Interpretation Guide for Ventana INFORM HPV Probes In · PDF fileInterpretation Guide for...
20
Interpretation Guide for Ventana INFORM ® HPV Probes In Situ Hybridization (ISH) Staining of Cervical Tissue Thomas M. Grogan, M.D. Hiro Nitta, Ph.D. Lidija Pestic-Dragovich, Ph.D. Lizhen Pang, M.S. Jay Ji, Ph.D. Innovations in Science and Medicine
Transcript of Interpretation Guide for Ventana INFORM HPV Probes In · PDF fileInterpretation Guide for...

Interpretation Guide for Ventana INFORM® HPV Probes In Situ Hybridization (ISH) Staining of Cervical Tissue
Thomas M. Grogan, M.D.Hiro Nitta, Ph.D.Lidija Pestic-Dragovich, Ph.D.Lizhen Pang, M.S.Jay Ji, Ph.D.
Innovations in Science and Medicine

�
Table of Contents
I. Introduction A. General Description of INFORM® HPV Probes B. Purpose of Interpretive Guide
II. IdentificationofAppropriateStainingPattern A. Staining Patterns of Episomal and Integrated HPV B. DefinitionofPositiveandNegativeResults C. HPV Pattern and Disease Progression
III. RepresentativeClinicalCaseMaterials A. Normal B. Cervical Intraepithelial Neoplasia (CIN) I C. Cervical Intraepithelial Neoplasia (CIN) II/III D. Squamous Cell Carcinoma E. Condyloma
IV. UseofControlSlidesforSystemQualityControl
V. AluPositiveControlProbeIIforTissueQualification
VI. Fixation
VII. InterpretingArtifacts A. Over-digestion Artifacts B. Leukocyte-associated Artifacts C. Drying Artifacts D. Chromogen Precipitate Artifact E. Nuclear Artifact
VIII. Bibliography

�
I. Introduction
A. GeneralDescriptionofINFORM®HPVProbes
The INFORM HPV III Family 16 Probe (B) contains a cocktail of HPV genomic probes in a formamide-based diluent. The intended targets are the common high-risk HPV genotypes found to be associated with cervical neoplasia. The probe cocktail has demonstratedaffinitytothefollowinggenotypes:16,18,31, 33,35,39,45,51,52,56,58,and66.
The INFORM HPV II Family 6 Probe (B) contains a cocktail of HPV genomic probes in a formamide-based diluent. The intended targets are the HPV genotypes found commonly in condyloma andsomeearlycervicalintraepitheliallesions,whicharenot commonly associated with cervical cancer. The probe cocktail hasdemonstratedaffinitytothefollowinggenotypes:6and11.
B. PurposeofInterpretiveGuide
Thefollowing53casesillustratethevarietyofstainingpatternsthat may be present in cervical biopsies when stained withVentanaINFORMHPVProbes(Figures1-19).The photomicrographs allow a new user to become familiar with the spectrum of staining patterns including episomal and integrative patterns of HPV positivity and patterns of artifactual staining that theymayencounterinavarietyofcervicaltissues,including normal,cervicalintraepithelialneoplasia(CINI,II/III), carcinoma,andcondyloma,whenusingavalidatedassay involving the Ventana INFORM HPV Probes. The intent is to provide pathologists with a tool to facilitate interpretation of INFORM HPV Probes staining results. Any staining performed in the end users lab should be interpreted within the context of the controls run with the clinical cases at the time of evaluation. See the package insert provided with these products for further information.
The images contained in this interpretive guide we obtained using anassaydevelopedandvalidatedatVentanaMedicalSystems,Inc.,employingtheINFORMHPVProbes.

