INTERACTION EFFECTS OF THE STARTLE RESPONSE AND HORMONAL …
74
INTERACTION EFFECTS OF THE STARTLE RESPONSE AND HORMONAL CHANGES ON KNEE STIFFNESS by Athena DeAngelis A thesis submitted to the Faculty of the University of Delaware in partial fulfillment of the requirements for the degree of Master of Science in Exercise Science Fall 2012 © 2012 Athena DeAngelis All Rights Reserved
Transcript of INTERACTION EFFECTS OF THE STARTLE RESPONSE AND HORMONAL …

INTERACTION EFFECTS OF THE STARTLE RESPONSE AND
HORMONAL CHANGES ON KNEE STIFFNESS
by
Athena DeAngelis
A thesis submitted to the Faculty of the University of Delaware in partial fulfillment of the requirements for the degree of Master of Science in Exercise Science
Fall 2012
© 2012 Athena DeAngelis All Rights Reserved

INTERACTION EFFECTS OF THE STARTLE RESPONSE AND
HORMONAL CHANGES ON KNEE STIFFNESS
by
Athena DeAngelis
Approved: __________________________________________________ Charles Buz Swanik, Ph.D. Professor in charge of thesis on behalf of Advisory Committee Approved: __________________________________________________ William B. Farquhar, Ph.D. Chair of the Department of Kinesiology and Applied Physiology Approved: __________________________________________________ Kathleen S. Matt, Ph.D. Dean of the College of Health Sciences Approved: __________________________________________________ Charles G. Riordan, Ph.D. Vice Provost for Graduate and Professional Education

iii
ACKNOWLEDGEMENTS
I would like to say a special thank-you to several people who have been a great
support system and have provided me with everything I needed to finish this project.
First and foremost I want to thank all my lab-mates and friends that have helped as
volunteer subjects and assisting in all aspects of performing testing. These special
people include Kathy Liu, Craig Oates, Jen Halterman, Chris Clyde, Peter Braun, and
Dan Tocci. I really want to acknowledge Alan Needle for providing all his expertise,
advice, time and mentorship over the past two years. Finally, I could not do this
without awesome friendships and support that I will treasure forever with Christina
Shields, Rob Hulbert and Matt Astolfi.
The University of Delaware provided me the opportunity to work along side
some of the best researchers including my committee members: Dr. Kaminski, Dr.
Knight and Dr. Royer. I would also like to thank my advisor and chair, Dr. Swanik,
for providing me with guidance throughout this entire thesis process and giving me his
expertise in joint stiffness and neurocognitive function to assist me in completing this
degree.
Finally, I would be nothing without the love and support my family
continuously gives me everyday of my life. Even though they are not experts with my
project, they were always a phone-call away to talk to and always support everything I
was doing in order to earn my degree. Without them, I would not be the person I am
today.

iv
TABLE OF CONTENTS LIST OF TABLES ........................................................................................................ vi LIST OF FIGURES ...................................................................................................... vii ABSTRACT ................................................................................................................ viii Chapter
1 INTRODUCTION ........................................................................................ 1
2 METHODS ................................................................................................... 5
2.1 Experimental Design .............................................................................. 5 2.2 Participants ............................................................................................. 5 2.3 Instrumentation ....................................................................................... 6 2.3.1 Stiffness and Proprioception Device ............................................. 6 2.3.2 Electromyography ......................................................................... 7 2.4 Procedures .............................................................................................. 8 2.5 Data/Statistical Analysis ......................................................................... 9
3 RESULTS ................................................................................................... 11 3.1 Demographics & Maximum Voluntary Isometric Contraction ............ 11 3.2 Startle Effects on Stiffness and EMG Variables .................................. 11 3.2.1 Stiffness & Startle ........................................................................ 11 3.2.2 EMG & Startle ............................................................................. 11 3.3 Startle Effects on Group Differences ................................................... 13
4 DISCUSSION ............................................................................................. 14 4.1 Stiffness Regulation and the Acoustic Startle ...................................... 14 4.2 Group Effects ........................................................................................ 19 4.3 Limitations ............................................................................................ 21 4.4 Conclusion ............................................................................................ 22
5 LEGEND .................................................................................................... 23
6 LITERATURE REVIEW ........................................................................... 40
v
7 REFERENCES ........................................................................................... 52 Appendix
A: STIFFNESS AND PROPRIOCEPTION DEVICE ........................................... 58 B: PAR-Q FORM ................................................................................................... 61 C: DEMOGRAPHIC AND HEALTH HISTORY QUESTIONNAIRE ................ 62 D: QUADRICEPS & HAMSTRING STRETCHING TECHNIQUE ................... 64 E: IRB APPROVAL LETTER ............................................................................... 65

vi
LIST OF TABLES
Table 1: Demographics ............................................................................................. 23 Table 2: Short-range (4°) Startle Normalized Stiffness ............................................ 24 Table 3: Total (40°) Startle Normalized Stiffness .................................................... 25 Table 4: Electromechanical Delay (EMD) Values ................................................... 26 Table 5: Peak EMG Values for Startle Passive-Reactive Trials ............................... 27 Table 6: Time to Peak (TTP) Values; Startle Trials ................................................. 29 Table 7: Time to Peak (TTP) Obicularis-Oculi; Startle Trials ................................. 31 Table 8: Onset Values for Passive-Reactive (Startle) Trials .................................... 32 Table 9: Pre-Perturbation (150 prior-0ms) Area Values; Startle Trials ................... 34 Table 10: Post-Perturbation (0-250ms) Area Values; Startle Trials ........................... 36 Table 11: Post-Post Perturbation (250-600ms) Area Values; Startle Trials ............... 38

vii
LIST OF FIGURES
Figure 1: Five Perturbation Techniques and Instructions ......................................... 10
Figure 2: Neuronal Circuit ........................................................................................ 50 Figure A.1: Subject Positioning on the SPAD for testing protocols ............................ 60

viii
ABSTRACT
Context: Growing evidence suggests the nervous system has a significant role in
the high rate of non-contact anterior cruciate ligament injuries. Females are the
most susceptible, but evidence for a hormonal role is conflicting. The startle reflex
is universal across animals and stiffens limb muscles after sudden, unanticipated
events. No studies have investigated how hormonal changes during the menstrual
cycle may interact within the nervous system to alter the startle response and knee
stiffness regulation among males and females. Objective: To assess if reactive
knee joint stiffening strategies are affected differently in males and females during
an acoustic startle. Design: Post-test only with repeated measures. Setting:
University laboratory Patients or Other Participants: 18 males (21.3±2.0 yrs,
82.8±15.8 kg, 179.5±6.9 cm) and 18 females (20.9±2.0 yrs, 61.8±7.6 kg,
164.4±6.8 cm) with no previous knee injury participated in this study. All females
were tested at 2 points in the menstrual cycle to form 3 groups: Males (M),
Female-Follicular (FF), and Female-Ovulation (FO). Interventions: Subjects were
seated on a custom stiffness device that generated a rapid 40° flexion perturbation
to the knee (30° to 70° flexion arc). Subjects remained relaxed prior to the
perturbation, and were instructed to react with maximal extension force as quickly
as possible when the perturbation was sensed. A total of 6 trials were performed,
with an acoustic startle (50ms, 1000Hz, 100dB) applied 100ms prior to the

ix
perturbation on 3 randomly selected trials. Main Outcome Measures: Normalized
knee stiffness (Δtorque/Δposition, Nm/°/kg) was calculated at the short-range (0-
4°) and for the total perturbation (0-40°). The average of the control (CON) and
startle trial (ST) were used for analysis. Repeated-measures analyses of variance
comparing gender (M, FF, FO) and startle condition (CON, ST) were used for
analysis at both short-range and total range. Results: The startle significantly
increased short-range stiffness (F=4.24, p=0.04), and decreased total stiffness
(F=11.25, p<0.001). Pairwise comparisons revealed that at short-range, ST
displayed a significantly greater stiffness of 0.047±0.002Nm/°/kg, (p=0.003)
compared to the CON (0.043±0.003Nm/°/kg). However, for total stiffness, the
startle response caused significantly less total stiffness (0.028±0.002Nm/°/kg) than
the CON (0.037±0.002Nm/°/kg, p=0.004) condition. No significant gender or
menstrual cycle phase differences were observed for stiffness values.
Conclusions: This is the first study to indicate that the startle response can
significantly disrupt the normal knee stiffness regulation strategies that are
required to maintain joint stability, and this effect may occur equally in males and
females. Gender and menstrual cycle phase do not appear to affect knee stiffness
or negatively interact with the startle response. Further studies should explore the
potential role of startle responses in accidents and unintentional non-contact
injuries.
Key Words: anterior cruciate ligament, menstrual cycle, stiffness, acoustic startle
1
Chapter 1
INTRODUCTION
Knee injuries are commonly experienced among the physically active
population, with anterior cruciate ligament (ACL) sprains affecting over 250,000
people per year. (Adachi et al., 2008; J. T. Blackburn et al., 2009; Griffin et al., 2000)
Non-contact ACL (NC-ACL) injuries account for over 70% of all ruptures and likely
result from sudden errors in coordination during abrupt deceleration maneuvers like
landing, or cutting.(Fleming et al., 2003; Kirkendall & Garrett, 2000; Olsen et al.,
2004) Females suffer this injury 2-8 times more often than males, and most
researchers believe intrinsic factors such as knee valgus collapse, anterior tibial sheer
and knee laxity are responsible for the higher incidence. However, these prior
observations may only reflect underlying disruptions in neuromuscular control that
ultimately lead to pathological joint kinematics. (Boden et al., 2000; C.Swanik et al.,
2004; C.Swanik et al., 1999) Moreover, theories for the potential neurophysiological
source of these coordination errors have been limited, especially in males. It is
plausible that two common neurological influences, the startle response and menstrual
cycle, interact to heighten ones risk for NC-ACL injury. (Adachi et al., 2008)
Precise muscle activation strategies can help stress-shield ligamentous
structures from excessive loading by regulating joint stiffness during sport-specific
maneuvers.(Lephart et al., 1992) Both quadriceps and hamstring musculature provide
this capacity of dynamic stabilization at the knee, however, sudden unanticipated
events may interrupt the feed-forward and feedback motor control necessary for

2
optimal temporal/spatial muscle recruitment levels. (Rozzi et al., 1999; C.Swanik et
al., 2004; C.Swanik et al., 1999) Recently, greater attention has been focused on
attributes of the central nervous system (CNS) that may be associated with
unintentional musculoskeletal injuries and the promise of reducing injury prone
behaviors.(C.Swanik et al., 2007; Baumeister et al., 2008, Ribot-Ciscar et al., 2009)
It is well documented that unanticipated events can provoke a universal startle
response within the CNS, which results in a brief, but widespread change in
neuromuscular activity. (Davis, 1984; Koch, 1999) When an unexpected startle
response is provoked, neuromuscular changes to preparatory (feed-forward) and
reactive (feedback) muscle contractions in the extremities can be observed, potentially
altering the stiffness regulation necessary for energy absorption and dynamic joint
stabilization. (LaCroix, 1981; Freeman, 1966; Davis, 1984; Koch, 1999) The most
common startle research model uses an unexpected acoustic stimulus, which during
ordinary physical activities and real-world settings may be synonymous with any
sudden extraneous events, noises, or interpersonal communications. (Leumann et al.,
2001) While much of the previous research has focused on NC-ACL injury
mechanisms in women, the startle response may help explain why males too suffer a
loss of coordination and high incidence of this unintentional musculoskeletal injury.
Some research suggests that females may have different reactions to
unanticipated startle events than males. (Hausmann et al., 2000; McCormick &
Teillon, 2001) In response to an auditory stimulus, females have shown faster
responses and higher lower-limb muscle activation. (Kofler et al., 2001) The

3
differences in female startle response have been suggested to result from hormonal
changes. (Braff et al., 2001; Kofler et al., 2001)
The female menstrual cycle and hormone concentration level change is one
remarkable difference between males and females and may be linked to variations in
female neuromuscular control and dynamic stability. (Adachi et al., 2008) Previous
studies tend to focus on ACL characteristics such as laxity and collagen formation;
however, Zazuluk (2006) reported that these results are inconclusive. There is limited
research linking the idea of hormonal alterations to neuromuscular control and joint
stability. Although some debate exists, ACL injuries appear more prevalent during the
ovulation stage of the menstrual cycle, when estrogen is at its peak. (Deie et al., 2002;
Eiling et al., 2007; Park et al., 2009) This hormonal change, along with dysmenorrhea
seen around day 14 of the cycle, may contribute to alterations in sensorimotor
characteristics and athletic performance leading to increased risk of injury. (Adachi et
al., 2008; Eiling et al., 2007) Estrogen levels also cause increased synthesis of the
neurotransmitter dopamine, creating a more responsive effect to the acoustic
startle.(Braff et al., 2001; Jovanovic, 2004) Since estrogen peaks during ovulation, this
would suggest that with an increase of dopamine the reflex would be most affected
during this phase of the cycle. (Jovanovic, 2004) Therefore, changes in hormonal
levels during the menstrual cycle may contribute to differences in both the startle
response and joint stiffness regulations, but these interactions have not been observed.
The purpose of this study was to determine if gender and menstrual cycle
differences occur with an acoustic startle, and whether these alterations influence the

4
quadriceps and hamstring muscle activation strategies responsible for knee joint
stiffness regulation. By combining measures of muscle stiffness and acoustic startle
trials, more information may be found on this potential source for heightened risk of
non-contact ACL injuries. In this study we tested the hypothesis that (1) there is
altered muscle activation and stiffness occurring when the acoustic startle trials occur
compared to the control conditions, (2) males react to the acoustic startle with quicker
muscle activation leading to an increase in stiffness compared to females and (3) the
female menstrual cycle interacts with the startle response leading to a change in
muscle activation and joint stiffness.

