Intestinal obstruction
126
-
Upload
dr-armaan-singh -
Category
Health & Medicine
-
view
148 -
download
5
Transcript of Intestinal obstruction
• Intestinal obstruction is a significant mechanical impairment or complete arrest of the passage of contents through the intestine. Intestinal obstructions account for 20% of all acute surgical admissions. Mortality and morbidity are dependent on the early recognition and correct diagnosis of obstruction. If untreated, strangulated obstructions cause death in 100% of patients. However, the mortality rate decreases to 8% with prompt surgical intervention (Vicky P. Kent, RN, PhD, CNE, 2009).
• Nanay Ganda, 84 years old, was admitted last December 8, 2010 at General Santos Doctors’ Hospital under the care of Dr. Albano, had complaints of inability to defecate by about 4 days. A background of one year history of intermittent abdominal pain with bloating was claimed by the patient.
• The impression to the result of the ultrasound of her whole abdomen is to consider ileus; partial obstruction and fecal stasis. Dr. Albano believed that the symptoms being manifested were results of a disorder she has in a long time. Since they weren’t able to have that checked and it wasn’t figured out earlier, the signs become more evident now. It’s also because these manifestations develop and progresses relatively slowly. It was then that the physician decided to let the patient undergo exploratory lap to detect what really had cause the obstruction.
• It was December 13, 2010 when the surgeon discovered a tumor at the site of the obstruction particularly at the descending colon and immediately removed it. The found tumor was then subjected for biopsy.
Intestinal obstruction is a significant mechanical impairment or complete arrest of the passage of contents through the intestine. Overall, the most common causes of mechanical obstruction are adhesions, hernias, and tumors. Other general causes are diverticulitis, foreign bodies (including gallstones), intussusceptions (bowel folding into itself), and volvulus (twisting of the colon).
The symptoms usually include cramping pain, vomiting, constipation, and lack of flatus. Diagnosis is clinical which is confirmed by abdominal x-rays. Treatment is fluid resuscitation, nasogastric suction, and, in most cases, surgery.

Intestinal obstructions account for 20% of all acute surgical admissions. Mortality and morbidity are dependent on the early recognition and correct diagnosis of obstruction. If untreated, strangulated obstructions cause death in 100% of patients. However, the mortality rate decreases to 8% with prompt surgical intervention (Vicky P. Kent, RN, PhD, CNE, 2009).
In the course of this study, 84 year-old, Nanay Ganda, admitted last December 8, 2010 at General Santos Doctors’ Hospital under the care of Dr. Albano, had complaints of inability to defecate by about 4 days. A background of one year history of intermittent abdominal pain with bloating was claimed by the patient
Because of this, Dr. Albano believed that the disorder had a gradual onset and its symptoms were experienced timely yet later with age. The patient recently claimed that pain usually starts at the right upper quadrant and radiates all throughout the abdomen. Abdominal distention was also observed with rounded asymmetric contour of the abdomen. The bowel sounds were normal at first and becomes quiet later on. She also had episodes of vomiting.
Last December 13, 2010, the patient had undergone exploratory laparotomy and the surgeon found out that there was a presence of tumor and immediately removed it. However, the result of the biopsy has not been seen. She also had a colostomy to eliminate waste products until such time the colon heals.
The study focuses on the nature and possible causes which may lead people to experience this obstruction. The patient is in her older age and same with other elders who have the same case as Nanay Ganda, it is difficult in their part to deal with the disorder. Since they are older, they need more attention and care from the medical team, and particularly, from their significant others.
It is for this reason why the student nurses decided to have the case. To give awareness and knowledge of what is the disorder all about and how can somebody be of help to manage patients with this case especially the older ones.
This will be a big implication in the medical and nursing care since it is a challenge to diagnose a bowel obstruction. The keys to successful management are to identify signs and symptoms that may present very subtly at first, followed by a commitment to help the patient before the condition becomes aggravated. Whatever the treatment, participation in management and postoperative care is vital. Staying current with new findings and methods is the best course.


General Objectives:
Comprehend and recognize salient points that are important to remember when dealing with patients who manifested intestinal obstruction; its nature, causes, clinical manifestations, management, and prognosis This is to enhance the students’ and other health care providers’ awareness, knowledge, and understanding of it in order to promote health, prevent the disease and help manage patients with this kind of disorder to recover.
Specific Objectives:
Present the introduction of the studied disease;State the purpose of the study;Present the obtained initial database of the patient;Present the nursing history including the past and present illness of the patient, as well as his activities of daily living;
Present the patient’s cephalocaudal assessment;
Identify the anatomy and physiology of the system involved (Gastrointestinal System);
Trace the pathophysiology of the disorder process through an illustration and explanation;
Compare the clinical manifestations of the disorder based on the theories and actual observations;
Explain the assessment and diagnostic findings;
Interpret the laboratory results and the nursing responsibilities;
Discuss the medical and nursing management for the said condition.
