International Experiences with Personal Health Records ... · • Face validity check of...
40
Don E. Detmer, MD, MA President & CEO, American Medical Informatics Association Bethesda, MD Professor of Medical Education, University of Virginia AARP “Does IT Work: Next Generation Care in the Information Age?” Washington, DC 23 March 2006 International Experiences with Personal Health Records & Lessons for U.S. National Policy
Transcript of International Experiences with Personal Health Records ... · • Face validity check of...

Don E. Detmer, MD, MAPresident & CEO, American Medical Informatics Association
Bethesda, MDProfessor of Medical Education, University of Virginia
AARP “Does IT Work: Next Generation Care in the Information Age?” Washington, DC 23 March 2006
International Experiences withPersonal Health Records & Lessons for
U.S. National Policy

• PHR Taxonomy• NHIIs & PHRs:
– Current status & aspirations• Best practice lessons• Take home messages for US Policy• * Study with Detmer & Steen (AMIA)
AARP International Personal Health Record Study*:
Australia, Canada, England & New Zealand

3500 members from 42 nations
Physicians; nurses; pharmacists; computer, information, & behavioral scientists; biomedical engineers; academic researchers; educators; IT managers; related corporate partners
http://www.amia.org
American Medical Informatics Association

• Review of government materials/websites & related published & other available literature
• Structured interview of 11 acknowledged national &/or international experts- Telephone (9) & e-mail (2)
• At least 2 each for Australia, Canada, United Kingdom, & New Zealand plus experts in Sweden
Study Methods (1)

• Face validity check of preliminary findings with 3reviews & comments from AARP experts
• Conclusions & Recommendations for USA
–Solely by DED & EBS
Study Methods (2)

“An electronic application through which individuals can maintain & manage their health information, & that of others for whom they are authorized, in a private, secure, & confidential environment that allows the individual or other authorized persons to access and share such information.”
ASTM International ePHR Definition E2211-02 Standard

“ If you’ve seen one PHR; you’ve seen one PHR.* ”
Types:
• Paper-based• Computer-based• Computer-based but not linked with care ,
e.g., separately maintained• Fully integrated with clinician’s record
* e-PHRs: A bit like a unicorn: Everyone knows about them but nobody has seen one.

• The Patient has access to: – Appointments – Problem List – Medications – Allergies – Subset of test results – Demographic & Insurance information– Educational materials
• The patient access is via secure internet with their permission. • Patients can request appointments, get meds mailed to them,
securely message their physician, etc. •The Physician sees virtually all information; Some
departments such as addiction medicine is hidden.
Homer Chin, MD, KP
eiPHR (Integrated EMR/PHR) “The Gold Standard”

eiPHR“…beyond satisfaction & into trust.”
Source: Charles Safran

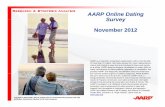
PATIENT Records –Clinic & Hospital
Records
PERSONALRecords –
Consumer & e-health records
PUBLIC HEALTH/POPULATION
Records –Community Records
Data Banks Repositories
Interlocking computer-based health records (C3PRs)supported by knowledge & IT infrastructure
First-classHealth Care
EnvisionedUSA
Infrastructure: Knowledge & Delivery
NCVHS 2002-3

Aging populationsNew technology & treatmentsRising public expectationsAwareness of health system deficienciesPatient demand for greater choice & involvement in decision makingHealth IT underdeveloped in terms of national goals for potential positive impact
Challenges Shared by all FiveHealth Care Systems

Equal access to health servicesRaising qualityImproving health outcomesAchieving sustainable financingImproving efficiencyFostering greater responsivenessCitizen involvement in decision making
System Objectives of all fourHealth Care Systems studied

Patient safety must be assured, & quality of services must be improved.Population health, primary care, & chronic disease management capabilities are pivotal.A robust information infrastructure that enables connectivity among providers is essential.The health system & electronic patient records must be patient-centered & support patient empowerment while maintaining patient privacy.
Guiding Principles of all FourHealth Care Systems