4
A. StainingPatternsofEpisomalandIntegratedHPV
When utilizing the INFORM HPV III Family 16 Probe (B) in the Ventana-validatedassay,thepresenceofHPVisdemonstratedwhen either the episomal or integrated pattern is found within the nuclei of cervical epithelial cells (Figure1).
Theepisomalpatternappearsasalarge,homogeneous, globular navy-blue precipitate within the epithelial cell nucleus (seeCases1-3).Theintegrativepatternisadiscrete,stipplednavybluenuclearpattern(seeCases4-6).AsshowninCases1-3,theepisomalpatternisgenerallyprominentinthesuperficialkeratinized region of the epithelium often within koilocytotic cells. Thediscrete,dot-likenuclearintegrativepatternismoreofteningroupsofepithelialcellsinamorebasallocation(Case7,Figure2).Insomecases,thenuclearintegrativepatternmaybesodiscreteastorequiremicroscopicexaminationathighermagnification(40xor100xobjective)tojudgenuclearepithelialcelllocalization.Inthiscontext,itisspecificallythefindingofadistinctpattern
(e.g.afieldofepithelialcellswithdot-likenuclearspots),whichis pivotaltojudgingpositivity.Incontrast,thefindingofarare“speck” of navy-blue in a rare scattered cell could be artifactual as a pattern of cellular involvement is not evident.
These characteristic nuclear epithelial cell patterns of staining indicatepositivity.Incontrast,artifactualnon-specificstainingunrelated to HPV manifests distinctly separate features. As illustratedinSectionVII,thenon-specific,non-HPVassociatedartifactsmayincludefocalnon-cellularstromalprecipitates,aslightdiffuselow-levellightbluestaining,theperiodicstaining ofthecytoplasmofPMNsandeosinophils,andnon-specificstaining of nucleoli and lymphocyte/endothelial cells. With someoftheseartifacts,itagainmaybenecessarytoexamineborderlinecasesathighermagnification(40xor100xobjective) tojudgenuclearlocalization.
Fig.1StainingPatternsWithINFORMHPVIIIFamily16Probe(B)
Case1
II. Identificationof AppropriateStainingPattern
•EpisomalPattern:Cases1-3
•IntegrativePattern:Cases4-6
Case2 Case3
Case4 Case5 Case6

5
B. DefinitionofPositiveandNegativeResults
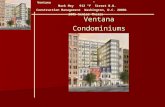
Case 7 (Figure �) illustrates the quintessential features of judgingINFORMHPVIIIFamily16Probe(B)stainingwhenusingthe Ventana-validated assay. The case is an example of Cervical Intraepithelial Neoplasia (CIN I) at the transition zone of the cervix.Inthiscase,theCINIlesionaltissue(rightsideofphoto) isseeninclosecontiguitywithadjacentnormalcervicalepithelial(leftsideofphoto).Inthisexample,therearetwopositive patterns:(1)the“episomal”stainingwithinthesuperficial epithlial cells overlying the CIN I lesional tissue and (�) the discrete,dot-likenuclear,or“integrative”,patterninthemid-andbasallayerCINlesionaltissue.Importantly,anegativestainingpatternisfoundwithinthenon-lesionaladjacentnormalcervicalepithelialnuclei,endocervicalglands,andthestromalcells, includingfibroblasts,endothelialcells,andlymphocytes.Of noteisaverysuperficiallayerofnavy-blueIndiaInkusedatcolposcopy to mark lesional tissue.
AsshowninCase7,thedeterminationofatruepositiveINFORM
HPVIIIFamily16Probe(B)ISHresultrequiresfindingeitherthe episomal and/or integrative pattern of navy-blue staining in lesionalcervicalepithelium,inthecontextofadjacentnegativestaining within non-lesional cervical epithelium and endocervical glandsandinnon-lesionalstromalcells,fibroblasts,lymphocytes,andendothelialcells,whilediscountingartifactualstaining, such as found in the cytoplasm of PMN and India Ink margins. Substantial artifactual staining of non-lesional cells of epithelial ornon-epithelialoriginmayprecludejudgingapositiveresult.
The determination of a true negative INFORM HPV III Family 16 Probe(B)ISHresultrequiresfindingnosignal(neitherglobular“episomal” or discrete “integrative” pattern) within lesional epithelialcells,inthecontextofanuclearDNA-positivecontrolprobe result and an appropriate cell line slide control (Section IV and V).
Normal
Fig.2InterpretiveExample:Case7
Episomal Integrated

