
Intern Boot Camp: Sepsis Cassie Kovach PGY-3. Outline/Objectives Identification of sepsis Work up of...
46
Intern Boot Camp: Sepsis Cassie Kovach PGY-3
-
Upload
collin-jackson -
Category
Documents
-
view
228 -
download
0
Transcript of Intern Boot Camp: Sepsis Cassie Kovach PGY-3. Outline/Objectives Identification of sepsis Work up of...
Intern Boot Camp:Sepsis
Cassie KovachPGY-3
Outline/Objectives
• Identification of sepsis• Work up of sepsis• Triaging sepsis• Treatment of sepsis
Outline/Objectives
• Identification of sepsis• Work up of sepsis• Triaging sepsis• Treatment of sepsis
Sepsis is a continuum
• SIRS (Systemic Inflammatory Response Syndrome)• Sepsis• Severe sepsis• Septic shock
SIRS Physiology
• Inflammatory state affecting the whole body• Release of cytokines
acute phase reaction fever, leukocytosis vasodilation/vascular leak hypotension, tachy,
edema, hypoxemia, tissue hypoperfusion
• Non-specific
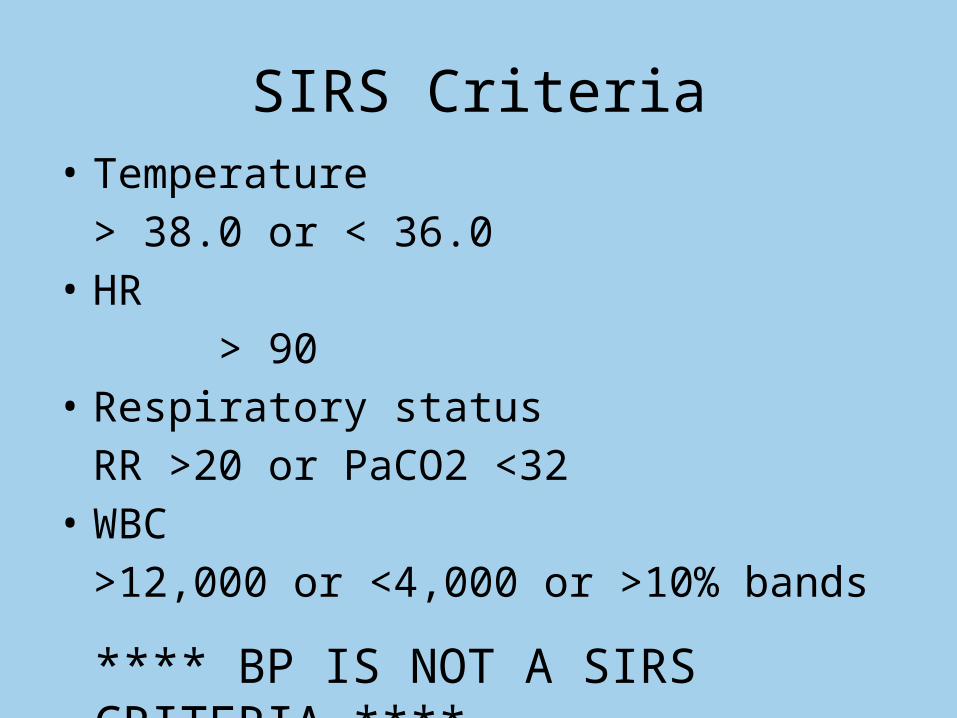
SIRS Criteria• Temperature
> 38.0 or < 36.0• HR
> 90• Respiratory status
RR >20 or PaCO2 <32• WBC
>12,000 or <4,000 or >10% bands
**** BP IS NOT A SIRS CRITERIA ****
Sepsis
• 2/4 SIRS criteria + identified or suspected infection
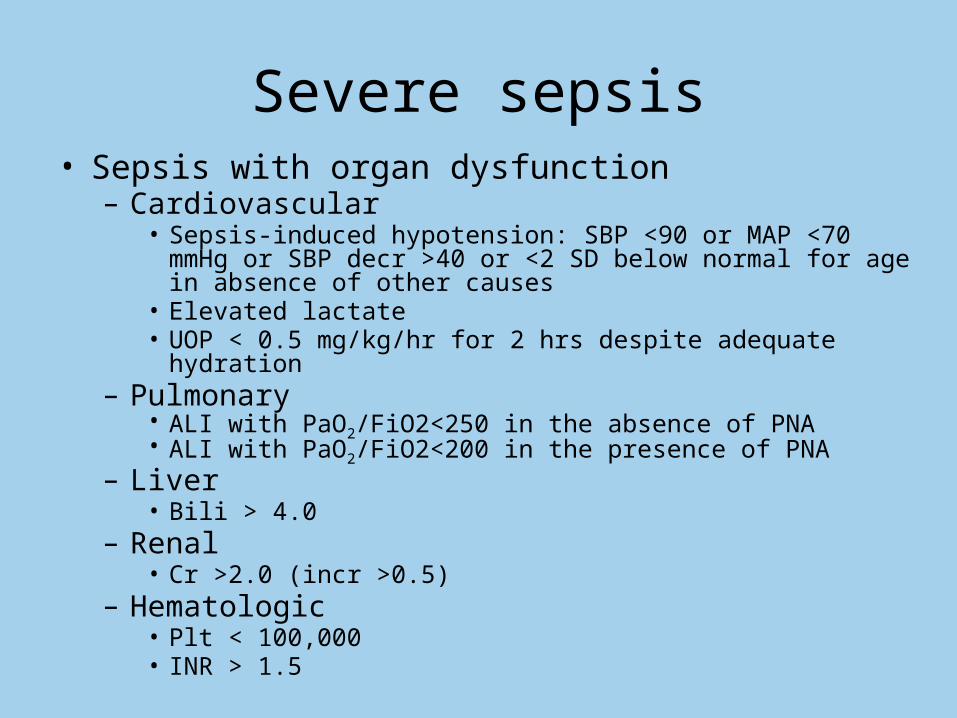
Severe sepsis• Sepsis with organ dysfunction– Cardiovascular
• Sepsis-induced hypotension: SBP <90 or MAP <70 mmHg or SBP decr >40 or <2 SD below normal for age in absence of other causes
• Elevated lactate• UOP < 0.5 mg/kg/hr for 2 hrs despite adequate hydration
– Pulmonary• ALI with PaO2/FiO2<250 in the absence of PNA• ALI with PaO2/FiO2<200 in the presence of PNA
– Liver• Bili > 4.0
– Renal• Cr >2.0 (incr >0.5)
– Hematologic• Plt < 100,000• INR > 1.5
Septic shock
• Sepsis + hypotension despite “adequate” fluid resuscitation
Sick or not sick?
