
INTERACT Webinar Series - … Dietz, RN, MBA, CPHQ Sheila Eckenrode, BSN, MA, CPHQ ... Provide...
37
INTERACT Webinar Series September 30, 2015 with presenters: Carol Dietz, RN, MBA, CPHQ Sheila Eckenrode, BSN, MA, CPHQ Florence Johnson, RN, MSN, MHA Session 8: Change in Condition File Cards and Care Paths
Transcript of INTERACT Webinar Series - … Dietz, RN, MBA, CPHQ Sheila Eckenrode, BSN, MA, CPHQ ... Provide...

INTERACT Webinar Series
September 30, 2015
with presenters:
Carol Dietz, RN, MBA, CPHQ
Sheila Eckenrode, BSN, MA, CPHQ
Florence Johnson, RN, MSN, MHA
Session 8: Change in Condition File
Cards and Care Paths

New England QIN-QIO Care Transitions Teams
2
Connecticut
Florence Johnson
Sheila Eckenrode
Carol Dietz
Rhode Island
Kathleen Calandra
Nelia Odom
New Hampshire
Joyce Johnson
Margaret Crowley
Tim Boyd
Vermont
Liz Klepner
Gail Cogan
Massachusetts
Lynne Chase
Sheryl Leary
Lori Nerbonne
Maine
Maureen Leary

Today’s Session Objectives
3
Welcome nursing homes from the New England region
Understand how to use the INTERACT Change in Condition File
Cards and Care Paths
Develop a plan for implementing the Change in Condition File
Cards and Care Paths on each of your units within your facility
Understand the importance of using the SBAR tool when reporting
a change of condition to the MD/APRN/PA and during an acute
care transfer
15 minute state-specific group discussion

Polling question
My facility has started inputting data into the:
1) Advancing Excellence ‘Safely Reduce Hospitalizations
Tracking Tool’
2) INTERACT Readmission Tracking Tool - using a
computer
3) INTERACT Readmission Tracking Tool - using a paper
tool
4) Our facility is using another readmission tracking tool
5) Our facility has not started tracking readmission data
yet
4

Decision Support Tools
• Acute Change in Condition
File Cards
• Care Paths
• Designed to provide staff with
evidence based best practices
5
Acute Change in Condition File
Cards • Can be used by all nursing home licensed
nursing staff and primary care clinicians
• Provide guidance on when to communicate
acute changes in status to MD, NP, and /or PA
• Recommend placement at nurse’s station or
on med carts for quick reference
• 4" x 6" laminated cards may be put in a flip-
chart or rolodex format for placement by
nursing station phones, or med carts
6

Care Paths
Provide decision trees for
the implementation of
evidence based best practice
Helpful for new graduates,
orientation of new staff and
may be used to support
policy and procedure
7
Nursing Home Studies
with presenters:
Leeanne Shaw-Quinn MSN, GNP-BC
LaShawn Wilcoxson, RN
8
EMPOWERING NURSES TO
“INTERACT”
A fun way to bridge the gap
between theory and practice
Leeanne Shaw-Quinn MSN, GNP-BC

Adult Learning: Critical Theory
• Be in the moment: mindfulness techniques:
deep breaths, Tibetan singing bowls, raising
brain wave vibration.
• Judgment free : clear one’s thoughts to receive
new information
• Appreciate : Diversity : cultural, diverse nursing
experience and training
• Step outside the box: to view situations from a
different perspective

• Change theory: pre contemplation,
contemplation, action, completion, review
• Patricia Benner: novice to expert
• Case studies: adult learning
• Mentorship: group process
Theoretical Constructs

• Present a painting: describe a
painting from the point of view
of nursing
• Share the written point of view
of an artist.
• Discuss: patient observations:
noting change in condition from
baseline. Nursing assessment
skills in a moment in time.
• SBAR: Situation, background,
assessment, recommendation
Describe a Painting
• Groups: provide case study to simulate a
situation for use of the interact/SBAR assessment
tool.
• With use of groups: encourages information
sharing and problem solving.
• Formulation of a 30 second summary of SBAR.
Case Study
• Using a phone in separate room:
nursing groups have a team member
place a call.
• Goal: to simulate calling a provider with
a change of condition. (to describe a
“picture” of patient scenario with use of
the SBAR)
• Provider: placed as the receiver of the
phone call: takes notes and provides
immediate feedback.
• Discussion: mutual support as group.
Role Play

