
International Health Policy Program -Thailand Challenges to universal health coverage in Thailand...
14
1 International Health Policy Program - Thailand International Health Policy Program -Thailand Challenges to universal health coverage in Thailand Phusit Prakongsai, M.D. Ph.D. Viroj Tangcharoensathien, M.D. Ph.D. International Health Policy Program (IHPP) Ministry of Public Health of Thailand Presentation to the 13 th Annual Scientific Conference (ASCON XIII) ICDDR,B, Dhaka, Bangladesh 15 March 2011
-
Upload
wilfrid-barber -
Category
Documents
-
view
215 -
download
1
Transcript of International Health Policy Program -Thailand Challenges to universal health coverage in Thailand...

1
Inte
rna
tio
na
l H
ea
lth
Po
lic
y P
rog
ram
-T
ha
ila
nd
Inte
rnati
onal H
ealt
h P
olic
y P
rogra
m -
Thaila
nd
Challenges to universal health
coverage
in Thailand
Phusit Prakongsai, M.D. Ph.D.Viroj Tangcharoensathien, M.D. Ph.D.
International Health Policy Program (IHPP)Ministry of Public Health of Thailand
Presentation to the 13th Annual Scientific Conference (ASCON XIII)ICDDR,B, Dhaka, Bangladesh
15 March 2011

2
Inte
rna
tio
na
l H
ea
lth
Po
lic
y P
rog
ram
-T
ha
ila
nd
Inte
rnati
onal H
ealt
h P
olic
y P
rogra
m -
Thaila
nd
Health financing arrangements and three public Health financing arrangements and three public
health insurance schemes in Thailand after health insurance schemes in Thailand after
achieving UC in 2002achieving UC in 2002
Health care finance and service provision of Thailand after achieving universal coverage (UC)
General tax
General tax Standard Benefitpackage
Tripartite contributionsPayroll taxes
Risk relatedcontributions
CapitationCapitation & global
Co-payment budget with DRG for IP
Services
Fee for servicesFee for services - OP
Population Patients
Ministry of Finance - CSMBS(6 million beneficiaries)
National Health Insurance Office The UC scheme (47 millions of pop.)
Social Security Office - SSS(9 millions of formal employees)
Voluntary private insurance
Public & Private Contractor networks
Source: Tangcharoensathien et al. (2010)
Traditional FFS for OPDirect billing FFS(2006+) for OP
FFSuntil 2006, DRG for IP
Capitation for OP
DRG with global budget
Full capitation
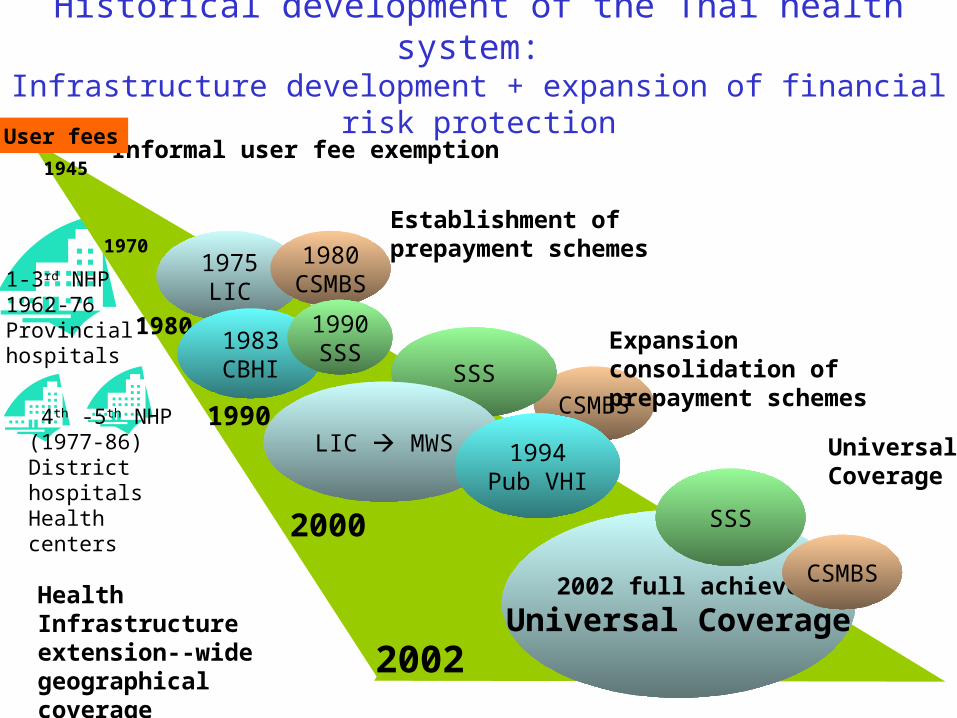
1945
2000
2002
Informal user fee exemption
1980
1970
User fees
1-3rd NHP1962-76Provincial hospitals
Health Infrastructure extension--wide geographical coverage
Historical development of the Thai health system: Infrastructure development + expansion of financial risk
protection
1975LIC
1990
Establishment of prepayment schemes
1983CBHI
1980CSMBS
1990SSS
Universal Coverage
CSMBS
2002 full achieve
Universal Coverage
SSS
LIC MWS 1994Pub VHI
CSMBS
SSS
Expansion consolidation of prepayment schemes
4th -5th NHP (1977-86) District hospitalsHealth centers