Outline the drug study from the patient’s medication;
State the discharge planning of the patient;
List the health teachings given to the patient;
State the prognosis of the disease;
Enumerate the problem list;
Present the Gordon’s Functional Pattern of the patient; and
Present the nursing care plan made for the patient.

Name: Nanay Ganda
Age: 84 years old
Sex: Female
Address: Block 17 Lot 14 Gensanville Subd., Bula, GSC
Religion: Roman Catholic
Civil Status: Married
Birthdate: September 12, 1926
Birthplace: Bajada, Davao City
Room: 242 A and 242 B
Date of Admission: December 8, 2010
Attending Physician: Dr. Albano
Chief Complaints: Generalized Abdominal Pain; Inability to defecate; Abdominal distention
Admitting Diagnosis: T/C Ileus Partial Obstruction; Fecal Stasis
Occupation/Source of Income : Housewife

A. History of Present Illness
4 days before the admission, Nanay Ganda experienced inability of defecating. She also recalled and claimed that it’s approximately a year that she has been suffering from intermittent pain in the abdominal area. She cited that pain starts at the right upper quadrant and radiates all throughout the abdomen.
Nanay Ganda and her children then decided to let her be seen by a physician. They scheduled the check-up last December 8, 2010. According to them, the physician advised Nanay Ganda to be admitted on that same day, after doing assessment and series of laboratory tests such as complete blood count and fluid serum. After 5 days being at the hospital, she had episodes of vomiting.

The impression to the result of the ultrasound of her whole abdomen is to consider ileus; partial obstruction and fecal stasis. Dr. Albano believed that the symptoms being manifested were results of a disorder she has in a long time. Since they weren’t able to have that checked and it wasn’t figured out earlier, the signs become more evident now. It’s also because these manifestations develop and progresses relatively slowly.
It was then that the physician decided to let the patient undergo exploratory lap to detect what really had cause the obstruction. It was December 13, 2010 when the surgeon discovered a tumor at the site of the obstruction particularly at the descending colon and immediately removed it. The found tumor was then subjected for biopsy.
B. Past Medical History
•Immunization and Childhood Illness
The patient can only recall being immunized with BCG and OPV. She had a history of having chicken pox infection when she was on her 1st year high school. She also experienced cough and colds, fever, diarrhea, constipation, sore throat, rashes, and nausea and vomiting.
• Compliance to Health Management
Nanay Ganda rarely visits a doctor to have a check-up. However, she is using herbal medicines since her childhood days depending on what condition she has such as oregano, guava, bitter gourd, and ginger.
She also takes over the counter drugs and what she mentioned were Solmux, Neozep, Biogesic, Mefenamic acid, Bentyl, and Loperamide. She said that when she was still on her 30’s to 40’s, she is taking multivitamins which is Enervon and later on, she stopped taking it.
• Menarche
Her menarche started when she was in her 6th grade. She was 11 years old back then on the year 1938.
C. Family History
There is no known inherited condition present in her both paternal and maternal family. She’s the first in their family to be experience intestinal obstruction.
D. Activities of Daily Living
•Personal Hygiene
The patient is able to bathe herself. She takes a bath everyday. According to her, before and after eating her meals, she only washes her hands with the use of water though sometimes, she can be able to use soap.
• Nutrition
Since she believes that eating fruits and vegetables is good for her and will be able to maintain her health, she doesn’t seek for medical assistance that much.
She eats her meals three times a day with snacks in between. She admitted that she only drinks 4-5 glasses of water a day which approximately is equal to 1.5L. She drinks coffee in the morning and afternoon. She claimed that she has allergies on food particularly shrimps.
• Elimination
She voids 4-5 times a day. Her urine color is yellow which is dark most of the times. There is no burning sensation/ pain felt during urination. She usually moves her bowel every morning with brown and formed stools. But recently, she is having difficulty in defecating.
• Rest and Sleep
She can sleep for 7-9 hours per night. Her earliest time in going to sleep is at 9:30 PM while the latest time in waking up is at 6:30 AM. She sometimes takes a nap at noon for about 1-3 hours. She said that she doesn’t experience any difficulties in going to sleep and doesn’t take any sedatives.
• Exercise
The patient ambulates within the house and does household chores. She also takes a walk at their subdivision in visiting their neighbors or buying at the store. She does simple exercises on the upper and lower extremities by means of shaking and stretching.
