
INTERNAL MEDICINE RESIDENTS NOON … MEDICINE RESIDENTS NOON CONFERENCE: INPATIENT GLYCEMIC CONTROL...
48
INTERNAL MEDICINE RESIDENTS NOON CONFERENCE: INPATIENT GLYCEMIC CONTROL Presented by: Leyda Callejas PGY5 Endocrinology , Diabetes and Metabolism Acknowledgements: Dr. P Orlander Dr. V Lavis Dr. N Shah
Transcript of INTERNAL MEDICINE RESIDENTS NOON … MEDICINE RESIDENTS NOON CONFERENCE: INPATIENT GLYCEMIC CONTROL...

INTERNAL MEDICINE RESIDENTS NOON
CONFERENCE:
INPATIENT GLYCEMIC CONTROL
Presented by: Leyda Callejas
PGY5 Endocrinology , Diabetes and Metabolism
Acknowledgements:
Dr. P Orlander
Dr. V Lavis
Dr. N Shah
DEFINITIONS OF GLUCOSE
ABNORMALITIES
• Hypoglycemia is defined a BG level <70 mg/dL
• Mild to moderate hypoglycemia is when BG levels are
between 40 and 69 mg/dL.
• Severe hypoglycemia is when BG is <40 mg/dL.
AACE/ ADA Consensus: Inpatient Hyperglycemia, Endocr Pract. 2009;15(No. 4)
DEFINITIONS OF GLUCOSE
ABNORMALITIES
• Hyperglycemia is defined as any blood glucose (BG) value
>140 mg/dL.
• In patients without a previous diagnosis of diabetes mellitus
(DM) and Hemoglobin A1c (HbA1c) values of < 6.5%
elevated BG may be due to stress hyperglycemia.
• HbA1c values of >6.5% suggest that DM preceded
hospitalization.
AACE/ ADA Consensus: Inpatient Hyperglycemia, Endocr Pract.
2009;15(No. 4)

HYPERGLYCEMIA IN HOSPITALIZED PATIENTS
• Irrespective of its cause, hyperglycemia associated with
adverse outcomes
• Hyperglycemia occurs in patients with known or undiagnosed
diabetes, or it occurs during acute illness in those with
previously normal glucose tolerance (“stress hyperglycemia”)
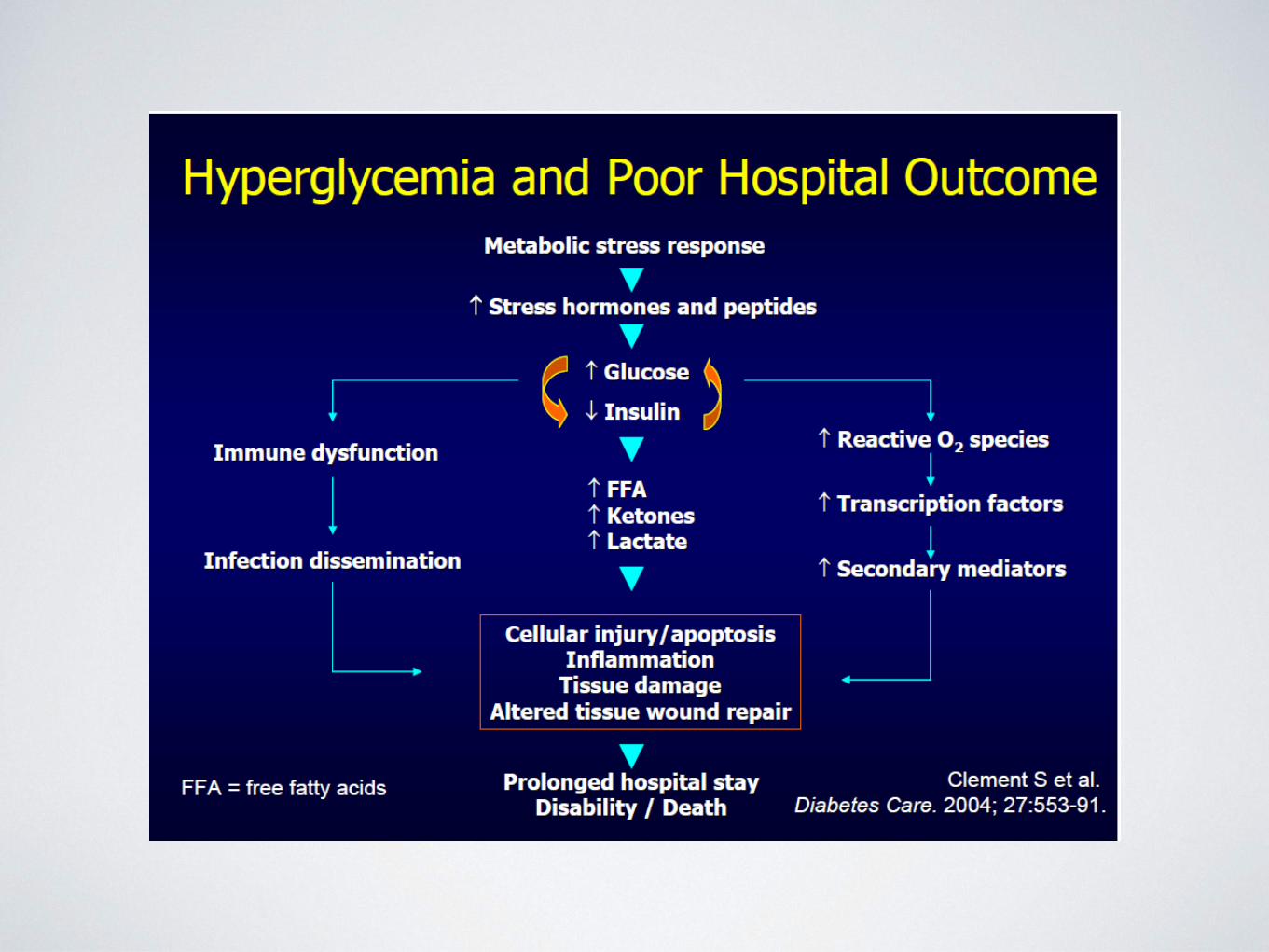
• Possible connections between hyperglycemia and
complications:
• Impaired collagen synthesis
• Impaired WBC function
• Increased production of free radicals and activation of
inflammatory markers
Stress Hyperglycemia
Dungan et al, Lancet 2009 1789-807