• Severe sepsis/septic shock mortality ~18-46% • ~10% of all pts in ICU• Most common cause of death in ICU
Case 1• 38 yo F just finished running marathon, goes to medical
tent because of lightheadedness– VS: 37.4, 130, 88/60, 24, 97% RA– Labs not available
• How many SIRS criteria?2
• Does this patient have sepsis?No
Case 2• 65 yo M presents with productive cough, fever, chills.– VS: 38.1, 92, 120/80, 16, 90% RA– Labs: WBC 3.8, Hb 9, plt 180
RFP WNL, HFP WNL, lactate WNL, coags WNL
• How many SIRS criteria?3
• Does this patient have sepsis?Yes
• Would it make a difference in diagnosis of sepsis if had CXR which showed LLL infiltrate?
No• Does this patient have severe sepsis?
No• Does this patient have septic shock?
No
Case 3• 89 yo F sent from NH with confusion, diarrhea– VS: 35.8, 98, 22, 85/45, 97% RA– Labs: WBC 10,000 with 12% bands, Hb 10, plt 160
bicarb 15, Cr 1.3 (baseline 0.7), lactate 4.1ABG: 7.29/25/89
• How many SIRS criteria?4
• Does this patient have sepsis?Yes
• Does this patient have severe sepsis?Yes
• Does this patient have septic shock? Possibly- will need to see how her BP responds to IVFs
SIRS Criteria• Temperature
> 38.0 or < 36.0• HR
> 90• Respiratory status
RR >20 or PaCO2 <32• WBC
>12,000 or <4,000 or >10% bands
**** BP IS NOT A SIRS CRITERIA ****
Outline/Objectives
• Identification of sepsis• Work up of sepsis• Triaging sepsis• Treatment of sepsis
History?
• Source• Severity
History?• Source– Lung
• Cough, sore throat, rhinorrhea• Sick contacts
– Blood• Fatigue, lines in place, IVDU
– Urine• Dysuria, hematuria, flank pain
– GI• Diarrhea, nausea, vomiting, abd pain• Recent abx or hospitalization, recent travel, sick contacts
– Other: Skin/soft tissue, bone/joint, ascites, CNS, heart• Skin changes, rash, joint pain, HA, confusion, back pain, neck
stiffness, photophobia
History?
