Inter-annual variability of urolithiasis epidemic from semi-arid part of Deccan Volcanic Province,...
14
This article was downloaded by: [University of Tennessee At Martin] On: 01 October 2014, At: 10:07 Publisher: Taylor & Francis Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK International Journal of Environmental Health Research Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/cije20 Inter-annual variability of urolithiasis epidemic from semi-arid part of Deccan Volcanic Province, India: climatic and hydrogeochemical perspectives Sanjay S. Kale a , Vikram Shantaram Ghole a , N.J. Pawar b & Deepak V. Jagtap c a Department of Environmental Sciences, University of Pune, Pune, India. b Department of Geology, University of Pune, Pune, India. c Chaitanya Kidney Stone Treatment and Research Center, Hospital, Saswad, Pune, India. Published online: 22 Jul 2013. To cite this article: Sanjay S. Kale, Vikram Shantaram Ghole, N.J. Pawar & Deepak V. Jagtap (2014) Inter-annual variability of urolithiasis epidemic from semi-arid part of Deccan Volcanic Province, India: climatic and hydrogeochemical perspectives, International Journal of Environmental Health Research, 24:3, 278-289, DOI: 10.1080/09603123.2013.818105 To link to this article: http://dx.doi.org/10.1080/09603123.2013.818105 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content.
Transcript of Inter-annual variability of urolithiasis epidemic from semi-arid part of Deccan Volcanic Province,...

This article was downloaded by: [University of Tennessee At Martin]On: 01 October 2014, At: 10:07Publisher: Taylor & FrancisInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
International Journal of EnvironmentalHealth ResearchPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/cije20
Inter-annual variability of urolithiasisepidemic from semi-arid part of DeccanVolcanic Province, India: climatic andhydrogeochemical perspectivesSanjay S. Kalea, Vikram Shantaram Gholea, N.J. Pawarb & DeepakV. Jagtapc
a Department of Environmental Sciences, University of Pune,Pune, India.b Department of Geology, University of Pune, Pune, India.c Chaitanya Kidney Stone Treatment and Research Center,Hospital, Saswad, Pune, India.Published online: 22 Jul 2013.
To cite this article: Sanjay S. Kale, Vikram Shantaram Ghole, N.J. Pawar & Deepak V. Jagtap (2014)Inter-annual variability of urolithiasis epidemic from semi-arid part of Deccan Volcanic Province,India: climatic and hydrogeochemical perspectives, International Journal of Environmental HealthResearch, 24:3, 278-289, DOI: 10.1080/09603123.2013.818105
To link to this article: http://dx.doi.org/10.1080/09603123.2013.818105
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.

This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Uni
vers
ity o
f T
enne
ssee
At M
artin
] at
10:
07 0
1 O
ctob
er 2
014

Inter-annual variability of urolithiasis epidemic from semi-arid partof Deccan Volcanic Province, India: climatic and hydrogeochemicalperspectives
Sanjay S. Kalea*, Vikram Shantaram Gholea, N.J. Pawarb and Deepak V. Jagtapc
aDepartment of Environmental Sciences, University of Pune, Pune, India; bDepartment ofGeology, University of Pune, Pune, India; cChaitanya Kidney Stone Treatment and ResearchCenter, Hospital, Saswad, Pune, India
(Received 20 January 2013; final version received 3 June 2013)
Semi-arid Karha basin from Deccan Volcanic Province, India was investigated forinter-annual variability of urolithiasis epidemic. The number of reported urolithpatient, weather station data and groundwater quality results was used to assessimpact of geoenvironment on urolithiasis. Data of 7081 urolith patient were pro-cessed for epidemiological study. Gender class, age group, year-wise cases and uro-lith type were studied in epidemiology. Rainfall, temperature, pan evaporation andsunshine hours were used to correlate urolithiasis. Further, average values of ground-water parameters were correlated with the number of urolith episodes. A total of 52urolith samples were collected from hospitals and analysed using FTIR technique toidentify dominant urolith type in study area. Result shows that male population ismore prone, age group of 20–40 is more susceptible and calcium oxalate uroliths aredominant in study area. Year-wise distribution revealed that there is steady increasein urolithiasis with inflation in drought years. In climatic parameters, hot days aresignificantly correlated with urolithiasis. In groundwater quality, EC, Na and F areconvincingly correlated with urolith patients, which concludes the strong relationbetween geo-environment and urolithiasis.