• Being in the moment: to receive new information
• Group process, mentor, critical thinking
• Case study: simulation exercise
• Review, reflect, revise
Conclusion

Caleb Hitchcock Health
Center at Duncaster
LaShawn Wilcoxson, R.N.
Director of Clinical Service, CDP

Why roll out INTERACT at Caleb ?
• Improve communication among multi-disciplinary team
• Identify high-risk residents
• Improve clinical decision making
• Improve resident, staff and physician satisfaction
• Decrease potentially avoidable emergency department evaluations/or hospitalization of Duncaster’ s residents and patients

Implementation Goal
• Duncaster will implement the Interact tools
across the Continuing Care Community
(Independent Living, Assistive Living, and Caleb
Health Center) and decrease readmissions.
– INTERACT training
– Presented to the Board at annual meeting
– Presented to the Health advisory Board at meeting
– Presented to the families and staff
– Presented by A.P.R.N to Licensed staff/ training

INTERACT phases
• Phase one: – Stop and Watch Early Warning Tool
– Care Paths, Acute Change in Condition File Cards
– SBAR forms and Progress Notes
– Hospital Communication Tools
• Phase Two: – Hospital Communication Tools
– Transfer Checklist Envelope
– Transfer Data list and sample forms
• Phase Three: – Medication Reconciliation Work sheet
– Advance Care Planning Tools
Phase one
• Stop and Watch Early Warning Tool
• Care Paths
• Acute Change in Condition file Cards
• SBAR forms and Progress Notes Hospital
Communication Tools

Phase Two
• Hospital Communication Tools
• Transfer Checklist Envelope
• Transfer Data list and sample forms

Phase Three
• Medication
Reconciliation
Worksheet
• Advance Care
Planning Tools

Phase Four
• Quality Improvement
• Hospitalization Rate Tracking Tool
• Quality Improvement Tool for Review of Acute
Care Transfers

Blue box envelope sent to hospital
front back

25

15-Minute Sharing Session – State Specific
Connecticut Nursing Homes who have signed an
INTERACT participation agreement as part of a Community
of Care
– please stay on the line
New Hampshire Nursing Homes:
Tim Boyd ([email protected])
– 1-855-309-6568
– Passcode: 861864
26
Sharing Session
Review issues from last
month’s homework
Discuss successes and
barriers during 15
minute sharing session
Discuss this month’s
homework
27
• Minimum participation viewing the INTERACT webinars:
70% (at least 7 webinars)
and
• Send monthly readmission data to Qualidigm for at least
three months
or
• Enter data into the Advancing Excellence tool: ‘Safely
Reducing Hospitalization Tracking Tool’ and sign the
Data Use Agreement (DUA) document allowing
Qualidigm to access your readmission data for three
months
INTERACT Participation Certification

Readmission Tracking Tool
29
2015 Readmission Rate Collection Tool
Organization: Name of person
completing form
Month
Enter total number of
residents (average daily
census at end of month)
Enter total number of
Hospital Readmissions
within 30 days
Enter total number of
transfers to the ED within
30 days
Enter total number of
transfers to an
Observation bed/unit
within 30 days
Calculated 30-Day
Readmission Rate
January
February
March
April
May
June
July
August
September
October
November
December
Total Annual 0 0 0

Accessing the INTERACT Webinars
after each session
New England QIN-QIO website:
www.healthcarefornewengland.org/
• Click on the ‘Events’ tab
• Scroll down to the ‘Previous Events’ link
• Click on the webinar recording link
• Complete the information before downloading the
webinar presentation
30