• Religion
She is a Roman Catholic who has a strong faith in God. She goes to the church with her youngest child and her grandchildren to attend the mass every Sunday. She always brings with her the rosary and always prays at night.
• Sexuality
The patient is married and has 4 children. She has no history of Sexually Transmitted Disease or any disease affecting her sexual organ. Her menarche was on the year 1938 when she was still 11 years old and she is now on her menopausal stage.
E. Hospitalization
This was her first hospitalization. She never experienced being hospitalized before because her parents would just bring her to manghihilot in their place.

Date Conducted: December 13 – 14, 2010
a.General Appearance
Pre-operative Phase
IVF of D5NM 1L x 160 hooked at her left cephalic vein
Vital Signs
12-13-10
8 AM 12PM Normal
T 360C 360C 36.5-37.50C
PR 93 bpm 94 bpm 60-100 bpm
RR 30 cpm 24 cpm 12-20 cpm
BP 110/80mmHg 110/80mmHg 90/60-120/90 mmHg
Thin Clean and well-groomed Conscious and coherent Tries to be calm and relaxed Facial grimacing at times Oriented to people, time, and place Frequent sighing
Post-operative Phase
IVF of PLR 1L x 8 hours as main line hooked at her left cephalic vein with a side drip of PNSS 500mL + 2 ampules Voltaren at 20cc/hr and an IVF of PNSS 1L x KVO hooked at her right cephalic vein with a side drip of 2units PRBC
Vital Signs
12-14-10
8 AM 12PM Normal
T 360C 36.50C 36.5-37.50C
PR 70 bpm 84 bpm 60-100 bpm
RR 18 cpm 18 cpm 12-20 cpm
BP 120/70 mmHg 100/60mmHg 90/60-120/90 mmHg
Uses oxygen via face mask at 3 LPM She has a nasogastric tube attached to a
drainage bottle Calm but shows evidence of weakness A colostomy is being attached to
colostomy bag at the left upper quadrant of her abdomen
A vertical surgical incision is present on the abdomen with clean and intact dressing
Foley catheter is attached to uro bag draining well with dark yellow urine
Skin, Hair, Nails
Light brown in color same all throughout the bodySenile skin turgorWrinkles present on the face and neckDry and flaky prominent over the extremitiesBrown-colored macules on the face and upper extremitiesNo edema
Unblemished skin No masses noted No lesions found Warm to touch Evenly distributed short, thin, white
hair Short and thick fingernails and
toenails
Head
NormocephalicOblong-shapedSymmetric facial featuresSymmetric facial movements Without lesions, lumps, or masses noted
Eyes
Eyebrows are unevenly distributed and alignedEyelashes are short and curl outwardsSunken eyeballsWhite scleraPale conjunctivaPupils appear smaller in size and both react to light and accommodationBilateral blinking
Ears
Color is same as facial skinSymmetricalMobile and firm pinna that recoils after it is foldPinna aligned with the outer canthus of the eyeNo unnecessary foul dischargesCan hear sounds in both ears
Nose
Color is same as facial skinSymmetricGreenish discharges present after operationNo lesions
Mouth
SymmetricDark colored dry lipsAble to purse lipsNo lesions notedDark colored gumsNo swellingUses denturesTongue is moist and pink in color which is in central positionTongue moves freely
Neck
Color is same with the headWrinkles presentNot enlargedHead centeredCoordinated movement
Spine and Back
Spinal curvature is accentuatedBefore operation, patient can turn to sides with slight discomfortAfter operation, patient is flat on bed
Thorax and Lungs
Decrease in depth of respiration during inspirationUse of accessory organs during expirationBefore operation, respiration rate is 24 cpmAfter operation, respiration rate is 18 cpmVibrations present and can be felt on the chestClear breath sounds
Breast
Color is same all throughout the abdomenSlightly unequal in sizeGenerally symmetricAppears flaccidLacks firmnessNo masses and lesions foundAreola and nipples are darker in pigmentationNo discharges noted
Heart
Present and audible heartbeatsBeats with regular rhythmBefore operation, cardiac rate is 90 bpmAfter operation, cardiac rate is 73 bpm
AbdomenPre-operative Phase
Uniform colorUnblemished skinRound with asymmetric contourRises with inspiration and falls with expirationsUmbilicus centrally positionedHypoactive bowel sounds auscultated
Abdominal distention
Claimed that pain starts at the right upper quadrant and radiates all throughout the abdomen
The impression to the result of the ultrasound of her whole abdomen is to consider ileus; partial obstruction and fecal stasis
Post-operative Phase
Symmetric contourA colostomy is being attached to colostomy bag at the left upper quadrant of her abdomenA vertical surgical incision is present on the abdomen with clean and intact dressingNo tenderness
Upper Extremities
Both arms are in the same size and length Movement is limited No lesions noted No masses noted No rashes found Dry and flaky skin Brown-colored macules noted Senile skin turgor
Lower Extremities
Both legs are in the same size and length
No lesions and masses noted Dry and flaky skin Fissures noted With lesser hair distributed in the
legs
Musculoskeletal
Muscles are equal in size on both sides of the body
Flaccid muscles No tremors found and no presence
of tenderness or swelling Limited range of motion; decreased
strength; becomes weak in prolonged activities
Neurologic
Has poor posture but is able to walk and maintain balance; but aided during ambulation
Reaction to stimuli are slower Has reduced speed of movement
Genitourinary
On menopausal stage No history of disease affecting
genitals After operation, a foley catheter is
attached to uro bag draining well with dark yellow urine; no pain during urination

Abdominal CT scan - combines special x-ray equipment with sophisticated computers to produce multiple images or pictures of the inside of the body. These cross-sectional images of the area being studied can then be examined on a computer monitor, printed or transferred to a CD.
