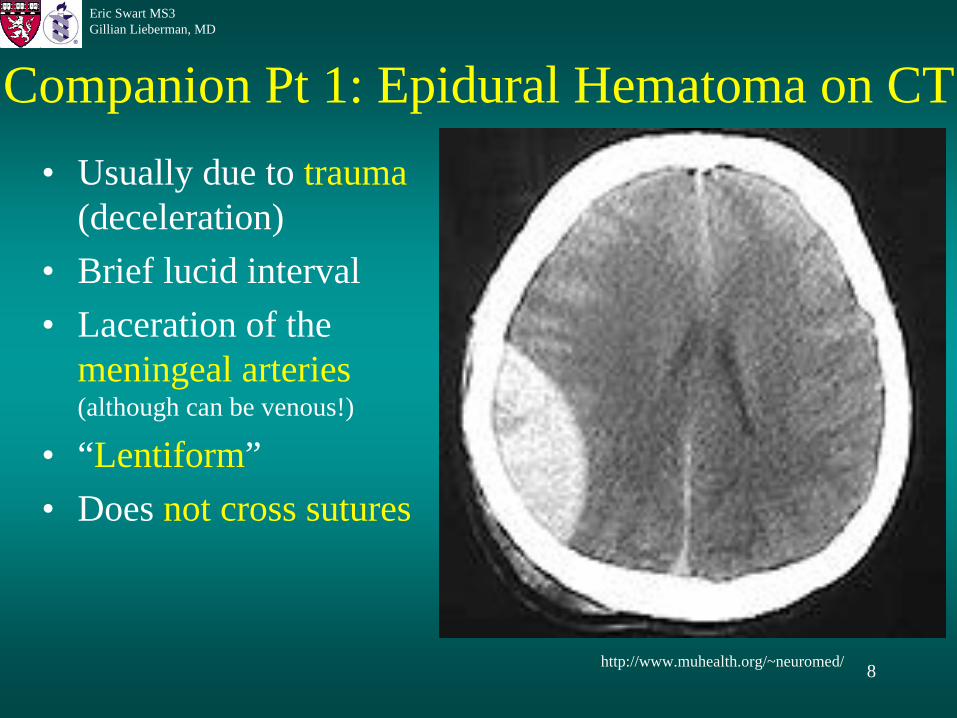
Companion Pt 1: Epidural Hematoma on CT• Usually due to trauma
(deceleration) • Brief lucid interval• Laceration of the
meningeal arteries (although can be venous!)
• “Lentiform”• Does not cross sutures
http://www.muhealth.org/~neuromed/
9
Eric Swart MS3Gillian Lieberman, MD
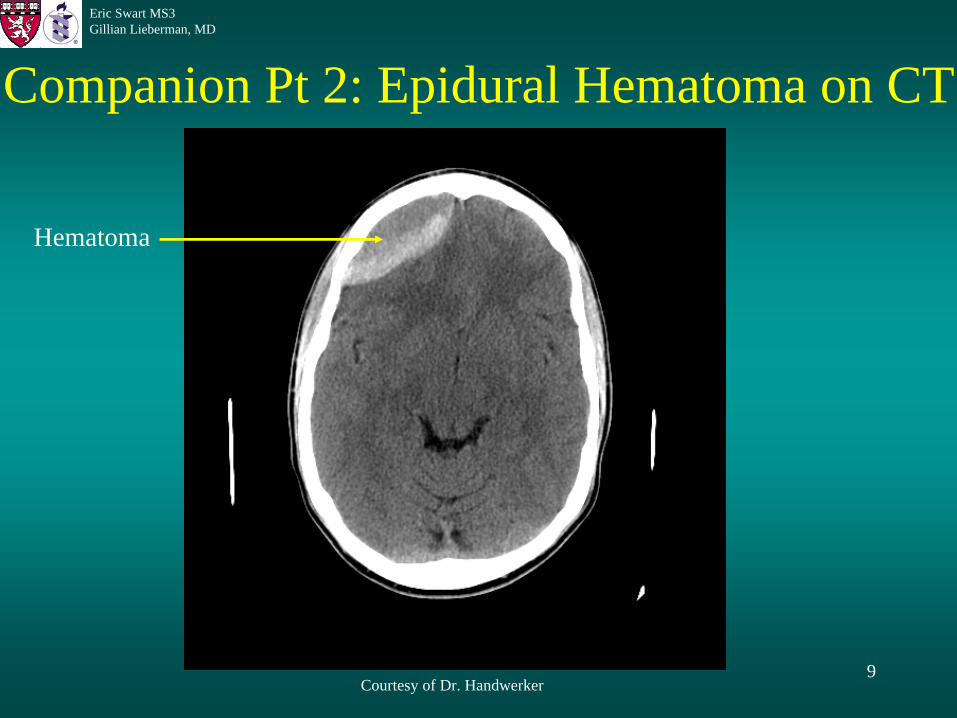
Companion Pt 2: Epidural Hematoma on CT
Courtesy of Dr. Handwerker
Hematoma
10
Eric Swart MS3Gillian Lieberman, MD
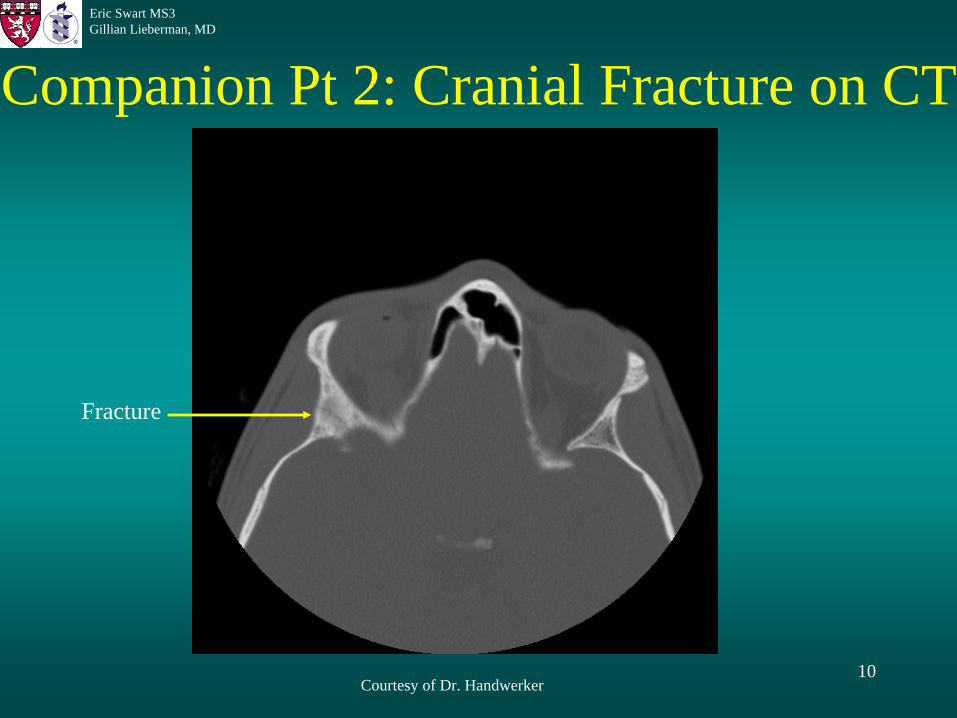
Companion Pt 2: Cranial Fracture on CT