Homework from Session #8
During your next team meeting:
• The team will review together the Advanced Planning
tools and Communication Guide
• The team will discuss how and when the staff nurses, social
workers, supervisors and leadership/medical director will
be educated on the use of these tools and will decide
which unit will begin to use these tools
• A timeline will be developed by the team to define when
the education will occur and when the tools will first be
implemented
• The plan will include a debrief by the team and the
participating staff as to how things went after the tools are
used for the first time
31

Group Discussion
Do you have any lessons learned, successes, or
challenges that you want to share as you:
• developed the process for educating your staff on the
INTERACT tools used for Advanced Care Planning?
• talked with your leadership and Medical Director about
tool implementation?
• used the tools for the first time in your facility?
• discussed this initiative with your community?
32

Homework for Session #9
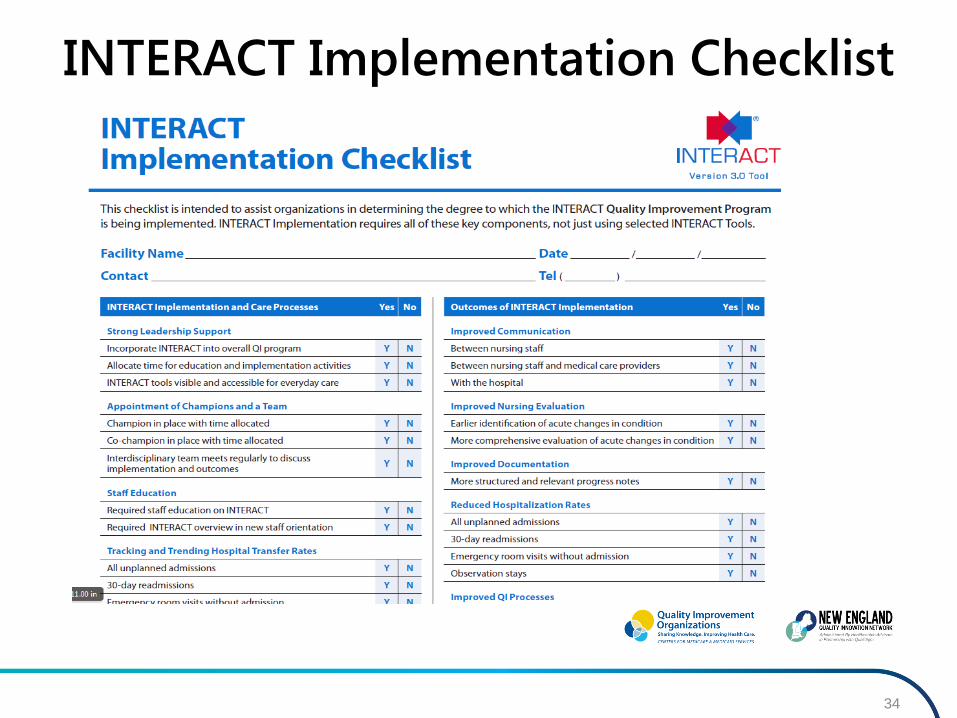
• Review the INTERACT Implementation Checklist
to assist your team in identifying the degree to
which the INTERACT QI Program has been
implemented into your facility
• Implementation requires all of these key
components, not just using selected INTERACT
tools
33
34
INTERACT Implementation Checklist

Homework for Session #9
• If you find a gap in any of the areas on the
Implementation Checklist, conduct a root cause
analysis as to why the implementation of the
tool or process has not taken place
• Be ready to share your finding during the next
webinar on October 28th
35

Questions?
36

Contact Information
Regional INTERACT team contacts:
Florence Johnson, RN, MSN, MHA
Certified INTERACT ® Educator
(860) 613-4187
Sheila Eckenrode, BSN, MA, CPHQ
(860) 613-4197
Carol Dietz, RN, MBA, CPHQ
(860) 632-3737
37
This material was prepared by the New England Quality Innovation Network-Quality Improvement Organization (QIN-QIO), the Medicare Quality
Improvement Organization for New England, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S.
Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. 11SOWQIN_NE-6733-2015029


