Keywords: urolithiasis; epidemiology; semi-arid; Deccan Volcanic Province;groundwater
Introduction
Urolithiasis commonly known as kidney stone disease is well documented for itsgeographical as well as timescale prevalence (Chandrajith et al. 2006). A majority ofthese areas are observed in most of water-scarce areas all over the world (Pendse &Singh 1986). However, relation between drinking water chemical parameters and occur-rence of urolithiasis outbreaks was ignored at the time of kidney stone medical treat-ment and management. Hence, there is an urgent need of considering its environmentalsupporting factors. In view of this, urolithiasis epidemiology from Karha basin fromDeccan Volcanic Province (DVP), India was investigated for its hydrogeochemical andclimatic perspectives.
*Corresponding author. Email: [email protected]
International Journal of Environmental Health Research, 2014Vol. 24, No. 3, 278–289, http://dx.doi.org/10.1080/09603123.2013.818105
� 2013 Taylor & Francis
Dow
nloa
ded
by [
Uni
vers
ity o
f T
enne
ssee
At M
artin
] at
10:
07 0
1 O
ctob
er 2
014

About 5–10% human population can be targeted all over world by this diseasealong their total lifetime (Coe et al. 2005). However, the area-specific prevalence andepidemics of kidney stone are very uncommon in all parts of the world and reported asa “Kidney stone belt” (Sierakowski et al. 1979). Well-identified kidney stone prevalenceareas all over the world like the USA, the UK, Argentina, Africa, Kuwait, Iraq, SriLanka and India (some part of Rajasthan, Gujarat and Maharashtra as well as somehilly regions from north India) (Rose & Westbury 1975; Sierakowski et al. 1979;Mbonu et al. 1984; Pendse & Singh 1986; El-Reshaid et al. 1997; Ali & Rifat 2005;Deshmukh & Khan 2006; Pinduli et al. 2006) have been observed in this study.
The same analogy was used here for exploring the possibility of climatic factorssuch as rainfall, daily temperature and groundwater-level fluctuations as one of thecausative factor for kidney stone problem in that area by conducting local hospital-levelsurveys and studying environmental conditions. The objective of the present study wasthreefold: (1) to classify the reported urolith patients as age, gender, year-wise and dom-inant urolith type to understand magnitude of epidemics; (2) to study the correlation ofurolithiasis with climatic conditions like rainfall, number of hot days, annual sunshinehours and annual pan evaporation; (3) to understand the correlation between urolithiasisand groundwater quality.
Study area
The area under investigation was the Karha river basin (Figure 1) having a geographicalarea about 1333 km2, from semi-arid region of DVP, India. The Karha basin is boundby longitudes 73° 52′ 07″W to 74° 41′ 01″E and longitudes 18° 3′ 41″ S to 18° 26′ 31″N.The major settlements of study area are Saswad and Baramati (Figure 1).
Climatically, it is present in semi-arid and rain-fed region of Maharashtra. Geologi-cally, it is the situated central part of DVP of Indian Peninsula (Figure 2). Dug wellsare the principle source of water supply for drinking and other purposes in the studyarea. Groundwater withdrawal is confined to vesicular, weathered, jointed and fracturedupper basaltic crust, which is overlain by thin soil cover. Depleting groundwater levelsare common, the condition being further aggravated by frequent drought-like situations.
The total population of study area is 149,449 individuals and male to female ratio isapproximately 1:1 from Government of India Census 2011. Totally, 94 villages are pres-ent in Karha basin. The major crop production is millet, which is a major part of dietamongst people with vegetables, cereals and pulses.
Materials and methods
In present study, patient data of 7081 urolith patients reported from year 1994 to 2008(15 years) were procured from hospitals and clinics located at Saswad and Baramatitowns. It was processed for gender and age group classification. To find out thedominant urolith type from the study area, a total of 52 urolith samples were collectedand analysed by FTIR technique for their chemical composition.
Surface weather station data (Table 1) for Pune station were procured from the IndiaMeteorological Department (IMD), Regional office, Pune to correlate with the yearlykidney stone patient data from study area. The major climate parameters like annualrainfall, yearly total pan evaporation, daily temperature data and number of hot days ina year were used to identify the role of climatic factors in urolith formation. Beforecorrelate, the procured data were processed for thier annual average values. The number
International Journal of Environmental Health Research 279
Dow
nloa
ded
by [
Uni
vers
ity o
f T
enne
ssee
At M
artin
] at
10:
07 0
1 O
ctob
er 2
014

of summer hot days was calculated to their Tmax 97.5P percentile for 40.6 °C (Gadgil& Dhorade 2005).