Significant reduction in catastrophic health expenditure and gaps of household out-of-pocket payments for health
between rich and poor
8.17
4.82
3.74 3.65
2.87 2.57 2.451.99
1.641.27
4.58
3.673.29
2.782.38 2.22 2.06
1.68 1.55 1.27
2.05 1.95 1.69 1.66 1.74 1.68 1.66 1.83 1.742.18
0
1
2
3
4
5
6
7
8
Decile
1
Decile
2
Decile
3
Decile
4
Decile
5
Decile
6
Decile
7
Decile
8
Decile
9
Decile
10
Hea
lth
pay
men
t :
Inco
me
(%)
1992
1994
1996
1998
2000
2002
2004
2006
2008
Incidence of catastrophic health expenditure 2000 to 2006, Thailand, exceed 10% of total household income
0.9%
4.0%
3.3%
5.4%
2.0%
0%
1%
2%
3%
4%
5%
6%
2000 2002 2004 2006
Q1 (poorest) Q5 (richest) All quintiles
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
45,000
50,000
Co
nsu
mp
tion
exp
en
ditu
re p
er
cap
ita (
Ba
ht)
0 10 20 30 40 50 60 70 80 90 100Cumulative percent (in ascending order of consumption expenditure)
Post-health OOP Pre-health OOP Poverty line
Health impoverishment -Thailand, 2008
0
1,000
2,000
3,000
4,000
5,000
0 5 10 15 20 25 30 35 40
11.0% 3.0%
0.71%
0.38%
0.75%
0.22%
0.57%
0.22%
0.37%
0.15%
0.56%
0.15%
17.1% 6.0% 12.8% 4.5% 11.1% 3.6% 10.3% 3.1%
Rural Urban Rural Urban Rural Urban Rural Urban Rural Urban
2002 2004 2006 2007 2008
Pre-health OOP impoverished Post-health OOP impoverished
Source: Analysis from household socio-economic surveys (SES) in various years 1992-2008, NSO - Thailand

5
Inte
rna
tio
na
l H
ea
lth
Po
lic
y P
rog
ram
-T
ha
ila
nd
Inte
rnati
onal H
ealt
h P
olic
y P
rogra
m -
Thaila
nd
Inequity in geographical distribution of doctors and nurses in 2007
Physicians
800-3,3053,306-6,2746,245-9,2729,243-12,300
Nurses
280 - 652653 - 904905 - 1,1561,157 – 1,408