5
Chapter 2
METHODS
2.1 Experimental Design
This study utilized a post-test only design with repeated measures. The
independent variables are gender (male and female), menstrual cycle phase (Follicular
(FF), and Ovulation (FO)) and condition (no startle and acoustic startle). The
dependent variables are measurements of short-range and total knee stiffness and
muscle activity (timing and amplitude).
2.2 Participants Eighteen male and eighteen female (tested twice) healthy volunteer
participants within the 18-25 years age range were recruited from the University of
Delaware population. The number of participants is determined through an a priori
power analysis using G*Power v3.1.2 (Heinrich-Heine-Universitat, Dusseldorf) with
parameters set at α = .05, 1- β = 0.80. Prior to testing, participants were provided
university-approved informed consent (UD IRB 231022-1) as well as a Physical
Activity Readiness Questionnaire (PAR-Q) and Demographic and Health History to
determine participation eligibility. If the participant answered, “Yes” to questions
pertaining to pains in the heart or chest, faintness or dizziness, bone or joint problems,
or low back problems; he/she were not included in the study. Participants were tested
on their dominant leg. This is defined by which leg the subject would use to single-leg
jump for distance. (Croce 2004, Russell 2007) Exclusion criteria for all participants
includes: (1) any fractures to the test leg within the previous year, (2) history of injury

6
to the leg within the previous 6 months (3) other knee injuries requiring surgery, (4)
any current bone, muscular, or joint injuries to the hip, knee, and ankle, (5) any
cardiovascular, metabolic or neurological that limits moderate physical activity, (6)
any hearing impairment or complications, and (7) any females taking oral
contraceptive medications or having irregular menstrual cycles.
2.3 Instrumentation 2.3.1 Stiffness and Proprioception Device (SPAD)
Stiffness testing was performed using a custom-built stiffness and
proprioception assessment device (SPAD). The SPAD is a device capable of
providing a perturbation to the knee at a controlled acceleration, deceleration , velocity
and range of motion. The SPAD is a brushless Danaher/Kollmorgen servomotor (B-
404-B-B4) that is fitted into a gearbox (UT018-050, 50:1) and connected to an
amplifier/controller (Copley Xenus driver XSL-12-36-R). The mated servomotor and
gearbox are mounted in a cast aluminum pedestal that is offset from the subject’s
chair. An adaptor arm and torque reaction sensor (Model # T5400, Futek Advanced
Sensor Technology, Irvine, CA) with a 565 N capacity and 1.43 X 105 ft-lb/rad
torsional stiffness is coupled to the gearbox. The signal conditioner digitally displays
torque values and also sends an analog torque signal through an A-D board (NI DAQ
6009, National Instruments, Austin, TX) that can be recorded and displayed in
LabVIEW software. For safety purposes, internal motor settings cannot exceed preset
speeds and there are three emergency stop switches that can disable the motor during

7
testing. The SPAD device is operated using a personal computer with a customized
LabVIEW virtual instrument and motor control software program.
2.3.2 Electromyography (EMG)
Surface electromyography (EMG) were collected from the vastus medialis,
vastus lateralis, medial hamstrings, and lateral hamstrings to determine stiffness
regulation strategies by analyzing the amplitude and timing of the muscular
contractions. There was also one electrooculography (EOG) self-adhesive Ag/AgCl
snap dual electrode (Noraxon USA Inc, Scottsdale, AZ) placed on obicularis oculi to
record EOG activity of the eye blinking and confirm a startle response. Self-adhesive
Ag/AgCl bipolar surface electrodes (Phillips Medical Systems, Andover, MA) were
used to collect EMG data of the leg musculature, and an EMG unit (Bortec AMT-8,
Bortec Biomedical, Calgary, Alberta, Canada) was used to record EMG with a real-
time visual display on the monitor. Electrode placement was identified by bony
landmarks and through palpation of the mid-belly of the contractile component of the
muscle during an isometric contraction. The reference electrode was placed on the
patella. Except for the eye muscle, each electrode is 10mm in diameter and was
placed 25mm apart. Electrode placement site was shaven, abraded, and cleansed with
an alcohol swab (70% ethanol solution) to decrease the impedance from the skin. The
EMG signal was converted from analog to digital data (NI DAQ 6009, National
Instruments, Austin, TX), and then passed to a computer where the raw EMG data was
sampled at 2,400 Hz and further analyzed with LABVIEW software (National
Instruments, Austin, TX). The EMG signal was bandpass filtered at 20-400Hz,

8
rectified, and low-pass filtered at 5Hz to create a linear envelope. EMG is normalized
to maximum voluntary isometric contractions (MVICs) for the muscles of the
quadriceps and hamstrings. All data collected with EMG equipment is used to
determine the timing, sequence, amplitude (area & peak), and pattern of the
quadriceps/hamstrings muscle groups during preparatory and reactive phases of the
stiffness testing.
2.4 Procedures
Participants were asked to report to the Human Performance Lab for a 90-
minute testing procedure. Females were asked to participate twice in the study: once
during the follicular phase and once during ovulation phase of the menstrual cycle.
After providing consent, completing all questionnaires, and satisfying the inclusion
criteria, participants then rode a stationary bike for a 5-minute warm-up followed by 5
minutes of stretching of their quadriceps and hamstrings as instructed with a handout
and verbal direction.
The participant was positioned on the SPAD with the dominant knee flexed to
30 degrees and the trunk positioned at 90 degrees of flexion. The axis of rotation of
the adapter arm attached to the servomotor was in line with the lateral knee joint line.
In order to ensure that all torque responses result from movement at the knee and not
the lower leg, a vacuum splint was secured to the lower leg below the knee to maintain
the ankle in a neutral position. A thigh pad was also used for stability so that
movement occurred only at the knee joint. All electrodes for EMG activity recordings
were attached to the same side determined as the dominant leg. Three maximum

9
voluntary isometric contractions (MVIC) were collected for the quadriceps and
hamstrings to determine an overall average and 30% of their maximum contraction.
The parameters of the perturbations for each testing condition remained the
same for each perturbation with a quick acceleration of 1000 deg/sec2 to a velocity of
100o/sec and a flexion arc of 40o going from knee extension to flexion. The various
testing conditions of reactive stiffening included both control trials and acoustic startle
trials. The five perturbation techniques were passive-nonreactive, active-nonreactive,
passive reactive, active reactive and active deactivate. (Figure 1) For the acoustic
startle condition, a high-pitched 100 dB tone, lasting 50ms at a frequency of 1000 Hz
sounded 100ms before perturbation. (Braff et al., 2001) Throughout all conditions, the
knee perturbation was randomly applied within a 10-second time span. Also, the
subjects were wearing headphones for all conditions to mute potential noisy
distractions. Resistance to the perturbation is detected by the torque sensor and
recorded by a computer. Joint stiffness is calculated as the Δ force (Nm) / Δ
displacement (degrees) / body mass (kg). There were six trials of each, and during the
passive reactive trials the acoustic startle was applied three times. We calculated
electromechanical delay (EMD) as the difference of when torque and EMG went
above 5 percent of peak.
2.5 Data/Statistical Analysis
A custom-written software program using LabVIEW was used to analyze
position and torque data, calculate stiffness and analyze all EMG signals. Stiffness

10
values were calculated from the position data at 3° and 40° of the flexion
perturbations. The EMG was averaged over the six trials for each of the five
perturbations. EMG was analyzed from a window of 150ms prior to perturbation and
600ms after the start of perturbation. The normalized stiffness values were obtained
by dividing each volunteer’s stiffness values by their body mass(kg). The significance
for all data is set a priori at p<.05. A repeated-measures ANOVA with one between-
subject factor (group, 3 levels), and one within-subjects factor (condition, 5 levels)
was used primarily to determine the differences in gender (cycle) and knee stiffness
and when the startle is applied. To determine mean statistical differences, pairwise
comparisons were used to assess changes in stiffness while the startle was applied
between males and females, as well as changes in muscle activation strategies post
hoc. This was also used to compare females during the two periods of their menstrual
cycle.
Figure 1: Five Perturbation Techniques and Instructions
Condition Instructions Passive Stiffness (PS) “Remain completely relaxed throughout the entire perturbation”
Active Stiffness (AS) “Push out to [30% MVIC] prior to the move. When you feel the perturbation, hold that amount of contraction without pushing more or less.”
Reactive Stiffness (RS) “Push out to [30% MVIC] prior to the move. When you feel the perturbation, resist it as hard and as fast as possible as if you are stopping your knee from bending.
Passive Reactive Stiffness (PRS)
“Remain completely relaxed prior to move. When you feel the perturbation, resist is as hard and as fast as possible as if you are stopping your knee from bending”
Deactivating Stiffness (DS) “Push out to [30% MVIC] prior to the move. When you feel the perturbation, turn off all your muscles and relax as quickly as possible.”

11
Chapter 3
RESULTS
3.1 Demographics and Maximum Voluntary Isometric Contractions
Demographic data for age, height, mass, and peak MVIC torque are displayed
in Table 1. Females and males ages ranged from 18-25 and were not significantly
different (p=.563). Males displayed significantly greater height, mass, and leg length
compared to female participants (p<.001). Peak torques during MVIC for quadriceps
and hamstrings MVICs also were significantly greater in male participants (p<.05).
3.2 Startle Effects on Stiffness and EMG Variables 3.2.1 Stiffness & Startle Results for normalized short-range (0 to 4°) and total (0 to 40°) stiffness from
PR trials are displayed in Tables 2 & 3, respectively. The startle was observed to
significantly affect both short-range (p=0.037) and total (p<0.001) stiffness. For short-
range stiffness, both the first (FST) startle trial (p=0.003) and the average of the startle
trials (AST) (p=0.005) displayed significantly greater stiffness than control (CON)
trials. However, for total stiffness, FST trials demonstrated significantly less total
stiffness than both CON (p=0.004) and AST (p<0.001) trials.
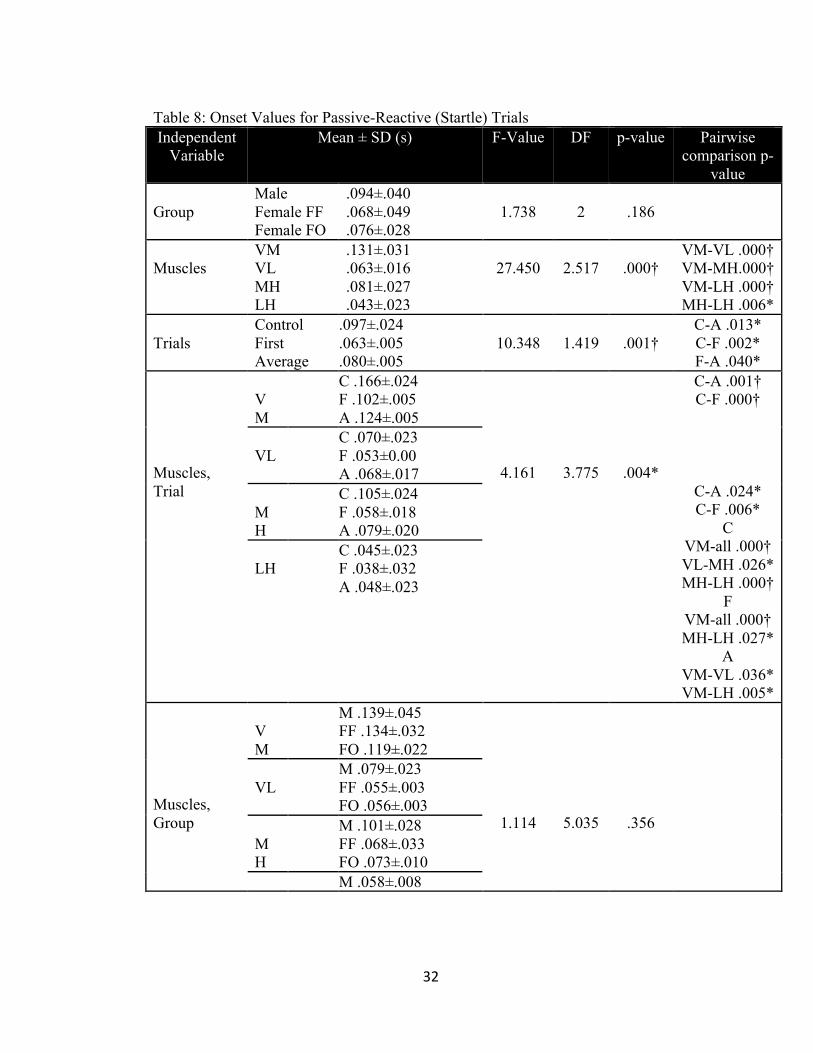
3.2.2 EMG & Startle EMG variables used for analysis during PR trials include peak EMG (table 5),
TTP for leg musculature (table 6), TTP for obicularis oculi (table 7), onset values
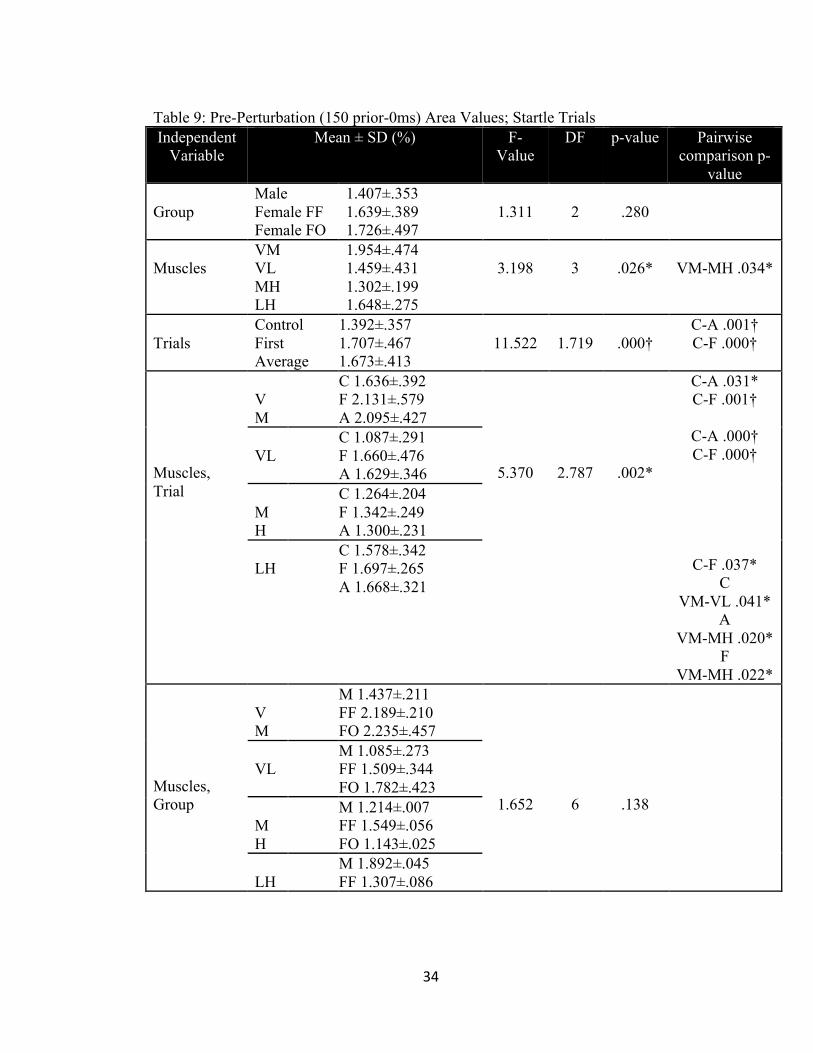
(table 8), areas for EMG activation 250 prior-to (table 9), 250ms following (table 10)
and 250-500ms following (table 11) the perturbation.