Abdominal X-Ray - An abdominal X-ray is a picture of structures and organs in the belly (abdomen). This includes the stomach, liver, spleen, large and small intestines, and the diaphragm, which is the muscle that separates the chest and belly areas. Often two X-rays will be taken from different positions. An abdominal X-ray may be one of the first tests done to find a cause of belly pain, swelling, nausea, or vomiting.
Abdominal Ultrasonography - An ideal clinical tool for determining the source of abdominal pain. It can simplify the differential diagnosis of abdominal pain, especially when pain and tenderness are present over the site of disease.
Barium Enema - X-ray examination of the large intestine (colon and rectum). The test is used to help diagnose diseases and other problems that affect the large intestine. To make the intestine visible on an X-ray picture, the colon is filled with a contrast material containing barium. This is done by pouring the contrast material through a tube inserted into the anus.
Laboratory studies (e.g., electrolyte studies and a complete blood cell count) reveal a picture of dehydration, loss of plasma volume, and possible infection.
Decompression of the bowel through a nasogastric or small bowel tube is successful in most cases. When the bowel is completely obstructed, the possibility of strangulation warrants surgical intervention.
Before surgery, intravenous therapy is necessary to replace the depleted water, sodium, chloride, and potassium.
The surgical treatment of intestinal obstruction depends largely on the cause of the obstruction. In the most common causes of obstruction, such as hernia and adhesions, the surgical procedure involves repairing the hernia or dividing the adhesion to which the intestine is attached. In some instances, the portion of affected bowel may be removed and an anastomosis performed. The complexity of the surgical procedure for intestinal obstruction depends on the duration of the obstruction and the condition of the intestine.
A colonoscopy may be performed to untwist and decompress the bowel. A cecostomy, in which a surgical opening is made into the cecum, may be performed for patients who are poor surgical risks and urgently need relief from the obstruction. The procedure provides an outlet for releasing gas and a small amount of drainage.
A rectal tube may be used to decompress an area that is lower in the bowel. The usual treatment, however, is surgical resection to remove the obstructing lesion.
A temporary or permanent colostomy may be necessary. An ileoanal anastomosis may be performed if it is necessary to remove the entire large colon.
Nursing management of the nonsurgical patient with a small bowel obstruction includes maintaining the function of the nasogastric tube, assessing and measuring the nasogastric output, assessing for fluid and electrolyte imbalance, monitoring nutritional status, and assessing improvement (eg, return of normal bowel sounds, decreased abdominal distention, subjective improvement in abdominal pain and tenderness, passage of flatus or stool).

The nurse reports discrepancies in intake and output, worsening of pain or abdominal distention, and increased nasogastric output. If the patient’s condition does not improve, the nurse prepares him or her for surgery. The exact nature of the surgery depends on the cause of the obstruction. Nursing care of the patient after surgical repair of a small bowel obstruction is similar to that for other abdominal surgeries
Fluid Serum December 8, 2010
Electrolytes exist in the blood as acids, bases, and salts (such as sodium, calcium, potassium, chloride, magnesium, and bicarbonate). They control such things as cardiac function and muscle contraction and are routinely measured by laboratory studies of the serum.
Fluid Serum is the cell-free fluid of the bloodstream. It appears in a test tube after the blood clots and is often used in expressions relating to the levels of certain compounds in the blood stream.
A Blood chemistry test is a procedure to examine the general health of a patient especially to assess the functioning of certain organs.