Courtesy of Dr. Handwerker
Fracture
11
Eric Swart MS3Gillian Lieberman, MD
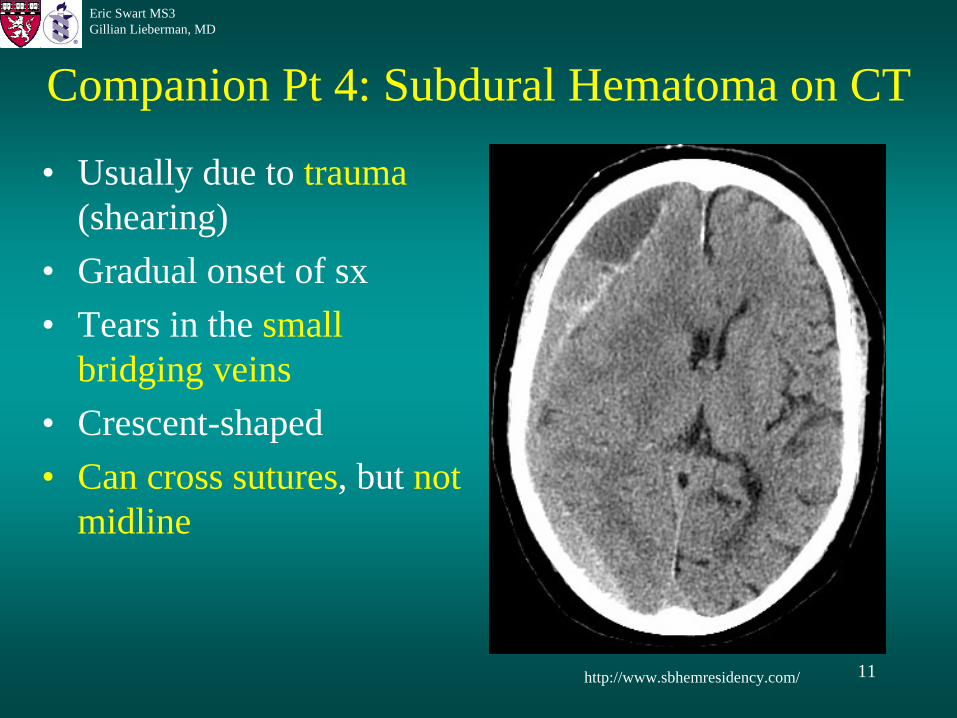
Companion Pt 4: Subdural Hematoma on CT
• Usually due to trauma (shearing)
• Gradual onset of sx• Tears in the small
bridging veins• Crescent-shaped• Can cross sutures, but not
midline
http://www.sbhemresidency.com/
12
Eric Swart MS3Gillian Lieberman, MD
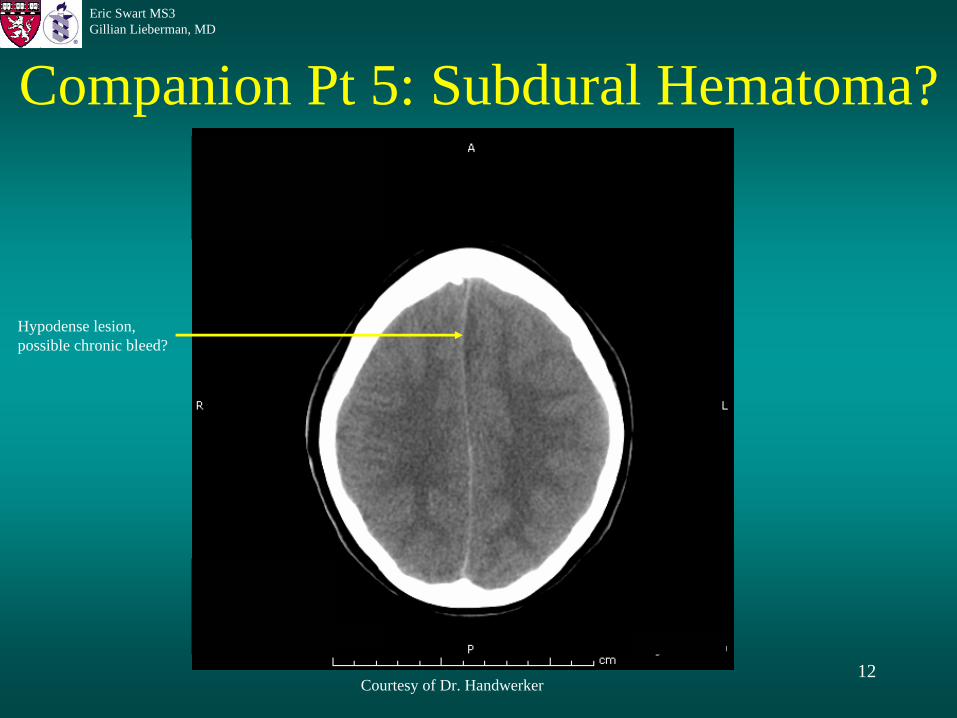
Companion Pt 5: Subdural Hematoma?
Courtesy of Dr. Handwerker
Hypodense lesion, possible chronic bleed?