The groundwater-level fluctuation and chemical analysis data of groundwatersamples from study area were obtained from Groundwater Survey and DevelopmentAuthority (GSDA), Pune (Table 2). These data were used to correlate with kidney stonepatient data. In study area, a total of 14 observatory dug wells were previously selectedby GSDA for continuous monitoring. The data were compared with groundwater qual-ity data from DVP carried out by other workers (Pawar et al. 2008; Naik et al. 2009).The data of groundwater parameter such as pH, EC, Ca, Mg, Na, K, HCO3, Cl, SO4,NO3 and F were used for correlation between urolithiasis and groundwater, which wasthe only available source for drinking water to people residing from study area.
Figure 1. Location map of the study area (After Pawar & Kale, 2006).
280 S.S. Kale et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
enne
ssee
At M
artin
] at
10:
07 0
1 O
ctob
er 2
014

Results and discussion
The results are given in urolithiasis epidemiology, the relationship between urolithiasisand climate, and the relationship between urolithiasis and groundwater quality. Theweather station data corresponding to Karha river basin are given in Table 1 and aver-age groundwater quality data are given in Table 2.
Table 1. Urolith patient incidence and rate per 10,000 population form Karha basin.
Year Number of urolith incidence Rate of urolith incidence per 10,000 individuals
1994 41 31995 111 71996 128 91997 84 61998 94 61999 62 42000 212 142001 351 232002 659 442003 450 302004 290 192005 375 252006 763 512007 2072 1392008 1389 93
(Total) 7081 (15 year average rate) 32
Note: Population of study area is 149,449.Source: Census of India 2001.
Figure 2. Location of Karha basin in DVP.
International Journal of Environmental Health Research 281
Dow
nloa
ded
by [
Uni
vers
ity o
f T
enne
ssee
At M
artin
] at
10:
07 0
1 O
ctob
er 2
014
Epidemiology of urolithiasis from Karha basin
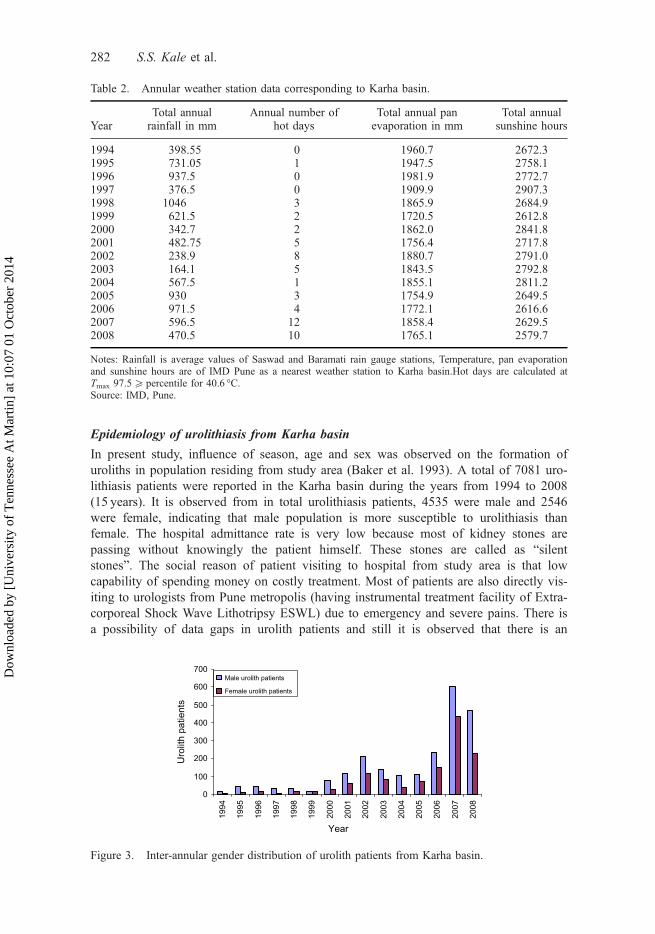
In present study, influence of season, age and sex was observed on the formation ofuroliths in population residing from study area (Baker et al. 1993). A total of 7081 uro-lithiasis patients were reported in the Karha basin during the years from 1994 to 2008(15 years). It is observed from in total urolithiasis patients, 4535 were male and 2546were female, indicating that male population is more susceptible to urolithiasis thanfemale. The hospital admittance rate is very low because most of kidney stones arepassing without knowingly the patient himself. These stones are called as “silentstones”. The social reason of patient visiting to hospital from study area is that lowcapability of spending money on costly treatment. Most of patients are also directly vis-iting to urologists from Pune metropolis (having instrumental treatment facility of Extra-corporeal Shock Wave Lithotripsy ESWL) due to emergency and severe pains. There isa possibility of data gaps in urolith patients and still it is observed that there is an
Table 2. Annular weather station data corresponding to Karha basin.