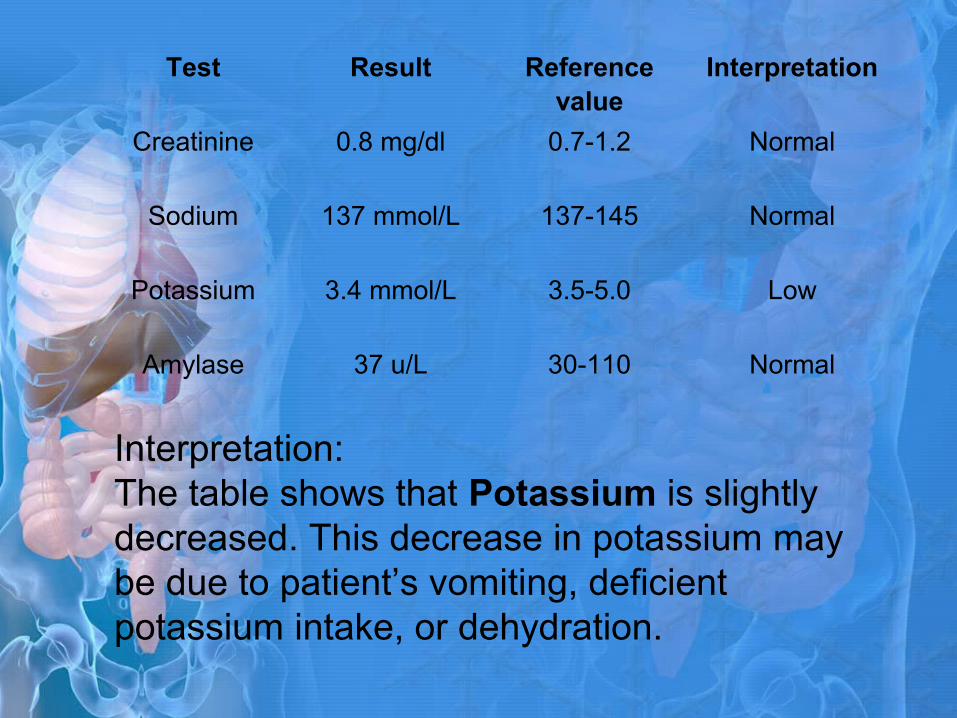
Test Result Reference value
Interpretation
Creatinine 0.8 mg/dl 0.7-1.2 Normal
Sodium 137 mmol/L 137-145 Normal
Potassium 3.4 mmol/L 3.5-5.0 Low
Amylase 37 u/L 30-110 Normal
Interpretation:The table shows that Potassium is slightly decreased. This decrease in potassium may be due to patient’s vomiting, deficient potassium intake, or dehydration.
Nursing Responsibilities:
•define and explain the test•state the specific purpose of the test•explain the procedure•discuss test preparation, procedure, and posttest care•some blood chemistry tests will have specific requirements such as dietary restrictions or medication restrictions.
Complete Blood CountDecember 8, 2010
The complete blood count (CBC) is one of the most commonly ordered blood tests. The complete blood count is the calculation of the cellular (formed elements) of blood. These calculations are generally determined by special machines that analyze the different components of blood in less than a minute.
This test may be a part of a routine check-up or screening, or as a follow-up test to monitor certain treatments. It can also be done as a part of an evaluation based on a patient's symptoms.
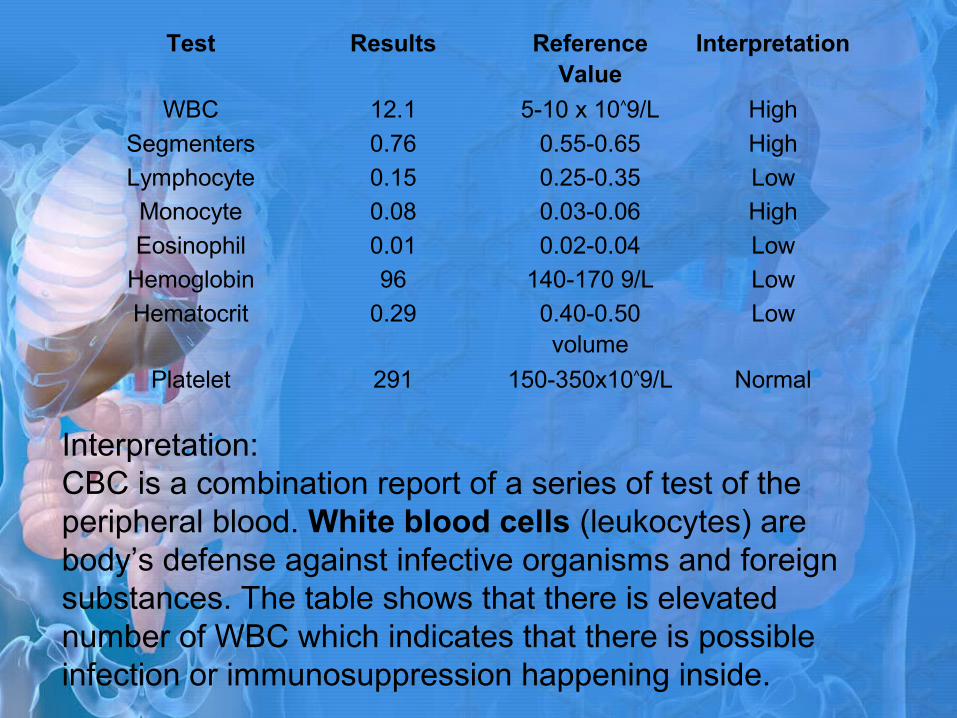
Interpretation: CBC is a combination report of a series of test of the peripheral blood. White blood cells (leukocytes) are body’s defense against infective organisms and foreign substances. The table shows that there is elevated number of WBC which indicates that there is possible infection or immunosuppression happening inside.
