International AIDS Conference 2014: A Moderately Rapid Review
73
The UC San Diego AntiViral Research Center sponsors weekly presentations by infectious disease clinicians, physicians and researchers. The goal of these presentations is to provide the most current research, clinical practices and trends in HIV, HBV, HCV, TB and other infectious diseases of global significance. The slides from the AIDS Clinical Rounds presentation that you are about to view are intended for the educational purposes of our audience. They may not be used for other purposes without the presenter’s express permission. AIDS CLINICAL ROUNDS
-
Upload
uc-san-diego-antiviral-research-center -
Category
Health & Medicine
-
view
263 -
download
1
description
Jill Blumenthal, M.D., of UC San Diego AntiViral Research Center, presents "International AIDS Conference 2014: A Moderately Rapid Review" at AIDS Clinical Rounds
Transcript of International AIDS Conference 2014: A Moderately Rapid Review

The UC San Diego AntiViral Research Center sponsors weekly presentations by infectious disease clinicians, physicians and researchers. The goal of these presentations is to provide the most current research, clinical practices and trends in HIV, HBV, HCV, TB and other infectious diseases of global significance. The slides from the AIDS Clinical Rounds presentation that you are about to view are intended for the educational purposes of our audience. They may not be used for other purposes without the presenter’s express permission.
AIDS CLINICAL ROUNDS
International AIDS Conference 2014: A Moderately Rapid Review
Jill Blumenthal, MD AIDS Rounds
8/8/2014

Overview
• HIV • HCV • PrEP • Most Innovative Implementation
Strategies









HIV

MODERN Study - Maraviroc (MVC) Once Daily With Darunavir/Ritonavir(DRV/r) Compared to
Tenofovir/Emtricitabine (TDF/FTC) With DRV/r: 48-Week Results
• Why MVC + boosted PI regimen? – Nucleoside toxicity-sparing – Daily regimenimproved adherence – Low risk of resistance and preservation of rx
options if virologic failure occurs – MOTIVATE and PK studies support use of MVC
150mg daily with selected ritonavir-boosted PIs – Prevalence of CCR5 tropic virus greatest in
treatment-naive



Conclusions
• MVC 150mg daily in 2-drug rx regimen showed statistically lower rates of viral suppression when compared to 3-drug regimen of TDF/FTC + DRV/r in naïve subjects over 48 weeks – termination of study 10/13
• Comparable efficacy by tropism assay used at screening
• Majority of PDTFs failed with VL <400 c/mL • No treatment-emergent resistance in either arm • Comparable safety and no unexpected safety
findings
HARNESS study: ritonavir-boosted atazanavir (ATV/r)+raltegravir (RAL) switch study in virologically
suppressed, HIV-1-infected patients
• NRTIs widely used but associated with development of resistance and toxicity/poor tolerability
• HARNESS study conducted to evaluate NRTI-sparing regimen
• Randomized 2:1, open-label, 48-wk, multinational study evaluating switch from 3-drug therapy (including 2 NRTIs) to ATV/r 300/100mg daily + RAL 400mg BID




Conclusions
• Switching to ATV/r+RAL was well tolerated but resulted in higher incidence of virologic rebound than in ATV/r+TDF/FTC group at 24 and 48 weeks
• At week 24, 5 of 7 patients who experienced virologic rebound in ATV/r+RAL arm had low-level viremia
• Major INSTI drug resistance mutations occurred in 1 patient treated with ATV/r+RAL regimen