13
Eric Swart MS3Gillian Lieberman, MD
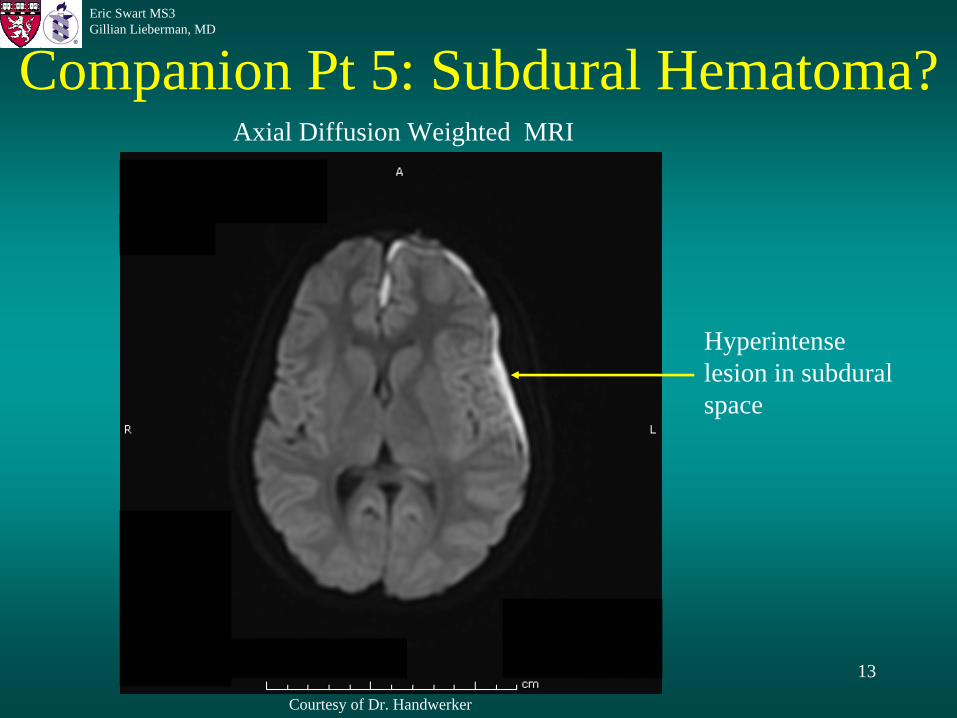
Companion Pt 5: Subdural Hematoma?
Courtesy of Dr. Handwerker
Axial Diffusion Weighted MRI
Hyperintense lesion in subdural space
14
Eric Swart MS3Gillian Lieberman, MD
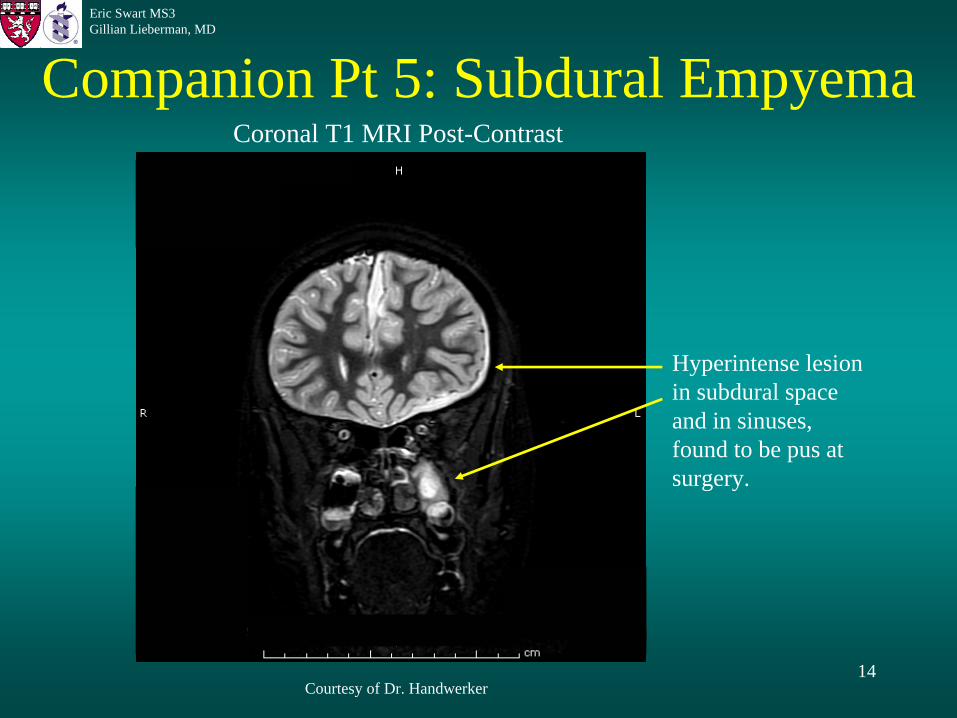
Companion Pt 5: Subdural Empyema
Courtesy of Dr. Handwerker
Coronal T1 MRI Post-Contrast
Hyperintense lesion in subdural space and in sinuses, found to be pus at surgery.
15
Eric Swart MS3Gillian Lieberman, MD
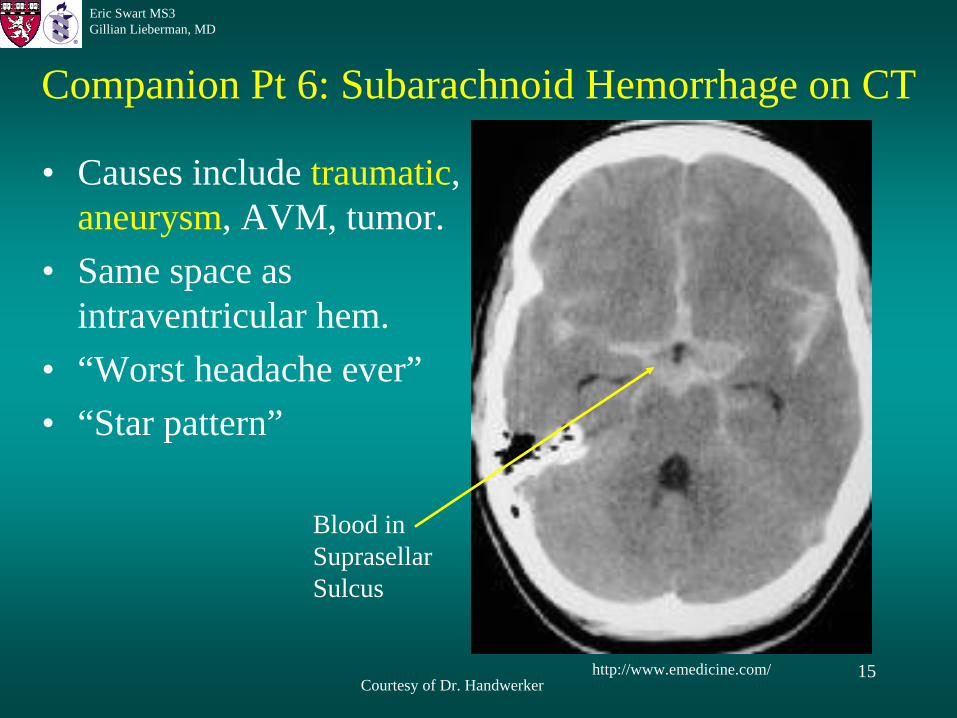
Companion Pt 6: Subarachnoid Hemorrhage on CT
• Causes include traumatic, aneurysm, AVM, tumor.