Test Results Reference Value
Interpretation
WBC 12.1 5-10 x 10^9/L High
Segmenters 0.76 0.55-0.65 High
Lymphocyte 0.15 0.25-0.35 Low
Monocyte 0.08 0.03-0.06 High
Eosinophil 0.01 0.02-0.04 Low
Hemoglobin 96 140-170 9/L Low
Hematocrit 0.29 0.40-0.50 volume
Low
Platelet 291 150-350x10^9/L Normal
Segmenters are above the normal range which indicates infection.
Low Lymphocyte, Eosinophil and Monocyte count indicates that the body's resistance to fight infection has been substantially lost and one may become more susceptible to certain types of infection, namely cancer and tumor. As lymphocyte cells make up fifteen to forty percent of the total white blood cells that circulate in the bloodstream, a low count can cause damage to organs.
Hemoglobin is the oxygen carrying protein within the RBC’s. The table shows that there is decreased hemoglobin concentration in the blood, which indicates that there is less oxygen being transported throughout the body, because of the less oxygen being transported. With this, the patient is likely experiencing difficulty of breathing that leads patient to have impaired gas exchange.
Hematocrit is the percentage of RBC mass to original blood volume. The table shows that hematocrit volume is decreased which indicates that there is over expansion of extra cellular fluid volume, since the patient has a decreased RBC she also have a decreased hematocrit level..
Nursing Responsibilities:
•Explain that the tests are done to detect any hematologic disorders as well as infection and inflammation.•Tell the patient that a blood sample will be taken and that she may feel slight discomfort from the tourniquet and needle puncture.
•Use gloves when collecting and handling all specimens.
•Transport the specimen to the laboratory as soon as possible after the collection.
•Do not allow the blood sample to clot, of the results will be invalid. Place the specimen in a biohazard bag.

Abdomen Supine and UprightDecember 8, 2010
Abdominal x-rays may be performed to diagnose causes of abdominal pain, such as masses, perforations, or obstruction. Abdominal x-rays may be performed prior to other procedures that evaluate the gastrointestinal (GI) tract or urinary tract, such as an abdominal CT scan and renal procedures.
Result:
Lung bases are clear. Free subphrenic air is noted. There are gas containing loops of small and large bowel in all quadrants with no definite pattern. An ovoid soft tissue density is seen in the right lower quadrant area overlying pattern of the right superior iliac crest. This is seen in the supine view only and may be in the soft tissues. Reacted gas is present. There are advance degenerative changes in lumbar spine characterized by osteophytes/ spurs formation. Asymmetrical narrowing of L4-L5 intervertebral joint space, left is seen with linear lucencies within. Mild levoseoliosis is noted.
Impression:
Essentially (-) study of the abdomen save for degenerative changed of the lumbar spine.
Abdomen Supine and UprightDecember 8, 2010
Abdominal x-rays may be performed to diagnose causes of abdominal pain, such as masses, perforations, or obstruction. Abdominal x-rays may be performed prior to other procedures that evaluate the gastrointestinal (GI) tract or urinary tract, such as an abdominal CT scan and renal procedures.
Abdomen Supine and uprightDecember 9, 2010
Re-examination no longer shows the ovoid soft tissue density in the right lower quadrant area or seen in the abdominal supine view. Gas containing loops of predominantly small bowel segments are still seen in all quadrants with no definite pattern. Rectal gas is present. Pro- peritoneal flank stripes are intact, abdomen are not displaced laterally.