6
Insomeinstances,particularlywithhigh-gradedysplastic cervicallesions(egCINII/IIIorCervicalCarcinoma),thestainingmayshowalowcopynumberintegrativepattern,whichmaybemostnoticeableathighermicroscopemagnification(eg40xor100xobjective).Figure3illustratestwosuchcases,onewithaHeLa-like(10-50copy)integratedpatternandanotherSiHa-like
verylowcopynumber.Inbothcases,thepivotalobservationisthefindingofadiscrete,specklednuclearlocalizationinvolvingnumerouscontiguouscervicalepithelialcellswiththeadjacentstroma,lymphocytes,submucosalglands,andnormalcervicalepithelial showing an absence of this pattern.
Fig.3InstructiveCases:Case8(a,b)andCase9(c,d)
A•10X B•40X
C. HPVPatternandDiseaseProgression
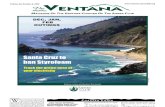
AsillustratedinFigures4Aand4B,theviralcopynumber and pattern of nuclear involvement varies with disease progression.InitiallywithCINIandCINII,theglobularepisomalpattern predominates consistent with the high viral copy number
and high infectivity of the patient. Subsequently in CIN III and overtcarcinomathemorebasallyorientedlowcopynumber,speckled,integrativepatternprevails.
Fig.4HPVCopyNumberandDiseaseProgression
C•40X D•100X
Virus vs. Disease
Disease progression
HP
V C
op
ies per cell
Condyloma CIN I CIN II CIN III SCCA
ASC
1
50
Infection Acute Infection
Normal Cytology Transformation Immortalization
Neoplasia Cancer
1000
LSIL HSIL
A.HPVandCervicalCancers B.HPVInfectionandDiseaseProgression
B. DefinitionofPositiveandNegativeResults(cont.)

7
Followingisaportfolioofcervicalbiopsiesfirstdiagnosed morphologically by Hematoxylin and Eosin (H&E) staining and then stained with INFORM HPV Probes for Family 16 and/or Family 6 HPV. Included are representative examples of normal cervical epithelial,CINI,CINII,CINIII,carcinomaandcondyloma.
ApositiveHPVresultisjudgedwheneithertheepisomalor integrated pattern is found. The episomal pattern appears as
a large homogeneous navy-blue precipitate within the nucleus. Theintegrativepatternisadiscrete,stipplednavybluenuclearpatternwithina“field”ofcervicalcells.Asshown,theepisomalpatternisgenerallyprominentinthesuperficialkeratinized region of the epithelium often within koilocytotic cells. The “speckled” nuclear integrative pattern is more often in more basal epithelial cells.
III. Representative Clinical Case Materials
A. Normal
These cases are all cervical biopsies taken at colposcopy in the context of a preceding abnormal PAP or a visual colposcopic abnormality.AsshowninFigure5,thesebiopsieswerealljudgedbyH&Emicroscopytobewithinnormallimitswithoutdefinitivepathologic alteration.
Ineachcase,theINFORMHPVIIIFamily16Probe(B)wasjudgedas negative with no evidence of either an episomal or integrative
patternpresent.Incomparisonwiththenegativereagentcontrol,a very slight bluish haze is found. This trace staining is unrelated to HPV.
InCases23and24,acommonartifactisnotedasavery superficiallayerofnavy-blueIndiaInkusedatcolposcopy to mark lesional tissue.
ClinicalExamples:
Fig.5NormalCervicalTissueStainedWithINFORMHPVIIIFamily16Probe(B)
Case22 Case23
Case24 Case25

8
B. CervicalIntraepithelialNeoplasia(CIN)I
These3casesillustrate,inFigure6,thehistopathologicand INFORM HPV III Family 16 Probe (B) staining characteristics ofCINIlesions.Asshown,apredominanceoftheepisomalnuclearstaininginthesuperficiallayersoftheepithelialare theusualfinding.
Occasionally,acaseofCINImayhavethemid-andbasal-layerspeckled,integrativepattern(seeCase7,Fig2).
Numerous studies have documented the high level of intraobserver and interobserver variability associated with thehistopathologicdiagnosisofCINI.Uponadjudicationinthe
ALTStrial,41%ofcasesdiagnosedonH&EasCINIwere down-gradedtonormaland13%wereupgradedtoCINIIand CIN III10. The biologic potential of CIN I lesions is characterized by high rates of spontaneous regression and low rates of progression to cancer. The poor reproducibility and uncertain biologic potential of CIN I have made the management of women with CIN I problematic. Recent evidence 2,3,5,11 suggests the identificationofintegratedHPVinthebasalepitheliumby means of in situ hybridization may distinguish patients with histologic CIN I who are at greater risk for the development of high-grade lesions.
Fig.6CINILesionalTissueStainedWithINFORMHPVIIIFamily16Probe(B)
Case26(A):H&E Case26(B):HPV
Case27:HPV Case28:HPV