• Same space as intraventricular hem.
• “Worst headache ever”• “Star pattern”
http://www.emedicine.com/Courtesy of Dr. Handwerker
Blood in Suprasellar Sulcus
16
Eric Swart MS3Gillian Lieberman, MD
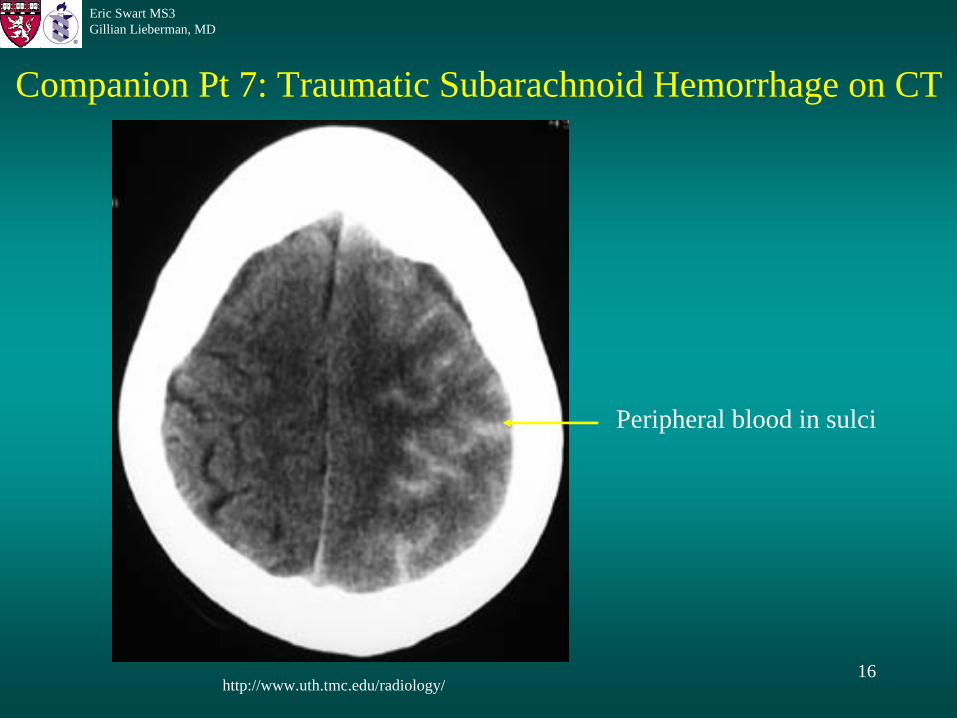
Companion Pt 7: Traumatic Subarachnoid Hemorrhage on CT
http://www.uth.tmc.edu/radiology/
Peripheral blood in sulci
17
Eric Swart MS3Gillian Lieberman, MD
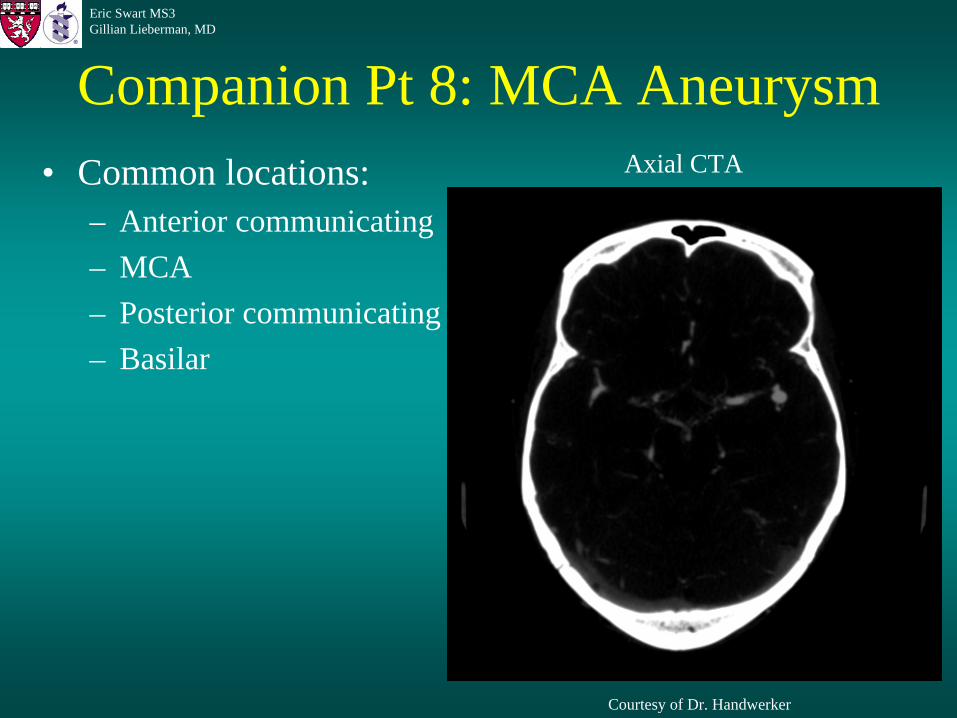
Companion Pt 8: MCA Aneurysm• Common locations:
– Anterior communicating– MCA– Posterior communicating– Basilar
Courtesy of Dr. Handwerker
Axial CTA
18
Eric Swart MS3Gillian Lieberman, MD
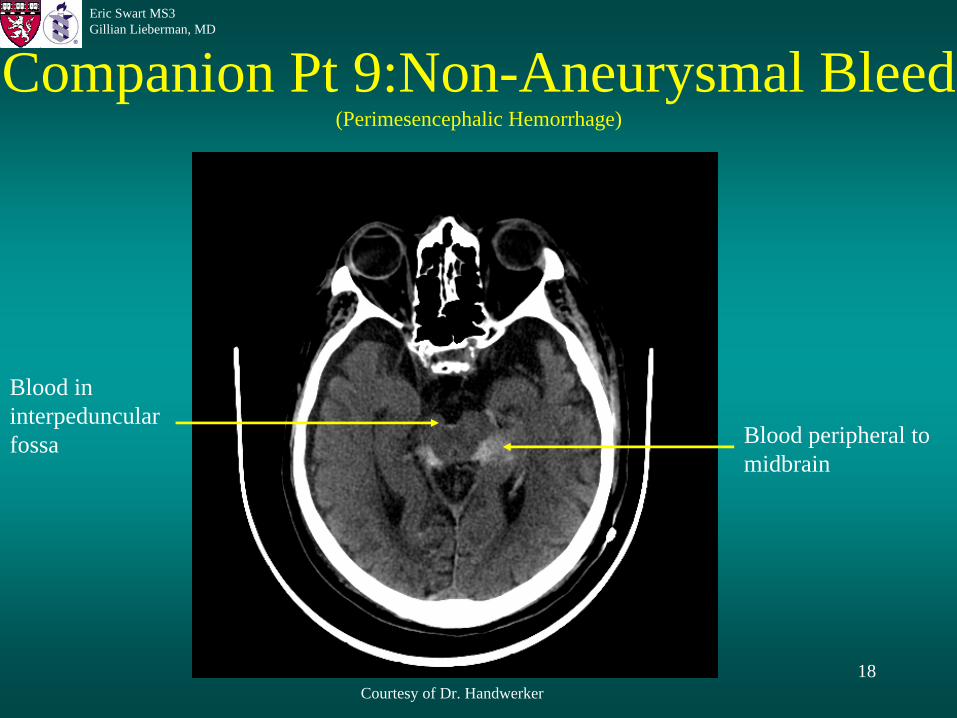
Companion Pt 9:Non-Aneurysmal Bleed (Perimesencephalic Hemorrhage)
Courtesy of Dr. Handwerker
Blood in interpeduncular fossa Blood peripheral to
midbrain
19
Eric Swart MS3Gillian Lieberman, MD
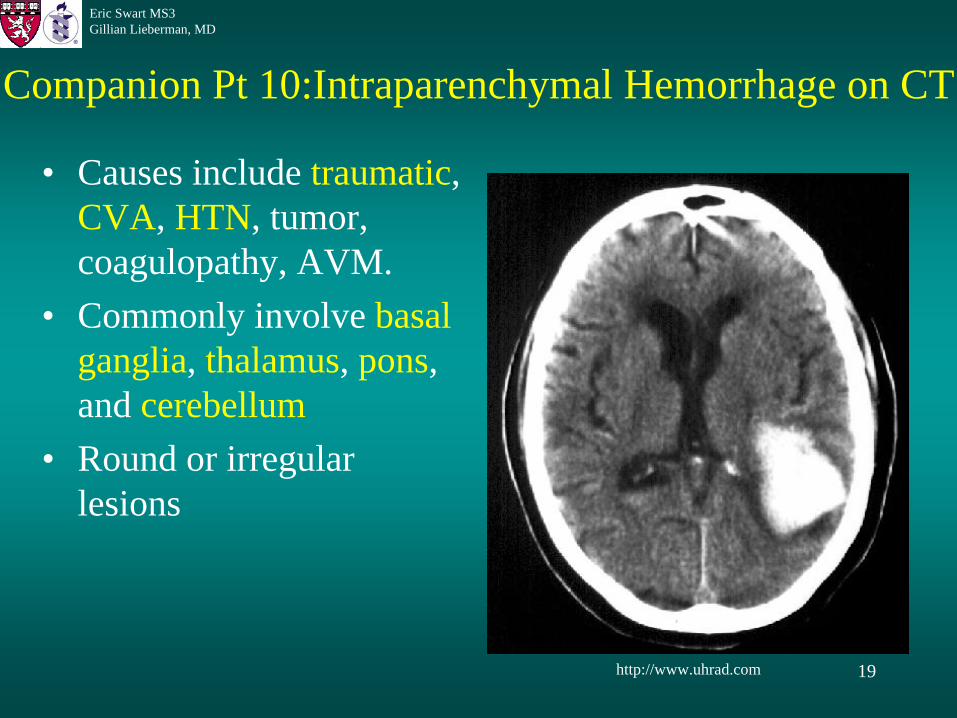
Companion Pt 10:Intraparenchymal Hemorrhage on CT
• Causes include traumatic, CVA, HTN, tumor, coagulopathy, AVM.
• Commonly involve basal ganglia, thalamus, pons, and cerebellum
• Round or irregular lesions
http://www.uhrad.com

20
Eric Swart MS3Gillian Lieberman, MD
Diffuse Axonal Injury• Results from shearing trauma• Diffuse, bilateral injury at the grey-white matter
junction• CT: multiple small intraparenchymal hem.• MRI may be more sensitive