12
A significant muscle by condition interaction effect was observed for all
variables (p<.05), with the exception of EMG area 250-500ms following the
perturbation, which was approaching significance (p=.055). The VM displayed
significantly lower peak EMG during FST trials compared to CON and AST trials
(p=0.040 and p=0.017). VM and VL revealed significantly shorter TTP for FST and
AST trials (p<.05) than CON and MH displayed significantly shorter TTP in FST in
relation to CON (p=.046). The VM and MH demonstrated significantly shorter onset
for both FST and AST than CON (p<.05). VM and VL showed a significant increase
in pre-perturbation area with FST and AST compared to CON (p<.05) and LH
presented significant increase in FST trials than CON (p=.037). Post-perturbation area
had a significant decrease for VL in AST trials compared to CON (p<.001).
The muscles also differed from each other within each startle condition.
During CON, FST and AST the quadriceps had significantly increased peak EMG
values than hamstrings (p<.001). CON trials showed a significant delay TTP for the
quadriceps compared to the hamstrings (p<.05). FST and AST had significant longer
TTP in quadriceps than hamstrings (p<.05) with AST also showing slower TTP in
lateral hamstrings than medial hamstrings (p=.048). CON and FST displayed longer
onset of VM compared to VL, MH and LH (p<.001) as well as MH delays to LH
(p<.05). CON also demonstrated decreased onset in VL than MH (p=.026) and AST
had longer onset in VM compared to VL and LH (p=.036 and p=.005). CON showed
increase in VM pre-perturbation activity than VL (p=.041) while FST and AST
displayed decrease in MH activity than VM (p<.05). All trials had an increase in post-

13
perturbation VM activity than the hamstrings (p<.05) with FST and AST also showing
increase in VL than MH (p<.05).
3.3 Startle Effects on Group Differences No significant group differences were observed for stiffness values. No
significant group by trial interaction effects was observed for either stiffness value.
No significant group differences were observed for any EMG variables. A significant
group by muscle interaction was only found for areas 250ms and 250-500ms
following the perturbation (p<.05). For the post-perturbation area, the FF and FO
groups has significantly higher EMG activity in VM compared to LH (p=.008 and
p=.027). Additionally, the FO group showed significantly less activity in MH than
both VM and VL (p<.001 and p=.011). In post-post perturbation area, both female
groups had significantly higher VM and VL activity compared to MH and LH
(p<.001) while ML demonstrated significant less activity in MH than both VM and
VL (p=.003 and p=.004). Furthermore, the VM had significantly decreased activity in
ML than FO (p=.024). No significant group by startle interaction effect for any EMG
variable was observed.
Results for electromechanical delay (EMD) are presented in Table 4. No
significant differences were observed between groups; however, differences were
detected between muscles, p<.001. Post-hoc analysis indicated MH had a significant
higher EMD than VM, VL and LH (p<.001).

14
Chapter 4
DISCUSSION
The purpose of the present study was to determine how stiffness of the knee
joint is affected by an acoustic startle, as well as hormonal differences associated with
gender and the menstrual cycle. Neuromuscular, neurocognitive, and mechanical
differences are thought to play a significant role in the high incidence (70%) of non-
contact joint injury mechanisms (Boden et al., 2000; Fleming et al., 2003), and even
greater factor among females who suffer a disproportionate number (2-8x greater) of
ACL tears compared to males. (Arendt & Dick, 1995; Eiling et al., 2007; Griffin et al.,
2000; C. Swanik et al., 2007) However, few studies have investigated the influence of
extrinsic factors, such as startling events, on the neuromuscular control and joint
stiffness regulation needed for knee stability. The primary finding of this study was
that joint stiffness and muscle activation patterns were significantly affected by an
acoustic startle in both males and females, while differences between groups were not
observed. These findings suggest that startling events may negatively influence the
normal stiffness regulation strategies needed for functional joint stability regardless of
gender, and attenuation of this startle response should be considered in future knee
injury mechanism and prevention studies.
4.1 Stiffness Regulation and the Acoustic Startle
A measure of the resistance provided by a joint to external loading is crucial
for understanding functional stability and injurious mechanisms, as one’s failure to
optimally regulate joint stiffness can lead to excessive loading in capsuloligamentous

15
structures and potential damage. Furthermore, since joint stiffness is largely dependent
on muscle recruitment, including measures of muscle activity can allow greater
understanding of where failures in stiffness regulation may be occurring beyond that
provided by passive connective tissue structures. Muscular contraction can increase
joint stiffness 10-fold, however an optimal level of stiffness is task dependent, and
based on both performance and stability needs (Swanik 1997; Nichols & Houk 1976;
Rack & Westbury, 1974). In order to maintain proper biomechanical alignment the
joint must undergo a controlled, columnar buckling, with the majority of energy being
absorbed and dissipated in the eccentric lengthening of surrounding musculature rather
than capsuloligamentous tissue (Hewett & Torg, 2009). These highly coordinated
muscle activation strategies include pre-programmed preparatory contractions, pre-
planned reflexes and involuntary reactions developed from within the central nervous
system (CNS) and therefore susceptible to strong stimuli and unanticipated events.
The acoustic startle is one example frequently used as a research model to assess the
effects of sensory stimuli on the CNS.
Startle events have been hypothesized to alter neuromuscular control by
disturbing both preparatory and reactive neuronal circuitry at the level of the
brainstem. (Ghez & Krakauer, 1991, Koch, 1999) These planned reflexes can help
explain how people will react to an event when anticipating certain proprioceptive
circumstances during activity (Nieuwenhuijzen et al, 2000). While studies have
investigated the effect of a startle on these neuronal circuits, and involuntary muscular
responses (Yeomans 1995; Koch 1999; Moffit et al. 2012), no research has

16
investigated its potential secondary effect on a measure of joint stability such as
stiffness.
Our results found an increase in short-range stiffness following the startle, but
then a decrease in total stiffness, which encompasses and larger, functional range of
motion. Limited research is available with the startle and biomechanics, but a study
by Nieuwenhuijzen et al showed decreases in leg musculature range-of-motion during
a gait analysis (2000) and Moffit et al displayed changes in neuromuscular activation
with an applied startle (2012). Short-range stiffness is typically associated with the
passive components of the joint, a reverse pivot of bound actin-myosin cross-bridges,
as well as the series and parallel elastic components of the muscle. (Sinkjaer et al.,
1988, Crago et al, 1976; Nichols & Houk 1976; Houk et al, 1967) Our startle response
was purposely initiated in a brief period of time before the external knee perturbation,
in an attempt to replicate a potential unanticipated sensory disturbance just prior to
joint loading, which may occur during physical activity. The higher short-range
stiffness likely reflects a disturbance in neuromuscular control as we found earlier
quadriceps muscle activation during these trials. Quadriceps activation is important for
maintaining knee stability because this group is among the primary antigravity
muscles (Bellew, 2002). However, when contracting earlier that anticipated during
the joint range of motion, the quadriceps may contribute to increased anterior shear
forces and a knee hyperextension moment. This combination would potentially place
the knee in a more vulnerable position for ACL injury (Rozzi et al, 1999; Griffin et al,
2000).

17
In addition to altered short-range stiffness, our results also supported
decreased stiffness for the entire 40-degree perturbation. The total-stiffness is largely
dependent on the ability to regulate the reverse cross-bridge cycling of an eccentric
contraction as the knee is forced into flexion (Sinkjaer et al, 1998). Our results showed
that the startle caused an initial, early heightening of joint stiffness that then was
attenuated throughout the remainder of the perturbation; a potentially detrimental
combination for avoiding knee injury. Previous studies have also linked alterations in
muscle stiffness to knee injury. (Swanik 2007; Blackburn et al 2009; Boden et al
2000) The inability to sufficiently stiffen the knee, as one would normally accomplish
through muscle activation, could expose capsuloligamentous structures to excessive
loads that would otherwise be absorbed through controlled muscle lengthening.
When considering these muscle activation patterns, nearly all variables were
affected by the acoustic startle. While the quadriceps muscles were observed to have
greater EMG activity than the hamstring muscles throughout all trials, the startle
prolonged the onset and time-to-peak (TTP) activity of the vastus medialis muscle.
Furthermore, the startling event before the perturbation caused an early increase in
EMG activity but decreased muscle activity when compared to control trials during
and after the perturbation (Tables 10 & 11). We hypothesize that this overall
decreased EMG activity, in conjunction with our findings of decreased total joint
stiffness, may be related to an “uncontrolled buckling” observed in a jump landing
where absorption of ground reaction forces occurs with the joint in a more vulnerable
position. (Boden et al., 2000; Fleming et al., 2003; Hewett & Torg, 2009) If an

18
unanticipated event occurs just prior to joint loading, a startle reflex may be initiated.
The involuntary startle causes an early quadriceps activation and knee extension
moment, appearing to us as heightened short-range stiffness. Under real-world
conditions such as landing or cutting, this effect may cause the knee joint to move
towards a hyper-extended position, which is associated with ACL tears. Furthermore,
as the startle response subsides, less muscle activity was observed and subsequently
less total stiffness of the joint resulted. The level of total joint stiffness that resulted
from the startle event was less than under normal conditions, suggesting that the
optimal stiffness regulation strategy for dynamic stability was significantly disrupted.
The inability to maintain normal stiffness regulation throughout the total range of
motion could result in uncontrolled columnar buckling during functional activities
(Hewett & Torg, 2009).
For further analysis, we compared the average of 3 applied startles to the initial
startle. Previous research has suggested that following the initial startle, the effect of
subsequent startles would be diminished and therefore may make differences more
difficult to detect. (Blumenthal et al., 2005) Our results supported this finding as the
greatest differences in joint stiffness were observed in the initial trial, and several
EMG differences were observed as well (Tables 3, 5–8). The first startle had
significantly decreased total stiffness when compared to the control and average trials.
A decreased peak EMG was observed during initial trials as well as increased time-to-
peak and decreased onset times. This demonstrates that there is an attenuation of the
startle for both stiffness and muscle activation after the initial startle is introduced. It

19
is unclear how long the attenuation of a startle response may last, but these changes do
show promise for future research into prevention and rehabilitation approaches that
can minimize the potentially disruptive neuromuscular effects of sudden unanticipated
events.
4.2 Group Effects
No group differences were observed for any stiffness or EMG measures.
Throughout the literature, females are observed to tear their ACL more frequently than
males.(Huston & Wojtys, 1996; Rozzi et al., 1999) However, the reasons behind this
common phenomenon are inconclusive, often attributing differences to
neuromuscular, strength, stiffness and the female menstrual cycle characteristics.
Moreover, little attention has been directed toward explaining why males also suffer
NC-ACL injuries. (Wojtys et al., 1998; Blackburn et al., 2009; Griffin et al., 2000; C.
Swanik et al., 2007) The menstrual cycle tends to show the most hormonal changes
during the ovulation phase with some data showing increases in laxity and stiffness.
(Van Lunen et al., 2003; Wojtys et al., 1998) This study did not support the claim that
the menstrual cycle causes significant changes in neuromuscular control or stiffness.
Some theories also blame quadriceps dominance in females, leading to knee joint
hyperextension and improper mechanics; however, our study observed that all groups
recruited these muscles similarly. Previous studies tend to show a decrease in stiffness
in females compared to males, which leads to a decrease in joint stabilization and
increases in ACL injuries, however, many of these studies do not account for
normalized body weight between genders as our study did. (Blackburn et al., 2009;

20
Granata et al., 2002) Unlike other stiffness studies comparing genders, our study did
not use dynamic tasks such as jumping rather than a controlled seated dynamic
movement in order to minimize other joint axial loads and to concentrate specifically
on the knee joint.
Males tend to have greater strength, a more balanced muscle contribution,
greater muscle mass, and higher muscle fiber recruitment than females. (Blackburn et
al., 2009; Wojtys et al., 2002) In our study, females showed a decrease in MVIC for
quadriceps and hamstrings than males, supporting that females have less over-all
quadriceps and hamstring strength. The reason for females having a higher injury rate
is often contributed to the neuromuscular control strategy and their lack of control
during dynamic tasks (Rozzi et al., 1999, Griffin et al., 2000; C. Swanik et al., 2007)
Currently there is conflicting evidence, however, supporting the claims of why males
and females both suffer from a higher incidence of non-contact ACL injury. In fact,
the mechanism explaining why males also suffer from non-contact injuries has not
been offered. This study showed similar activation strategies with no significant
difference between groups. Although, from the results, female groups did have data
that was trending towards slower TTP, lower peak EMG, and slower muscle onsets. A
larger subject pool would provide more data to see if this effect continues to lead
towards significance. A group-muscle significant difference was seen with both
female groups following the 40-degree perturbation where the VM had higher EMG
activity compared to the other three muscles measured during the first startle. This
could lead towards a quad-dominance effect following startling perturbation

21
maneuvers, and this dominance could support the incidence of higher injuries. It is
possible that our startle response main effect size was large enough to conceal
potential interaction effects between groups. However, more research, with larger
subject pools is needed to provide additional evidence on whether there could be
group and gender differences with a startle event.
4.3 Limitations
One of the largest limitations to this study was that the subject pool was small
and larger groups could potentially lead to overall group differences. In future studies,
more participants are warranted to have a better understanding of how gender groups
could have altered stiffness and muscle activation patterns. In this study we measured
body weight (kg) to normalize stiffness values, however, it may be prudent to use lean
body mass due to the variations in body types that were included in this study. Lean
body mass is a more accurate portrayal of a person’s body composition. Another
limitation was that females faced the acoustic startle in more than one sitting, which
could lead to some suspicion of a habituation effect; however, prior research shows
that there is a minimal learning effect when a startle stimulus is tested on two separate
days making this limitation unlikely. The females also self-reported the accuracy of
their menstrual cycle, which is difficult to assess how honest these reports were for the
precision of our study. In future studies, ovulation kits and hormonal level testing can
improve the accuracy of the menstrual cycle timeline, which may give a better
understanding of how the 28-day cycle can alter muscle stiffness and activation.