9
C. CervicalIntraepithelialNeoplasia(CIN)II/III
In contrast with the predominance of the episomal pattern in CINI,themajorityofCINII/IIIcases(Figure7)illustratetwo patterns of HPV positivity. These include the prominent globular “episomal”stainingfoundnotablyinthesuperficialepithelialcells.Theserepresentthe“infective”,exfoliatedform,which isinvolvedinsubsequentdiseasetransmission.Further, belowintheepithelium,arefoundtheepithelialcellswithan integrative pattern of staining. These include cells from the mid-leveltobasal-levelepithelialcells,whicharethoughtto
represent the sites of HPV-clonal integration into host cells. Theadjacentstromalcells,endothelialcells,andlymphocytes are appropriately negative.
AsillustratedinCase32,someCINIIIlesionsmaycontain only the integrative pattern with very low viral copy number. In this instance only one integration site per epithelial nucleus is observed.
Fig.7CINII/IIILesionalTissueStainedWithINFORMHPVIIFamily16Probe(B)
Case29 Case30 Case31
Case32 Case33 Case34

10
D. SquamousCellCarcinoma
Thesecasesofinvasivecervicalsquamouscarcinoma(Figure8)demonstrate nuclear HPV integrative pattern positivity in the neoplastic epithelial cell nuclei. While invasive cervical carcinomamayshowtwopatternsofstaining,bothepisomal andintegrative,themajorityofcervicalcarcinomacases have a very low viral copy number (as documented in the literature),whichmanifestintissuesectionISHasthe prominence of the integrated pattern of nuclear staining.
AsshowninCases35and36,theintegrativepatternmayoften be the sole staining found in the neoplastic cells. Notice in the two cases illustrated the viral copy number and number of integration sites per nucleus is very similar to that observed within HeLa nuclei within the cell line control slide (see Figure 10).Theadjacentstromal,lymphocyte,andendothelialcells are negative.
Fig.8CervicalCarcinomaLesionalTissueStainedWithINFORMHPVIIIFamily16Probe(B)
Case35(A) Case35(B) Case35(C)
Case36(A) Case36(B) Case36(C)

11
E. Condyloma
Condylomaaresuperficialwart-likelesionsfoundwithinthe epitheliumofthecervixandfoundinassociationwith“specific”HPV genotypes (e.g. HPV 6 and 11). These HPV 6/11-associated lesions are expectedly negative for INFORM HPV III Family 16 Probe(B)(seeFig9,Case37(B))andpositiveforINFORMHPVIIFamily6Probe,asshowninFigure10(Case37andCase38).
ThestainingpatternsinCases37and38speaktothespecificityof the INFORM HPV Family 16 and Family 6 Probes.
Fig.9CondylomaStainedWithINFORMHPVIIIFamily16(B)andHPVIIFamily6Probes
Case37(A):H&E Case37(B):INFORMHPVIIIFamily16Probe(B)
Case37(C):INFORMHPVIIFamily6Probe(B) Case38:INFORMHPVIIFamily6Probe