21
Eric Swart MS3Gillian Lieberman, MD
Courtesy of Dr. Kang
Companion Pt 11: Diffuse Axonal Injury on CT

22
Eric Swart MS3Gillian Lieberman, MD
30 Days in the Life of a Hemorrhage• Five distinct stages of a intracranial hemorrhage:
– Hyperacute: <12 hours– Acute: 12 h – 2 days– Early subacute: 2 – 7 days– Late subacute: 8 days – 1 month– Chronic >1 month – years
• Imaging principles:– Clot density changes dominate on CT– Changes in hemoglobin dominate on MR

23
Eric Swart MS3Gillian Lieberman, MD
CT Appearance of Aging Hemorrhage• Clot is initially liquid mix of RBC’s, WBC’s,
platelets, and serum.– hyperacute = isointense
• As the clot contracts, the core becomes denser while the surrounding areas become edematous. – acute – early subacute = hyperintense
• Over time, the clot degrades, and the edema subsides.– late subacute – chronic = isointense-hypointense,
may enhance with contrast due to BBB breakdown
24
Eric Swart MS3Gillian Lieberman, MD
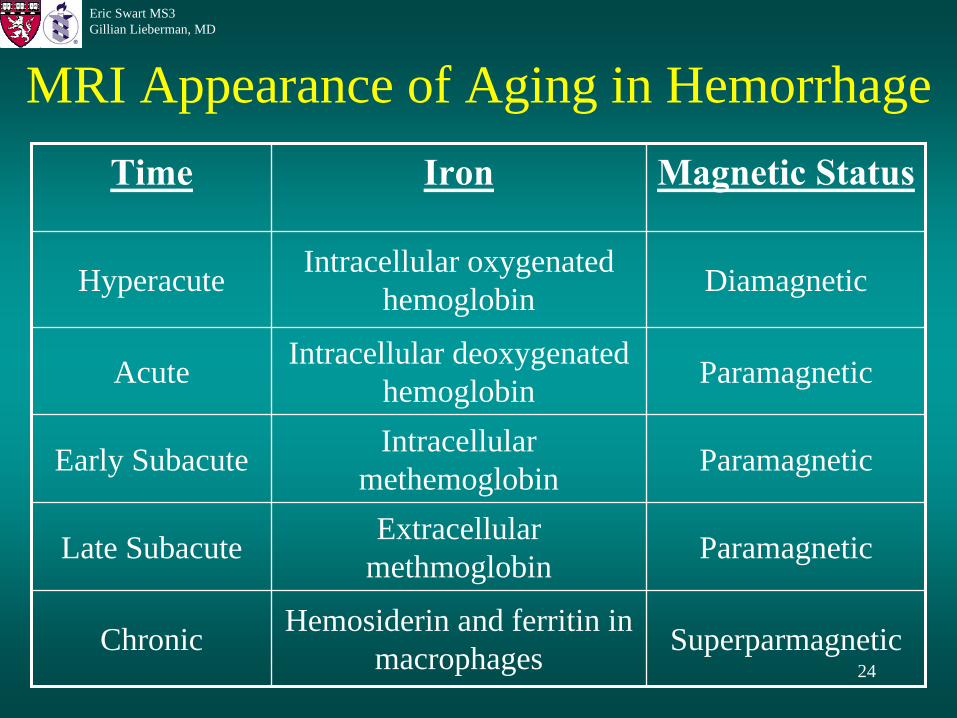
MRI Appearance of Aging in HemorrhageTime Iron Magnetic Status
Hyperacute Intracellular oxygenated hemoglobin Diamagnetic
Acute Intracellular deoxygenated hemoglobin Paramagnetic
Early Subacute Intracellular methemoglobin Paramagnetic
Late Subacute Extracellular methmoglobin Paramagnetic
Chronic Hemosiderin and ferritin in macrophages Superparmagnetic