22
4.4 Conclusion
The results from this study indicate that startle events can significantly alter
neuromuscular control and stiffness regulation strategies at the knee joint. Regardless
of gender, this event caused alterations in preparatory and reactive muscle recruitment
strategies necessary for dynamic restraint and joint stability. Overall, the first startle
caused the greatest significant differences in the measures investigated. This suggests
a single, uniquely timed startling event could expose both males and females to a
failure of the dynamic restraint mechanism and non-contact related ACL injuries.
More-over, startle events could be used in prevention and rehabilitation exercises,
however, from this study’s results, proper care should be taken due to the significant
disruption in neuromuscular control that the startle is found to have on unanticipated
perturbation maneuvers.

23
Chapter 5
LEGEND
Table 1: Demographics
Female (N=18) Male (N=18) p-value Age (yrs) 20.89 ± 1.97 21.28 ± 2.02 0.563 Weight (kg) 61.77 ± 7.63 82.75 ± 15.84 <.001† Height (cm) 164.41 ± 6.79 179.49 ± 6.86 <.001† Leg Length (cm) 40.34 ± 1.88 43.82 ± 2.02 <.001† QMVIC (Nm) 740.61 ± 230.70 1023.20 ± 272.42 .002* HMVIC (Nm) 647.20 ± 198.02 1075.81 ± 258.99 .002* *Significance at p<.05, †Significance at p<.001; QMVIC-Quadriceps maximum voluntary contraction, HMVIC – hamstrings maximum voluntary contraction

24
Table 2: Short-range (4°) Startle Normalized Stiffness (Nm/o/Kg) Independent
Variable
Mean ± SD F-Value
DF
p-value
Pairwise comparison
p-value Group Males
Females-FF Females-FO
.047±.002
.048±.005
.044±.004
.506
2
.606
Trials
Control First Average
.043±.003
.047±.002
.050±.003
4.236
1.198
.037*
C-F .003* C-A .005*
Group, Trials
Control
M FF FO
.046±.011
.042±.012
.040±.008
.461
2.395
.668
First
M FF FO
.047±.012
.049±.014
.045±.011 Average
M FF FO
.049±.018
.053±.028
.047±.024 *Significance at p<.05, M-Male, FF-Female Follicular, FO-Female Ovulation; C-Control Trials, A-Average of 3 startle trials, F-First startle trial

25
Table 3: Total (40°) Startle Normalized Stiffness (Nm/o/Kg) Independent
Variable
Mean ± SD F-Value
DF
p-value
Pairwise comparison
p-value Group Males
Females-FF Females-FO
.034±.006
.032±.005
.036±.006
.373
2
.691
Trials
Control First Average
.037±.002
.028±.002
.038±.003
11.248
1.385
.000†
C-F .004* F-A .000*
Group, Trials Control
M FF FO
.038±.016
.035±.012
.038±.013
.126
2.770
.934
First
M FF FO
.027±.022
.027±.021
.030±.020 Average
M FF FO
.038±.012
.035±.016
.041±.017 †Significance at p<.001; M-Male, FF-Female Follicular, FO-Female Ovulation; C-Control Trials, A-Average of 3 Startle Trials, F-First Startle Trial

26
Table 4: Electromechanical Delay (EMD) Values Independent
Variable
Mean ± SD (ms)
F-Value
DF
p-value Pairwise
comparison p-value
Group
Males Female-FF Female-FO
73.142 ± 7.705 73.013 ± 8.367 68.671 ± 8.550
2.315
2
.109
Muscles
VM VL MH LH
67.909 ± 4.548 66.003 ± 3.120 83.218 ± 2.083 69.306 ± 4.072
15.450
3
.000†
VM-MH .000†
VL-MH .000† MH-LH .000†
Group, Muscle
VM
M 69.738 ± 11.974 FF 71.258 ± 17.172 FO 62.732 ± 15.118
.721
6
.633
VL
M 65.448 ± 14.112 FF 69.444 ± 12.800 FO 63.117 ± 17.131
MH
M 83.472 ± 15.929 FF 85.162 ± 10.337 FO 81.019 ± 10.626
LH M 73.912 ± 15.853 FF 66.188 ± 15.301 FO 67.816 ± 16.244
†Significance at p<.001, M-Male, FF-Female Follicular, FO-Female Ovulation; VM-Vastus Medialis, VL-Vastus Lateralis, MH-Medial Hamstrings, LH-Lateral Hamstrings

27
Table 5: Peak EMG Values for Startle Passive-Reactive Trials Independent
Variable
Mean ± SD (% Max)
F-Value
DF
p-value Pairwise
comparison p-value
Group
Male Female FF Female FO
37.836 ± 17.032 40.536 ± 24.840 41.455 ± 25.768
.231
2
.795
Muscles
VM VL MH LH
62.769 ± 7.825 58.910 ± 9.267 15.806 ± 2.435 22.285 ± 4.560
55.404
1.722
.000†
VM-MH .000†
VM-LH .000† VL-MH .000† VL-LH .000†
Trials
Control First Average
42.557 ± 24.964 36.317 ± 19.204 40.954 ± 23.747
6.290
1.342
.009*
C-F .013* F-A .037*
Muscles, Trial
VM
C 68.967±3.804 F 54.820±3.906 A 64.521±7.626
4.349
2.106
.015*
C-F .017* F-A .040*
C-F .025*
C, F, A VM-MH
.000† VM-LH .000† VL-MH .000† VL-LH .000†
VL
C 62.510±9.994 F 53.367±6.483 A 60.853±11.419
MH
C 15.997±2.729 F 15.489±2.811 A 15.931±2.854
LH
C 22.755±4.031 F 21.592±6.137 A 22.509±5.305
Muscles, Group
VM
M 57.660±6.566 FF 62.988±8.558 FO 67.659±7.312
1.254
3.443
.297
VL
M 48.611±2.666 FF 64.580±9.328 FO 63.539±6.298
MH
M 17.493±2.411 FF 17.288±9.476 FO 12.636±4.490
LH
M 27.581±3.014 FF 17.287±8.514 FO 21.988±4.740
Control
M 40.412±21.686 FF 44.538±30.529

28
Trials, Group
FO 42.721±29.521 .537
2.684
.639
First M 35.528±16.346 FF 35.471±21.826 FO 37.951±24.562
Average
M 37.569±17.610 FF 41.598±28.232 FO 43.698±30.571
†Significance at p<.001, *Significance at p<.05; M-Male, FF-Female Follicular, FO-Female Ovulation; VM-Vastus Medialis, VL-Vastus Lateralis, MH-Medial Hamstrings, LH-Lateral Hamstrings

29
Table 6: Time to Peak (TTP) Values; Startle Trials Independent
Variable Mean ± SD (s) F-Value DF p-value Pairwise
comparison p-value
Group
Male Female FF Female FO
.367±.069
.398±.079
.375±.067
.215
2
.808
Muscles
VM VL MH LH
.419±.057
.438±.052
.308±.047
.356±.048
12.717
2.345
.000†
VM-MH.000† VL-MH .000† VL-LH .015*
Trials
Control First Average
.426±.074
.351±.063
.363±.056
10.762
2
.000†
C-A .002* C-F .001†
Muscles, Trial
VM
C .487±.025 F .367±.016 A .402±.023
2.466
4.337
.043*
C-A .002* C-F .000†
C-A .003* C-F .050*
C-F .046*
C VM-MH .001† VM-LH .003* VL-MH .002* VL-LH .006*
F VM-MH .000† VL-MH .001†
A VM-MH .023* VL-MH .000† MH-LH .048*
VL
C .496±.033 F .412±.020 A .405±.036
MH
C .357±.025 F .267±.018 A .301±.039
LH
C .365±.045 F .357±.066 A .345±.053
Muscles, Group
VM
M .426±.059 FF .432±.072 FO .398±.055
1.202
4.690
.316
VL
M .416±.047 FF .441±.071 FO .456±.045
M .299±.044

30
MH
FF .303±.073 FO .324±.031
LH
M .327±.022 FF .417±.014 FO .323±.019
Trials, Group
Control
M .412±.076 FF .458±.067 FO .409±.088
.333
4
.855
First M .342±.075 FF .360±.075 FO.350±.056
Average
M .347±.046 FF.377±.074 FO .366±.058
†Significance at p<.001, *Significance at p<.05; M-Male, FF-Female Follicular, FO-Female Ovulation; VM-Vastus Medialis, VL-Vastus Lateralis, MH-Medial Hamstrings, LH-Lateral Hamstrings; C-Control Trials, A-Average of 3 startle trials, F-First startle trial

31
Table 7: Time to Peak (TTP) Obicularis-Oculi; Startle Trials Independent
Variable Mean ± SD (s) F-Value DF p-value Pairwise
comparison p-value
Group
Male Female FF Female FO
.771±.341 1.110±.480 .995±.227
.642
2
.530
Trials
Control First Average
.685±.142 1.268±.297 .923±.348
4.007
1.452
.034*
Trials, Group
Control
M .521±.813 FF .762±.832 FO .773±.990
1.091
2.905
.357
First
M 1.160±1.719 FF 1.657±1.871 FO 1.226±1.622
Average
M .632±.787 FF .911±1.009 FO .987±1.054
*Significance at p<.05, M-Male, FF-Female Follicular, FO-Female Ovulation; C-Control Trials, A-Average of 3 startle trials, F-First startle trial
32
Table 8: Onset Values for Passive-Reactive (Startle) Trials Independent
Variable Mean ± SD (s) F-Value DF p-value Pairwise
comparison p-value
Group
Male Female FF Female FO
.094±.040
.068±.049
.076±.028
1.738
2
.186
Muscles
VM VL MH LH
.131±.031
.063±.016
.081±.027
.043±.023
27.450
2.517
.000†
VM-VL .000† VM-MH.000† VM-LH .000† MH-LH .006*
Trials
Control First Average
.097±.024
.063±.005
.080±.005
10.348
1.419
.001†
C-A .013* C-F .002* F-A .040*
Muscles, Trial
VM
C .166±.024 F .102±.005 A .124±.005
4.161
3.775
.004*
C-A .001† C-F .000†
C-A .024* C-F .006*
C VM-all .000† VL-MH .026* MH-LH .000†
F VM-all .000† MH-LH .027*
A VM-VL .036* VM-LH .005*
VL
C .070±.023 F .053±0.00 A .068±.017
MH
C .105±.024 F .058±.018 A .079±.020
LH
C .045±.023 F .038±.032 A .048±.023
Muscles, Group
VM
M .139±.045 FF .134±.032 FO .119±.022
1.114
5.035
.356
VL
M .079±.023 FF .055±.003 FO .056±.003
MH
M .101±.028 FF .068±.033 FO .073±.010
M .058±.008

33
LH FF .015±.012 FO .058±.010
Trials, Group
Control
M .120±.052 FF .087±.064 FO .082±.042
2.838
1.002
.394
First M .070±.023 FF .050±.044 FO .068±.019
Average
M .093±.030 FF .067±.043 FO .079±.027
†Significance at p<.001, *Significance at p<.05; M-Male, FF-Female Follicular, FO-Female Ovulation; VM-Vastus Medialis, VL-Vastus Lateralis, MH-Medial Hamstrings, LH-Lateral Hamstrings; C-Control Trials, A-Average of 3 startle trials, F-First startle trial
34
Table 9: Pre-Perturbation (150 prior-0ms) Area Values; Startle Trials Independent
Variable Mean ± SD (%) F-
Value DF p-value Pairwise
comparison p-value
Group
Male Female FF Female FO
1.407±.353 1.639±.389 1.726±.497
1.311
2
.280
Muscles
VM VL MH LH
1.954±.474 1.459±.431 1.302±.199 1.648±.275
3.198
3
.026*
VM-MH .034*
Trials
Control First Average
1.392±.357 1.707±.467 1.673±.413
11.522
1.719
.000†
C-A .001† C-F .000†
Muscles, Trial
VM
C 1.636±.392 F 2.131±.579 A 2.095±.427
5.370
2.787
.002*
C-A .031* C-F .001†
C-A .000† C-F .000†
C-F .037* C
VM-VL .041* A
VM-MH .020* F
VM-MH .022*
VL
C 1.087±.291 F 1.660±.476 A 1.629±.346
MH
C 1.264±.204 F 1.342±.249 A 1.300±.231
LH
C 1.578±.342 F 1.697±.265 A 1.668±.321
Muscles, Group
VM
M 1.437±.211 FF 2.189±.210 FO 2.235±.457
1.652
6
.138
VL
M 1.085±.273 FF 1.509±.344 FO 1.782±.423
MH
M 1.214±.007 FF 1.549±.056 FO 1.143±.025
LH
M 1.892±.045 FF 1.307±.086