YearTotal annualrainfall in mm
Annual number ofhot days
Total annual panevaporation in mm
Total annualsunshine hours
1994 398.55 0 1960.7 2672.31995 731.05 1 1947.5 2758.11996 937.5 0 1981.9 2772.71997 376.5 0 1909.9 2907.31998 1046 3 1865.9 2684.91999 621.5 2 1720.5 2612.82000 342.7 2 1862.0 2841.82001 482.75 5 1756.4 2717.82002 238.9 8 1880.7 2791.02003 164.1 5 1843.5 2792.82004 567.5 1 1855.1 2811.22005 930 3 1754.9 2649.52006 971.5 4 1772.1 2616.62007 596.5 12 1858.4 2629.52008 470.5 10 1765.1 2579.7
Notes: Rainfall is average values of Saswad and Baramati rain gauge stations, Temperature, pan evaporationand sunshine hours are of IMD Pune as a nearest weather station to Karha basin.Hot days are calculated atTmax 97.5P percentile for 40.6 °C.Source: IMD, Pune.
0
100
200
300
400
500
600
700
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
Year
Uro
lith
patie
nts
Male urolith patients
Female urolith patients
Figure 3. Inter-annular gender distribution of urolith patients from Karha basin.
282 S.S. Kale et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
enne
ssee
At M
artin
] at
10:
07 0
1 O
ctob
er 2
014

increase in hospital admittance (Figure 3). The available urolith patient data were pro-cessed for the rate of urolith patients per 10,000 individuals from study area (Table 1).This explains how climate can have a detectable effect on the incidence of stone diseasein consideration that in this population, the effect of diet on the risk of stone formationis minimal or event absent.
Further, gender-wise distribution of urolith patients remains equivalent during theyears from 1994 to 2008 whether their numbers are increasing every year (Figure 3). InFigure 3, three distinct inflation loops are observed during the years 1994–1999 (nourolithiasis prevalence years), 2000–2004 (starting of urolithiasis prevalence) and 2005–2008 (dominance of urolithiasis). The emergence of urolithiasis prevalence in thepopulation of study area was observed during the years 2000–2004, which are severelydrought years experienced in study area. As the result of this, groundwater depletedseverely promoting the groundwater mineralization and exceeding its ionic concentrationdue to evaporation dominance (Table 3) (Pawar 1993). However, population in Karhabasin have no other alternative to drinking water and, unknowingly, continue to use thishighly mineralized groundwater for drinking and cooking purposes. In year 2005, amplerainfall is observed to recharge the previously depleted groundwater level. Due to this,considerable recharge of groundwater was observed in aquifers of Karha basin (Tables 2and 3). During high rainfall years, instead of diluting recharged water, groundwater getsconsiderably mineralized due to the dissolution of secondary carbonates previouslyprecipitated in drought years (Tables 2 and 3) (Pawar et al. 2008).
For urolithiasis, more prone age group is 21–40 years, after that the risk of urolithia-sis decreases in age groups 41–60, 0–20 and >60 having comparably less risk of uro-lithiasis in Karha basin. It is interesting to note that age group of 21–40 has highervulnerability to kidney stone as anatomical disorder as it is younger group. This group
Table 3. Annual averages of groundwater quality parameters from Karha basin during the period1994–2008 (15 years).
Year WL EC Ca Mg Na K HCO3 Cl SO4 NO3 F
1994 7.6 592.5 16.4 42.8 17.9 0.2 72.8 77.5 16.7 22.8 0.41995 7.5 676.9 54.1 38.6 22.1 0.2 124.6 170 47 13.4 1.11996 7.9 706.9 47.8 40.8 23 0.3 135.2 180 93.5 20.8 1.11997 7.5 745 25.3 25.9 22.8 0.4 130 115 37.7 23 0.51998 8.3 690 19.1 19.3 23.9 0.3 109 81.8 33 24.5 0.41999 8.1 687.5 22.8 22.9 28.9 0.7 101.5 84.3 31 26 0.52000 8.9 952.3 66.2 36.7 51.8 0.5 140.7 159.8 50.4 1.5 0.72001 11.1 1086.8 60 26.9 122.3 1 206.7 203.4 125.4 2.3 0.82002 12 1375.3 100.2 97.7 398.3 1.6 148.6 531.1 450.3 11.1 1.12003 17 1203.8 117.4 75.7 200 5.6 130.3 400.1 254.9 10.1 0.92004 18 999.7 104 50.2 173.7 6.4 99.5 272.5 94 3.2 0.82005 11.8 1112.2 55.8 29.9 103.2 6.6 162 158.9 96.6 16.8 1.32006 8.4 1797.3 44.1 58.8 202.8 7.8 328 226 131.8 18.8 1.52007 9.6 2015.9 76.3 60.2 323 5.2 202 284.7 349.4 26.1 2.92008 10.1 1283 56.6 42.8 231.8 3.9 170 217.5 219 20.6 2.3Min 7.5 592.5 16.4 19.3 17.9 0.2 72.8 77.5 16.7 1.5 0.4Max 18 2015.9 117.4 97.7 398.3 7.8 328 531.1 450.3 26.1 2.9Avg 10.25 1061.67 57.74 44.61 129.70 2.71 150.73 210.84 135.38 16.07 1.09SD 3.31 423.48 31.28 21.34 121.66 2.84 61.19 124.07 128.56 8.66 0.70
Note: All parameters are in mg/L except WL is groundwater level in metres and EC is measured in μS/cm.Source: GSDA data.