SCOPE OF THE PROBLEM OF HYPERGLYCEMIA
IN HOSPITALIZED PATIENTS
• 12 % admissions‐ previously unrecognized DM
or stress hyperglycemia
• 26 % of admissions‐ known DM
• 70 % ‐ non diabetic patients having cardiac
surgery become hyperglycemic( BG > 150)
Umpierrez, JCEM 87:978, 2002
Leibowitz ANN Thor Surg 90:1825, 2010
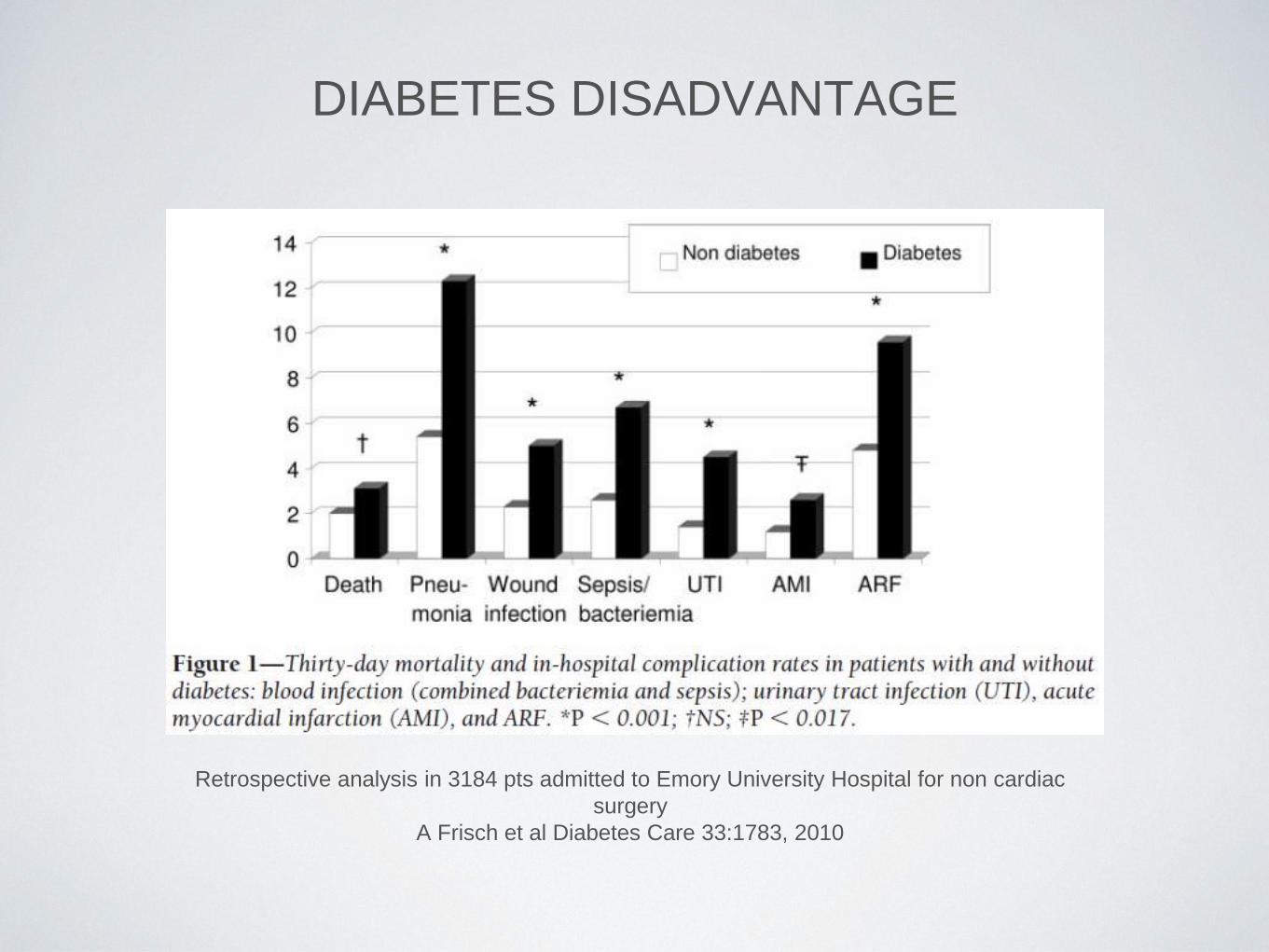
DIABETES DISADVANTAGE
Retrospective analysis in 3184 pts admitted to Emory University Hospital for non cardiac
surgery
A Frisch et al Diabetes Care 33:1783, 2010
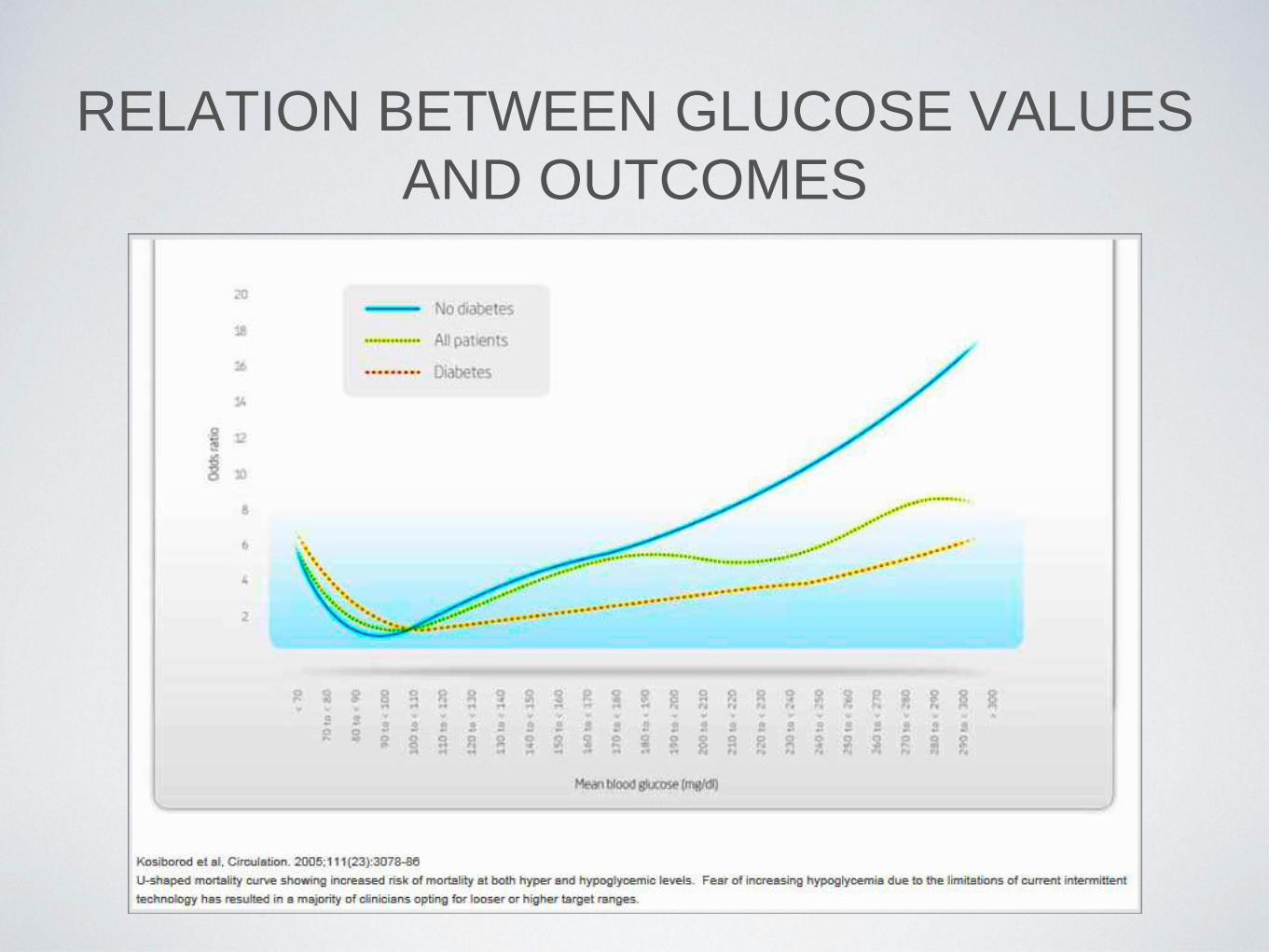
RELATION BETWEEN GLUCOSE VALUES
AND OUTCOMES
CAUSES OF GLUCOSE INSTABILITY IN
HOSPITALIZED PATIENTS
• Changes in nutrition (NPO, enteral, parenteral feedings)
• Changes in clinical status/meds (pressors,
glucocorticoids)
• Prolonged use of SSI as monotherapy
• Failure of clinician to make adjustments
• Poor coordination of BG testing and administration of
insulin
• Poor communication during times of transfer of care
• Poor understanding of when insulin can be held and
when it should be given (DM-1 vs DM-2, long acting vs
short acting)
• Insulin errors (writing and transcription)