Dolutegravir versus raltegravir in antiretroviral-experienced, integrase-inhibitor-naive adults with
HIV: week 48 results from the SAILING study • DTG shown to be effective in ART-naïve (SPRING-2 and
SINGLE) and INI-resistant subjects (VIKING-3) • SAILING is a phase 3, randomized 1:1, double-blind,
active-controlled, non-inferiority study • Eligible patients had two consecutive VL > 400 c/ml,
resistance to two or more classes of antiretroviral drugs, and had 1-2 fully active drugs for background therapy.
• Received either daily DTG 50 mg or BID RAL 400 mg, with investigator-selected background therapy.
• Primary endpoint was proportion of patients with VL < 50 c/mL at week 48
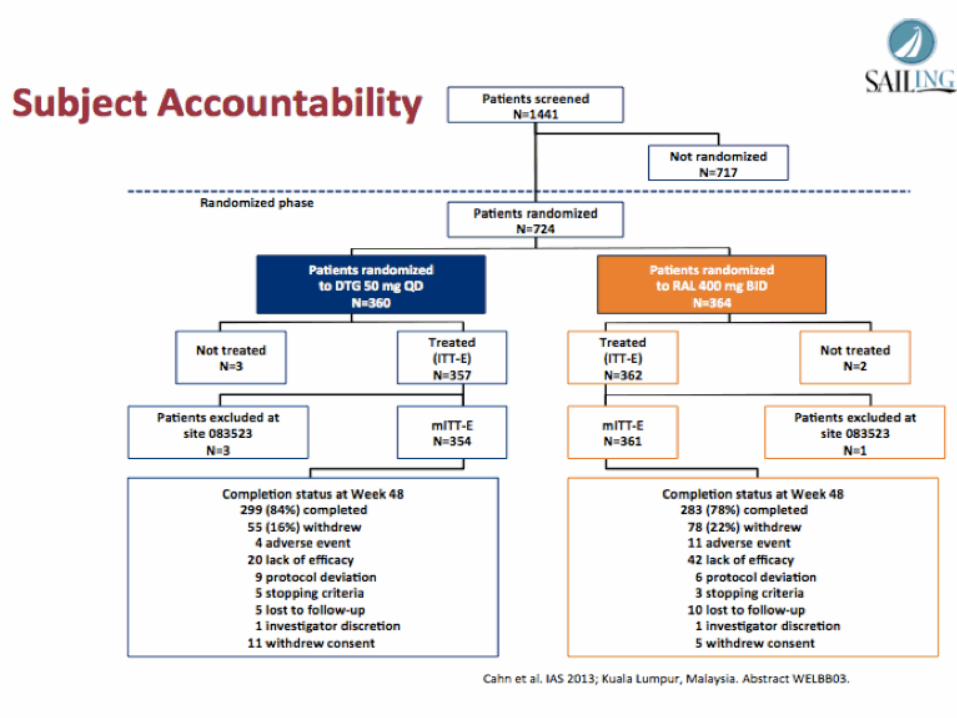



Conclusions
• DTG once daily had higher virologic efficacy when compared to RAL bid in experienced, INI-naïve population – 71% on DTG vs 64% on RAL had VL < 50 c/mL at wk 48
• Similar tolerability and safety profile • Statistical superiority driven by fewer withdrawals
due to lack of efficacy, fewer protocol-defined virologic failures and lower rx-emergent resistance

Major HIV Headlines • No Detectable HIV RNA or DNA in 2 allogeneic HSCT
Australian Patients Still on ART • SALT study: As maintenance therapy, ATV/r plus 3TC
was non-inferior to ATV/r plus 2 NRTIs • OLE study: As maintenance therapy, LPV/r plus 3TC
was non-inferior to LPV/r plus 2 NRTIs • Less frequent HIV VL monitoring not a/w higher risk of
treatment failure among immunologically stable HIV+ on ART
• HIV RNA between 20-50 c/mL did not increase risk of treatment failure compared to those with HIV RNA < 20 c/mL.