• Strong emphasis on standards to enable connectivity & interoperability.
• Privacy is a priority & is recognized as a greater challenge in those countries where both federal (national) & state/ provincial laws must be aligned. In each of the four countries, a privacy commissioner provides a visible focal point for the development of privacy policy & the enforcement of privacy laws.
• Unique personal health identifiers are planned or are in use at the national level in three of the countries & at the province level in Canada.
• The public is increasingly using the Internet & does so for health purposes much of the time.
Similarities in the HIT Environments of the four nations

Australia: HealthConnectState by state EHR network
Canada: Health InfowaypanCanadian EHR framework built on provincial system
England: Connecting for HealthNew Zealand: Recently revised IT strategy for health
National Approaches to NHII & EHRs

Key Driver: Electronic Medical Record System for Clinical Operations
Key Driver: Population / Public Health Records for Management
PHRs: England’s HealthSpace, etc.; less integrated than NCVHS model
Architecture of NHIIs of Australia, Canada, England & New Zealand
Aspiration for PHRs going forward: Integrate for Chronic Care Purposes

• Limited use of PHRs & ePHRs today.• England’s National Health Service (NHS) offers HealthSpace, a patient-initiated health organizer. • England & Australia plan patient access to part of clinical care records in the future (by 2008 in England), but with limited functionality.• ePHR activity limited to small-scale evaluations• Less private sector focus on ePHRs than in US• No explicit plans for eiPHRs
Findings on ePHRs

Best Practices1. UK implementing ePHR for all citizens within national framework
for EHRs (HealthSpace) - Personal online health organizer
2. Australia & UK provide good examples of consumer engagements
• Australia Consumer Health Forum
• NHS Connecting for Health
3. Canada - significant national public investment; implementation focused on regional needs & status
4. All countries studied ahead of US with regard to privacy framework
5. The European Union e-Citizen program provides a model for improving computer skills among potential ePHR users.

• National patient identifier• Public education needed
– ( see EU e-Citizen program)
• Chronic illness over generally healthy individuals• Payment an issue in non-national health care systems
Other Best Practices:Take Home Messages from Sweden’s SUSTAIN system

PHRs: England, Australia, New Zealand, Canada
National Financing: England, Canada, Australia, New Zealand
Unique Health Identifiers: All
Decision Support Systems: Australia, England, Canada, New Zealand
Educational Strategy:All
NHII Scorecard?

USA OnlyePHRs are a ‘hot topic’Equity of access is not a key
healthcare policyIndividual control/autonomy
emphasized over educationNo policy for personal
authenticationMostly rhetoric & meager Federal $
investment
Conclusions (1) : Consumers/Citizens &National Health Policy Emphasis
Nations Studied
ePHRs not a ‘hot topic’
Policy assures equity of access to care
Education emphasized over patient control
Personal Unique Health ID / National IT Card
Strongest concern is for confidentiality & security over privacy
Action & Substantial $ / £ s

USA – EPRs as ‘hot topic.’
Individual Autonomy & Personal Control; Health through research
Individual Autonomy & Control* ≈ Mistrust & Suspicion
Policy Outcome: Privacy Policy becomes endless debate with health & privacy in conflict
Conclusions (1) : Ascendant Principles for Government’s Role
’Hans, this surgery is a serious business.’- Hans Brinker & the Silver Skates.
Nations Studied - Education as ‘hot topic’.
Social solidarity; Health through services
Social Solidarity ≈ Trust
Policy Outcome: Privacy Policy moves on to dealing with confidentiality, security, & sanctions for breaches
Onora O’Neill: Autonomy and Trust in Biomedical Ethics Cambridge University Press 2001

An idealist believes the short run doesn’t count. A cynic believes that the long run doesn’t matter. A realist believes that what is done or left undone in the short run determines the long run.
- Sidney J. Harris

Identify sponsors to address key policy research questions
One urgent research study: Explore the relative importance of privacy in those care institutions where ‘clicks & mortar’ care options exist & patients may chose to either ‘play or opt out’.
Recommendation 1: Create a focused ePHR/NHII Research Agenda