TREATMENT OF HYPERGLYCEMIA IN
CRITICALLY ILL PATIENTS

HYPERGLYCEMIA IS ASSOCIATED WITH INCREASED MORTALITY IN ICU PATIENTS, INDEPENDENT OF SEVERITY OF ILLNESS
Hyperglycemia is associated with increased mortality in ICU patients, independent of severity of illness
Mortality risk increases with mean glucose across the entire cohort (n = 259,040) starting at mild hyperglycemia (p < 0.0001). Odds ratios for mortality after adjustment for severity of illness are represented as point estimates with 95% confidence intervals for each mean glucose category; exclusion of unity represents a significant association.
Crit Care Med. Dec 2009; 37(12): 3001–3009.
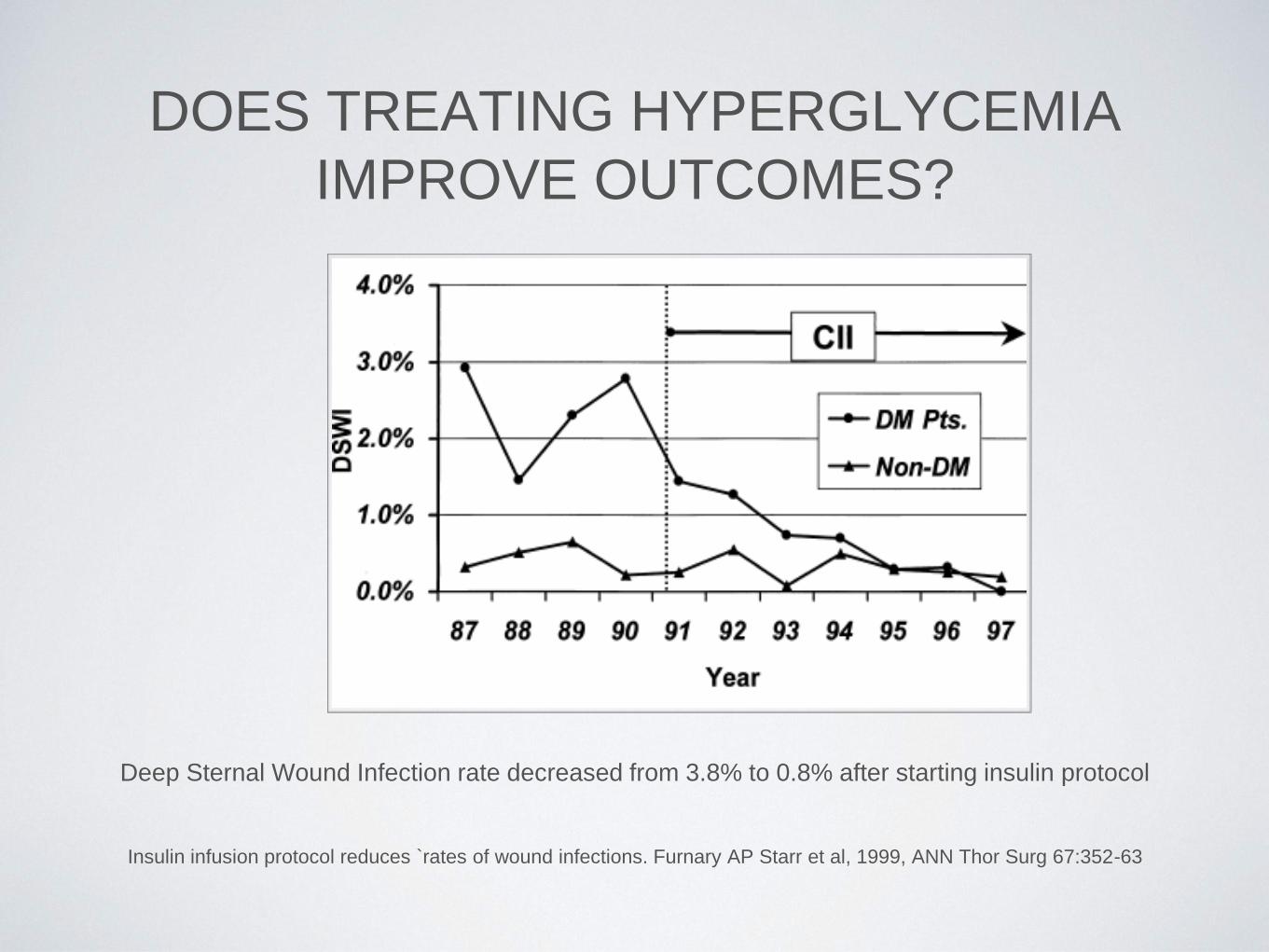
DOES TREATING HYPERGLYCEMIA
IMPROVE OUTCOMES?
Insulin infusion protocol reduces `rates of wound infections. Furnary AP Starr et al, 1999, ANN Thor Surg 67:352-63
Deep Sternal Wound Infection rate decreased from 3.8% to 0.8% after starting insulin protocol
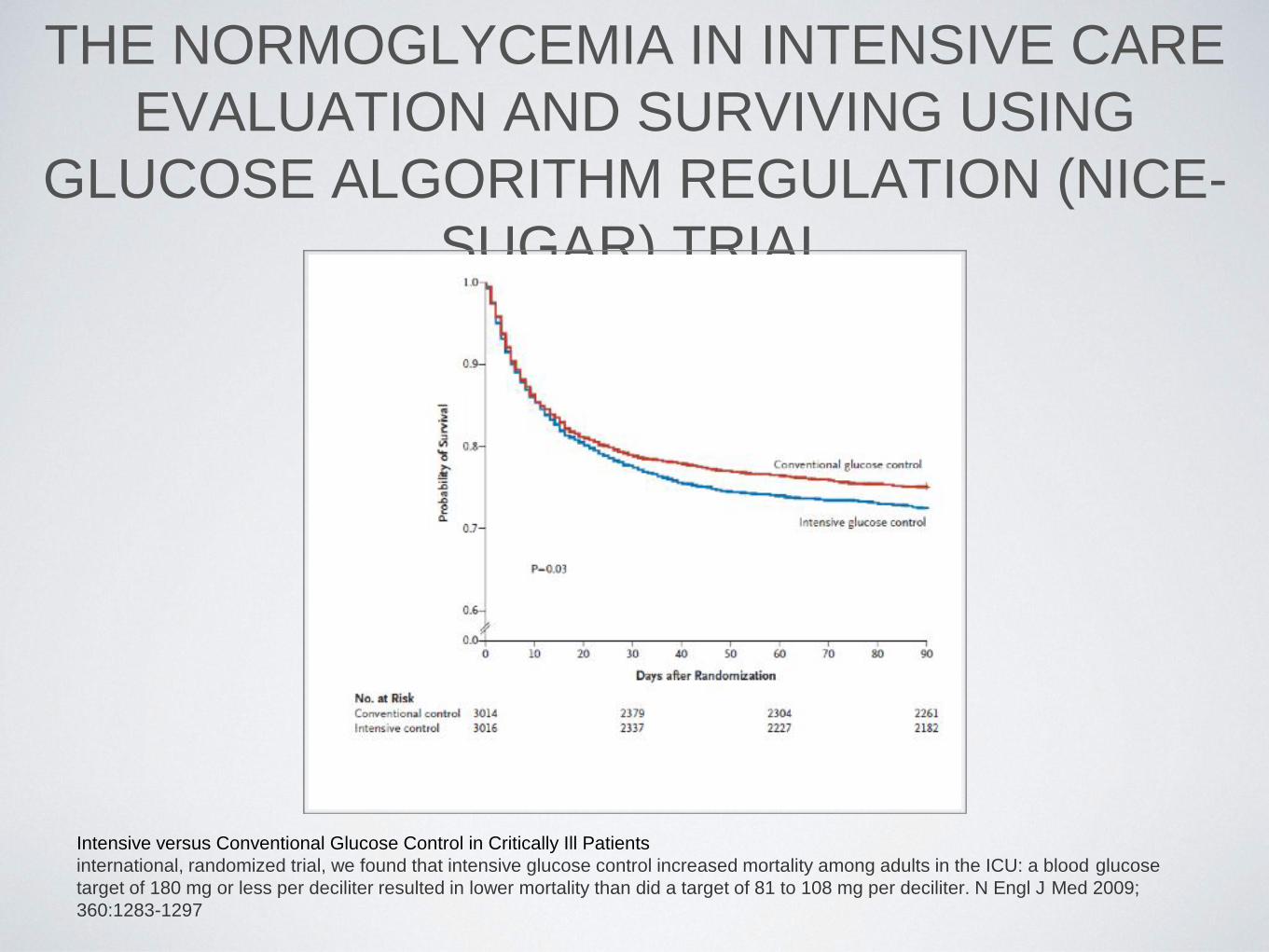
THE NORMOGLYCEMIA IN INTENSIVE CARE
EVALUATION AND SURVIVING USING
GLUCOSE ALGORITHM REGULATION (NICE-
SUGAR) TRIAL
Intensive versus Conventional Glucose Control in Critically Ill Patients
international, randomized trial, we found that intensive glucose control increased mortality among adults in the ICU: a blood glucose
target of 180 mg or less per deciliter resulted in lower mortality than did a target of 81 to 108 mg per deciliter. N Engl J Med 2009;
360:1283-1297