Nursing Responsibilities:
•Remove any clothing, jewelry, or other objects that might interfere with the procedure.•Given a gown to wear.•Position in a manner that carefully places the part of the abdomen that is to be observed. The patient may be asked to stand erect, to lie flat on a table, or to lie on the side on a table, depending on the x-ray view the physician has requested.
•Body parts not being imaged may be covered with a lead apron (shield) to avoid exposure to the x-rays.
Nursing Responsibilities:
•Once positioned, ask the patient to hold still for a few moments while the x-ray exposure is made. Also, ask the patient to hold his/her breath at various times during the procedure.•It is extremely important to remain completely still while the exposure is made, as any movement may distort the image and even require another x-ray to be done to obtain a clear image of the body part in question.•The x-ray beam is then focused on the area to be photographed.
UrinalysisDecember 9, 2010
Routine urinalysis is performed for general health screening to detect renal and metabolic diseases; to diagnose diseases or disorders of the kidneys or urinary tract. In addition, it is performed to help diagnose specific disorders such as endocrine diseases.
Interpretation: The physical and chemical properties of the
patient’s urine show normal results. Normally, blood must be absent in the urine. Presence of blood may indicate acute kidney infections, chronic infections, and stone formation in the kidneys.
Color Reaction Transparency Specific gravity
Light yellow 6.0 Clear 1.003
Sugar AlbuminNegative Negative
Pus cell RBC0.1/ HPF 0.1/ HPF
Nursing Responsibilities:
•Explain how to collect a clean catch specimen of at least 15 mL.•Explain that there is no food or fluids restriction.•Obtain a first voided morning specimen if possible.•Medications may be restricted for it may affect laboratory results.
FecalysisDecember 9, 2010
It refers to a series of laboratory tests done on fecal samples to analyze the condition of a person's digestive tract in general. Among other things, a fecalysis is performed to check for the presence of any reducing substances such as white blood cells (WBCs), sugars, or bile and signs of poor absorption as well as screen for colon cancer.
Interpretation: Black stool may be a result of possible
internal bleeding, particularly somewhere in the digestive tract.
Color Chemical and occult blood
Result
Black Positive No intestinal parasite seen
Nursing Responsibilities:
•Discourage patient from taking aspirin, alcohol, vitamin C, ibuprofen, and certain types of food if fecal sample will be checked for any sign of blood.
•The patient must urinate first to prevent any urine from mixing with feces. •The patient must wear gloves when it's time to handle stool and transfer it to a safer container. This will prevent any possibilities of being contaminated or infected by bacteria found within the stool. •Solid and liquid fecal samples are both acceptable as long as they do not have urine or other foreign substances like soap, water, and toilet paper mixed in them.
Nursing Responsibilities:
•If the patient is suffering from diarrhea, placing a plastic wrap and securing it under the toilet seat could facilitate the collection process.
•Collected samples must be brought to the doctor's office or laboratory as soon as possible. Delays could compromise the quality of the sample.
• Volume or amount is also important so the patient must be sure he has collected an adequate amount of stool.
Potassium TestDecember 10, 2010
This test measures the amount of potassium in the blood. Potassium (K+) helps nerves and muscles communicate. It also helps move nutrients into cells and waste products out of cells.
Test Result Reference value
Interpretation
Potassium 4.1 3.6-5.0 mmol/L Normal
Interpretation: The potassium level of the patient is normal.
Ultrasound in the Whole AbdomenDecember 10, 2010
It is an ideal clinical tool for determining the source of abdominal pain. It can simplify the differential diagnosis of abdominal pain, especially when pain and tenderness are present over the site of disease.
Result:
Liver is normal in size and contour. It shows normal homogenous echo pattern. No mass lesion is noted. Intrahepatic bile ducts and CBD are not dilated. Hepatic vessels are unremarkable. Gallbladder is physiologically distended. It shows normal wall thickness. No internal echoes are noted. No pevicholecystic fluid collection is seen.
Pancreas and spleen are normal. Right kidney measures 9.6 x 4.2 cm with cortical thickness of 1.2 cm. Left kidney measures 9.5 x 4.0 cm with cortical thickness of 1.5 cm. Both are normal in size showing homogenous corticomedullary parenchymal echogenecity. No echogenic focus or mass lesion is noted. There is no separation of the central echo complexes. Proximal uterus is not dilated. Uterus is atrophic and is compatible with the age of the patient. No abnormal masses are seen in both advexac.
Moderately dilated, fecal-filled segment of large bowel are noted in both paracolic gutters, iliac regions and pelvis. No evident mass lesion is appreciated.