35
FO 1.744±.120 Trials, Group
Control
M 1.273±.467 FF 1.455±.368 FO 1.448±.294
1.341
3.437
.266
First M 1.456±.290 FF 1.689±.370 FO 1.977±.641
Average
M 1.493±.345 FF 1.772±.457 FO 1.754±.482
†Significance at p<.001, *Significance at p<.05; M-Male, FF-Female Follicular, FO-Female Ovulation; VM-Vastus Medialis, VL-Vastus Lateralis, MH-Medial Hamstrings, LH-Lateral Hamstrings; C-Control Trials, A-Average of 3 startle trials, F-First startle trial

36
Table 10: Post-Perturbation (0-250ms) Area Values; Startle Trials Independent
Variable Mean ± SD (%) F-Value DF p-value Pairwise
comparison p-value
Group
Male Female FF Female FO
4.252±.078 4.711±1.482 4.879±1.819
.958
2
.392
Muscles
VM VL MH LH
6.125±1.106 5.078±1.055 3.234±.602 4.020±.872
9.218
3
.000†
VM-MH.000† VM-LH .005* VL-MH .017*
Trials
Control First Average
4.379±1.188 4.571±1.431 4.892±1.648
4.219
1.511
.028*
C-A .003*
Muscles, Trial
VM
C 5.844±.847 F 5.968±1.408 A 6.562±1.301
3.217
3.015
.025*
C-A .000† C
VM-MH .000†
VM-LH .025* F
VM-MH .000†
VM-LH .000† VL-MH .002*
A VM-MH
.002* VM-LH .026* VL-MH .031*
VL
C 4.508±.361 F 5.064±1.431 A 5.662±1.129
MH
C 3.219±.668 F 3.262±.732 A 3.222±.683
LH
C 3.946±.963 F 3.991±.856 A 4.123±1.163
Muscles, Group
M
VM 4.771±.461 VL 3.999±.488 MH 3.256±.066 LH 4.983±.289
2.214
5.876
.047*
VM-LH .008*
FF
VM 6.538±.573 VL 5.388±.853 MH 3.914±.103 LH 3.006±.043
VM 7.066±.536

37
FO VL 5.847±.842 MH 2.532±.036 LH 4.072±.126
VM-MH.000† VM-LH .027* VL-MH .011*
Trials, Group
Control
M 4.341±.782 FF 4.296±1.225 FO 4.501±1.742
1.591
3.023
.199
First
M 3.901±.715 FF 4.844±1.622 FO 4.969±1.879
Average
M 4.514±.910 FF 4.995±1.886 FO 5.168±2.294
†Significance at p<.001, *Significance at p<.05; M-Male, FF-Female Follicular, FO-Female Ovulation; VM-Vastus Medialis, VL-Vastus Lateralis, MH-Medial Hamstrings, LH-Lateral Hamstrings; C-Control Trials, A-Average of 3 startle trials, F-First startle trial

38
Table 11: Post-Post Perturbation (250-600ms) Area Values; Startle Trials Independent
Variable Mean ± SD (%) F-Value DF p-value Pairwise
comparison p-value
Group
Male Female FF Female FO
6.765±2.655 7.367±4.134 7.894±4.861
1.057
2
.357
Muscles
VM VL MH LH
11.134±1.533 10.676±2.038 2.950±.484 4.607±1.047
55.329
2.309
.000†
VM-MH.000† VM-LH
.000† VL-MH
.000† VL-LH .000†
MH-LH .032*
Trials
Control First Average
7.450±4.052 6.769±4.353 7.806±4.535
1.309
4.029
.039*
F-A .008*
Muscles, Trial
VM
C 11.500±1.316 F 9.935±1.439 A 11.969±1.484
1.770
3.140
.055
VL
C 10.753±1.914 F 9.803±2.232 A 11.474±2.420
MH
C 2.964±.571 F 2.844±.514 A 3.041±.563
LH
C 4.585±1.058 F 4.496±1.311 A 4.740±1.225
Muscles, Group
M
VM 9.714±1.220 VL 8.242±.823 MH 3.197±.219 LH 5.905±.168
2.452
4.618
.043*
VM-
MH.003* VL-MH
.004*
VM-MH.000† VM-LH
.000† VL-MH
FF
VM 11.195±.737 VL 11.402±.797 MH 3.325±.034 LH 3.546±.176
FO
VM 12.494±1.253 VL 12.386±1.108 MH 2.328±.056
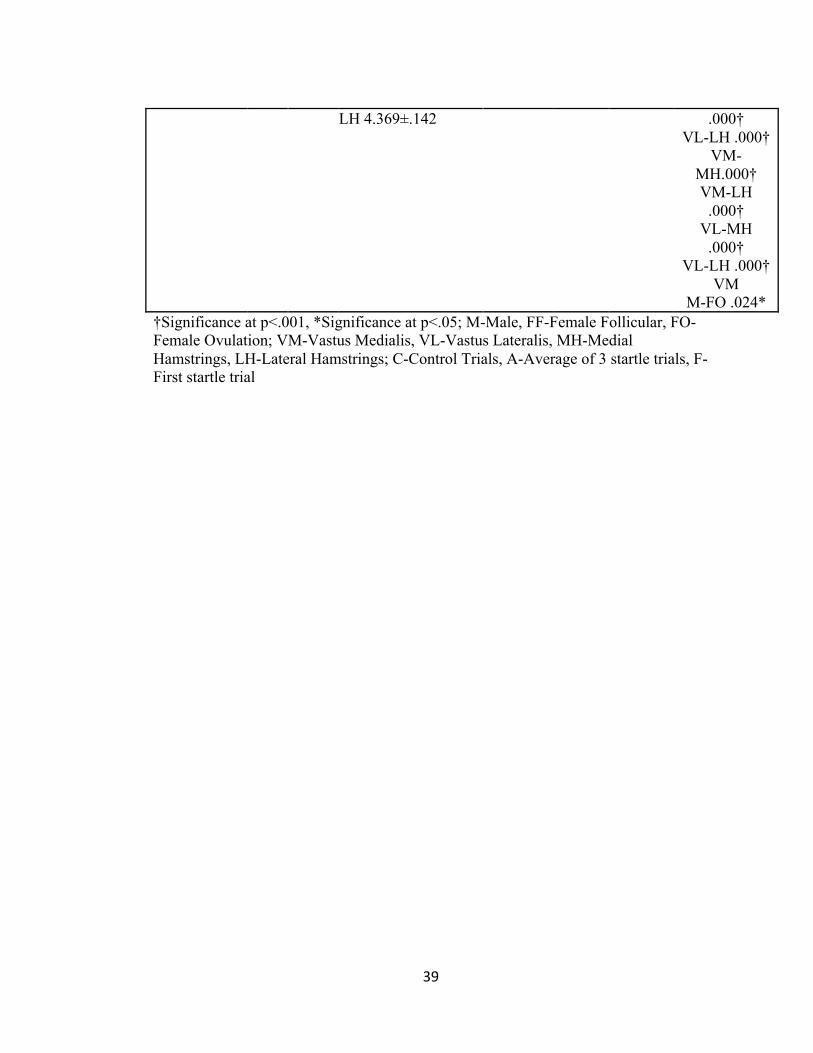
39
LH 4.369±.142 .000† VL-LH .000†
VM-MH.000† VM-LH
.000† VL-MH
.000† VL-LH .000†
VM M-FO .024*
†Significance at p<.001, *Significance at p<.05; M-Male, FF-Female Follicular, FO-Female Ovulation; VM-Vastus Medialis, VL-Vastus Lateralis, MH-Medial Hamstrings, LH-Lateral Hamstrings; C-Control Trials, A-Average of 3 startle trials, F-First startle trial

40
Chapter 6
LITERATURE REVIEW
Incidental, non-contact anterior cruciate ligament (ACL) sprains affect
primarily young (aged 15-25) athletic populations and are continuing to be a very
common knee injury. (Griffin et al., 2006; Wojtys et al., 1998) Approximately
100,000 ACL reconstruction surgeries are performed annually in the United States
with an estimated cost of $17,000 to $25,000 per case for surgical and rehabilitation
interventions.(Grindstaff, 2006) Additionally, an average of 6 months is lost from
normal activity when surgery is performed to repair the ACL. Recent research shows
osteoarthritis after 10 years in 905 surgical and nonsurgical ACL cases as well as
alterations in joint loading, which also causes complications with this injury. (Holm et
al., 2010) Generally, ACL sprains affect young women more often than men, however
conclusive studies do not exist to explain the underlying mechanisms that may be
causing this unintentional injury. (Griffin et al., 2000; Griffin et al., 2006) Because
over 70% of ACL tears are a non-contact injury, which means there was no player-on-
player contact, this infers that errors in neuromuscular control led to the injurious
biomechanics during routine functional tasks such as jump landings running and
cutting maneuvers. (Boden et al., 2000; Fleming et al., 2003; Kirkendall & Garrett,
2000; Olsen et al., 2004) It is imperative to continue research towards understanding
the mechanisms behind unintentional non-contact injury, such that prevention
programs can be implemented.

41
Joint Stabilization
The knee joint relies on both static and dynamic restraint to maintain stability.
(Lephart et al., 1992, Freeman, 1966, Johansson, 1991, C.Swanik et al., 1999)
Stiffness properties can measure the muscle tension that assists with joint stability.
Knee joint stability is influenced by multiple factors including capsulo-ligamentous
structures, muscle forces, and proprioceptive influences from static and dynamic
restraints. (C.Swanik et al., 1999) Static restraints include ligaments, bones and the
capsule that control and limit joint motion. Dynamic restraints are comprised of the
musculotendinous units, which help produce and absorb forces in response to changes
in joint loads. When static and dynamic restraints work together, they can help guide
joint kinematics and absorb loads during the high velocity movements of physical
activity. Generally, when dynamic stabilization is compromised, an increase in the
accessory motion of tibial translation can increase the risk of ACL injury. As a static
stabilizer, the ACL provides 86% of restraint against anterior tibial translation, and
when surrounding musculature do not help resist this motion, stresses beyond the
ACLs strain limit can cause tissue failure. (Butler et al., 1980) In some cases the loss
of an ACL does not result in a functionally unstable joint because quadriceps and
hamstring musculature act in synergy with the remaining static restraints, allowing
some patients to cope with the loss of the ligament. These “copers” rely on proper
muscle activation to provide dynamic stabilization. (Eastlack & Snyder-Mackler,
1999)
Dynamic stability can be described as the ability to prepare for and react to

42
unanticipated joint loads throughout activity. (Williams et al., 2001) Muscle fibers
contracting at optimal force, length and velocity relationships help maintain this type
of stability, with the quadriceps and hamstrings serving as the primary dynamic
stabilizers of the knee joint. (Branch et al., 1989; C.Swanik et al., 2004; C.Swanik et
al., 1999) Through co-contraction, both muscle groups create a state of joint force
equilibrium to help reduce the amount of anterior translation placed upon the ACL,
which if left unrestrained leads to ligament ruptures. (Li et al., 1999) Prior research
has shown that aggressive quadriceps loading increases the anterior tibial translation,
which places greater stresses on the ACL and may lead to injury.(Kirkendall &
Garrett, 2000) The quadriceps are the primary anti-gravity muscles that absorb loads
during sudden knee flexion during tasks such as landing and cutting.(Snyder-Mackler,
2007) The hamstring muscles contractions may often protect against ligament injury
as they provide a posterior tibial shear force limiting loads placed on the ACL.
(MacWilliams et al., 1999) Some females demonstrate earlier recruitment of the
quadriceps than the hamstrings delaying the hamstring reactions to anterior stress on
the ACL.(Hurd et al., 2006; Huston & Wojtys, 1996) Delayed recruitment of muscle
fibers can affect the timing of force production and mechanical restraint necessary for
joint stability.
Electromechanical delay (EMD) is defined as the time between onset of
electrical muscle activity and force production or joint motion. (Granata et al., 2000;
Moore et al., 2002) When perturbations are introduced, males tend to have a shorter
EMD compared to females (Bell & Jacobs, 1986), which for women can delay muscle

43
stiffening and place them in a more vulnerable state for injury. Pre-motor planning
and pre-activation of the muscles can affect mechanoreceptors and have been shown
to affect reactions to sudden perturbations. (Dietz et al., 1981) Rozzi et al (1999)
showed females had increased joint laxity and EMD when reacting to joint motion.
Precise pre-contractions of knee musculature can increase the joint stiffness because it
allows for a quicker force production. (Draganich et al., 1989) Stiffness properties can
measure the muscle tension that assists with joint stability.
Muscle stiffness is defined as the muscle’s ability to resist changes in length
(change in force/change in length). (Latash, 1993) Joint stiffness from the energy
exchange between static and dynamic restraints is drastically enhanced by voluntary
contractions, reflexive contractions, descending corticospinal drive, and muscle tone.
(Sinkjaer et al., 1988, C.Swanik et al., 2004) Additionally, joint stiffness may be
altered by gender differences including different muscle activation patterns, joint
biomechanics, and hormonal changes associated with the menstrual cycle; as well as
extrinsic influences such as, cognitive processes, and external stimuli. (Hausmann et
al., 2000; McCormick & Teillon, 2001; C.Swanik et al., 2007; Wojtys et al., 1998) All
of these factors can potentially cause variations in joint stiffening and neuromuscular
control, leading to an increased risk of injury to the knee ligaments. Blackburn et al
(2009) has shown that males have increases in muscle stiffness, and these have
corresponded to decreases in EMD. Females also showed a decline in force
production, which may limit the ability to maintain joint equilibrium reducing overall
joint stability. However, Hinsey et al (2010) did not find gender differences in

