Internal medicine Acute kidney injury
34
Internal medicine Acute kidney injury Presented by: Kholod Hamad MSc Clinical Pharmacy, BCPS
Transcript of Internal medicine Acute kidney injury

Internal medicine
Acute kidney injury
Presented by:
Kholod Hamad
MSc Clinical Pharmacy, BCPS

• Definition and incidence
• Classification and causes
• Clinical manifestations
• Diagnosis and clinical evaluation
• Course and prognosis
• Management
• Non-dialysis treatment of established acute kidney injury
• Renal replacement therapy
Key Points

Introduction
Structure and Function of the kidney
• Primary unit of the kidney is the nephron
• 1 million nephrons per kidney
• Composed of a glomerulus and a tubule
• Kidneys receive 20% of cardiac output

Renal blood flow

The production and elimination of urine requires three basic physiologic events:
1.Blood flow to the glomeruli
2.The formation and processing of ultra filtrate by the glomeruli and tubular cells
3.Urine excretion through the ureters, bladder and urethra

Pathophysiology of Kidney failure
• It is characterised by an abrupt reduction (usually within a 48-h period) in kidney function.
• This results in an accumulation of nitrogenous waste products and other toxins.
• Many patients become oliguric (low urine output) with subsequent salt and water retention.
• In patients with pre-existing renal impairment, a rapid decline in renal function is termed ‘acute on chronic renal failure’.

ACUTE KIDNEY INJURY (FORMERLY ACUTE RENAL FAILURE)
Sudden decline in renal function with increasing BUN/Cr ratio, with or without changes in urine output.
Causative factors:
• Impaired renal perfusion
• Acute renal disease
• Renal ischemia
• Obstructive uropathy.

The RIFLE criteria for the definition and stagingof acute renal disease
• Increased creatinine ×1.5 or GFR decrease >25%Risk
• Increased creatinine × 2 or GFR decrease >50%Injury
• Increased creatinine × 3 or GFR decrease >75% or creatinine > 4 mg per 100 mL (acute rise of >0.5 mg per 100 mL dL)Failure
• Persistent acute renal failure = complete loss of renal function >4 weeksLoss
• Complete loss of kidney function for >3 monthsEnd stage renal disease

Etiology
Causes are generally subdivided into three categories:
1. Prerenal: Most common etiology in children; usually a result of dehydration, although other forms of impaired perfusion can be a cause
2. Renal: a. Parenchymal disease through arterial or glomerular lesions
b. acute tubular necrosis
3. Postrenal: Obstruction of the urinary tract, found often in neonates with anatomic abnormalities

Causes of acute kidney injuryClassification Common clinical disorders
Prerenal(1)
Hemorrhage cardiac myopathy Dehydration renal artery stenosis Severe burns Hypovolemic shock Non steroidalanti-inflammatory drugs
Renal(2)
Drug induced (contrast media, aminoglycosides, amphotericin B)Glomerulonephritis Systemic lupus erythematous
Post renal(3)
Ureter ObstructionMalignancyAnticholinergic drugs Renal calculi

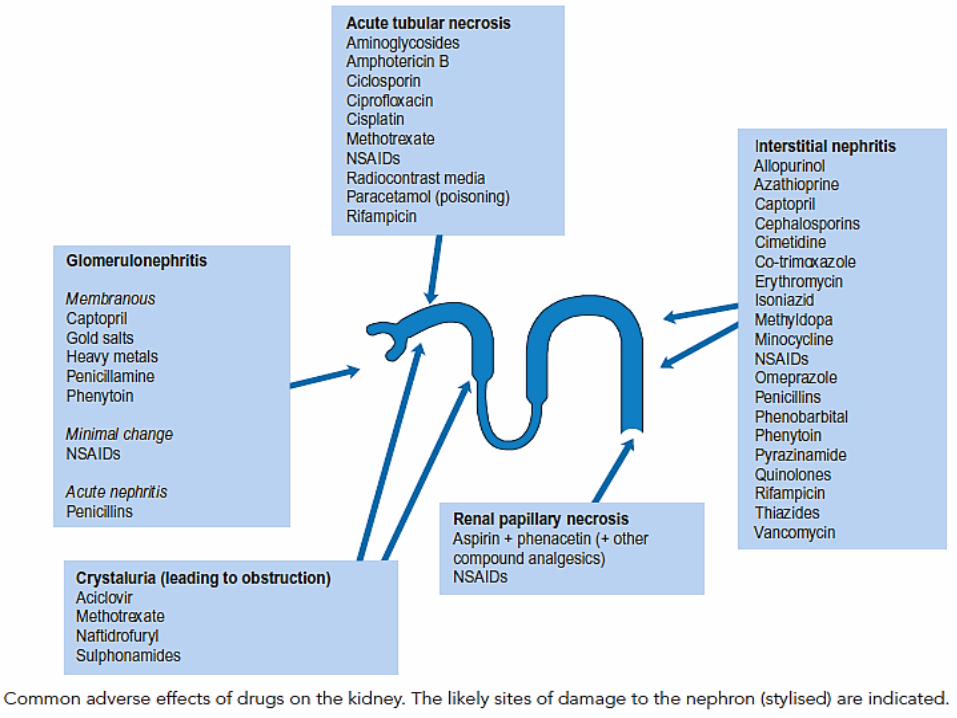
Common clinical factors known to cause acute tubular necrosis
• Hypoperfusion
• Radiocontrast media
• Sepsis
• Rhabdomyolysis
• Nephrotoxin
• Immunosuppressant
• NSAIDs