• Severity– Fevers/chills, appetite, po intake– Progression– Onset
Labs?
• Source• Severity
Labs?• Source– Lung
• sputum cx– Blood
• Bcx: 2 peripheral + 1 from each line the pt has (central lines, HD lines, art lines, etc)
– Urine• UA + Ucx
– GI• C diff, fecal leuks, stool cx
– Other• culture of any drainage, diagnostic paracentesis, LP, ESR, CRP
**** ALWAYS CULTURE BEFORE STARTING ANTIBIOTICS ****
Labs?
• Severity– Does patient have evidence of any organ damage?
Need to evaluate organ systems to determine• CBC• RFP• HFP• Lactate• Coagulation screen• ABG• ScvO2
Studies?
• Source• Severity
Studies?
• Source/Severity– Lung• CXR, CT chest
– Blood• TTE
– Urine/GI• CT abd
– Other• CT head, MRI (for OM)
Outline/Objectives
• Identification of sepsis• Work up of sepsis• Triaging sepsis• Treatment of sepsis
When to transfer to MICU
• Sepsis– Usually can treat on the floor
• Severe sepsis– Floor or MICU depending on how severe the organ
dysfunction is• Severe lactic acidosis MICU• Respiratory distress requiring intubation MICU
• Septic shock– MICU
Outline/Objectives
• Identification of sepsis• Work up of sepsis• Triaging sepsis• Treatment of sepsis
Treatment
• Early Goal Directed Therapy– Rivers et al 2001
• Surviving Sepsis Campaign– International guidelines last came out in 2012– Recently updated in April 2015 to incorporate new
studies on sepsis
Early Goal Directed Therapy• Single center, 263 enrolled patients• Purpose: evaluate efficacy of 6 hrs of EGDT prior
to admission to ICU• Results: – 30.5% mortality in EGDT group compared to 46.5%
mortality in standard therapy (p=0.009)– During interval from 7-72 hrs, pts in EGDT had higher
mean ScvO2, lower lactate, higher pH than standard therapy