TREATMENT OF HYPERGLYCEMIA IN
CRITICALLY ILL PATIENTS
• Insulin infusion should be used to control hyperglycemia
in the majority of critically ill patients in the ICU setting,
with a starting threshold of no higher than 180 mg/dL.
• Once therapy has been initiated, the glucose level should
be maintained between 140 and 180 mg/dL.
• Targets less than 110 mg/dL are not recommended.
AACE/ ADA Consensus: Inpatient Hyperglycemia, Endocr Pract. 2009;15(No. 4)

ADVANTAGES & DISADVANTAGES OF
INSULIN INFUSION
• Advantages:
• Easily adjustable
• Lower risk for hypoglycemia with higher goals
• Disadvantages:
• Intensive nursing monitoring
• Hourly glucose checks
• Do not address prandial needs
TRANSITION FROM DRIP TO
SUBCUTANEOUS (SC) INSULIN
• Patients with Type 1 and Type 2 DM should receive
first dose of scheduled SC insulin 1-2 hrs before
discontinuing the insulin drip.
• Patients with out a diagnosis of DM but who are
requiring at least 2 units/ hr on the insulin drip should
also be converted to SC insulin

TRANSITION FROM DRIP TO
SUBCUTANEOUS (SC) INSULIN
• In order to calculate insulin requirements you can:
• Review requirements on insulin drip (75-80%)
• Use weight based dosing
• Use home insulin dose as a guide
TREATMENT OF HYPERGLYCEMIA IN
NON-CRITICALLY ILL PATIENTS

TREATMENT OF HYPERGLYCEMIA IN NON-
CRITICALLY ILL PATIENTS
• There is no RCT data for establishing specific
guidelines in non-critically ill patients.
• For the majority of patients on insulin, premeal
glucose targets should generally be <140 mg/ dL in
conjunction with random BG values <180 mg/dL .

TREATMENT OF HYPERGLYCEMIA IN NON-
CRITICALLY ILL PATIENTS
• For avoidance of hypoglycemia, if BG levels decline
below 100 mg/dL see if any changes can be done.
• Modification of the regimen is necessary when BG
values are <70 mg/dL, unless the event is easily
explained by other factors (such as a missed meal)
TREATMENT OF HYPERGLYCEMIA IN NON-
CRITICALLY ILL PATIENTS • Scheduled subcutaneous administration of insulin is the
preferred method for achieving and maintaining glucose
control in non-ICU patients with diabetes or stress
hyperglycemia.
• Non-insulin agents are inappropriate in most hospitalized
patients.
• The recommended components of inpatient subcutaneous
insulin regimens are a basal, a nutritional, and a
supplemental (correction) element
• Should avoid overuse of sliding scale insulin (SSI) for
management of hyperglycemia.
INSULIN THERAPY