1�
A. StainingPatternsofEpisomalandIntegratedHPV
The determination of a true negative and/or positive HPV INFORM ISHresultrequires,inthesamerun,apositivecontrolslidesuchas a known HPV-positive control slide (see Figure 11) or an indexcasewithanintegrative-onlypattern(seeFigure10). The appropriate positive “integrative” nuclear pattern is found in both CaSki and HeLa cells and absent in HPV negative cells. The CaSki cells are HPV 16 genotype cells with abundant copy number(200-600copies/cell).HeLacellsareHPV18genotypecellswithlowerviralcopynumber(10-50copies/cell).TheHeLacell line in particular serves as a sensitivity control for the low
levelintegrativestainingpattern,whichmaybefoundinsomeCIN III (Figure 7) and in most invasive cervical carcinomas (Figure 8and10).TheHPV-negativecellsserveasanimportantindicatorof inappropriate noise in the HPV assay.
The importance of using a patient sample “index case” is well illustratedbyCase40(seeFigure10).Thispatientsampleofcervical carcinoma has a HeLa-like level of HPV expression and the multiple blocks available allow the use of either a same-slide or same-run control from a constant source for extended time.
IV. Use of Control Slides for System Quality Control
Fig.10Patient“IndexCase”ControlSamples
CaSki-likeCase:Case39 HeLa-likeCase:Case40
Fig.11
A.HPV3in1SystemControlSlide B.HPVCellLinesStainedWithHPVIIIFamily16Probe(B)
CaSki HeLa Negative
CaSki
HeLa
NegativeC33
(Negative)
+ +

1�
Specifically,theAluPositiveControlProbeIIdetectsAlurepeats.A positive nuclear signal within epithelial and non-epithelial cells confirmsthetissuesamplecontainsintactDNA(Figures12and1�). A negative Alu Positive Control Probe II indicates loss of DNA intactness probably related either to tissue handling and/or tissue fixation.TheAluPositiveControlprobeservesastheequivalent ofthe“housekeepinggene”controlusedinPCRassays.Accordingly,likePCR,ifDNAintactnessislost,anegativeresultmaynotbetrueand study of additional lesional tissue is necessitated.
Figures 1� and 1� illustrate two clinically relevant examples of thisassay.InCase41,theAluorDNApositivityisstrongerwithcellconditioningthanwithoutcellconditioning,indicatingthe importanceoftheunmaskingofDNAbyheat,pH,orenzymes.InCases42and43areshowntherelationshipbetweenAluorDNAabundance and Alu signal and HPV assay signal.
V.AluPositiveControlProbeIIforTissueQualification
Fig.13GenomeIntegrityandISHAssay
Case42(A) Case42(B)
Case43(A) Case43(B)
Fig.12DNAPositiveAluControlSlides
Case41(A):Alu,noCC*-*CC=CellConditioning Case41(B):AluwithCC

14
NoticeinCase43thenearlyabsentAluISHismirroredbyanearly-absent HPV result.
Thus,theAluISHprobemaybeusedtooptimizetheconditionsfor detection of HPV DNA allowing selection of ideal DNA signal preservation relative to cell conditioning or denaturation conditions.Finally,theAluISHprobemayproveespecially useful when there is an unexpected HPV-negative result in the faceoflesionaltissue(egCINI,II,III).Inthisinstance,the
Alu ISH assay might be absent or nearly absent establishing the lack of DNA preservation as an explanation of the unexpected negativeassayresult(Figure13).ThefindingofapositiveAluISHresult,whileindicatingtheintactnessofbiopsyDNA,doesnotestablishDNAaccessibilityoropennessrelatedtofixationmethodor assay sensitivity. Accordingly while DNA may be intact and accessibleforhybridizationwithneutralbufferedformalin,it maybeintactbutnotaccessiblewithcertainfixatives(Figure14).
VI. Fixation
Fig.14HPVIn SituHybridizationPerformanceinSiHaCellLines
NBF
The Ventana-validated assay was developed utilizing tissue fixedin10%neutralbufferedformalin.Artificialtumors generated using the SiHa characterized human cell line (1-� copiesHPV16pernucleus)werefixedinavarietyoffixatives foreighteenhours,twodays,orfivedays.Tissuewasprepared in5μmsectionsandstainedusingHPVIIIFamily16Probe(B) with extended cell conditioning and ISH protease � for four minutes.Figure14illustratestheabilityoftheVentanavalidatedassaytodetectHPVindifferentiallyfixedtissue.Resultsshow
HPV staining is robust in Neutral Buffered Formalin and Zinc Formalinfixedtissues;nodegradationofsignalorlossof antigenunmaskingisnotedforfixationtimesfromeighteen hourstofivedays.Incontrast,PreferandBouinsfixativesshow different levels of detection among the times tested when compared to Neutral Buffered Formalin. Less than optimal tissue acquisition,fixationandstoragearemajorfactorsintheability to detect HPV signal for microscopic interpretation.
ZincFormalin Prefer Bouin’s
TissueFixationLength
5Days
2Days
18Hours