International Journal of Environmental Health Research 283
Dow
nloa
ded
by [
Uni
vers
ity o
f T
enne
ssee
At M
artin
] at
10:
07 0
1 O
ctob
er 2
014

is also known as productive age group and performs most of the laborious work in theirdaily livelihood. Hence, the rate of dehydration is higher in this age group. This givesmore opportunity to explore the climatic and hydrogeochemical reasons if any in thepopulation of study area. It was observed during present study that other epidemiologi-cal factors are remained stable along 15-year period of the study. This is due toagricultural lifestyle of population having less possibility to sudden change in diet andworking profession. About 90% of population are residing in rural environment and,totally or partially, are dependent on agriculture as a prime source of income.
After analysis of 52 urolith samples on FTIR, it was revealed that the majority ofurolith is of calcium oxalate type and varying composition of calcium oxalate monohy-drate and calcium oxalate dihydrate. However, 14 out of 52 show uric acid content inurolith matrix. Many uroliths are smaller in size ranging from 2 to 10mm except fewhaving size more than 10mm. It is observed that calcium oxalate monohydratecomposition is more in urolith matrix. Various six types of FTIR spectra were observedin collected urolith samples, within that most of uroliths have higher concentration ofcalcium oxalate monohydrates than calcium oxalate dihydrate from study area. Morethe calcium oxalate monohydrate, more the hardness of urolith as is observed byCosta-Bauza et al. (2007).
Relation between urolithiasis and climate from Karha basin
The poor correlation was observed between rainfall and urolithiasis; however, lowamount of rainfall introduces high groundwater mineralization and increases droughtcondition in study area. In an absence of sufficient rainfall, groundwater levels getdepleted and accumulation of excess salts in groundwater from aquifer material varies.Since the study area shown (Table 2) has constantly decreasing trends in the totalannual rainfall since 1997 up to 2002, it results in increased groundwater-level deple-tion. This increases its residence time and drought conditions accelerate evaporation,which result in exceeded groundwater mineralization (Pawar 1993). People from studyarea have to depend on such water for drinking purposes. Consumption of high saltcontaining groundwater may disturb the physiology and mineral balance of human bodyand may be one of the causative factors for urolithiasis.
A plot of number of hot days verses urolith patients positive correlation is made inFigure 4. Generally, 1–3 hot days are experienced in study area per year but in droughtconditions the number exceeds up to more than four, which may be critical factor fortriggering kidney stone formation in mass population. When heat stroke occurs at thattime, the body is unable to regulate its own temperature. The body’s temperature risesrapidly, the sweating mechanism fails, and the body is unable to cool down (Loughnanet al. 2010). Urinary tract stones in the regular season in summer heat caused renalcolic because of hot weather, which leads to substantial increase in human perspiration,resulting in severe loss of body water and reduction in the urine volume (Chandrajithet al. 2006). Therefore, the case of original stone patients or potential patients withinduced renal colic stone is the result of concentrated urine (Hassan et al. 2001).
The annual evaporation data and the total annual pan evaporation do not showany correlation with the annual number of kidney stone patients reported during thestudy period 1994–2008. This factor was considered with the understanding of thefact that high evaporation may exhaust some portion of water content in the form ofperspiration from human body. The same observation was reported for annual sun-shine hours.