PHYSIOLOGIC INSULIN SECRETION
Insulin is secreted into portal system
• Fasting or Basal‐
Low level constantly secreted to decrease hepatic
production of glucose from breakdown of muscle
• Prandial or Bolus‐
Spike in insulin to lower glucose absorbed from food
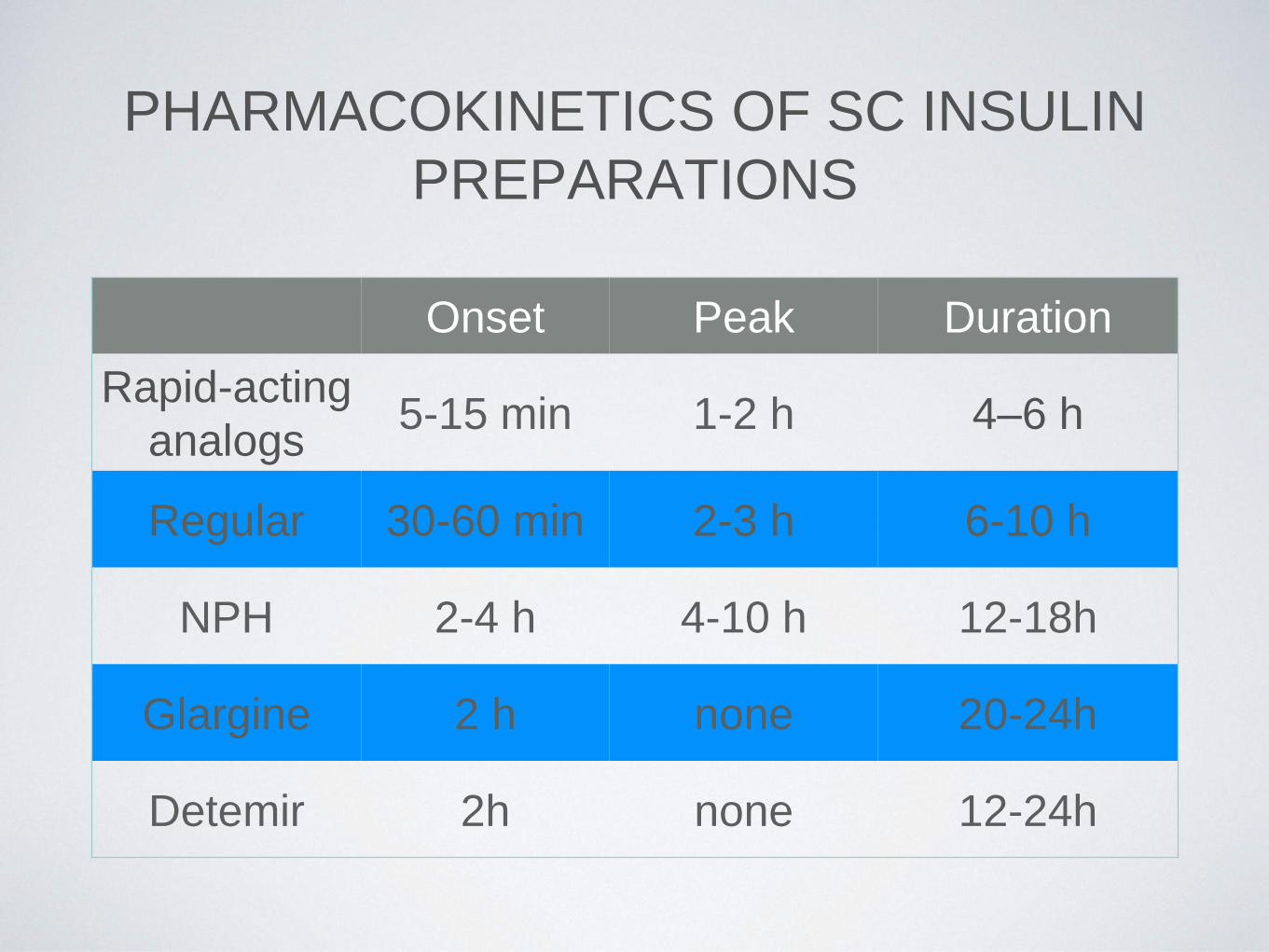
PHARMACOKINETICS OF SC INSULIN
PREPARATIONS
Onset Peak Duration
Rapid-acting
analogs 5-15 min 1-2 h 4–6 h
Regular 30-60 min 2-3 h 6-10 h
NPH 2-4 h 4-10 h 12-18h
Glargine 2 h none 20-24h
Detemir 2h none 12-24h
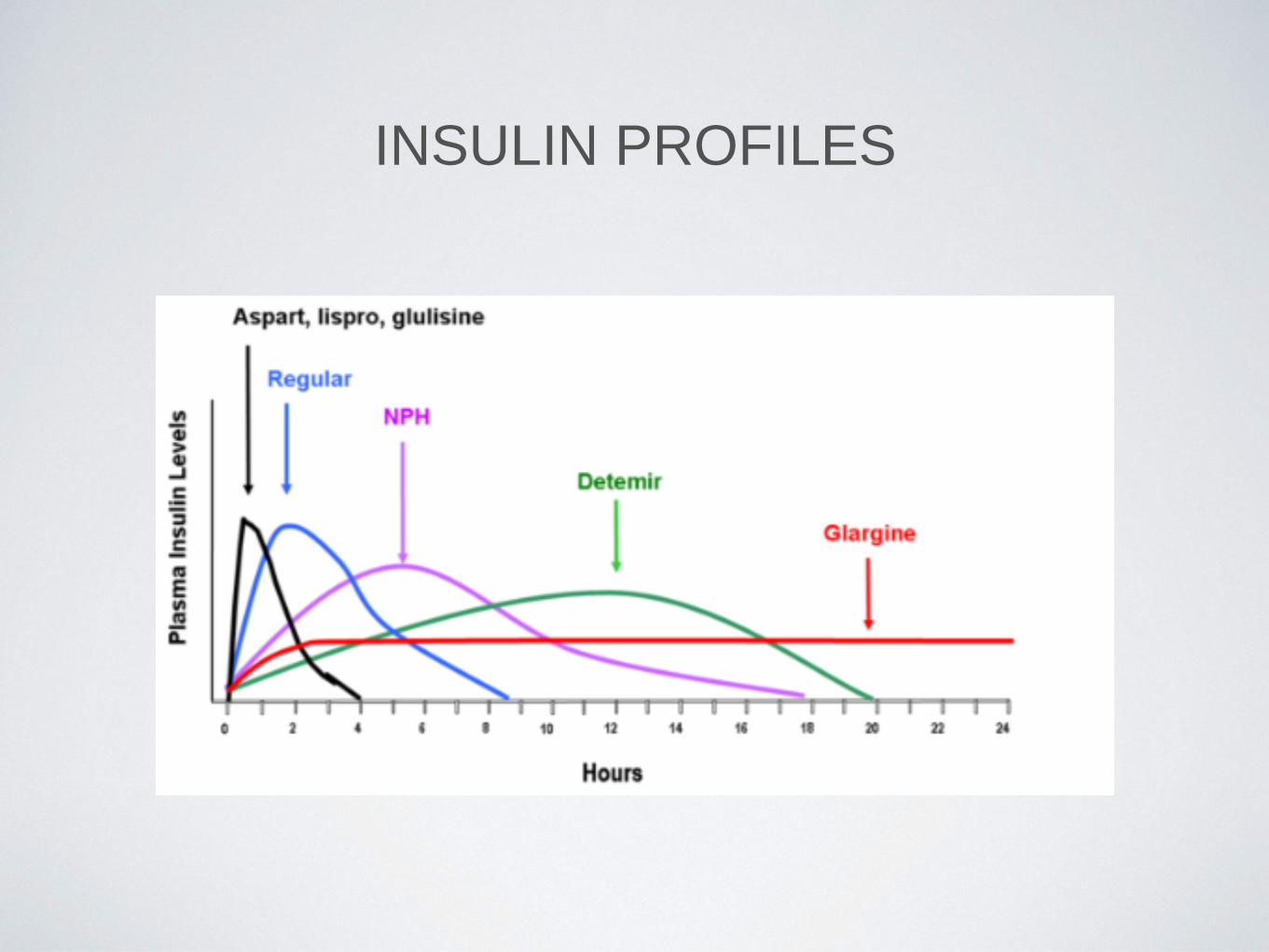
INSULIN PROFILES