15
A. OverdigestionArtifacts
AsillustratedinFigure15,useofoverlystrongamountsof protease or prolonged protease treatment may result in a
loss of tissue integrity making interpretation of lesional tissuedifficult.
VII.InterpretingArtifacts
B. Leukocyte-associatedArtifacts
Cytoplasmicstainingofleukocytes,asshowninFigure15, occursfrequently.Thisnon-specificdensecytoplasmstaining is unrelated to the DNA probes. It is associated with the secondaryantibodiesand/orbioconjugatesreactingnon- specificallywithcytoplasmiccomponents.Thelocalization inthecytoplasm,andnotthenuclei,ofbothpolymorphonuclear(PMNs)leukocytesandeosinophilsindicatesanon-specific, non-viral-associated artifact.
Occasionally acute cervicitis with an abundance of PMNs is seen. The consequent artifactual staining is readily perceived as non-specificasthesignalisfoundinthecytoplasmofPMNsandnot in the nuclei of epithelial cells. Note that the “true positive” integrative pattern of HPV staining is also found in the epithelial cellsofCase46.
Case44(B):StrongProtease1 Case46:PMNArtifact
Fig.15ArtifactsWithINFORMHPVIIIFamily16Probe(B)
Case44(A):WeakProtease2 Case45:PMNArtifacts

16
C. DryingArtifacts
Rarely,liquidreactants(buffersandliquidcoverslip)maywickoffthe slide resulting in focal drying artifact. This may result in focal deposition of chromogen (eg NBT-BCIP complex) resulting in either a pool or band of blue dye (see Figure 16).
Fig.16ArtifactsWithINFORMHPVIIIFamily16Probe(B)
Case47 Case48
Case49 Case50

17
D. ChromogenPrecipitateArtifact
Rarely,theNBT-BCIPchromogenmaydiscretelyprecipitate resultinginirregular,“meteorite-like”darkbluefociofdye(seeFigure16).These“burr-like”objectsarenotablyfoundabovetheplaneoffocusofthetissuesurface,incontrastwiththetrue“episomal” staining with smooth globular
navy-bluestaining,whichiswithinthefocalplaneofthe epithelial nucleus. Rarely the NBT-BCIP chromogen may precipitate in crystalline form (see Figure 17). This artifact iscausedspecificallybyinadequatedehydrationpriorto cover-slipping.
Fig.17ChromogenPrecipitateArtifact:Case51

18
E. NuclearArtifact
Two separate nuclear artifacts have been observed as rarities. First,apalebluestainingofnucleolimaybenoted(seeFigure18).Thisphenomenonisnotavirus-associatedphenomenonbutmostprobablyreflectsweakcross-hybridizationwithRNAundercertainfixationandcellconditioningcircumstances.As illustrated,thisphenomenoncharacteristicallyoccursinallnucleoli,includingbothepithelialandnon-epethelialcells. Second,stipplednuclearand/orcytoplasmicstainingmayoccur
inablotchypatternwithinlymphocytes,fibroblasts,andsomeendothelialcells(seeFigure19).Thisartifacthasnoviral associationand,again,mayreflectweakcross-hybridization with RNA under certain circumstance. The presence of this phenomena in lymphomal and stromal cells indicates non-specificstainingandintheextrememaypreclude diagnostic interpretation.
Fig.18NuclearArtifact:Case52 Fig.19NuclearArtifact:Case53