25
Eric Swart MS3Gillian Lieberman, MD
Summary: Appearance of Hemorrhage on CT and MRI
Time CT MR T1 MR T2
Hyperacute:< 12 hours – – ↑
Acute:12 h – 2 days ↑ – ↓
Early subacute:2 – 7 days ↑ ↑ ↓
Late subacute:8 days – 1 month – ↑ ↑
Chronic:>1 month – years –
↓ ↓ ↑
= Hyperintense = Isointense = Hypointense
26
Eric Swart MS3Gillian Lieberman, MD
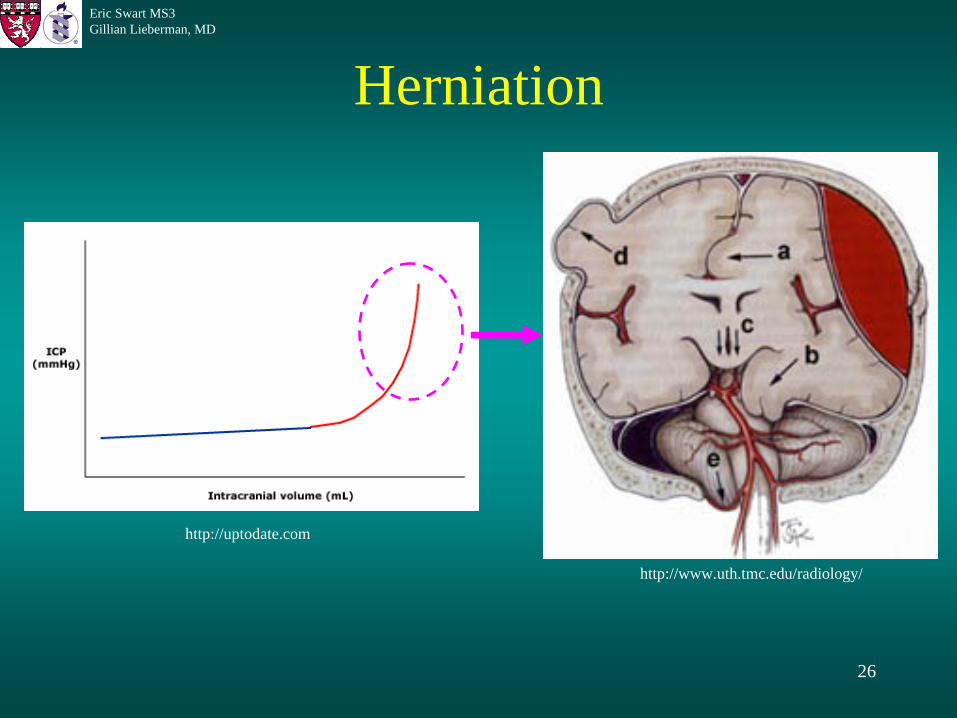
Herniation
http://uptodate.com
http://www.uth.tmc.edu/radiology/
27
Eric Swart MS3Gillian Lieberman, MD
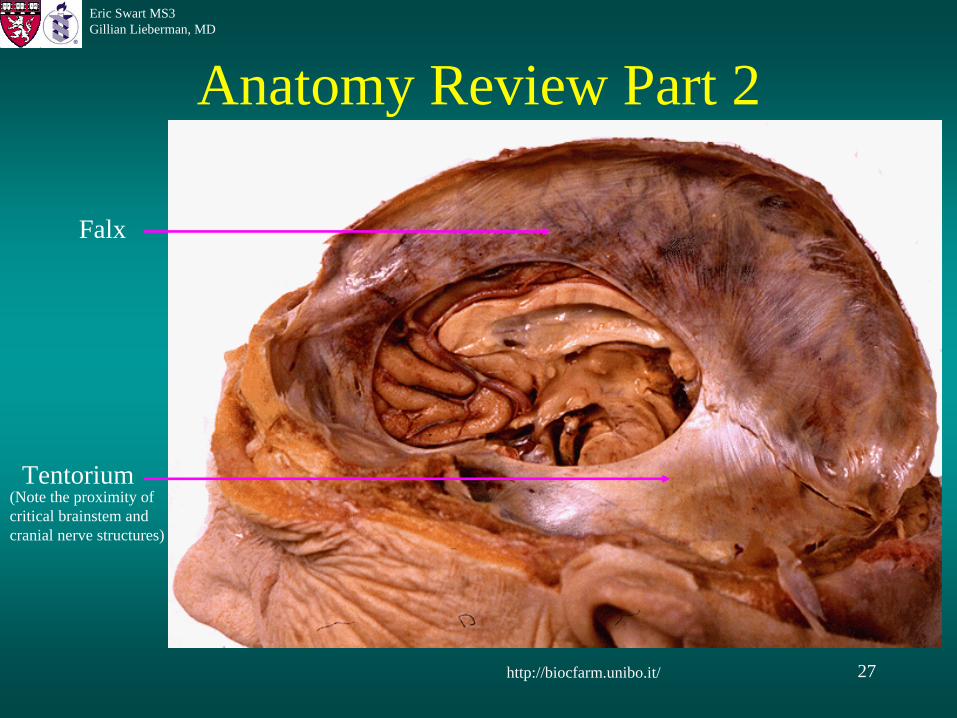
Anatomy Review Part 2
http://biocfarm.unibo.it/
Tentorium
Falx
(Note the proximity of critical brainstem and cranial nerve structures)
28
Eric Swart MS3Gillian Lieberman, MD
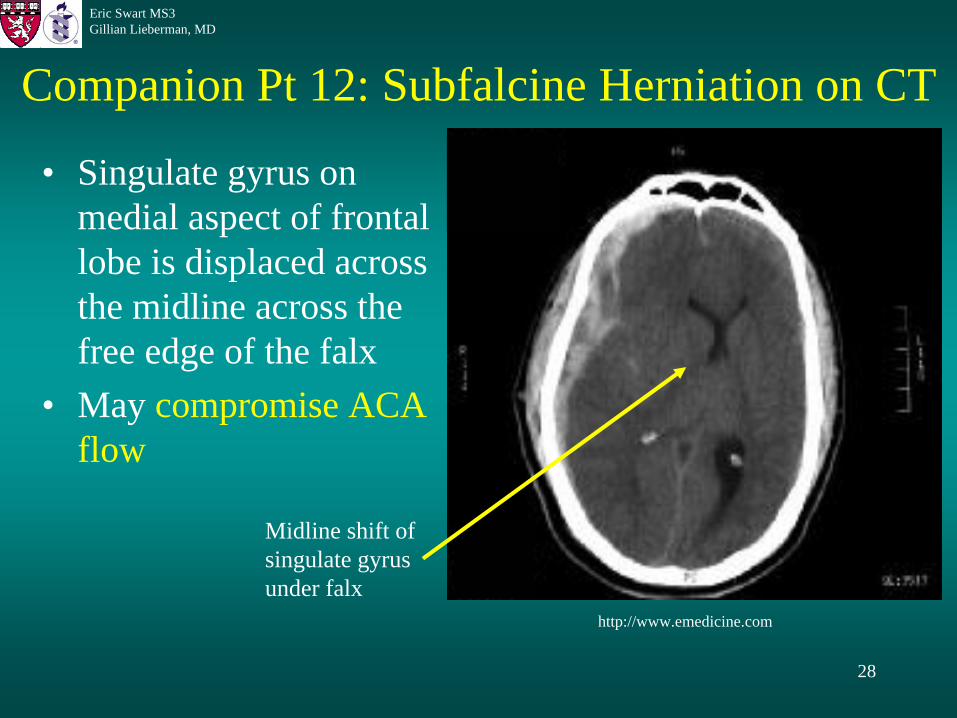
Companion Pt 12: Subfalcine Herniation on CT
• Singulate gyrus on medial aspect of frontal lobe is displaced across the midline across the free edge of the falx
• May compromise ACA flow
http://www.emedicine.com
Midline shift of singulate gyrus under falx
29
Eric Swart MS3Gillian Lieberman, MD
Transtentorial Herniation• Medial aspect of temporal lobe (uncus) migrates
across tentorium• Causes 3rd nerve compression• Can also be ascending herniation, most often
from tumor in posterior fossa
30
Eric Swart MS3Gillian Lieberman, MD
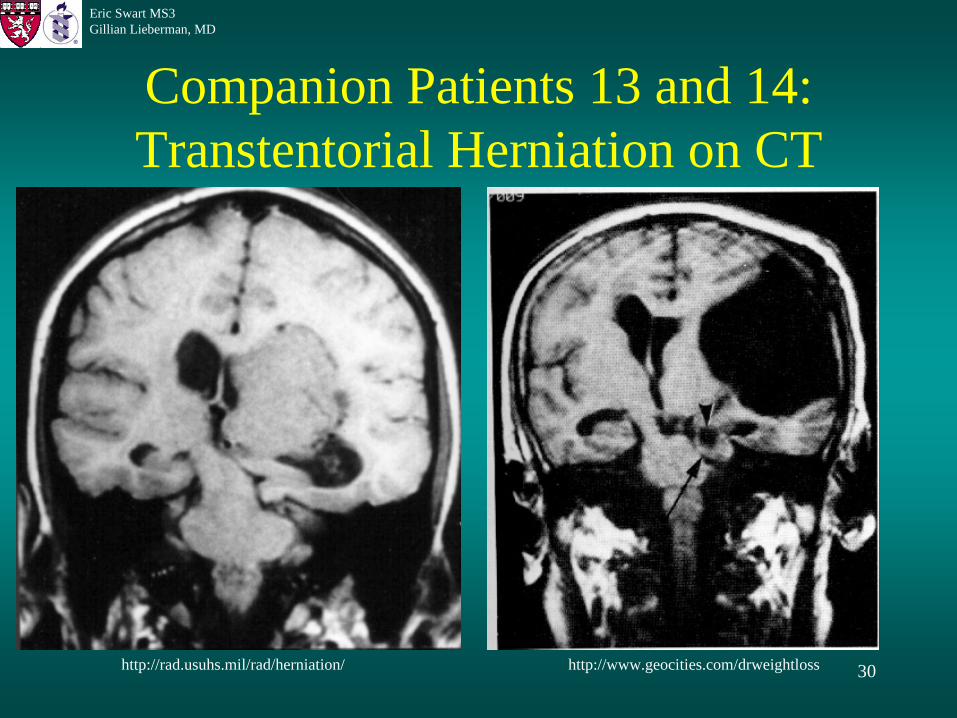