49% 48%51%
47% 47%
52%50% 51% 53%
55% 55% 55% 56%54%
51%
24%22% 23% 23%
25% 24%22%
18%
30%26% 26%
28% 27% 27% 26%
23%21%
22%20%
24%22%
24% 24% 24% 26%28% 27%
29% 28% 28%
0%
10%
20%
30%
40%
50%
60%
Qtr1
Qtr2
Qtr3
Qtr4
Qtr1
Qtr2
Qtr3
Qtr4
Qtr1
Qtr2
Qtr3
Qtr4
Qtr1
Qtr2
Qtr3
2004 2005 2006 2007
CS
SS
UC
45%47% 48%
50%52% 50% 51%
53% 54% 55% 56%54% 56% 58% 59%
17% 17% 16% 17%18%
20% 20% 22% 21% 20% 19% 20%
16% 16% 17% 17% 18% 18% 19% 20% 20% 20% 20% 20% 20% 21% 21%
0%
10%
20%
30%
40%
50%
60%
Qtr1
Qtr2
Qtr3
Qtr4
Qtr1
Qtr2
Qtr3
Qtr4
Qtr1
Qtr2
Qtr3
Qtr4
Qtr1
Qtr2
Qtr3
2004 2005 2006 2007
CS
SS
UC
Cesarean section Laparoscopic cholecystectomy
Use of expensive proceduresUse of expensive proceduresVariations across 3 public insurance schemesVariations across 3 public insurance schemes
Source: Limwattananon et al. (2009)

Angiotensin II receptor blockers
0
5
10
15
20
25
30
35
40
45
50
Jan
Apr Ju
l
Oct
Jan
Apr Ju
l
Oct
Jan
Apr Ju
l
Oct
Jan
Apr Ju
l
Oct
Jan
Apr Ju
l
Oct
2003 2004 2005 2006 2007
CS
SS
UC
Single source statins and new antihyperlipidemia
0
5
10
15
20
25
30
35
40
45
50
Jan
Apr Ju
l
Oct
Jan
Apr Ju
l
Oct
Jan
Apr Ju
l
Oct
Jan
Apr Ju
l
Oct
Jan
Apr Ju
l
Oct
2003 2004 2005 2006 2007
CS
SS
UC
Clopidogrel
0
5
10
15
20
25
30
35
40
45
50
Jan
Apr Ju
l
Oct
Jan
Apr Ju
l
Oct
Jan
Apr Ju
l
Oct
Jan
Apr Ju
l
Oct
Jan
Apr Ju
l
Oct
2003 2004 2005 2006 2007
CS
SS
UC
Coxibs
0
5
10
15
20
25
30
35
40
45
50
Jan
Apr Ju
l
Oct
Jan
Apr Ju
l
Oct
Jan
Apr Ju
l
Oct
Jan
Apr Ju
l
Oct
Jan
Apr Ju
l
Oct
2003 2004 2005 2006 2007
CS
SS
UC
Use of expensive OP medicinesUse of expensive OP medicinesVariations across 3 public insurance schemesVariations across 3 public insurance schemes
Source: Limwattananon et al. (2009)

8
Inte
rna
tio
na
l H
ea
lth
Po
lic
y P
rog
ram
-T
ha
ila
nd
Inte
rnati
onal H
ealt
h P
olic
y P
rogra
m -
Thaila
nd
Double-digit cost escalationDouble-digit cost escalationCSMBS’ OP-IP health expenditures CSMBS’ OP-IP health expenditures (1988-2010)(1988-2010)
8Source: Comptroller General Department, Ministry of Finance
-2%
23%
12%13%
20%
12%
6%
10%
-2%
15%
12%
16%
20%46,588
61,304
37,004
54,904
46,481
17,058
26,043
20,476
16,44013,587
9,954
3,1566,000
4,316
62,196
13,905
21,896
30,833
38,803
9,5097,007
1,729 2,337 3,3745,8664,826
45,531
1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Annual growth (real term) Total expenditure (million Baht) Outpatient (million Baht) Inpatient
(Expenditures in nominal term)
1997 Asian economic crisis
and conservative reform
2006 implementation:
- IP DRG system
- OP direct billing

9
Inte
rna
tio
na
l H
ea
lth
Po
lic
y P
rog
ram
-T
ha
ila
nd
Inte
rnati
onal H
ealt
h P
olic
y P
rogra
m -
Thaila
nd
Medium- and long-term HCF modeling by ILO experts in 2008
Expenditure Share in GDP of Financing Agencies - Long-term Trends
0.0
1.0
2.0
3.0
4.0
5.0
6.0
1994 1996 1998 2000 2002 2004 2006 2008 2010 2012 2014 2016 2018 2020 2022 2024 2026
Per
cent
MoPH OthMin LocGovt StateEnterprise CSMBS SocSec UC WCF PrivIns TrafficIns ERBenefits PrivHH NonProfit RoW