Major HIV Headlines (cont) • SPANC study: Australian study found that more than
half of HSIL lesions regressed spontaneously, making the optimal treatment uncertain.
• CHARTER cohort analysis: Not taking ART, markers of poor general health, and neuropsychiatric comorbidities predicted faster neurocognitive decline
• Male medical circumcision is associated with a reduction of HIV incidence among women in South Africa where MMC roll-out is ongoing (ANRS-12126)
• HDAC inhibitor romidepsin is safe and effectively reverses HIV-1 latency in vivo as measured by standard clinical assays

HCV

All-oral therapy with sofosbuvir plus ribavirin for the treatment of HCV genotypes 1, 2, 3 and 4 infection in
patients co-infected with HIV (PHOTON-2)
• Sofosbuvir (SOF)- NS5B nucleotide polymerase inhibitor with pan-genotypic antiviral activity – high barrier to resistance – 400mg PO daily
• Co-infected patients need effective IFN-free HCV therapy that can be safely given with ART
• Endpoints – SVR12 – Safety


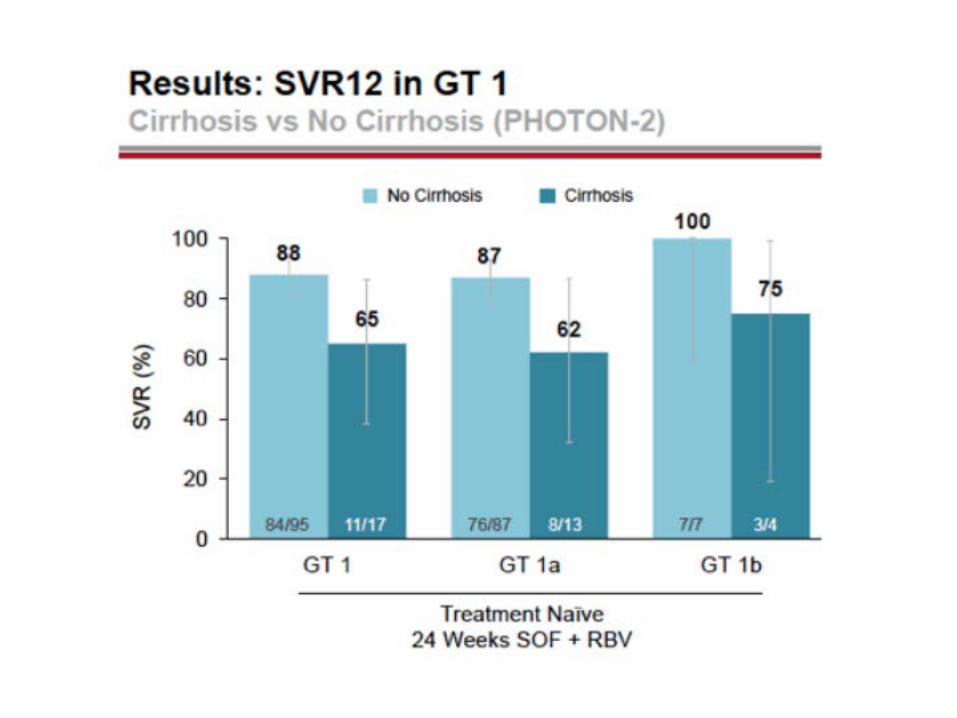




Conclusions
• SVR rates high (>85%) for all genotypes – In G1 treatment-naïve, SVR12 rates significantly higher
in noncirrhotics – In G2-4 with cirrhotics vs noncirrhotics, not as much
difference • No S282T mutations detected by deep
sequencing • SOF well-tolerated with low rate of rx
discontinuations due to AEs • SOF + RBV effectively co-administered with
TDF/FTC + ATV/r, DRV/r, RPV or RAL

SAPPHIRE-II Subgroup Analysis: ABT-450/r/Ombitasvir (ABT-267), Dasabuvir (ABT-333), and Ribavirin Regimen Achieves High Sustained Virologic Response
Rates 12 Weeks Post-treatment in Treatment-experienced Patients With Chronic HCV GT 1 Infection, Regardless of Baseline Characteristics
• ABT-450 is an HCV NS3/4A PI – Co-dosing with ritonavir increases peak, trough and overall
drug exposures • Ombitasvir (ABT-267) is NS5A PI • Dasabuvir (ABT-333) is NS5B RNA polymerase inhibitor • Safety and efficacy from SAPPHIRE-II with 12 week
regimen in non-cirrhotic, treatment-experienced patients with chronic HCV GT1 previously reported SVR12 rate 96.3%
• Logistic regression analysis to explore association between subgroup variables and SVR12