44
stiffness when normalizing for body size and strength. If muscle stiffness is increased,
this can help maximize joint stabilization at the knee and help decrease injuries seen
within the joint. (Blackburn et al., 2009)
Neuromuscular Control
Neuromuscular control is the coordinated ability of the nervous and
musculoskeletal systems to control movements, prepare for and react to joint
perturbations. (Freeman, 1966, Lacroix, 1981, Williams et al., 2001) Unfortunately,
sport competition presents many unanticipated events that may alter the nervous and
musculoskeletal systems. Neuromuscular control incorporates proprioception, visual
influences, and vestibular feedback with cortical and spinal motor commands. (Ghez
& Krakauer, 1991; Rozzi et al., 1999; C. Swanik et al., 2007) Mechanoreceptors
embedded in muscles, joint capsules, and ligaments play a large role as sensory organs
contributing to neuromuscular control. (Johannsson, 1991) These receptors send
afferent signals to the central nervous system in response to tension, compression,
loads and other forms of mechanical deformation.(Prochazka et al., 1989) Feedback
and feed-forward motor control processes counter most unexpected changes that may
affect joint stability. (Dietz et al., 1981; Lacroix, 1981; Rozzi et al., 1999; Williams et
al., 2001) Feed-forward systems work by the pre-activation of muscles in anticipation
of changes in joint movements and loads. (Ghez & Krakauer, 1991) Feedback
systems work to provide reactive muscle activity during unanticipated tasks and
impact dynamic restraint. (C. Swanik et al., 1999; Ghez & Krakauer, 1991)
Musculotendinous mechanoreceptors include Golgi tendon organs and muscle

45
spindles. (Gordon & Ghez, 1991) Golgi tendon organs are generally found within the
musculotendinous junction of muscles and react to changes in muscle tension or force,
providing the nervous system with specific force-feedback. (Houk & Henneman,
1967; Houk & Rymer, 1981; Nichols & Houk, 1976) Muscle spindles are sensitive to
changes in muscle length and velocity and have modifiable sensitivity through the
fusimotor system. (Gordon & Ghez, 1991; Matthews, 1981) Primarily, they increase
firing in response to increases in muscle length and changes in rate of muscle
lengthening. (Gordon & Ghez, 1991; Hulliger, 1984) Their sensitivity is set in advance
depending on the specific anticipated task. Muscle stiffness is affected by the force
and length feedback properties of Golgi tendon organs and muscle spindles. (Houk &
Rymer, 1981; Nichols & Houk, 1976) If joint perturbations and outside stimuli
coincide with unforeseen events like movements to the limb or acoustic noises, the
feed-forward and feedback processes that enable dynamic stabilization and stiffness
regulation may be compromised. Some research has suggested that females may be
more prone to knee injury because of these influences.(Griffin 2000)
Gender Factors
Females are at 2-8 times greater risk of ACL injury than their male counterparts.
(Arendt & Dick, 1995; Eiling et al., 2007; Park et al., 2009) Recent research has
shown biomechanical, neuromuscular and cognitive characteristic differences
suggesting potential reasons why females may be more susceptible to this injury.
(Griffin et al., 2000; C. Swanik et al., 2007) Decreases in joint proprioception, delays
in muscle reflexes, increases in knee laxity and increases in quadriceps dominance all

46
heighten the risk for ACL injuries and are seen more in females than males.(Huston &
Wojtys, 1996; Rozzi et al., 1999)
Blackburn et al (2009) performed a study comparing gender-based
characteristics that may contribute to stiffness differences. An increase in
musculotendinous stiffness leads to changes in muscle timing and magnitude of force.
(Myer et al., 2005; Rozzi et al., 1999) Decreased values of force production and
stiffness seen in females may contribute to the greater risk of ACL injury because the
neuromechanical properties needed to activate the muscle do not transpire as quickly
in females than males. A key finding of this study showed greater stiffness values
correlated with the cross-sectional area of the muscles suggesting males will have
increased stiffness. (Blackburn et al., 2009) However, there is limitation to
Blackburn’s study as stiffness was extrapolated from oscillating perturbation, rather
than using true measured values of stiffness. Males demonstrated a heightened
musculotendinous stiffness allowing for increases in joint stability. (Blackburn et al.,
2009) Since females generally have less muscle mass than males, females show
decreases in stiffness and delays in producing force, which could cause an increase in
injuries. (Blackburn et al., 2009; Wojtys et al., 2002) Due to a relatively quicker force
production of the hamstrings in males, the amount of anterior tibial translation would
therefore be limited and provide better stability to the knee joint. Hormonal effects
have been linked to differences seen between males and females caused primarily by
the menstrual cycle.
The 28-day female menstrual cycle is one of the greatest differences between
47
genders. (Van Lunen et al., 2003; Wojtys et al., 1998) Estrogen is the leading hormone
that shows changes throughout the menstrual cycle and is thought to contribute to the
increase of female ACL injury. (Deie et al., 2002; Eiling et al., 2007; Adachi et al.,
2008) Estrogen peaks during the ovulation days: 10-14(Wojtys et al., 1998), and is
found to affect decreases in soft tissue strength, increases in laxity, decreases in
muscle function and the central nervous system. (Sciore et al., 1998; Shikata et al.,
1979) Another hormone that has gained increasing attention is relaxin, not found in
males, which also has receptors on the ACL and may be influenced by estrogen.
(Dragoo et al., 2003; Sherwood et al., 1993) Several studies have found laxity to peak
during the ovulation period of the female cycle. (Deie et al., 2002; Eiling et al., 2007;
Park et al., 2009) There is an increase in injury rate during the ovulation stage found
as well. (Wojtys et al., 1998) However, Zazulak et al (2006) produced a systematic
review showing six of the nine studies examined did not show a laxity and cycle
correlation.
Effects on motor skills from estrogen increases are influenced by menstrual
symptoms, which cause decreases in neuromuscular joint protection. (Wojtys et al.,
1998) Some of these suggested motor effects include fine motor dexterity skills,
diminished muscular protection to the joint and decreases in musculotendinous
stiffness. (Eiling et al., 2007) Neural effects caused by menstrual cramps and
discomfort, usually peaking during ovulation, has also been thought to add to high
incidence of ACL injury in women. (Eiling et al., 2007) It has been suggested that
these premenstrual symptoms causing discomforts and pain contribute to alterations in

48
athletic performance and neuromuscular control, which may contribute to non-contact
injury. (Arendt & Dick, 1995; Eiling et al., 2007) Dysfunctions to the females during
the cycle have been studied previously showing changes, however, the results are not
conclusive. This study will look into how an acoustic startle disruption will affect
female muscular activity and joint stiffness during the menstrual cycle changes.
Startle Response
Disruptions from acoustic startles such as whistles and crowd noise may also
alter the processes for muscle stiffness and neuromuscular control regulations in
protecting the joint.(Koch, 1999) A universal startle response is provoked during these
unexpected events, and neuromuscular control changes can be observed through
alterations in preparatory (feed-forward) and reactive (feedback) muscle contractions,
potentially altering the stiffness regulation necessary for dynamic joint stabilization.
(Ghez & Krakauer, 1991) The startle reflex usually begins by a contraction of the
facial muscles in response to sudden intense visual, tactile or auditory stimuli, with the
eye-blink being the first seen response controlled by the orbicularis oculi: a striated
sphincter muscle encircling the orbit that closes the eye during a blink. (Blumenthal et
al., 2005; Braff et al., 2001; Koch, 1999; Landis & Hunt, 1939) The acoustic startle is
primarily used in the laboratory setting to elicit a response.(Favaron et al., 2010)
Blumenthal et al (2005) reported that the best way to record EMG activity of the
orbicularis oculi and record the first activity after a startle is to place electrodes below
the lower eyelid. Collecting the response from this location shows the first central
nervous system response to the startle from the facial musculature. An acoustic

49
startle causes a response to an outside stimulus where the body has a parasympathetic
response and is described as a startle reflex through a motor response. (Favaron et al.,
2010; Nieuwenhuijzen et al., 2000) The acoustic startle is influenced by stimulus
intensity, interval, other motor behavior and genetic differences. (Davis, 1970)
Habituation is shown in a reduction of response from an acoustic startle meaning that
the first introduction to the stimulus generally creates the greatest response compared
to trials without the stimulus.(Davis, 1984; Koch, 1999) Males are shown to have a
greater pre-pulse inhibition (PPI) response to the startle compared to females. (Braff
et al., 2001; Swerdlow et al., 1993b) Swerdlow et al suggest that the hormonal
changes between males and females cause variability in the response to outside
stimuli. PPI limits the reaction to a strong stimulus, such as loud acoustic noise. This
allows the nervous system to adjust when this occurs and the muscles functionally
adapt to the outside stimuli. (Braff et al., 2001; Swerdlow et al., 1993b)
A neuronal circuit made of three sets of synapses in the lower brainstem
mediates the startle response. (Davis et al., 1982) These three synapses are started with
spiral ganglion cells in the cochlea, followed by the cochlear root neurons synapsing
onto the pontine reticular nucleus (PnC) and the PnC neurons synapsing on spinal and
cranial motor neurons. (Davis et al., 1982) This circuit is highly controlled through
the role of PnC. (Koch et al., 1992) Although the pathway ends with cranial motor
neurons, parallel pathways can also effect extremities including the knee
joint.
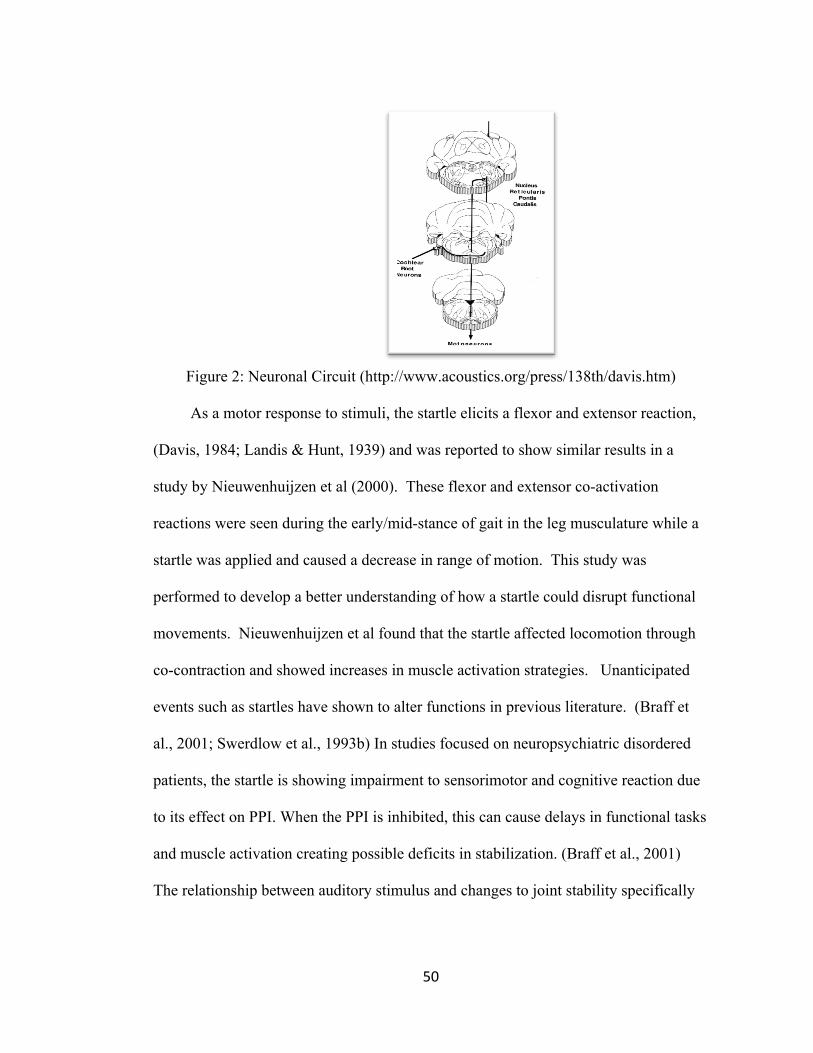
50
Figure 2: Neuronal Circuit (http://www.acoustics.org/press/138th/davis.htm)
As a motor response to stimuli, the startle elicits a flexor and extensor reaction,
(Davis, 1984; Landis & Hunt, 1939) and was reported to show similar results in a
study by Nieuwenhuijzen et al (2000). These flexor and extensor co-activation
reactions were seen during the early/mid-stance of gait in the leg musculature while a
startle was applied and caused a decrease in range of motion. This study was
performed to develop a better understanding of how a startle could disrupt functional
movements. Nieuwenhuijzen et al found that the startle affected locomotion through
co-contraction and showed increases in muscle activation strategies. Unanticipated
events such as startles have shown to alter functions in previous literature. (Braff et
al., 2001; Swerdlow et al., 1993b) In studies focused on neuropsychiatric disordered
patients, the startle is showing impairment to sensorimotor and cognitive reaction due
to its effect on PPI. When the PPI is inhibited, this can cause delays in functional tasks
and muscle activation creating possible deficits in stabilization. (Braff et al., 2001)
The relationship between auditory stimulus and changes to joint stability specifically

51
at the knee is not highlighted in current literature which could add further knowledge
to the ACL injury occurrences in sport.
Summary
ACL injuries affect many athletes every year, but more females than males.
Quadriceps and hamstring stiffness contributes to muscle firing and activation
differently in males and females. Decreased stiffness values are often seen as a
contributing factor to ACL injuries, which can be preventable with better dynamic
stabilization. The female menstrual cycle has continuing estrogen hormonal fluxes
during the 28-day period, which shows alterations in neuromuscular control and joint
stability. When these processes are altered, the risk of injury increases in the female
population. The acoustic startle response can also disrupt muscular stiffness, dynamic
joint stability, and may interact with the menstrual cycle to cause variations in
neuromuscular control. Studying gender differences combined with a startle stimulus
may lead to further insight to causes of ACL injury.