COMPONENTS OF MULTIPLE DOSE INSULIN
REGIMEN • Basal‐ Glargine ,NPH, Detemir
•Circulates between feedings
•Restrains glucose production, and catabolism of stored fuels
•Defends against ketoacidosis
•About 50% of daily insulin requirement
•Nutritional / Bolus insulin -Aspart, Glulisine, Lispro, Regular)
•Mimics rapid secretion of insulin in response to feeding
•Promotes assimilation of ingested nutrients
•Moderates post-prandial hyperglycemia
•Correction doses
•Single doses of short or rapid-acting insulin, for short-term adjustment of the
blood sugar over the next few hours
•Usually given in conjunction with meals, as a positive or negative adjustment of
the dose of prandial insulin

ENDOGENOUS INSULIN VERSUS
MULTIDOSE INJECTION REGIMEN
ADVANTAGES OF MULTIDOSE INJECTION
REGIMEN
• Mimics physiological insulinemia
• More opportunities for dosage adjustment
• Can adjust basal & nutritional insulin independently
• Reduced risk of hypoglycemia
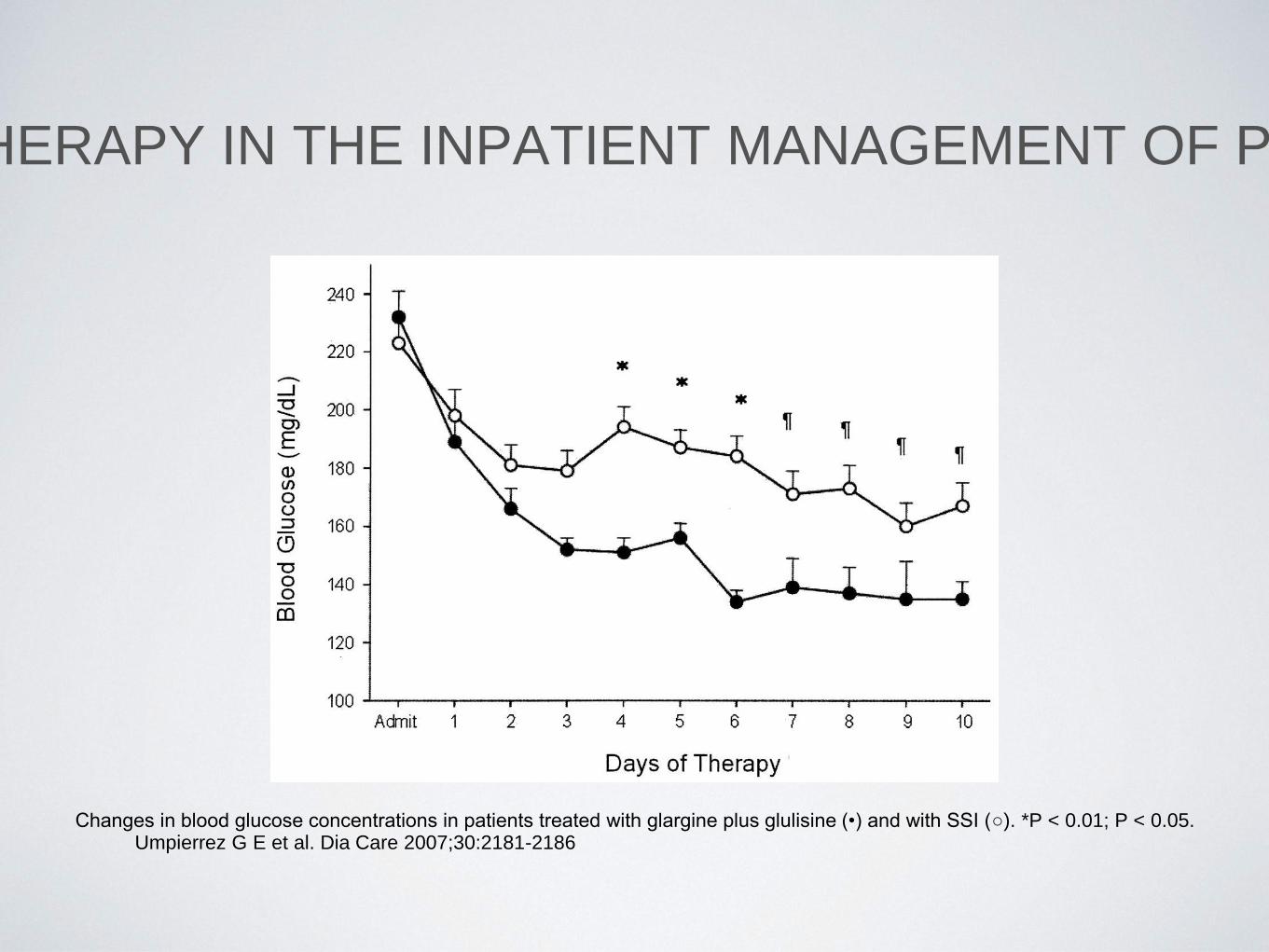
RANDOMIZED STUDY OF BASAL-BOLUS INSULIN THERAPY IN THE INPATIENT MANAGEMENT OF PATIENTS WITH TYPE 2 DIABETES (RABBIT 2 TRIAL).
Changes in blood glucose concentrations in patients treated with glargine plus glulisine (•) and with SSI (○). *P < 0.01; P < 0.05. Umpierrez G E et al. Dia Care 2007;30:2181-2186

Basal Bolus versus SSRI – non-ICU

INSULIN REGIMENS
• Calculate total daily dose of insulin (TDD)
• 0.4 units / kg if BG concentration is 140-200 mg/dl
• 0.5 units / kg if BG is between 201-400 mg/dl
• 0.3 units / kg if elderly / impaired renal function
• Give one-half of total daily dose as basal and one-half
as bolus
Umpierrez et al, Diabetes Care 2007; JCEM 2009; Diabetes Care 2011