Companion Patients 13 and 14: Transtentorial Herniation on CT
http://www.geocities.com/drweightlosshttp://rad.usuhs.mil/rad/herniation/
31
Eric Swart MS3Gillian Lieberman, MD
Central Herniation• Diffuse increase in ICP displaces each cerebral
hemisphere downward through tentorium• Compresses upper brainstem
32
Eric Swart MS3Gillian Lieberman, MD
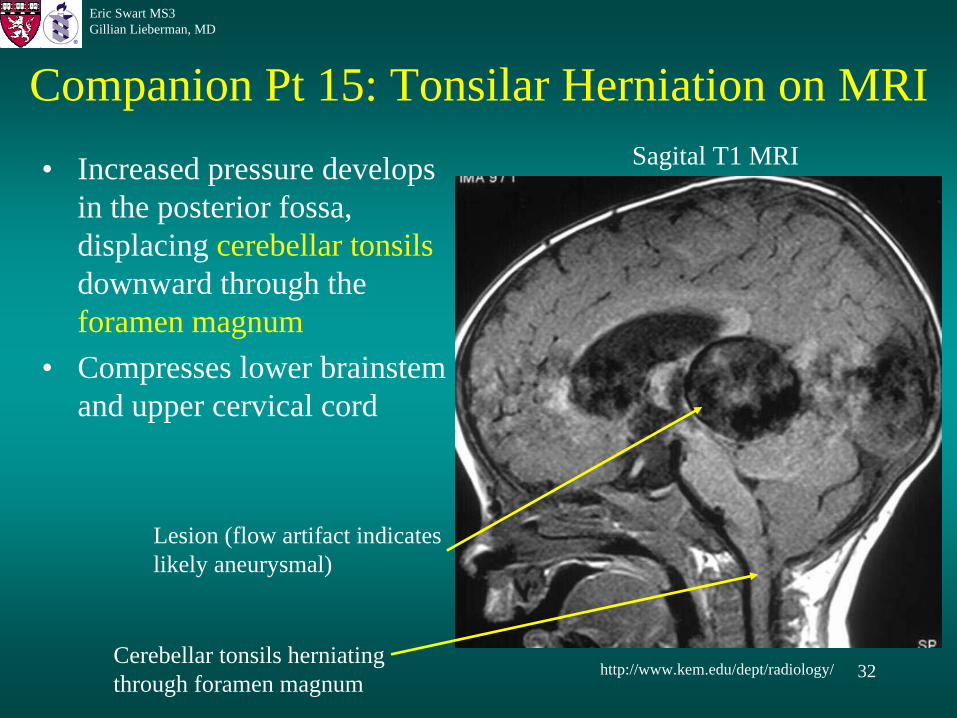
Companion Pt 15: Tonsilar Herniation on MRI
• Increased pressure develops in the posterior fossa, displacing cerebellar tonsils downward through the foramen magnum
• Compresses lower brainstem and upper cervical cord
http://www.kem.edu/dept/radiology/Cerebellar tonsils herniating through foramen magnum
Lesion (flow artifact indicates likely aneurysmal)
Sagital T1 MRI
33
Eric Swart MS3Gillian Lieberman, MD
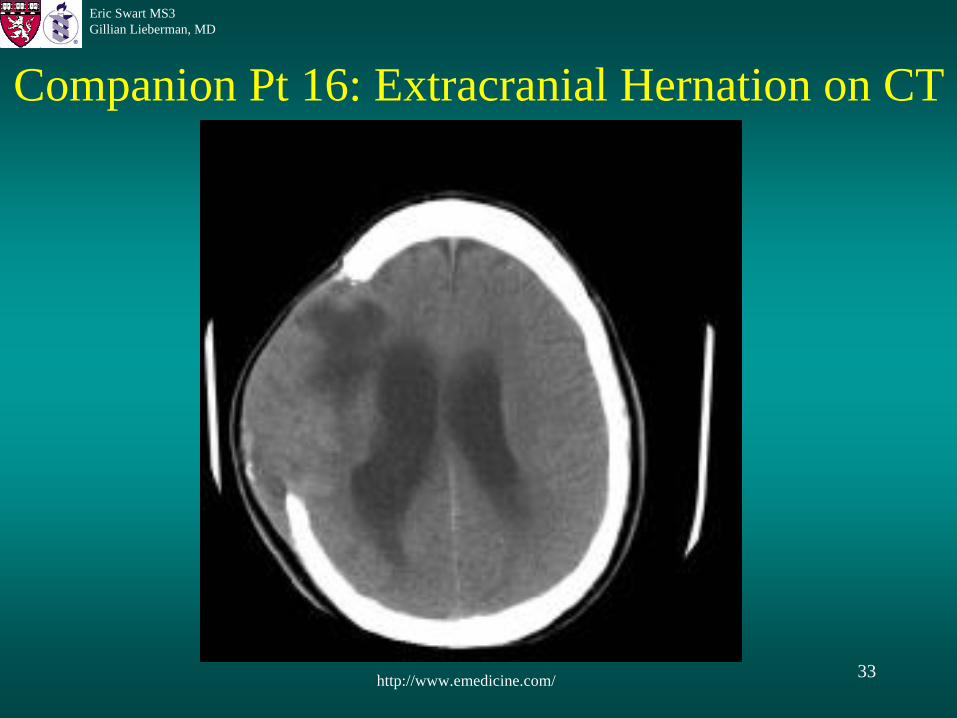
Companion Pt 16: Extracranial Hernation on CT
http://www.emedicine.com/
34
Eric Swart MS3Gillian Lieberman, MD
Summary• Intracranial hemorrhage is defined by its
location with respect to the meninges– Trauma is usually the most common cause
• Hemorrhage undergoes a predictable temporal sequence of changes that can be seen on MR and CT and used to estimate the age of the bleed.
• An increase in mass can cause increased ICP and can result in extremely dangerous herniations.– Dural reflections are commonly involved