19
VIII. Bibliography1 CooperK,EvansM,MountS.Biologyandevolutionofcervicalsquamousintraepitheliallesions:ahypothesiswithdiagnosticprognosticimplications.AdvancesinAnatomic
Pathology2003;10(4):200-3
2 LizardG,RoignotP,Brunet-LecomteP,ChardonnetY.Morphologicalanalysisofinsituhybridizationsignalsincervicalintraepithelialneoplasia
containinghumanpapillomavirustype16or18:relationshipwithhistologicalgradeandDNAcontent.Cytometry1998;34:180-6
3 CooperJ,HerringtonCS,SticklandJE,EvansMF,McGeeJOD.Episomalandintegratedhumanpapillomavirusincervicalneoplasiashownby
non-isotopicinsituhybridization.JClinPathol1991;44:990-6
4 SanoT,HikinoT,NiwaY,KashiwabaraK,OyamaT,FududaT,NakajimaT.Insituhybridizationwithbiotinylatedtyramideamplification:detectionofhumanpapillomavirusDNAin
cervicalneoplasticlesions.ModPathol1998;11:19-23
5 EvansME,MountSL,BeattyBG,CooperK.Biotinyl-tyramide-basedinsituhybridizationsignalpatternsdistinguishhumanpapillomavirustypeandgradeofcervicalintraepithelial
neoplasia,ModPathol2002;15:1339-47
6 GrafAH,CheungAL,Hauser-KornbergerC,DandachiN,GubbsRR,DietzeO,HackerGW.ClinicalrelevanceofHPV16/18testingmethodsincervicalsquamouscellcarcinoma.
ApplImmunohistochemMolMorphol,2000;8:300-9
7 NuovoGJ.Theroleofhumanpapillomavirusingynecologicdiseases.InAdvancesinPathologyandLaboratoryMedicine,vol.8,1995,Mosby-YearBook,Inc
8 QureshiMN,RudelliRD,TubbsRR,BiscottiCV,LayfieldLJ.RoleofHPVDNAtestinginpredictingcervicalintraepitheliallesions:comparisonof
HCHPVandISHHPV.DiagnosticCytopathology2003;29:149-55
9 WrightTC,CoxJT,MassadLS,CarlsonJ,TwiggsLB,WilkinsonEJ.2001Consensusguidelinesforthemanagementofwomenwithcervical
intraepithelialneoplasia.AmJObstetGynecol,2003;189:295-304
10 StolerM,SchiffmanM,InterobserverReproducibilityofCervicalCytologicandHistologicInterpretations,JAMA2001,285:1500-5
11 PeitsaroP,JohanssonB,SyrjanenS.Integratedhumanpapillomavirustype16isfrequentlyfoundincervicalcancerprecursorsasdemonstrated
byanovelquantitativereal-timePCRtechnique.JClinMicrobiology2002;40(3)886-91
2 TranablocP,MetaplasiaandHighGradeCIN,DiagnosticDifficulties.GynecolObstetFertil.2002;30:845-9
13 AtlasofDiagnosticImmunohistopathology,L.True,ed.,Lippincott1990,pg.12.18
14 ACOGPracticeBulletinNo.45,“CervicalCytologyScreening.ClinicalManagementGuidelinesforObstetrician-Gynecologists.”August2003
15 GuidancefortheSubmissionofImmunohistochemistryApplicationstotheFDA,June3,1998.DivisionofClinicalLaboratoryDevices,OfficeofDeviceEvaluation,CenterforDevices
andRadiologicalHealth,FoodandDrugAdministration
16 Review Criteria for In Vitro Diagnostic Devices that Utilize Cytogenetic In Situ Hybridization Technology for the Detection of Human Genetic Mutations (Germ Line and Somatic).
DraftVersion:February15,1996.Page2.DivisionofClinicalLaboratoryDevices,OfficeofDeviceEvaluation,CenterforDevicesandRadiologicalHealth,FoodandDrugAdminis-
tration
17 MunozN,BoschFX,deSanjoseS,HerreroR,CastellsagueX,ShahKV,SnijdersPJF,MeijerCJLM,fortheInternationalAgencyforResearchonCancerMulticenterCervical