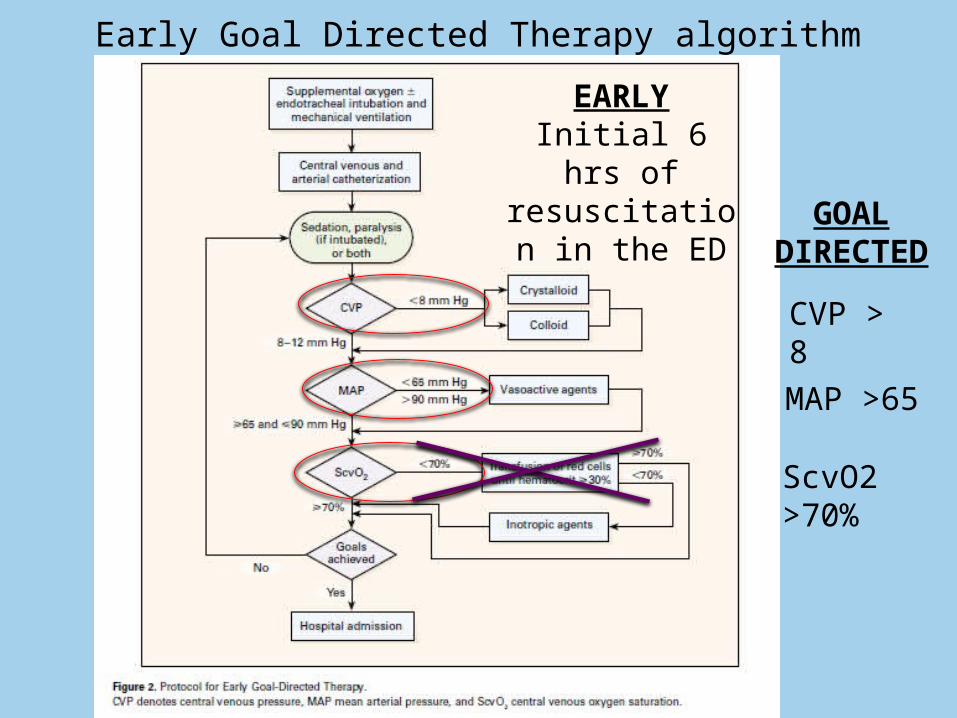
• We typically follow a version of the algorithm from this trial in the ICU
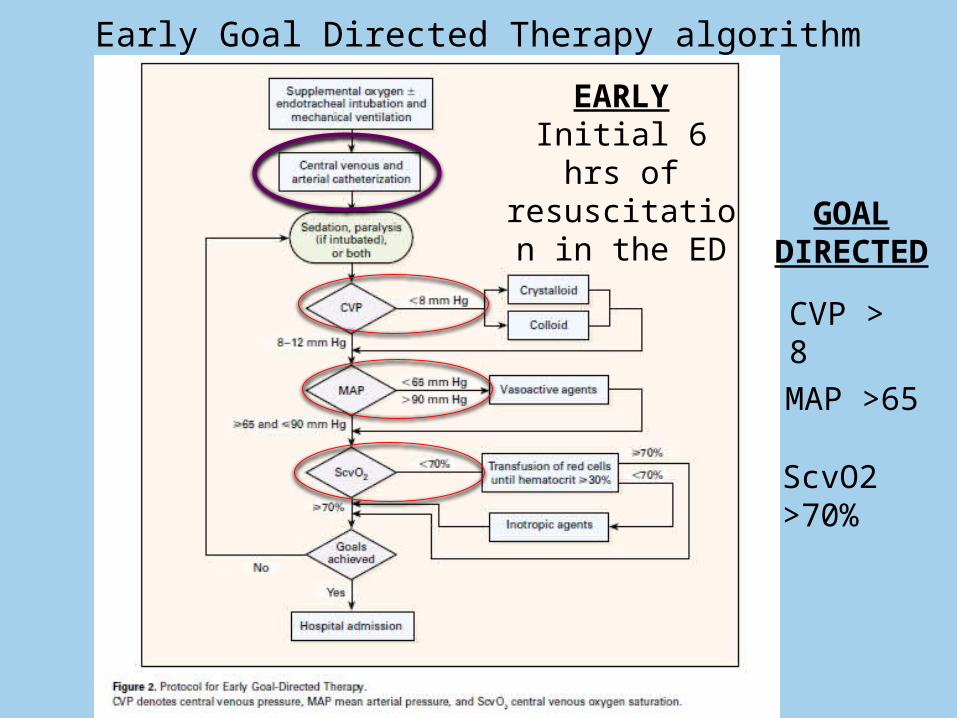
CVP > 8
MAP >65
ScvO2 >70%
Early Goal Directed Therapy algorithmEARLY
Initial 6 hrs of resuscitation in
the ED GOAL DIRECTED
CVP??
• Approximation of R atrial pressure• Gives an idea of volume status• Measured by the nurses off of a central line
(terminates in the SVC… near the R atrium)• Mechanical ventilation increases CVP (because
of PEEP)
MAP??
• Mean arterial pressure• Approximates average blood pressure
throughout the cardiac cycle• MAP = 2/3 DBP + 1/3 SBP• Automatically calculated in our EMR and on
BP monitor
ScvO2??
• Central venous O2 saturation• = the oxygen saturation of blood that is
returning to the R atrium (lowest O2sat in the body before going to lungs)
• Drawn from a central line• Indication of tissue hypoxia (more tissue
hypoxia more oxygen extraction at tissue level decreased O2 saturation of blood returning to heart)
CVP > 8
MAP >65
ScvO2 >70%
Early Goal Directed Therapy algorithmEARLY
Initial 6 hrs of resuscitation in
the ED GOAL DIRECTED
ProCESS Trial• Published in NEJM May 1, 2014• Multicenter, 1341 patients enrolled• Purpose: to determine if EGDT is generalizable and if all
aspects of protocol are necessary• Results:
– At 60 days: no sig difference between EGDT and either protocol-based standard therapy group or usual-care group
– No sig difference in 90 day mortality, 1 yr mortality, or need for organ support
• Conclusion: “protocol-based resuscitation of patients in whom septic shock was diagnosed in the emergency department did not improve outcomes.”