Conclusions
• 96.3% of 297 experienced GT-1 infected patients treated with ABT-450/r/ombitasvir, dasabuvir and RBV achieved SVR12
• SVR12 rates high across subpopulations • Among subgroup variables analyzed in logistic
regression model, only baseline VL a/w likelihood of achieving SVR12

TURQUOISE-I: SAFETY AND EFFICACY OF ABT-450/R/OMBITASVIR, DASABUVIR, AND RIBAVIRIN IN PATIENTS CO-INFECTED WITH HEPATITIS C AND HIV-1


Conclusions
• IFN-free 3D + RBV in co-infected patients, naïve and experienced, cirrhotics vs non-cirrhotics – SVR12 of 93.5% with 12 weeks of therapy – SVR4 of 96.9% with 24 weeks of therapy – When coadministered with ATV or RAL, well-
tolerated with no treatment-emergent serious adverse events

Ledipasvir/Sofosbuvir is Safe and Effective as a Single-Tablet-Regimen for Treatment of Patients with Genotype 1 Chronic
Hepatitis C Virus, Including those with Compensated Cirrhosis
• Ledipasvir (LDV)- NS5A inhibitor with picomolar potency against GT1a and 1b; 90mg PO daily
• Sofosbuvir (SOF)- NS5B nucleotide polymerase inhibitor with pan-genotypic antiviral activity; high barrier to resistance; 400mg PO daily
• LDV/SOF FDC- combination 90/400mg PO daily; no food effect





Conclusions
• 97% of GT-1 pts in LDV/SOF phase III study achieved SVR – Ion-1: LDV/SOF for 12 weeks achieved SVR12 of 99%
in GT-1 naïve and 94% among those w/ cirrhosis – Ion-3: LDV/SOF for 8 weeks achieved SVR12 of 94% in
GT-1 naïve without cirrhosis – Ion-2: LDV/SOF for 12 weeks achieved SVR12 of 94%
in GT-1 who failed PegIFN + RBV + HCV Pis • Adding RBV did not increase SVR12 rates • LDV/SOF STR safe and well-tolerated

Major HCV Headlines
• Interferon-free 3 DAA (ABT-45-/r/Ombitasvir) Plus Ribavirin Regimen in HCV Genotype 1-Infected Patients on Methadone or Buprenorphine Achieved SVR24 of 97.4% (naïve and experienced)
• Hepatic Safety Comparable for DTG to other HIV therapy in INI-naïve Patients– Experienced may be at Greater Risk for Viral Hepatitis-related IRIS
• FIB-4 Predicts Major Liver Complications and Death in HCV+ People Starting ART

PrEP

Early Data Show Good Adherence to Intermittent PrEP by MSM in French Trial (Ipergay)
• Potential benefits of iPrEP – Higher adherence: more convenient dosing
regimen – Improved efficacy
• Coitally-dependent use of TDF gel effect in CAPRISA 004 but daily TDF gel ineffective in VOICE
– Better safety: lower drug exposure (kidneys, bones)
– More cost-effective





Conclusions
• First analysis of adherence showed a very high detection rate of TFV and FTC in plasma with “on demand” PrEP
• Results are encouraging but not demonstration of efficacy
• Second phase of study to be implemented