Clinical Presentation
The hallmark of early renal failure is oliguria

Complications
Often depend on clinical severity; usually includes:
• Fluid overload (hypertension, CHF, pulmonary edema)
• Electrolyte disturbances (hyperkalemia), metabolic acidosis, hyperphosphatemia, and uremia.

Diagnosis and clinical evaluation
• In hospital, AKI diagnosed incidentally by the detection of increasing serum creatinineand/or a reduction in urine output.
• Monitoring fluid balance in acute kidney disease ( BP, Heart sounds, chest X ray, pulsoximetry, skin turgor)
• Monitoring serum electrolytes and acid base balance

The investigations of acute kidney injury
Full history including drug history
Clinical examination, including fluid balance assessment
Urinalysis
Blood examination
Ultrasound scan of renal tract is mandatory

Course and prognosis
• Pre-renal acute kidney injury
The majority of cases will recover within days of onset following prompt correction of the underlying causes
ATN may be divided into three phases:
• Oliguric phase
• Diuretic phase
• Recovery phase

• Post-renal acute kidney injury
• Identification and relief of the obstruction is important
• If the underlying problem is benign then there may be no long-term adverse consequences
• If the cause is due to a malignancy, long-term survival is dependent on whether this can be cured

Management
• Early preventive and supportive strategies
• Identification of patients at risk
• Withdrawal and avoidance of nephrotoxic agents
• Optimization of renal perfusion
• Establishing and maintaining an adequatediuresis

Non-dialysis treatment of established acute kidney injury
Uraemia and intravascular volume overload
• Symptoms of uraemia include nausea, vomiting and anorexia
• Intravascular fluid overload must be managed by restricting NaCl intake to about 1–2 g/day

Hyperkalaemia (normal range 3.5–5.5 mmol/L)
• Dietary potassium should be restricted, and remove K sparing diuretic
• Emergency treatment is necessary if the serum potassium level reaches 7.0 mmol/L or if there are the progressive changes in the electrocardiogram associated with hyperkalaemia.

Emergency treatment of hyperkalaemiaconsists of the following:
• Calcium gluconate to improves myocardial stability
• IV Glucose together with 8–12 units of soluble insulin over 10 min
• Nebulised salbutamol has also been used to lower potassium

Acidosis
• The inability of the kidney to excrete hydrogen ions may result in a metabolic acidosis
• It may be treated orally or IV with sodium bicarbonate
• Extreme acidosis (serum bicarbonate of less than 10 mmol/L) is best treated by dialysis.

Hypocalcaemia and Hyperphosphataemia• Calcium malabsorption, probably secondary to
disordered vitamin D metabolism
• Oral calcium supplementation with calcium carbonate is usually adequate, and although vitamin D
• Hyperphosphataemia can occur in AKI because its execrated by kidney
• Calcium containing phosphate-binding agents may be used to retain phosphate ions in the gut
Infection
• Patients with AKI are prone to infection and septicaemia, which can ultimately cause death.
• Pyrexia must be immediately investigated and treated with appropriate antibiotic therapy
• Samples from blood, urine and any other material such as catheter tips should be sent for culture before antibiotics are started
• Use broad spectrum antibiotic until a causative organism is identified.