ARISE Trial, ProMISE Trial
• Published in NEJM in Oct 2014 and April 2015• Also multicenter, large trials (ARISE: Australia,
New Zealand, ProMISE: England)• General conclusion from both: Strict EGDT
protocol did not improve outcome
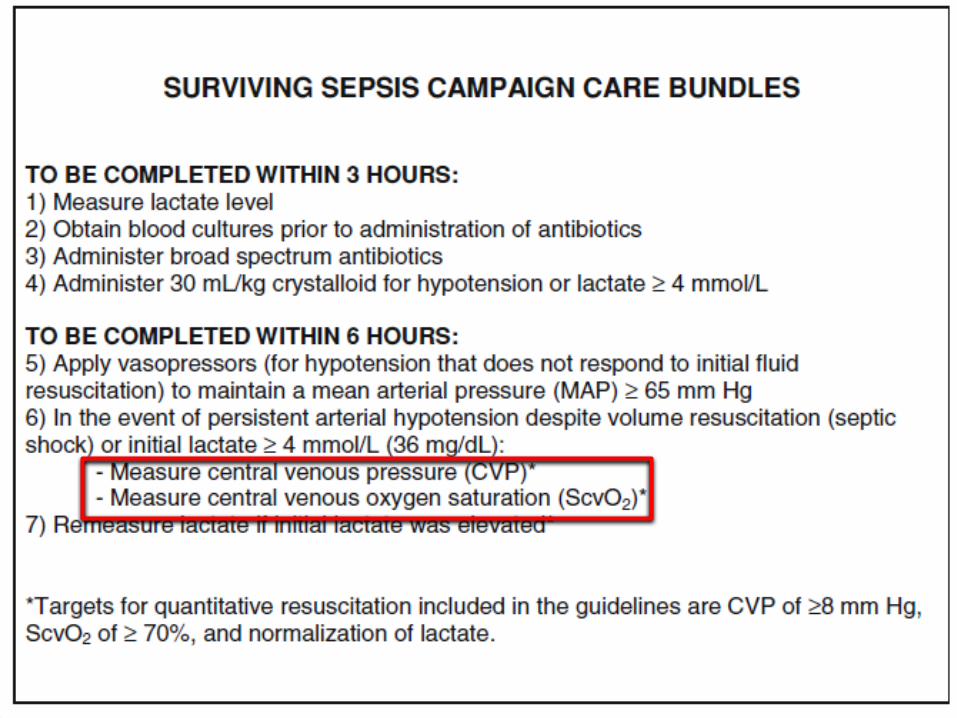
Surviving Sepsis Campaign
• Takes several studies into account when developing international guidelines for treating sepsis
• Splits care in to 2 “bundles”: one to be completed within 3 hrs and the other within 6– Note: all groups in ProCESS trial essentially
followed the 3 hr bundle– Updated in April 2015 to take into account the
3 new trials evaluating EGDT
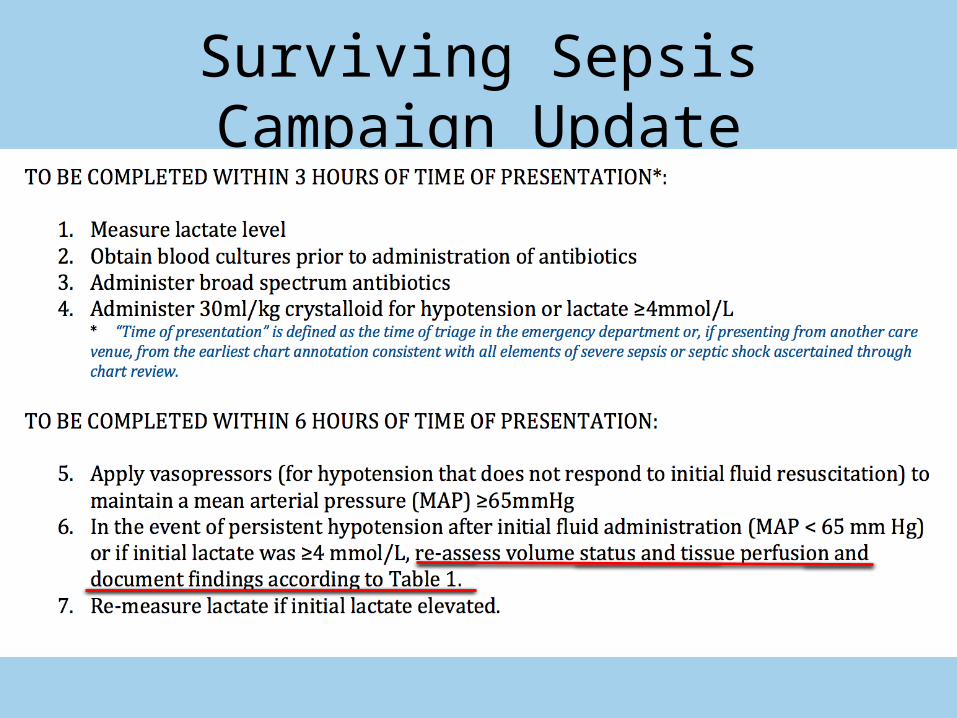
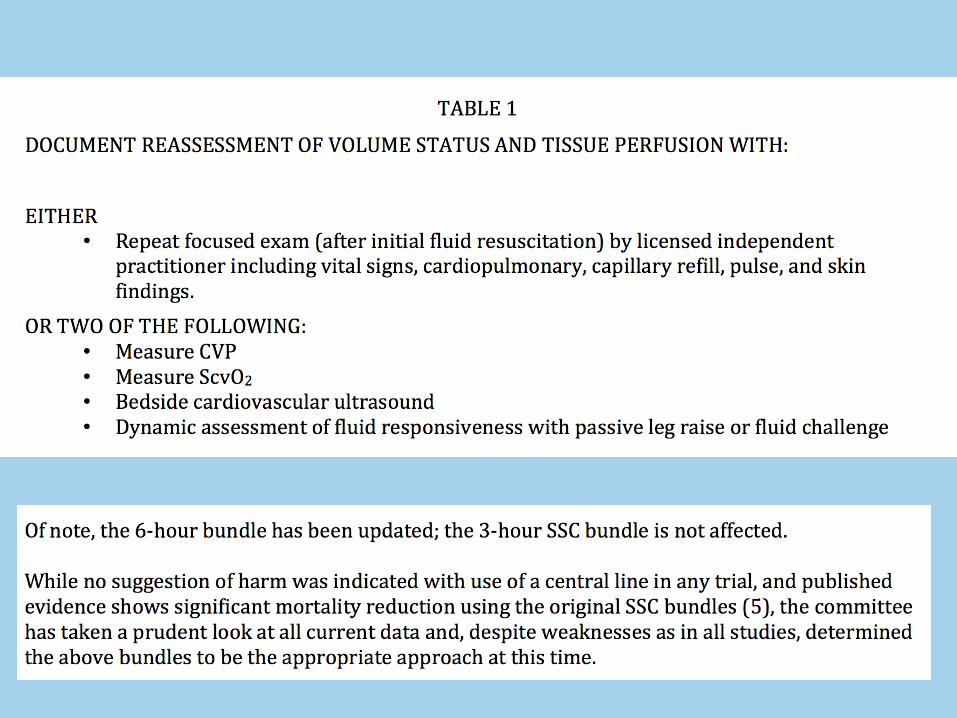
Surviving Sepsis Campaign Update
Initial Treatment• Antibiotics– If source is known, cater abx to the source– If source is unknown, use broad spectrum• Vanc/zosyn
• Fluids• Fluids• Fluids• Remove potential source (line holiday) within 12 hrs• Obtain labs to help determine severity (lactate)
*** WHEN GIVING FLUIDS, KEEP IN MIND PT’S RENAL FUNCTION AND EF ****
Hypotension