284 S.S. Kale et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
enne
ssee
At M
artin
] at
10:
07 0
1 O
ctob
er 2
014

Relation between urolithiasis and inter-annular groundwater quality
The average pH varies from 8.33 to 7.62 annually, showing that alkaline pH is the typi-cal characteristics of basaltic aquifers of DVP (Pawar 1993). The pH data are not corre-lating with annual urolith patients observed in Karha basin. Correlation of groundwaterquality parameter from Karha basin was made with number of urolith patients to under-stand the effect of geo-environmental condition on urolithiasis. In the present study, theplot of average annual electrical conductivity (EC) of groundwater verses number ofurolith patients significant correlation (R2 = 0.7588) (Figure 5(a)) was observed. SinceEC has shown affirmative correlation with a number of urolithiasis species, the authorthought that it would be more logical to correlate different ionic species separately toget an idea about any specific elements responsible for the development of kidneystone. Within that Ca, Mg, K, HCO3, Cl, SO4 and NO3 are not showing any correlationwith the number of urolith patients observed in the study area. However, Na (Figure 5(b)) and F (Figure 5(c)) are positively correlated with the number of urolith patientsobserved in the study area. It is difficult to explain such correlations in consideration ofa small range of variation of sodium and fluoride intake by water.
Further, a plot of Na verses number of urolithiasis cases (Figure 5(b)) shows posi-tive correlation. Though it is known that soft water contains higher concentration ofsodium while hard water contains higher concentration of calcium and magnesium,some recent studies reported that using sodium salts in diet is one of the risk factors ofurolithiasis (Massey 2005). The consumption of sodium in diet may enhance the cal-cium absorption in blood (Trinchieri et al. 2006). This may exert more pressure on renalsystem to eliminate the extra calcium from blood which creates favourable conditionsfor calcium to precipitate in the form of urolithiasis (Trinchieri et al. 2006). Thus, therole of Na is an equally important factor as evidenced from correlation studies. Thebody requires only 500mg of sodium each day. WHO recommends no more sodiumthan 2400mg per day; however, most people take more than the recommended amount.Consumption of 2.5 l of water may exceed the sodium concentration more than 500mg,increasing a load on the renal system.
However, in the case of F ion, there is a significant positive correlation with urolith-iasis (Figure 5(c)). Further, it is interesting to note that fluoride is found in trace amountin the urolith composition (Sai Sathish et al. 2008; Kale et al. 2011). Within 15 years of
R2 = 0.8322
0
500
1000
1500
2000
2500
0 2 4 6 8 10 12 14
Number of hot days in a year
No.
of u
rolit
h pa
tient
s re
porte
d
Figure 4. Relation between a number of annual urolith patient data and a number of hot days ina year.
International Journal of Environmental Health Research 285
Dow
nloa
ded
by [
Uni
vers
ity o
f T
enne
ssee
At M
artin
] at
10:
07 0
1 O
ctob
er 2
014

groundwater data, fluoride concentration is exceeded seven time of WHO (2002) per-missible limit of fluoride. It is to be noted here that from north India, the relationshipbetween fluoride concentration in drinking water and urolith prevalence in local popula-tion is reported by Singh et al. (2001). The positive correlation of F with the number ofpatients in the present study thus authenticates this finding. The fluoride is the mostreactive anionic species and it actively takes part in many human physiological pro-cesses. At higher level concentration, sometimes it destroys the cell from various tissuesof internal organs. This gives substantial pressure on renal system to filter out proteinmaterial of dead cell matter and possibly become nucleus in process of urolith forma-tion (Rotily et al. 2000). The increasing fluoride in groundwater is observed in studyarea as insufficient water was available for flushing of accumulated fluoride ions in sub-surface environment. Consecutive drought years aggravate the conditions.
R2 = 0.7588
0
200
400
600
800
1000
1200
0.0 500.0 1000.0 1500.0 2000.0 2500.0
Annual average of groundwater Electrical Conductivity (EC)in µS/cm
Ann
ual u
rolit
h pa
tient
R2 = 0.6159
0
200
400
600
800
1000
1200
1400
0.0 100.0 200.0 300.0 400.0 500.0Annual average of sodium concentration of groundwater in
mg/L
Ann
ual u
rolit
h pa
tient
R2 = 0.86
0
200
400
600
800
1000
1200
1400
0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5
Annual average of fluoride in groundwater (mg/L)
Ann
ual u
rolit
h pa
tient
(a)
(b)
(c)
Figure 5. Relation between urolithiasis, and (a) electrical conductivity, (b) sodium and (c)fluoride.
286 S.S. Kale et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
enne
ssee
At M
artin
] at
10:
07 0
1 O
ctob
er 2
014

In the present study, the geoenvironmental and climatic factors have been found tobe one of the important factors in the development of urolithiasis. Urinary tract stonesin the regular season, especially in summer heat caused renal colic because of hotweather, which leads to substantial increase in human perspiration, resulting in severeloss of body water and reduction in the urine volume (Chandrajith et al. 2006).