52
Chapter 7
REFERENCES
Adachi, N., Nawata, K., Maeta, M., & Kurozawa, Y. (2008). Relationship of the menstrual cycle phase to anterior cruciate ligament injuries in teenaged female athletes. Archives of Orthopaedic and Trauma Surgery, 128(5), 473-478.
Arendt, E., & Dick, R. (1995). Knee injury patterns among men and women in collegiate basketball and soccer: NCAA data and review of literature. The American Journal of Sports Medicine, 23(6), 694-701.
Baratta, R., Solomonow, M., Zhou, B. H., Letson, D., Chuinard, R., & D'Ambrosia, R. (1988). Muscular coactivation. the role of the antagonist musculature in maintaining knee stability. The American Journal of Sports Medicine, 16(2), 113-122.
Baumeister, J., Reinecke, K., & Weiss, M. (2008). Changed cortical activity after anterior cruciate ligament reconstruction in a joint position paradigm; an EEG study. Scandanavian Journal of Medical Sports Science, 18(4), 473-484.
Bell, D. G., & Jacobs, I. (1986). Electro-mechanical response times and rate of force development in males and females Medicine and Science in Sports and Exercise, 18(1), 31-36.
Bellew, J.W. (2002). The effect of strength training on control of force in older men and women. Aging Clinical and Experimental Research, 14(1), 35-41.
Blackburn, J. T., Bell, D. R., Norcross, M. F., Hudson, J. D., & Engstrom, L. A. (2009). Comparison of hamstring neuromechanical properties between healthy males and females and the influence of musculotendinous stiffness Journal of Electromyography and Kinesiology : Official Journal of the International Society of Electrophysiological Kinesiology, 19(5), e362-9.
Blumenthal, T. D., Cuthbert, B. N., Filion, D. L., Hackley, S., Lipp, O. V., & van Boxtel, A. (2005). Committee report: Guidelines for human startle eyeblink electromyographic studies. Psychophysiology, 42(1), 1-15.
Boden, B. P., Dean, G. S., Feagin, J. A.,Jr, & Garrett, W. E.,Jr. (2000). Mechanisms of anterior cruciate ligament injury. Orthopedics, 23(6), 573-578.
Braff, D. L., Geyer, M. A., & Swerdlow, N. R. (2001). Human studies of prepulse inhibition of startle: Normal subjects, patient groups, and pharmacological studies. Psychopharmacology, 156(2-3), 234-258.
Branch, T. P., Hunter, R., & Donath, M. (1989). Dynamic EMG analysis of anterior cruciate deficient legs with and without bracing during cutting. The American Journal of Sports Medicine, 17(1), 35-41.
Butler, D. L., Noyes, F. R., & Grood, E. S. (1980). Ligamentous restraints to anterior-posterior drawer in the human knee. A biomechanical study. The Journal of Bone and Joint Surgery.American Volume, 62(2), 259-270.

53
Crago, P.E., Houk, J.C., & Hasan, Z. (1976) Regulatory actions of human stretch reflex. Journal of Neurophysiology, 39, 925-935.
Davis, M. (1970). Effects of interstimulus-interval-length and varia- bility on startle-response habituation in the rat. J. Comp Physiol. Phychol., 72, 177-192.
Davis, M. (1984). The mammalian startle response. (pp. 287-351). New York: Plenum.
Deie, M., Sakamaki, Y., Sumen, Y., Urabe, Y., & Ikuta, Y. (2002). Anterior knee laxity in young women varies with their menstrual cycle. International Orthopaedics, 26(3), 154-156.
Dietz, V., Noth, J., & Schmidtbleicher, D. (1981). Interaction between pre-activity and stretch reflex in human triceps brachii during landing from forward falls.The Journal of Physiology, 311, 113-125.
Dragoo, J. L., Lee, R. S., Benhaim, P., Finerman, G. A., & Hame, S. L. (2003). Relaxin receptors in the human female anterior cruciate ligament. The American Journal of Sports Medicine, 31(4), 577-584.
Eastlack, M. E., Axe, M. J., & Snyder-Mackler, L. (1999). Laxity, instability, and functional outcome after ACL injury: Copers versus noncopers. Medicine and Science in Sports and Exercise, 31(2), 210-215.
Eiling, E., Bryant, A. L., Petersen, W., Murphy, A., & Hohmann, E. (2007). Effects of menstrual-cycle hormone fluctuations on musculotendinous stiffness and knee joint laxity. Knee Surgery, Sports Traumatology, Arthroscopy : Official Journal of the ESSKA, 15(2), 126-132.
Favaron, E., Bellodi, L., Biffi, S., Vanni, G., Zorzi, C., Liperi, L., et al. (2010). Acoustic startle response in panic disorder Psychiatry Research, 176, 254-256.
Fleming, B. C., Ohlen, G., Renstrom, P. A., Peura, G. D., Beynnon, B. D., & Badger, G. J. (2003). The effects of compressive load and knee joint torque on peak anterior cruciate ligament strains. American Journal of Sports Medicine, 31(5), 701-707.
Freeman, M.R.; Wyke, B. (1966) Articular contributions to limb reflexes: the effects of partial
neurectomy of the knee-joint on postural reflexes. Brit J Surg, 53, 61-68. Ghez, C., & Krakauer, J. (1991). Voluntary movement. In E. R. Kandel, J. H.
Schwartz & T. M. Jessell (Eds.), (4th ed., pp. 756-781). New York, NY: Elsevier Science Publishing.
Gordon, J., & Ghez, C. (1991). Muscle receptors and spinal reflexes: The stretch reflex. (3rd ed., pp. 564-580). New York, NY: Elsevier.
Granata, K. P., Ikeda, A. J., & Abel, M. F. (2000). Electromechanical delay and reflex response in spastic cerebral palsy. Archives of Physical Medicine and Rehabilitation, 81(7), 888-894.
Griffin, L. Y., Agel, J., Albohm, M. J., Arendt, E. A., Dick, R. W., Garrett, W. E., et al. (2000). Noncontact anterior cruciate ligament injuries: Risk factors and prevention strategies. The Journal of the American Academy of Orthopaedic Surgeons, 8(3), 141-150.

54
Griffin, L. Y., Albohm, M. J., Arendt, E. A., Bahr, R., Beynnon, B. D., Demaio, M., et al. (2006). Understanding and preventing noncontact anterior cruciate ligament injuries: A review of the hunt valley II meeting, january 2005.The American Journal of Sports Medicine, 34(9), 1512-1532.
Grindstaff, T. L., Hammill, R. R., Tuzson, A. E., & Hertel, J. (2006). Neuromuscular control training programs and noncontact anterior cruciate ligament injury rates in female athletes: A numbers-needed-to-treat analysis. Journal of Athletic Training, 41(4), 450-456.
Hausmann, M., Slabbekoorn, D., Van Goozen, S. H., Cohen-Kettenis, P. T., & Gunturkun, O. (2000). Sex hormones affect spatial abilities during the menstrual cycle. Behavioral Neuroscience, 114(6), 1245-1250.
Hewett, T.E., Torg, J.S., Boden, B.P., & Knowles, S.B. (2009). Video analysis of anterior cruciate ligament injury: abnormalities in hip and ankle kinematics. American Journal of Sports Medicine, 37(2), 252-259.
Holm, I., Oiestad, B. E., Risberg, M. A., & Aune, A. K. (2010). No difference in knee function or prevalence of osteoarthritis after reconstruction of the anterior cruciate ligament with 4-strand hamstring autograft versus patellar tendon-bone autograft: A randomized study with 10-year follow-up. The American Journal of Sports Medicine, 38(3), 448-454.
Houk, J., & Henneman, E. (1967). Responses of golgi tendon organs to active contractions of the soleus muscle of the cat. Journal of Neurophysiology, (3), 481.
Houk, J., & Rymer, W. Z. (1981). Neural control of muscle length and tension. (pp. 257-323). Bethesda, MD: V.B. Brooks.
Hulliger, M. (1984). The mammalian muscle spindle and its central control. Reviews of Physiology, Biochemistry and Pharmacology, 101, 1-110.
Hurd, W. J., Chmielewski, T. L., & Snyder-Mackler, L. (2006). Perturbation-enhanced neuromuscular training alters muscle activity in female athletes. Knee Surgery, Sports Traumatology, Arthroscopy : Official Journal of the ESSKA, 14(1), 60-69.
Huston, L. J., & Wojtys, E. M. (1996). Neuromuscular performance characteristics in elite female athletes. The American Journal of Sports Medicine, 24(4), 427-436.
Johansson, H., Sjolander, P., & Sojka, P. (1991). A sensory role for the cruciate ligaments. Clinical Orthopaedics and Related Research, (268)(268), 161-178.
Jovanovic, T., Szilagyi, S., Chakravorty, S., Fiallos, A. M., Lewison, B. J., Parwani, A., et al. (2004). Menstrual cycle phase effects on prepulse inhibition of acoustic startle. Psychophysiology, 41(3), 401-406.
Kirkendall, D. T., & Garrett, W. E.,Jr. (2000). The anterior cruciate ligament enigma. injury mechanisms and prevention. Clinical Orthopaedics and Related Research, (372)(372), 64-68.
Koch, M. (1999). The neurobiology of startle Progress in Neurobiology, 59(2), 107-128.
Koch, M., LingenhoÈhl, K., & Pilz, P. K. (1992).Loss of the acoustic startle response following lesions of the caudal pontine reticular formation:Possible role of giant neurons.Neuroscience, 49, 617-625.

55
Kofler, M., Muller, J., Reggiani, L., & Valls-Sole, J. (2001). Influence of gender on auditory startle responses Brain Research, 921(1-2), 206-210.
Lacroix, J. M. (1981). The acquisition of autonomic control through biofeedback: The case against an afferent process and a two-process alternative. Psychophysiology, 18(5), 573-587.
Landis, C., & Hunt, W. A. (1939). The startle pattern. New York: Farrar and Rinehart. Latash, M. L., & Zatsiorsky, V. M. (1993). Joint stiffness: Myth or reality?. Human
Movement Science, 12(6), 653-692. Lephart, S.M.; Perrin, D.H.; Fu, F.H.; Gieck, J.H.; McCue, F.C.; Irrgang, J. (1992) Relationship between
selected physical characteristics and functional capacity in the anterior cruciate-insufficient
athlete. J Orthop Sports Phys Ther, 16, 174-180. Leumann, L., Sterchi, D., Vollenweider, F., Ludewig, K., & Fruh, H. (2001). A neural
network approach to the acoustic startle reflex and prepulse inhibition. Brain Research Bulletin, 56(2), 101-110.
Li, G., Rudy, T. W., Sakane, M., Kanamori, A., Ma, C. B., & Woo, S. L. (1999). The importance of quadriceps and hamstring muscle loading on knee kinematics and in-situ forces in the ACL. Journal of Biomechanics, 32(4), 395-400.
MacWilliams, B. A., Wilson, D. R., DesJardins, J. D., Romero, J., & Chao, E. Y. (1999). Hamstrings cocontraction reduces internal rotation, anterior translation, and anterior cruciate ligament load in weight-bearing flexion. Journal of Orthopaedic Research : Official Publication of the Orthopaedic Research Society, 17(6), 817-822.
Matthews, P. B. (1981). Evolving views on the internal operation and functional role of the muscle spindle. The Journal of Physiology, 320, 1-30.
McCormick, C. M., & Teillon, S. M. (2001). Menstrual cycle variation in spatial ability: Relation to salivary cortisol levels. Hormones and Behavior, 39(1), 29-38.
Moore, B. D., Drouin, J., Gansneder, B. M., & Shultz, S. J. (2002). The differential effects of fatigue on reflex response timing and amplitude in males and females. Journal of Electromyography and Kinesiology : Official Journal of the International Society of Electrophysiological Kinesiology, 12(5), 351-360.
Myer, G. D., Ford, K. R., & Hewett, T. E. (2005). The effects of gender on quadriceps muscle activation strategies during a maneuver that mimics a high ACL injury risk position. Journal of Electromyography and Kinesiology : Official Journal of the International Society of Electrophysiological Kinesiology, 15(2), 181-189.
Nichols, T. R., & Houk, J. (1976). Improvement in linearity and regulation of stiffness that results from actions of stretch reflex. Journal of Neurophysiology, (1), 119-142.
Nieuwenhuijzen, P. H., Schillings, A. M., Van Galen, G. P., & Duysens, J. (2000). Modulation of the startle response during human gait. Journal of Neurophysiology, 84(1), 65-74.

56
Olsen, O. E., Myklebust, G., Engebretsen, L., & Bahr, R. (2004). Injury mechanisms for anterior cruciate ligament injuries in team handball: A systematic video analysis. The American Journal of Sports Medicine, 32(4), 1002-1012.
Park, S. K., Stefanyshyn, D. J., Loitz-Ramage, B., Hart, D. A., & Ronsky, J. L. (2009). Changing hormone levels during the menstrual cycle affect knee laxity and stiffness in healthy female subjects. The American Journal of Sports Medicine, 37(3), 588-598.
Prochazka, A., Trend, P., Hulliger, M., & Vincent, S. (1989). Ensemble proprioceptive activity in the cat step cycle: Towards a representative look-up chart. Progress in Brain Research, 80, 61-74; discussion 57-60.
Rack, P.M. & Westbury, D.R. (1974) The short range stiffness of active mammalian muscle and its effect on mechanical properties. Journal of Physiology, 240(2), 331-350.
Rozzi, S. L., Lephart, S. M., Gear, W. S., & Fu, F. H. (1999). Knee joint laxity and neuromuscular characteristics of male and female soccer and basketball players. The American Journal of Sports Medicine, 27(3), 312-319.
Sciore, P., Frank, C. B., & Hart, D. A. (1998). Identification of sex hormone receptors in human and rabbit ligaments of the knee by reverse transcription-polymerase chain reaction: Evidence that receptors are present in tissue from both male and female subjects. Journal of Orthopaedic Research : Official Publication of the Orthopaedic Research Society, 16(5), 604-610.
Sherwood, O. D., Downing, S. J., Guico-Lamm, M. L., Hwang, J. J., O'Day-Bowman, M. B., & Fields, P. A. (1993). The physiological effects of relaxin during pregnancy: Studies in rats and pigs. Oxford Reviews of Reproductive Biology, 15, 143-189.
Shikata, J., Sanada, H., Tamamuro, T., & Takeda, T. (1979). Experimental studies of the elastic fiber of the capsular ligament: Influence of ageing and sex hormones on the hip joint capsule of rats. Connective Tissue Research, 7(1), 21-27.
Sinkjaer, T., Toft, E., Andreassen, S., & Hornemann, B. C. (1988). Muscle stiffness in human ankle dorsiflexors: Intrinsic and reflex components. Journal of Neurophysiology, 60(3), 1110-1121.
Snyder-Mackler, L.; Hurd, W.J. (2007) Knee instability after acute ACL rupture affects movement patterns during the mid-stance phase of gait. J Orthop Research, 25(10), 1369-1377.
Swanik, C. B., Lephart, S. M., Swanik, K. A., Stone, D. A., & Fu, F. H. (2004). Neuromuscular dynamic restraint in women with anterior anterior cruciate ligament injuries. Clin Orthop Relat Res, 425, 189-199.
Swanik, C. B., Covassin, T., Stearne, D. J., & Schatz, P. (2007). The relationship between neurocognitive function and noncontact anterior cruciate ligament injuries. The American Journal of Sports Medicine, 35(6), 943-948.
Swanik, C. B., Lephart, S. M., Giraldo, J. L., Demont, R. G., & Fu, F. H. (1999). Reactive muscle firing of anterior cruciate ligament-injured females during functional activities. Journal of Athletic Training, 34(2), 121-129.