35
Eric Swart MS3Gillian Lieberman, MD
AcknowledgementsThanks to:• Gillian Lieberman, MD• Jason Handwerker, MD• James Kang, MD• Pamela Lepkowski• Larry Barbaras

36
Eric Swart MS3Gillian Lieberman, MD References
• Huisman, TA. Intracranial hemorrhage: ultrasound, CT, and MRI findings.
European Radiology 2005; 15:434-440.
• Parizel
PM, Makkat
S, Van Miert
E, van Goethem
JW, van den Hauwe
L, De Schepper
AM. Intracranial hemorrhage: principles of CT and MRI interpretation. European Radiology 2001; 11:1770-1783
• Ruigrok, YM, Rinkel, GJ, Buskens, E, et al. Perimesencephalic
hemorrhage and CT angiography: A decision analysis. Stroke 2000; 31:2976.
• Noveline, RA. Squire’s Fundamentals of Radiology 6th
edition. Cambridge, 2004.• Grossman RI, Yousem
DM. Neuroradiology: The Requisites 2nd
edition. 2003.• Nolte, J. The Human Brain: An Introduction to Its Functional Anatomy 5th
edition. 2002.• Moore, KL, Daley, AF. Clinically Oriented Anatomy 4th
edition. 1999.• http://uptodate.com• http://www.surgery.ucsf.edu• http://www.muhealth.org/~neuromed/• http://www.sbhemresidency.com/• http://www.uth.tmc.edu/radiology/• http://emedicine.com• http://www.uhrad.com• http://biocfarm.unibo.it/• http://rad.usuhs.mil/rad/herniation/• http://www.geocities.com/drweightloss• http://www.kem.edu/dept/radiology/