INSULIN REGIMENS
• Total daily dose (TDD)
• 1500‐1700 rule
• ISF ( insulin sensitivity factor) = 1500/TDD
• ISF/3 =Insulin to Carbohydrate Ratio
INSULIN REGIMENS
• Give supplemental short acting insulin “sliding-scale” protocol
for blood glucose >150 mg/dl before meals if tolerating PO
and if unable to eat, give scale every 6 h (6–12–6–12).
• Supplemental/sliding scale
• Low dose for TDD < 40 units/ day
• Medium dose for TDD 40‐ 80 units/ day
• High for TDD > 80 units/ day
• Reassess glucose control daily and adjust basal bolus as
indicated (20% change)
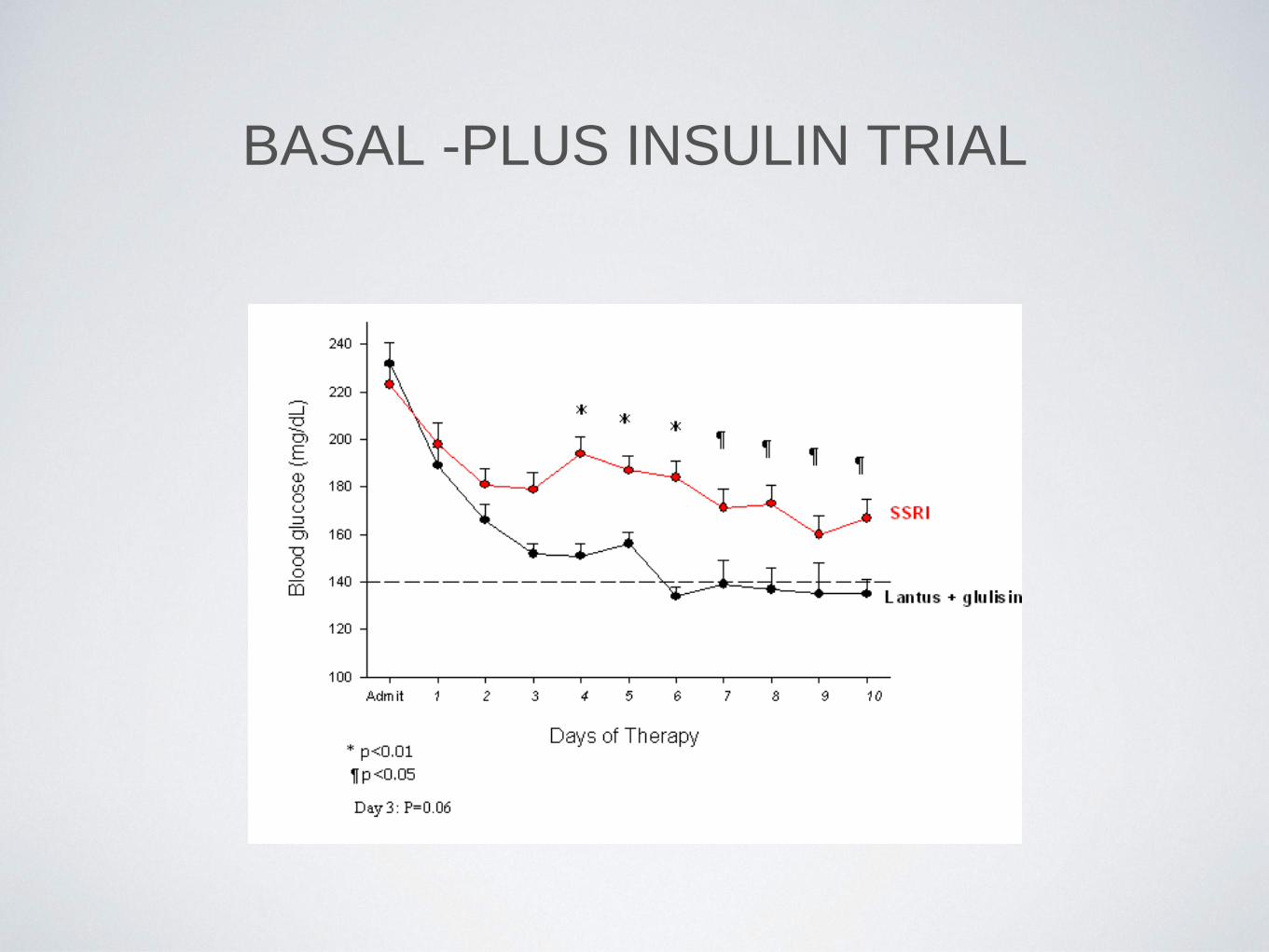
BASAL -PLUS INSULIN TRIAL
SPECIAL
CONSIDERATIONS
STEROID INDUCED HYPERGLYCEMIA
• Elevated postprandial BG , which are disproportionate to
fasting BG levels
• NPH‐ given at time of prednisone administration (0.1
units/kg/day for every 10 mg of prednisone)
• Glargine‐ if using dexamethasone or twice daily
prednisone

CONTINUOUS NUTRITION • TPN
• Add regular insulin to TPN 1unit:10 grams of
carbs
• Can administer correctional insulin Q6H (regular)
• At times the patient might require a basal dose as
well
• Continuous tube feeds
• NPH Q12H for basal needs & regular insulin Q6H
• 70/30 insulin every 6‐8H with SSI

NPO STATUS FOR PROCEDURES
• For a type 1 diabetic do not hold evening dose night
prior to procedure. The patient needs to receive basal
insulin. Can give 1/2 dose prior to procedure and give
dextrose containing IVF and administer a correction
dose after procedure.
• For a type 2 diabetic do not hold evening dose night
prior to procedure. You can omit AM insulin, give 1/2
dose prior to procedure or full dose after procedure

HYPOGLYCEMIA IN HOSPITALIZED
PATIENTS
• The key predictors of hypoglycemic events in
hospitalized patients include older age, greater illness
severity (presence of septic shock, mechanical
ventilation, renal failure, malignancy, and
malnutrition), diabetes, and the use of oral glucose
lowering medications and insulin

HYPOGLYCEMIA AND NEGATIVE
OUTCOMES • Hypoglycemia is associated with an increased risk of
mortality.
• Hypoglycemia is also associated with a prolonged
hospital length of stay .
• Patients with spontaneous hypoglycemia were noted to
have higher rates of in-hospital death (18.4 vs. 9.2% in
those without hypoglycemia; P < 0.001), mortality was
not increased in insulin-treated patients with iatrogenic
hypoglycemia (10.4 vs. 10.2% in those without
hypoglycemia; P = 0.92).
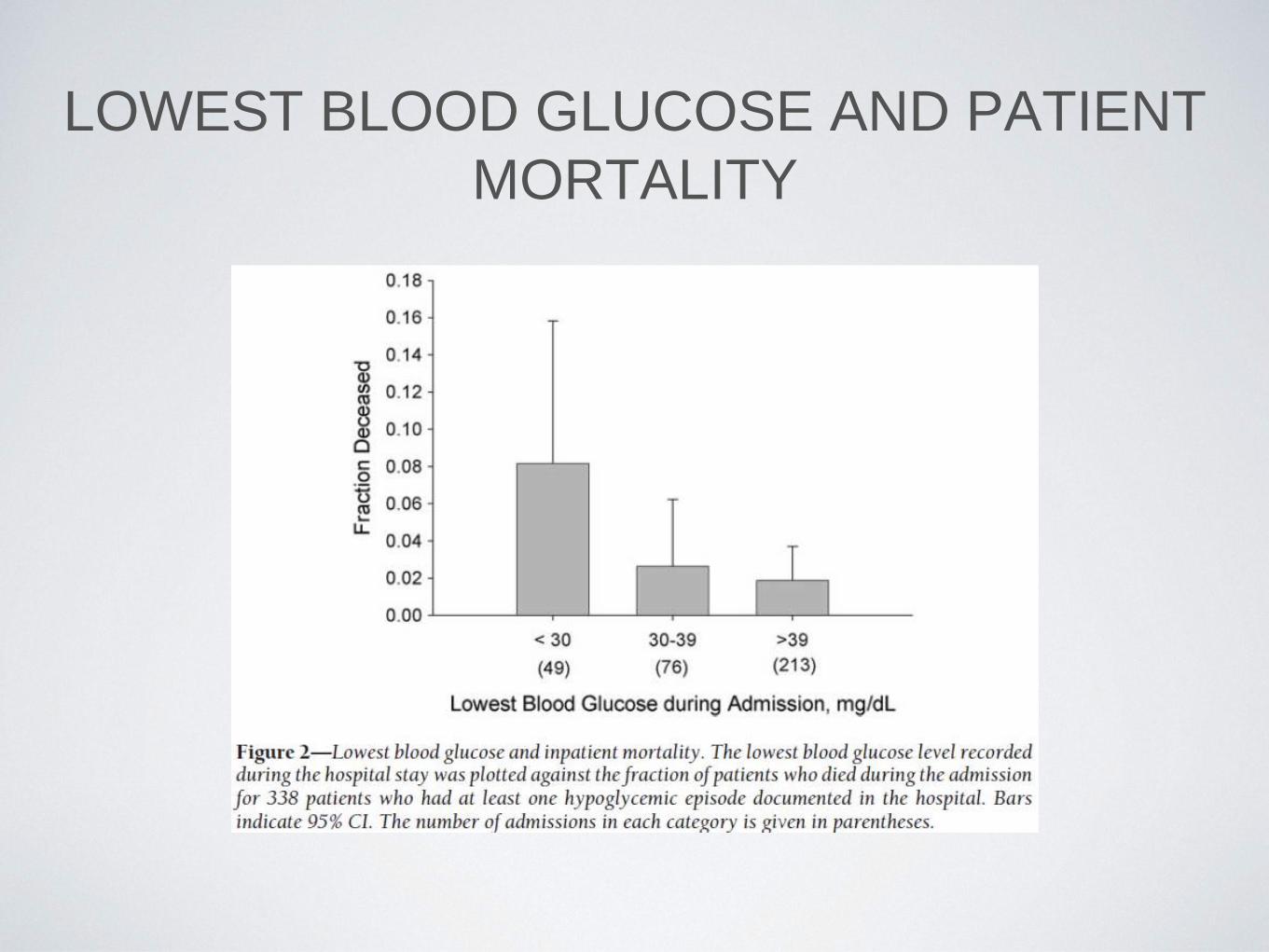
LOWEST BLOOD GLUCOSE AND PATIENT
MORTALITY