• Frequent droughts in the area which is inseparable part of semi-arid region ofDVP.
• Erratic nature of rainfall and poor leaching of salts that have affected both quan-tity and quality of groundwater resources.
• Since is no alternative to the use poor quality groundwater resources for drinkingpurpose, the people are dependent on it.
• Depletion in the groundwater level is also associated with mineralized groundwa-ter from deeper aquifers.
• Downstream part of the basin is more prone to urolithiasis as compared toupstream part.
• Increase in the groundwater salinity associated with increase in Na, Cl, SO4, Fand NO3 is collectively correlating in the form of EC with the number of urolith-iasis cases.
• Increase in the annual number of hot days from last decade is also one of the rea-sons to provoke urolithiasis in the study area.
Remedial measures
Considering all above facts regarding Karha basin, precautionary measures should beadopted to avoid the urolithiasis in semi-arid regions of DVP. The extra intake of min-eralized salts of groundwater should be avoided. Within that bore-well water should berestricted to drinking purpose; otherwise, appropriate treatments should be used toreduce the dissolved ionic constituents. For this primary treatment like filtration,adsorption, coagulation, ion exchange and reverse osmosis are found to be effective.
Harnessing the running monsoonal water with the help of sustainable watershedmanagement practices in the basin may found beneficial for the natural recharge of shal-low basaltic aquifers of Karha basin.
Artificial recharge of aquifers from rainwater is proved to be beneficial for flushingof precipitated salts form aquifers. This may reduce the dissolved salts in subsurfaceaqueous environment.
Three earthen-pot techniques, which definitely reduce considerable amount of dis-solved salts, have to be adopted for treating drinking water at household level effec-tively due to their low cost and easy operation.
Conclusions
Out of various causative factors of urolithiasis, environmental factors also have theirown contribution in the formation of uroliths in the population residing from semi-aridareas. The sudden change in climatic parameters (where they live) as well as groundwa-ter quality (which they drink) observe the urolithiasis occurrence in Karha basin, DVPof India.
International Journal of Environmental Health Research 287
Dow
nloa
ded
by [
Uni
vers
ity o
f T
enne
ssee
At M
artin
] at
10:
07 0
1 O
ctob
er 2
014

Year-wise distribution of urolith patient data shows steady increase and starts infla-tion from drought condition. The average annual urolith incident rate is 35 urolithpatients per 10,000 individuals in the study area. In epidemiological study, malepopulation is more prone than female, age group of 20–40 is more susceptible and cal-cium oxalate uroliths are dominant. The majority of uroliths are having maximum con-tribution of calcium oxalate monohydrate in their matrix, indicating that very harduroliths are present in the patients from study area.
In climatic factors, the number of hot days in a year is positively correlated withthe number of urolith patients. It enhances the dehydration phenomenon, which is moresusceptible for urolith formation. In drought period, groundwater level was criticallydeclined and also influences the groundwater quality by more natural solute accumula-tion in partially filled aquifers from study area.
However, groundwater quality parameters were correlated with a number of urolithpatients observed in the same period. Out of all groundwater parameters, EC, Na and Fare convincingly correlated with urolith patients. These parameters are associated withgroundwater salinity induced by semi-arid and drought conditions, indicating their asso-ciation with urolith formation from study area. People are using such highly mineralizedgroundwater for drinking purposes. Consumption of high salt containing groundwatermay disturb the physiology and mineral balance of human body and may be one of thecausative factors for urolithiasis.
The suitable remedial measures are suggested to combat environmentally inducedurolithiasis epidemics in semi-arid Karha basin. In conclusion, the present studyrevealed that there is strong relation between geo-environment and outbreaks of urolith-iasis in the semi-arid Karha basin.
ReferencesAli SH, Rifat UN. 2005. Etiological and clinical patterns of childhood urolithiasis in Iraq. Pediatr
Nephrol. 20:1453–1457.Baker PW, Coyle P, Bais R, Rofe AM. 1993. Influence of season, age and sex on the renal stone
formation in south Australia. Med J Aust. 159:390–392.Chandrajith R, Wijewardana G, Dissanayake CB, Abeygunasekara A. 2006. Biominerology of
human urinary calculi (kidney stones) from some geographic regions of Sri Lanka. EnvironGeochem Health. 28:393–399.