57
Swerdlow, N. R., Monroe, S. M., Hartston, H. J., Braff, D. L., Geyer, M. A., & Auerbach, P. P. (1993b). Men are more inhibited than women by weak prepulses. Biol Psychiatry, 34, 253-261.
Van Lunen, B. L., Roberts, J., Branch, J. D., & Dowling, E. A. (2003). Association of menstrual-cycle hormone changes with anterior cruciate ligament laxity measurements. Journal of Athletic Training, 38(4), 298-303.
Williams, G. N., Chmielewski, T., Rudolph, K., Buchanan, T. S., & Snyder-Mackler, L. (2001). Dynamic knee stability: Current theory and implications for clinicians and scientists. The Journal of Orthopaedic and Sports Physical Therapy, 31(10), 546-566.
Wojtys, E. M., Ashton-Miller, J. A., & Huston, L. J. (2002). A gender-related difference in the contribution of the knee musculature to sagittal-plane shear stiffness in subjects with similar knee laxity. The Journal of Bone and Joint Surgery.American Volume, 84-A(1), 10-16.
Wojtys, E. M., Huston, L. J., Lindenfeld, T. N., Hewett, T. E., & Greenfield, M. L. (1998). Association between the menstrual cycle and anterior cruciate ligament injuries in female athletes. The American Journal of Sports Medicine, 26(5), 614-619.
Zazulak, B. T., Paterno, M., Myer, G. D., Romani, W. A., & Hewett, T. E. (2006). The effects of the menstrual cycle on anterior knee laxity: A systematic review. Sports Medicine (Auckland, N.Z.), 36(10), 847-862.

58
APPENDIX A
Stiffness and Proprioception Assessment Device
Stiffness testing will be performed using a custom-built stiffness and
proprioception assessment device (SPAD) (Appendix 2). The SPAD is a brushless
Danaher/Kollmorgen servomotor (B-404-B-B4) that is fitted into a gearbox (UT018-
050, 50:1) that is connected to an amplifier/controller (Copley Xenus driver XSL-12-
36-R). The amplifier (input: 230 VAC, 3PH, output: 18 FLA, 50/60 Hz) is mounted
~4ft above the ground and connected to the motor with a 12-foot long feedback cable
(Model # CEF-RO- 006-900, Pacific Scientific, Rockford, IL) and also connected to a
personal computer through a Kvasar CAN cable. The controller receives a three-
phase, 240-volt, 30-amp enclosed I-T-E switch power supply through a power cable
(Model # CEP-A6-006-904, Pacific Scientific, Rockford, IL). The mated servomotor
and gearbox are mounted in a cast aluminum pedestal that is offset from the subject’s
chair. An adaptor arm and torque reaction sensor (Model # T5400, Futek Advanced
Sensor Technology, Irvine, CA) with a 565 N capacity and 1.43 X 105 ft-lb/rad
torsional stiffness is coupled to the gearbox. Signals from the torque reaction sensor
pass through a conditioner (Model # D502, Futek Advanced Sensor Technology,
Irvine, CA) at 60 Hz and have a 0 to 10 Vdc analog output range. The signal
conditioner digitally displays torque values and also sends an analog torque signal
through a BNC box so that is can be recorded and displayed in LabVIEW software.
For safety purposes, internal motor settings cannot exceed preset speeds and there are
three emergency stop switches that can disable the motor during testing. The operator

59
and test participant will each hold an emergency stop button. When depressed, the
motor is disabled. Also, if the adaptor arm moves within the last 5% of the
participant’s end range of motion a proximity sensor (#S4602896, Turck Inc. USA,
Minneapolis, MN) will disable the motor. When the motor is disabled, the operator
must re-start the power supply to continue tests. The LabVIEW motor control
software also has “soft limits” which will disable the motor amplifier if motion
exceeds individualized motion limits. The SPAD is also fitted mechanical stops to
limit motion through an adjustable range and brass screws in the adapter arm flange
connected to the gear box which will fail under excessive torque. The SPAD device is
operated using a personal computer with a customized LabVIEW virtual instrument
and motor control software program.
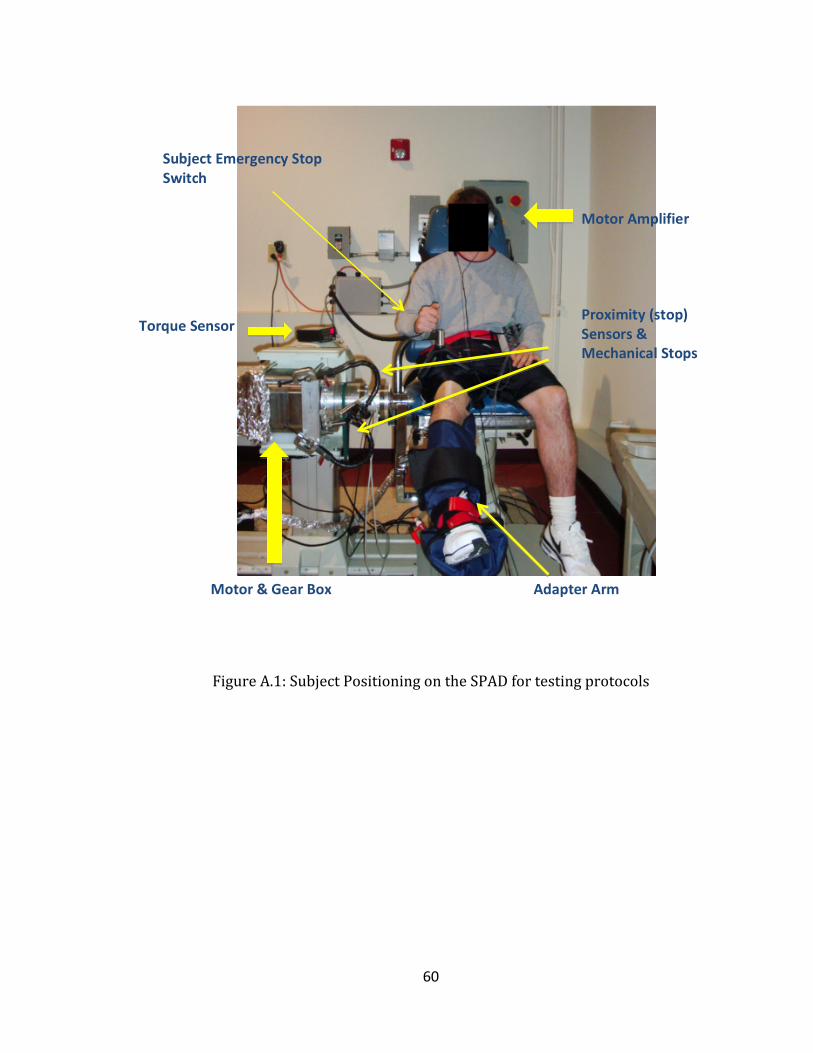
60
Figure A.1: Subject Positioning on the SPAD for testing protocols
Motor Amplifier
Torque Sensor
Motor & Gear Box
Subject Emergency Stop Switch
Proximity (stop) Sensors & Mechanical Stops
Adapter Arm

61
APPENDIX B
PAR-Q Form
1. Has your doctor ever said that you have a heart condition and that you should only do physical activity recommended by a doctor?
________ NO _______ YES 2. Do you frequently feel pain in your chest when you do physical activity? ________ NO ________YES 3. Do you often feel faint or have spells of severe dizziness? ________ NO ________ YES 4. Has a doctor ever said your blood pressure was too high ________ NO ________ YES 5. Has your doctor told you that you have a bone or joint problem such as arthritis
that could be aggravated or made worse by a change in your physical activity? ________ NO ________ YES 6. Do you know of any other reason why you should not do physical activity? ________ NO _________ YES 7. Are you over the age of 65 and not accustomed to vigorous exercise? ________ NO _________ YES If you answer YES to one or more of these questions please answer the following questions: 8. Have you recently consulted your physician about increasing your physical activity
and/or participating in a fitness evaluation? ________ NO _________ YES 9. If you answered “NO” to question 8, will you agree to consult your physician prior
to increasing your physical activity and/or participating in a fitness evaluation? ________ NO _________ YES Signature of PARTICIPANT _____________________ Date ________________ Signature of Investigator __________________________ Date ________________

62
APPENDIX C
Demographic and Health History Questionnaire
Participant ID: ______________ Date: ___________ Gender: M F Cycle: L F N/A Age: _______ Sport: _______ PLEASE ANSWER THE FOLLOWING CONDITIONS TO THE BEST OF YOUR ABILITY. 1. Are you currently unable to participate in lower extremity activities due to injury? NO___ YES___ (if so, explain)_______________________________ 2. Have you injured either knee within the last 6 months? NO___ YES___ (if so, explain)_______________________________ 3. Have you injured either ankle within the last 6 months? NO___ YES___ (if so, explain)_______________________________ 4. If yes to any of the above, please answer: Have you ever seen a doctor for your injury (s)? NO___ YES___ (if so, explain)_______________________________ 5. Do you have any other muscle or skeletal disorders that the researcher should be aware of? NO___ YES___ (if so, explain)_______________________________ 6. Are you presently taking any medications? (including prescribed and over the counter) NO___ YES___ (if so, explain)_______________________________ 7. Have you ever had any type of surgery that may prevent your participation in this study? NO___ YES___ (if so, explain)_______________________________ 8. Do you have any hearing deficits? NO___ YES___ (if so, explain)______________________________ 9. Do you have a history of neurological disorders that may prevent your participation in this study? NO___

63
YES___ (if so, explain)_______________________________ 10. Have you ingested any caffeine in the past 12 hours? NO___ YES___ (if so, explain)_______________________________ 11. Have you taken any over-‐the-‐counter medications in the past 12 hours? NO___ YES___ (if so, explain)_______________________________ 12. FEMALES: Have you had a regular menstrual cycle (lasting 26-‐32 days) during the past 6 months? NO____ YES____ Please indicate any medical and/or health concerns you may have which have not been addressed by the previous items on this form. If there are any questions please feel free to contact one of the investigators at the following: Athena DeAngelis, BS, ATC 541 South College Avenue, University of Delaware Newark, DE, 19716 (856)-‐816-‐7286 -‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐ Signature of participant Date -‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐-‐ Signature of investigator Date

64
APPENDIX D
Quadriceps & Hamstring Stretching Techniques QUADRICEPS:
Stand and touch the wall for support. Bend your heel towards your back and pull your ankle and forefoot to your rear end. Hold for 30 seconds and repeat 3 times.
HAMSTRINGS:
Stand and slightly bend your knees. Bend at the waist and reach towards your toes or floor and hold for 30 seconds. Repeat 3 times.

65
APPENDIX E
IRB Approval Letter
RESEARCH OFFICE 210 Hullihen Hall University of Delaware
Newark, Delaware 19716-1551 Ph: 302/831-2136 Fax: 302/831-2828
DATE: May 6, 2011 TO: Athena DeAngelis FROM: University of Delaware IRB STUDY TITLE: [231022-1] The Effects of an Acoustic Startle and Hormonal Changes on Knee Joint Stiffness SUBMISSION TYPE: New Project ACTION: APPROVED (E. Peloso, W. Farquhar) APPROVAL DATE: May 6, 2011 EXPIRATION DATE: May 5, 2012 REVIEW TYPE: Expedited Review REVIEW CATEGORY: Expedited review category # 4 Thank you for your submission of New Project materials for this research study. The University of Delaware IRB has APPROVED your submission. This approval is based on an appropriate risk/benefit ratio and a study design wherein the risks have been minimized. All research must be conducted in accordance with this approved submission. This submission has received Expedited Review based on the applicable federal regulation. Please remember that informed consent is a process beginning with a description of the study and insurance of participant understanding followed by a signed consent form. Informed consent must continue throughout the study via a dialogue between the researcher and research participant. Federal regulations require each participant receive a copy of the signed consent document. Please note that any revision to previously approved materials must be approved by this office prior to initiation. Please use the appropriate revision forms for this procedure. All SERIOUS and UNEXPECTED adverse events must be reported to this office. Please use the appropriate adverse event forms for this procedure. All sponsor reporting requirements should also be followed. Please report all NON-COMPLIANCE issues or COMPLAINTS regarding this study to this office. Please note that all research records must be retained for a minimum of three years. Based on the risks, this project requires Continuing Review by this office on an annual basis. Please use the appropriate renewal forms for this procedure. If you have any questions, please contact Jody-Lynn Berg at (302) 831-1119 or [email protected]. Please include your study title and reference number in all correspondence with this office.