CancerStudyGroup.EpidemiologicClassificationofHumanPapillomavirusTypesAssociatedwithCervicalCaner.NEnglJMed2003,348;6.
18 SchiffmanMH,BauerHN,HooverRN,GlassAG,CadellDM,RushBB,ScottDR,ShermanME,KurmanRJ,WacholderS,StantonCK,ManosMM.
EpidemiologicEvidenceShowingThatHumanPapillomavirusInfectionCausesMostCervicalIntraepithelialNeoplasia.JNatlCancerInst,1993,85,:958-964.
19 KlaseR,WoernerSM,RidderR,WentzensenN,DuerstM,SchneiderA,LotzB,MelsheimerP,vonKnebelDoeberitzM.DetectionofHigh-RiskCervicalIntraepithelialNeoplasia
andCervicalCancerbyAmplificationofTranscriptsDerivedfromIntegratedPapillomavirusOncogenes.CancerRes,1999,
59:6132-6136.
20 StolerMH,RhodesCR,WhitbeckA,WolinskySM,ChowLT,BrokerTR.HumanPapillomavirusType16and18GeneExpressioninCervicalNeoplasias.HumPathol,Feb1992;
23:117-128.
21 NuovoGJ.DetectionofHumanPapillomavirusinPapanicolaouSmears:CorrelationWithPathologicFindingsandClinicalOutcome.DiagnMolPathol,June1998,7:158-163.
22 HerringtonCS,AndersonSM,BauerHM,TronconeG,deAngelisML,NoellH,ChimeraJA,VanEyck,SL,McGeeJO’D.Comparativeanalysisof
humanpapillomavirusdetectionbyPCRandnon-isotopicinsituhybridization.JClinPathol1995;48:415-419.
23 WrightTC,SchiffmanM.AddingaTestforHumanPapillomavirusDNAtoCervical-CancerScreening.NEnglJMed,2003,348;6.
24 CooperK,McGeeJO’D.Humanpapillomavirus,integrationandcervicalcarcinogenesis:aclinicopathologicalperspective.JClinPatholMolPathol1997;50:1-3.
25 UngerER,VernonSD,LeeDR,MillerDL,ReevesWC.DetectionofHumanPapillomavirusinArchivalTissues:ComparisonofInSituHybridization
andPolymeraseChainReaction.JHistochemCytochem,46:535-540,1998.
26 VernonSD,UngerER,WilliamsD.ComparisonofHumanPapillomavirusDetectionandTypingbyCycleSequencing,LineBlotting,andHybrid
Capture.JClinMicrobiol,38:651-655,2000.
27 UngerER,HammerML,ChenggisML.Comparisonof35SandBiotinasLabelsforInSituHybridization:UseofanHPVModelSystem1..JHistochemCytochem,39:145-150,1991.
28 UngerER,LeeDR.InSituHybridization:PrinciplesandDiagnosticApplicationsinInfection.JHistotech,18:203:209,1995.
29 Unger,ER,VernonSD,ThomsWW,NisenbaumR,SpannCO,HorowitzIR,IcenogleJP,ReevesWC.HumanPapillomavirusandDisease-FreeSurvivalinFIGOStageIbCervical
Cancer.JInfectDis,172:1184-90,1995.
30 VernonSD,UngerER,MillerDL,LeeDR,ReevesWC.AssociationofHumanPapillomavirusType16IntegrationintheE2GenewithPoorDisease-FreeSurvivalfromCervical
Cancer.IntJCancer(PredOncol):74,50-56,1997.
31 Unger,ER.InSituDiagnosisofHumanPapillomaviruses.ClinLabMed,20:289:301,2000.

Innovations in Science and Medicine
©2006VentanaMedicalSystems,Inc.Printed in U.S.A.N4630306A
NorthAmericaVentanaMedicalSystems,Inc.1910E.InnovationParkDriveTucson,Arizona85755U.S.A.+1(520)887-2155(800)227-2155(U.S.)
EuropeVentanaMedicalSystems,S.A.Parcd'Innovation-BP30144Rue G. de KaysersbergF-67404IllkirchCEDEXFrance+33(0)390405200
MDCILtd.Arundel House1 Liverpool GardensWorthingWest Sussex BN11 1SL U.K.
Australia,NewZealandVentanaMedicalSystemsPtyLtd5/39GrandBoulevardMontmorencyVIC3094Australia+61(0)394316064
CorporateOffices
www.ventanamed.comVENTANA®,INFORM®,andBenchMark®areregisteredtrademarksofVentanaMedicalSystems,Inc.