Is there an optimal approach to introducing ePHRs to large populations? What levels and kinds of resources are needed to support large ePHR
implementations, particularly user support? How do various patient populations (e.g., different ages, healthy versus chronic
versus terminal patients) use ePHRs? Can we quantify the costs and benefits of ePHR systems for individual citizens,
health organizations, & the health system? These evaluations should include costs to consumers (computers, Internet service), costs to the ePHR manager (data management & transfer), & providers’ costs of interacting with PHRs. The evaluations should seek to measure the benefits to consumers, health providers, & third-party payers.
Can ePHR modules designed abroad to support chronic disease management be adapted for use in the United States? Can ePHR modules developed in the United States be shared among organizations?
Questions for ePHR/NHII Research Agenda

– Nongovernmental entities need to coalesce around a few, central defined policy priorities so that legislation can be passed.
Example: An opt-out personal health identifier for:» Care» Notification via email of IRB approved
research studies
Rec 2: Coalesce around a few priorities in order to advocate effectively for our NHII

Rec 3: Assess whether or not widespread NHII development & eiPHRs are achievable without unique personal health identifiers, including cost implications of differing approaches.
This multinational study would suggest that the answer to this question is ‘no’.

Personal Health Record is a topic of great interest.
USA approach to authentication discussion– Policy debate paralyzed by privacy
"The public fears that a national health information system willeliminate rights to privacy and consent.“
• Privacy Advocate’s Testimony to Energy and Commerce Subcommittee on Health. March 16, 2006.
*see Commission on Systemic Interoperability report
Needed: A USA Approach to Personal Authentication*

National Authentication Policy essential to get information relating on the right patient to the right person. Otherwise,
Neither good careNor good privacy protection
Options: Opt outOpt inStatus Quo: bumping along
PHRs & Unique Personal Identifier

AARP in concert with others, e.g., AMIA’ Got EHR?’, should study the EU’s e-Citizen program & adapt it for US use to engage serious health, computer, & numeracy literacy issues.
Rec 4: Invest in programs that increase citizen eiPHR education & skills.

• Considerations– Collaborate with WHO &
others to set standards– Give free access for all to
standards on NLM PubMedsite
Rec 5: Work to ensure that the US government becomes a key player in global
terminology & classification systems.

The Message
“In the absence of a national commitment and financial support to build a national health information infrastructure, the committee believes that progress on quality improvement will be painfully slow.”– Crossing the Quality Chasm: A New Health System
for the 21st Century, IOM, 2001

Current Goal of National Health IT Strategy: Transformation
– from Non-system of Costly, Inefficient, Highly Variable Care
– to System that is equitable, safe, patient-centered, efficient, effective, & timely

Will America respond to international experience?


Don E. Detmer, MD, MA 301 657-1291 [email protected]
References
1. Detmer DE. Building the National Health Information Infrastructure for Personal Health, Health Care Services, Public Health, and Research. BMC Med Inform Decis Mak. 2003; 3:1-40.
2. Berner ES, Detmer DE, Simborg D: Will the Wave Finally Break? A Brief View of the Adoption of Electronic Medical Records in the United States. J Am Med Inform Assoc. 2005 January-February;12(1):3-7. Epub 2004 Oct 18.
3. Pagliari C, Sloan D, Gregor P, Sullivan F, Detmer DE, Kahan JP, Oortwin W, McGillivray S: What is eHealth (4): A Scoping Exercise to Map the Field. JMIR 2005 (Mar31); 7(1):e9. see http://www.jmir.org/2005/1/e9/
4. Detmer DE, Singleton P. Policy for Informed Patients: A European Perspective. Harvard Health Policy Review Harvard Health Policy Review 2004 Spring;5(1)81-88.
5. Kalra P, Singleton P, Ingram D, Milan J, MacKay J, Detmer D, Rector A: Security and Confidentiality Approach for the Clinical E-Science Framework (CLEF) Methods Inf Med 2005; 44: 193-7.
6. Melzer D, Detmer D, and Zimmern R: Pharmacogenetics and Public Policy: Expert Views in Europe and North America. Pharmacogenomics 2003; 4:689-91.
With AARP’s leadership, it will. Thank you & best wishes.

AMIA Initiatives

American Medical Informatics Association
http://www.amia.org

Available in PMC 12 months after publication.NIH supported ~31% of 2004 articles

Annual Symposium• Strong tutorial program
– Primer series– EHR series– Methods series– Selected topics series
• Late breaking policy sessions
David Bates, MD, Program Chair