Mismatch between increasing burden of disease from NCD and pattern of health expenditure
DALY lost from Risk factors, Thailand 1999 and 2004
943
838
595
594
440
410
238
169
144
132
91
54
53
29
25
1,310
550
490
490
400
370
220
140
370
120
120
60
70
30
40
0 200 400 600 800 1000 1200 1400
Unsafe Sex
Alcohol
Blood pressure
Tobacco
Non-Helmet
BMI
Cholesterol
Low intake of fruit and vegetable
Illicit Drugs
P hysical Inactivity
Air P ollution
WSH
Malnutrition-Inter
Malnutrition-Thai
Non-Seatbelt
DALYs('000)
19992004
Health administration and health insurance
8.5%
Medical goods4.3%
Ancillary services 0.4%
Prevention and public health services
4.8%
Services of curative & rehabilitative care
78.1%
Gross capital formation
3.9%
0
50
100
150
200
250
300
350
400
450
500
Q1 Q2 Q3 Q4 Q5
Thou
sand
s
inactivity
low intake fruit
cholesterol
BMI
Blood pressure
smoking
Alcohol0
50100150200250300350400450500
Q1 Q2 Q3 Q4 Q5
Thou
sand
s
inactivity
low intake fruit
cholesterol
BMI
Blood pressure
smoking
Alcohol
DALYs attributable to risk factors

11
Inte
rna
tio
na
l H
ea
lth
Po
lic
y P
rog
ram
-T
ha
ila
nd
Inte
rnati
onal H
ealt
h P
olic
y P
rogra
m -
Thaila
nd
Structure of Health Information System Development in Thailand
MOPH
Thai Health Promotion Foundation
Health System Research Institute (HSRI)
Health Information System DevelopmentPlan and Networking
NHSO NESDB
Civil societies
NGOs
Professionals
NSO
Academics
Data owners
Steering committee
Management office

12
Inte
rna
tio
na
l H
ea
lth
Po
lic
y P
rog
ram
-T
ha
ila
nd
Inte
rnati
onal H
ealt
h P
olic
y P
rogra
m -
Thaila
nd
Key challenges of the Thai health care system
• Need strong political commitment and support• New health technologies and expensive services long-term
sustainability of health care finance for the UC scheme and primary care,
• An increasing disease burden from chronic NCD and the situation of aging society reallocate more resources to HP and disease prevention,
• Inefficiency and inequitable access to quality health services among beneficiaries of different health insurance schemes harmonization,
• The pandemic of new emerging infectious disease and unsuccessful control of tuberculosis and HIV/AIDS need revitalization,
• Poor governance of the Thai health systems,• Mal-distribution and internal brain drain of human resources for health,• The impact of economic crisis and international trade/agreement on
health of the Thai population, • Adequate investment in health information system M&E, • Long-term capacity building of health system and policy research.
12

13
Inte
rna
tio
na
l H
ea
lth
Po
lic
y P
rog
ram
-T
ha
ila
nd
Inte
rnati
onal H
ealt
h P
olic
y P
rogra
m -
Thaila
nd
ConclusionConclusion
13
Health outcome
Good Poor
Cost
Low Good Health
Low Cost
Poor Health
Low Cost
High Good Health
High Cost
Poor Health
High Cost

14
Inte
rna
tio
na
l H
ea
lth
Po
lic
y P
rog
ram
-T
ha
ila
nd
Inte
rnati
onal H
ealt
h P
olic
y P
rogra
m -
Thaila
nd
Acknowledgements• Ministry of Public Health (MOPH) of Thailand• National Statistical Office (NSO) of Thailand • National Health Security Office (NHSO) of Thailand• Health Systems Research Institute (HSRI), • Health Insurance System Research Office (HISRO) of
Thailand, • World Health Organization (WHO)• London School of Hygiene and Tropical Medicine (LSHTM),
United Kingdom


