Nutrition
There are two major constraints concerning the nutrition of patients with AKI:
• Patients may be anorexic, vomiting and too illto eat
• Oliguria associated with renal failure limitsthe volume of enteral or parenteral nutrition that can be given safely.

• Dialysis allows fluid to be removed and makes parenteral nutrition possible
• The need for protein may occasionally be increased in haemodialysis
• Dialysis leads to remove of many materials, vitamins and electrolytes
• Check for glucose, PH, Ca, Ph, albumin

Renal replacement therapy
Generally, replacement therapy is urgently indicated in AKI to:
1. Remove uraemic toxins when severe symptoms are apparent
2. Remove fluid resistant to diuretics
3. Correct electrolyte and acid–base imbalances

Forms of renal replacement therapy
The common types of renal replacement therapy used in clinical practice are:
• Haemodialysis: The patient's blood and a dialysis
solution are positioned on opposing sides of a semi-permeable membrane across which exchange of metabolites
occurs.
• Peritoneal dialysis: fluid may be instilled in the
peritoneum (fill), allowed to dwell for a specified time, and then drained. Solutes and fluid diffuse across the peritoneal
membrane.
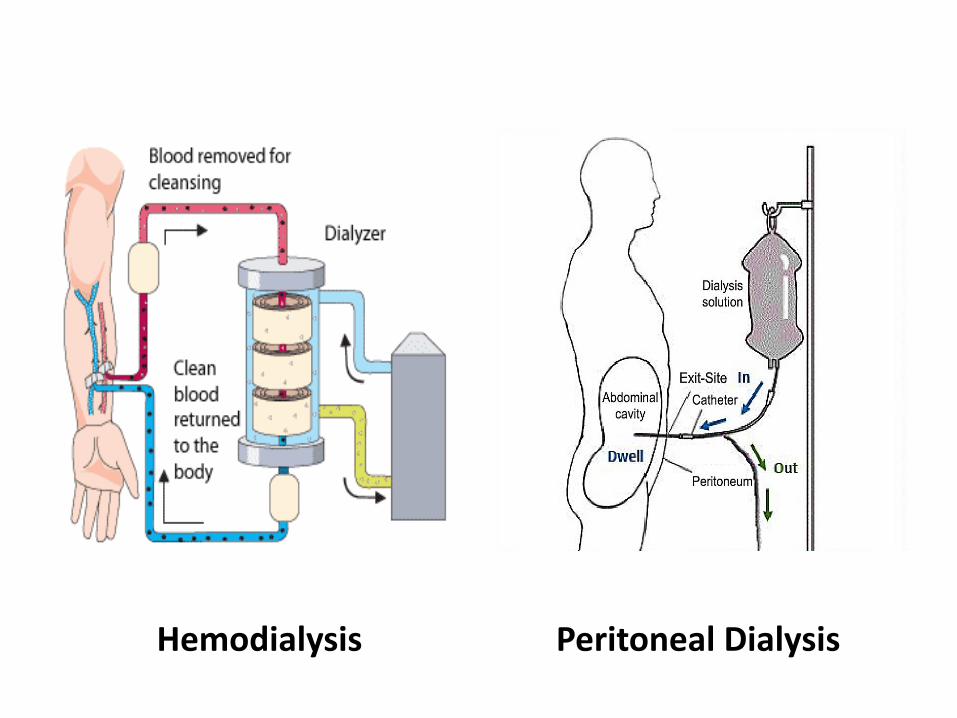
Hemodialysis Peritoneal Dialysis

Drug dosage in renal replacement therapy
Drug factors that favors clearance include: • Low molecular weight • High water solubility • Low protein binding• Small volume of distribution • Low metabolic clearance • Duration of dialysis procedure • Rate of blood flow to dialyser• Surface area and porosity of dialyser• Composition and flow rate of dialysate

The pharmacokinetic behavior of many drugs
may be altered in renal failure
• Absorption Oral absorption in AKI may be reduced by vomiting or diarrhea
• Metabolism renal metabolized drugs doses should be reduced
• Distribution presence of oedema or ascites increases the volume of distribution Serum protein binding may be reduced owing to either protein loss or alteration in binding caused by uraemia
• Excretion drug dosage adjustments

Characteristics of ideal drug to use in patient with renal failure
• No active metabolites
• Disposition unaffected by fluid balance changes
• Disposition unaffected by protein binding changes
• Response unaffected by altered tissue sensitivity
• Wide therapeutic margin
• Not nephrotoxic