STRATEGIES FOR TREATING
HYPOGLYCEMIA • For treatment of BG below 70 mg/dl in a patient who is alert and
able to eat and drink, administer 15–20 g of rapid-acting
carbohydrate such as:
• one–15–30 g tube glucose gel or 4 (4 g) glucose tabs
(preferred for patients with ESRD.
• 4–6 ounces orange or apple juice.
• 6 ounces “regular” sugar sweetened soda.
• 8 ounces skim milk.
• For treatment of BG below 70 mg/dl in an alert and awake
patient who is NPO or unable to swallow, administer 20 ml
dextrose 50% solution and consider starting IV dextrose 5% in
water
STRATEGIES FOR TREATING
HYPOGLYCEMIA
• For treatment of BG below 70 mg/dl in a patient with an
altered level of consciousness, administer 25 ml dextrose
50% (1/2 amp) and consider starting IV dextrose 5% in
water
• In a patient with an altered level of consciousness and no
available IV access, give glucagon 1 mg IM Limit, two
times.
• Recheck BG and repeat treatment every 15 min until
glucose level is at least 80 mg/dl.

INSULIN SUBQ ORDERS FOR PATIENTS ON
PARENTERAL/ENTERAL NUTRITION OR
NPO
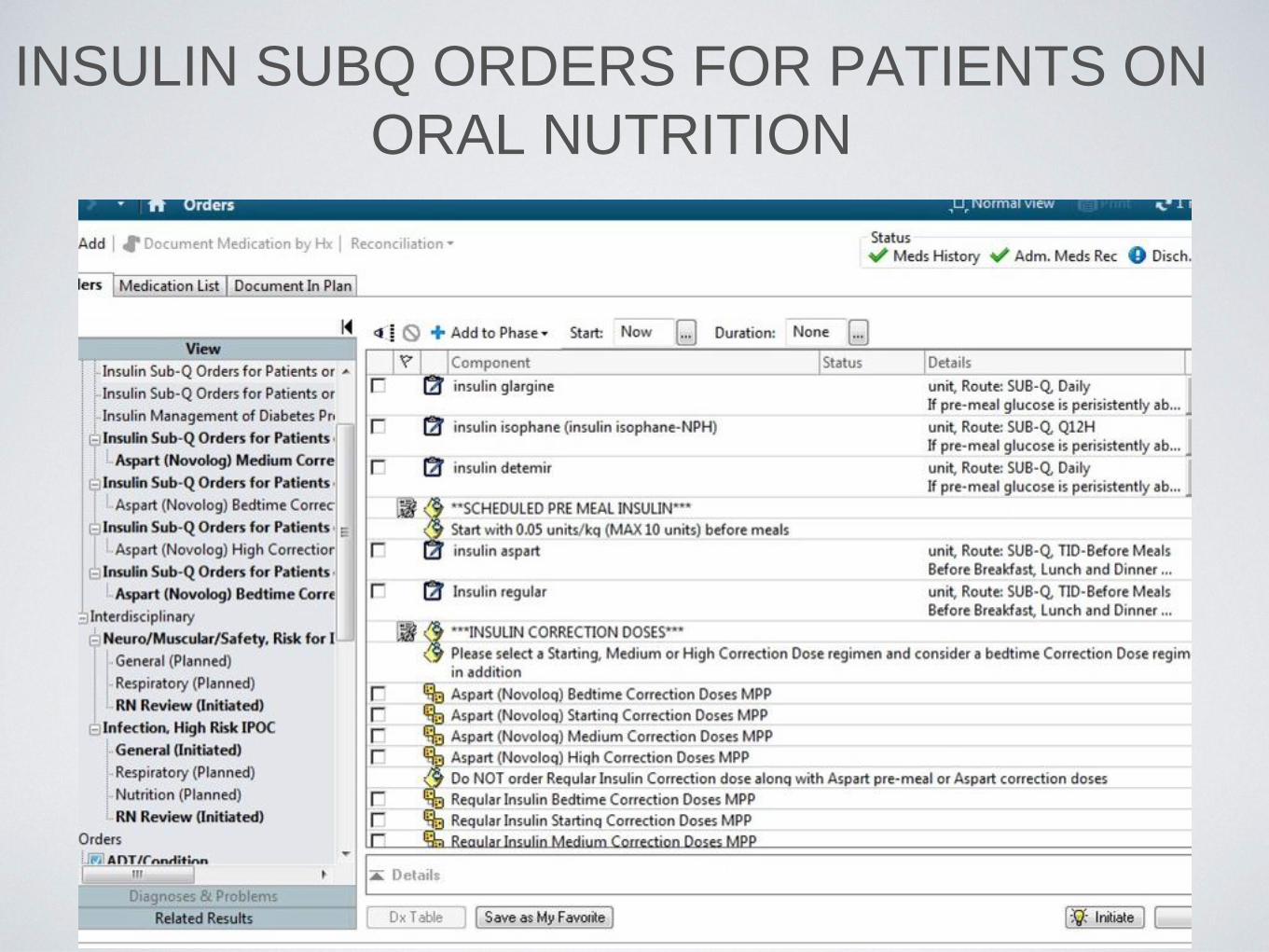
INSULIN SUBQ ORDERS FOR PATIENTS ON
ORAL NUTRITION

Thank you!













![Noon linebyalfonsorodriguezveradelmar1aug15[1]](https://static.fdocuments.in/doc/165x107/55cc58e0bb61eb40288b45e7/noon-linebyalfonsorodriguezveradelmar1aug151.jpg)