Impression:
Considers ileus; Partial obstruction
Fecal stasis
Nursing Responsibilities:
•Before procedure, instruct patient to be on NPO 8-12 hrs since air or gas car reduce quality of image•Assess abdominal distention because it may affect quality of image•During procedure, keep the patient in a supine position
Doctor’s Order
An exploratory laparotomy is done especially when a person complains of abdominal pain. The operation allowed the surgeon to examine the internal organs. Disease or damage can be uncovered. In some cases, the problem can be corrected during the surgery.

A colostomy is when the colon is cut in half and the end leading to the stomach is brought through the wall of the abdomen and attached to the skin. The end of the colon that leads to the rectum is closed off and becomes dormant. Usually a colostomy is performed for infection, blockage, or in rare instances, severe trauma of the colon. This is not an operation to be taken lightly. It is truly quite serious and demands the close attention of both patient and doctor. A colostomy is often performed so that an infection can be stopped and/or the affected colon tissues can heal.
•Assess and measure the nasogastric output•Assess fluid and electrolyte balance and administer IV as prescribed
•Monitor nutritional status•Assess improvement such as return of normal bowel sounds, decreased abdominal distention, abdominal pain and tenderness, passage of flatus or stool
•Prepare patient for surgery which includes preoperative teaching
•After surgery, provide wound care and post-operative nursing care•Place ice chips on the same day of surgery to ease the patient’s thirst. By the next day, the patient may be allowed to drink clear liquids. •Slowly add thicker fluids and then soft foods as the bowels begin to work again. •Patient may eat normally within 2 days after the surgery.
•The colostomy drains stool (feces) from the colon into the colostomy bag. Most colostomy stool is softer and more liquid than stool that is passed normally. The texture of stool depends on the location of the segment of intestine used to form the colostomy.

Drug Study
Prognosis
When client is to be discharged from the hospital, nursing care is still continued. With sufficient support at home, most client recover gradually. During home visits, the client’s physical status and progress towards recovery is assessed. The client’s understanding of therapeutic regimen is also assessed, and previous teaching is reinforced.
Method
•Instruct the significant others to take the following home medication as ordered by the physician.
•Explain to the significant others the drug names as well as the right route and dosage.
•Inform the significant others about the side effects that may occur brought by the medication.•Encourage the significant others to comply and follow religiously the right timing in taking the medication.•Confer with the patient’s family the need take precautions regarding medication therapy, activity, and dietary restriction.•Discuss with the patient’s family ways to cope with stressful situations in positive manner.
Method
•Instruct patient’s family to report for immediate occurrence of signs and symptoms to a health care professional.
•Reinforce and supplement patient’s family knowledge about diagnosis, prognosis, and expected level of function.•Provide patient’s family with specific directions about when to call the physician and what complications require prompt attention.•Peer support and psychological counseling may be helpful for some families.
Exercise/ Environment
•Once at home, patient may resume much of the normal activity short of aggressive physical exercise.
•Walk short distances everyday and gradually increase activity. •No lifting of a weight greater than 20 lbs (9kg) for 6 weeks. Exercise should be started cautiously.•Encourage to practice deep breathing exercise and range of motion exercises up to the level of capability.
Exercise/ Environment
•Explain the need for rest periods both before and after certain activities.
•Teach client the importance of stress management through relaxation technique,•Help improve patient’s self-concept by providing positive feedback, emphasizing strengths and encouraging social interaction and pursuit of interests.
Treatment
•Explain to the significant others the need to continue drug therapy•Provide patient’s family with a list of medications, with information on action, purpose and possible side effects.•Advise significant others to always comply with the medications. Call the physician if there is a problem taking them.

Hygiene
•Keep proper hygiene. Teach client’s family the importance of hygiene like daily oral care, bathing and changing clothes.•Proper Wound care must be observed.
Outpatient
•Advise to visit or have her follow up check-up with her attending physician.•Advise to call and notify the attending physician for any unusualities that may occur•Routinely, follow up check – up with patients within two weeks. If there are staples that require removal, postoperative problems, or wound issues, a follow-up appointment will be scheduled sooner.
Diet
•Emphasize to the client’s family the importance of proper nutrition, its need for early recovery. This can aid in restoring body functioning.•Provide dietary instructions to help patient’s family identify and eliminate foods that is needed by the patient.•Soft or low residue diet upon discharge; this should be continued at home for approximately 2 weeks (this includes breads, cereals, chicken, fish, and soup). •Avoid large quantities of raw fruits and vegetables.
•After 2 weeks, gradually reintroduce your regular diet.
•Encourage to drink plenty of fluids.
•Take nutrition supplements