Coe FL, Evan A, Worcester E. 2005. Kidney stone disease. J Clin Investig. 115:2598–2608.Costa-Bauza A, Ramis M, Montesinos V, Conte A, Piza P, Pieras E, Grases F. 2007. Type of
renal calculi: variation with age and sex. World J Urol. 25:415–421.Deshmukh S, Khan ZH. 2006. Evaluation of urinary abnormalities in nephrolithiasis patients from
Marathwada region. Indian J Clin Biochem. 21:177–180.El-Reshaid K, Mughal H, Kapoor M. 1997. Epidemiological profile, mineral metabolic pattern
and crystallographic analysis of urolithiasis in Kuwait. Eur J Epidemiol. 13:229–234.Gadgil A, Dhorade A. 2005. Temperature trends in twentieth century at Pune, India. Atmos
Environ. 39:6550–6556.Hassan I, Juncos LA, Milliner DS, Sarmiento JM, Sarr MG. 2001. Chronic renal failure second-
ary to oxalate nephropathy: a preventable complication after jejunoileal bypass. Mayo ClinProc. 76:758–760.
Kale SS, Pawar NJ, Wagholikar DS, Achyuthan H. 2011. Microstructure and growth band studiesof uroliths using optical and scanning electron microscopy. Curr Sci. 100:225–229.
Loughnan ME, Nicholls N, Tapper NJ. 2010. The effects of summer temperature, age and socio-economic circumstance on Acute Myocardial Infarction admissions in Melbourne, Australia.Int J Health Geogr. 9:41–51.
Massey LK. 2005. Effect of dietary salt intake on circadian calcium metabolism, bone turnoverand calcium oxalate kidney stone risk in post menopausal women. Nutr Res. 25:891–903.
288 S.S. Kale et al.
Dow
nloa
ded
by [
Uni
vers
ity o
f T
enne
ssee
At M
artin
] at
10:
07 0
1 O
ctob
er 2
014

Mbonu O, Attah, Attah I. 1984. Urolithiasis in an African Population. Int Urol Nephrol. 16:291–296.
Naik PK, Awasthi AK, Anand AVSS, Behera PN. 2009. Hydrogeochemistry of Koyana riverbasin, India. Environ Earth Sci. 59:613–629.
Pawar NJ. 1993. Geochemistry of carbonate precipitation from the groundwaters in basalticaquifers: an equilibrium thermodynamic approach. J Geol Soc India. 41:119–131.
Pawar NJ, Pawar JB, Kumar S, Supekar A. 2008. Geochemical eccentricity of ground water alliedto weathering of basalt from the Deccan Volcanic Province, India: insinuation on CO2
consumption. Aquat Geochem. 14:41–71.Pawar NJ, Kale VS. 2006. Waterfall tufa deposits from the Deccan Basalt Province, India: impli-
cations for weathering of basalts in the semi-arid tropics. Z Geomorph NF. 145:17–36.Pendse AK, Singh PP. 1986. The etiology of urolithiasis in Udaipur (western part of India). Urol
Res. 14:59–62.Pinduli I, Spivacow R, Valle E, Vidal S, Negri AL, Previgliano H, Farias RE, Andrade JH, Negri
GM, Boffi-Boggero HJ. 2006. Prevalence of urolithiasis in the autonomous city of BuenosAires, Argentina. Urol Res. 34:8–11.
Rose A, Westbury EJ. 1975. Influence of calcium content of water, intake of vegetables and fruitsand of other food factors upon the incidences of renal calculi. Urol Res. 3:61–66.
Rotily M, Leonetti F, Iovonna C, Berthezene P, Dupuy P, Vazi A, Berland Y. 2000. Effects oflow animal protein or high-fiber diets on urine composition in calcium nephrolithiasis. KidInt. 57:1115–1123.
Sai Sathish R, Ranjit B, Ganesh KM, Rao GN, Janardhana C. 2008. A quantitative study on thechemical composition of renal stones and their fluoride content from Anantapur District,Andhra Pradesh, India. Curr Sci. 94:104–109.
Sierakowski R, Finlayson B, Landes R. 1979. Stone incidences as related to water hardness indifferent geological regions of the United States. Urol Res. 7:157–160.
Singh PP, Barjatiya MK, Dhing S. 2001. Evidence suggesting that high intake of fluorideprovokes the nephrolithiasis in tribal population. Urol Res. 29:238–244.
Trinchieri A. 2006. The epidemiological trends in urolithiasis: impact on health care system. UrolRes. 34:151–156.
[WHO] World Health Organization. 2002. Guideline for drinking water quality. 2nd ed. Geneva:World Health Organization.Health criteria and other supporting information; p. 940–949.
International Journal of Environmental Health Research 289
Dow
nloa
ded
by [
Uni
vers
ity o
f T
enne
ssee
At M
artin
] at
10:
07 0
1 O
ctob
er 2
014