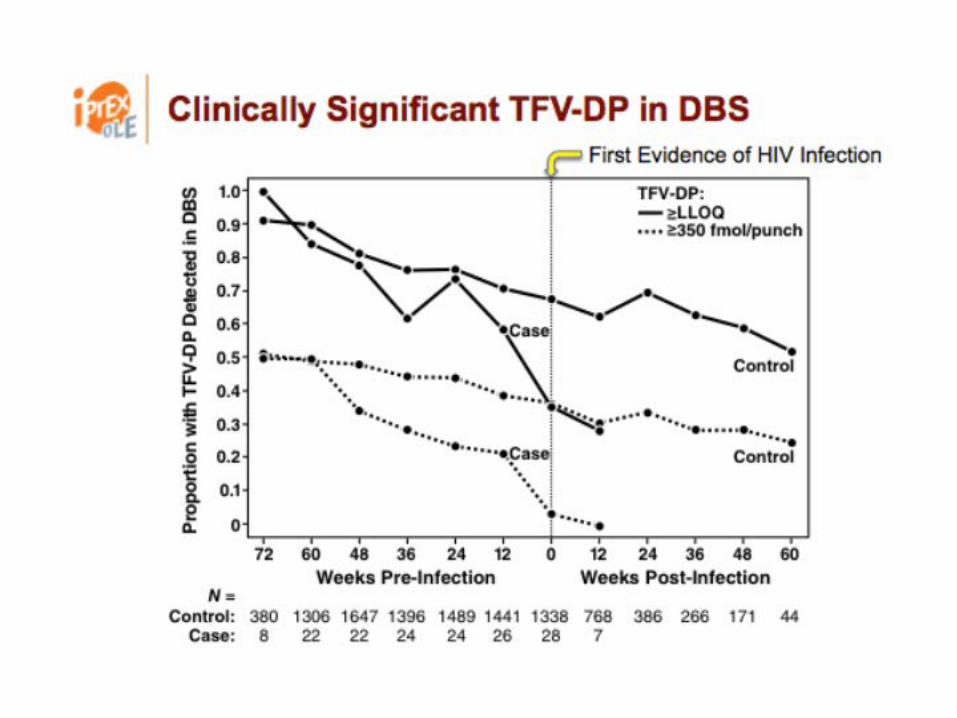
Uptake of pre-exposure prophylaxis, sexual practices, and HIV incidence in men and transgender women who have
sex with men: a cohort study (iPrEX OLE) • iPrEx was first placebo-controlled trial to show that
daily TDF/FTC PrEP lowers the risk of HIV acquisition • Analyzed MSM and transgender women who entered
the open-label extension, iPrEx OLE. – PrEP could be started at any time through week 48, and
follow-up of all participants continued to week 72. • Among 1770 people who enrolled at 11 sites in North
and South America, South Africa, and Thailand, 1603 eligible for PrEP. – 72% started PrEP at enrollment, 6% started PrEP later, and
23% never started PrEP (n=1225 on PrEP)




Conclusions • PrEP uptake is high across broad range of demographic groups
when provided free of charge by experienced PrEP providers • Sexual risk a/w
– Higher retention between randomized phase and OLE – Greater PrEP uptake – Greater adherence
• ***Adherence has to be good, not perfect*** – Risk reduction 84% (95% CI: 21 to 99%) with 2-3 tabs/wk – Risk reduction 100% (95% CI: 86-100%) with >3 tabs/wk
• PrEP fails if people stop while still at risk for HIV • TVF-DP concentrations in DBS are convenient markers of long term
average PrEP use that correlate strongly with PrEP protection

Medical Male Circumcision • A sport-based intervention to increase uptake of voluntary medical male
circumcision among adult male football players: results from a cluster-randomised trial in Bulawayo, Zimbabwe – "Make the Cut" intervention – “Cluster randomized trial” of 3 arms found that VMMC uptake after 3 months
were 9.8-fold higher in the two intervention groups compared to the control group.
• The effect of conditional economic compensation on uptake of voluntary medical male circumcision: a randomized controlled trial of a demand creation intervention for male circumcision in Kenya – RCT of 1504 men – Increasing levels of food voucher economic compensation (no
compensation, US $2.50, US $8.75, US $15.00) resulted in higher levels of VMMC uptake.
– Despite statistically significant increases in uptake, uptake was profoundly low ?level of compensation to achieve higher levels should be increased