• If not responsive to “adequate” hydration, will need pressors in the MICU– “Adequate”: 30 cc/kg (in 70 kg person, ~ 2 L)
Pressors
• Need central line– Aggressive fluid resuscitation– Administration of pressors– Measure CVP
• Need arterial line– More accurate BP monitoring– Know second-to-second changes in BP
Pressors
• Norepinephrine (Levophed) is 1st pressor used in sepsis
• Others you can add on if necessary:– Vasopressin– Epinephrine– Phenylephrine– Dopamine
Goals for treatment
• MAP >65• CVP 8-12 (not intubated), 12-15 (intubated)• ScvO2 >70%• Normal lactate• UOP > 0.5 ml/kg/hr
Tools for treatment• Fluids• Antibiotics• Pressors• Blood products- if Hb <7, plt <10,000• (Albumin)• Steroids- only if fluids/pressors not adequate• Mechanical ventilation• Central lines/arterial lines• Nutrition- in first 48 hrs• DVT/stress ulcer ppx
Summary
• SIRS criteria: T> 38.0 or < 36.0, HR> 90, RR >20 or PaCO2 <32, WBC >12,000 or <4,000 or >10% bands
• Sepsis workup should focus on identifying source and severity
• Initial treatment: cx, abx, fluids• Patients with septic shock and some with
severe sepsis require MICU


















