INTENSIVE CARE MEDICINE - egyfellow.mohealth.gov.eg · Intensive Care Medicine Egyptian Fellowship...
62
INTENSIVE CARE MEDICINE Egyptian Fellowship
Transcript of INTENSIVE CARE MEDICINE - egyfellow.mohealth.gov.eg · Intensive Care Medicine Egyptian Fellowship...
INTENSIVE CARE
MEDICINE
Egyptian Fellowship

Intensive Care Medicine Egyptian Fellowship
2
Intensive Care Medicine Egyptian Fellowship
3
Table of Contents Introduction; ..................................................................................................................................... 5
Structure of the training program for the ......................................................................................... 7
Egyptian Fellowship of Intensive care medicine ............................................................................. 7
First two years of training (Y1& Y2) ........................................................................................... 8
Third year of training (Y3, ICT1) ................................................................................................ 8
Fourth and fifth year of training ................................................................................................... 8
(Y4, ICT2 and Y5, ICT3) ............................................................................................................. 8
Regulations of the training program for the ..................................................................................... 9
Egyptian Fellowship of Intensive Care ............................................................................................ 9
Program Intended Learning Outcomes .......................................................................................... 13
Knowledge & Understanding ......................................................................................................... 13
Intensive care procedures ............................................................................................................... 18
Y1 & Y2 ......................................................................................................................................... 20
1-General Medicine (GM) (Internal medicine) .......................................................................... 20
2-Basic sciences ......................................................................................................................... 26
Y3 (ICM1)...................................................................................................................................... 30
1- Basic intensive care medicine ................................................................................................ 30
2-Adult Intensive care medicine ................................................................................................ 40
Y4 &Y5 (ICM3&ICM4) ................................................................................................................ 51
1- Pediatric intensive care medicine .......................................................................................... 51
2-Trauma and burns ................................................................................................................... 53
3- Surgical post operative intensive care ................................................................................... 57
4-Medical intensive care ............................................................................................................ 60
5- Toxicology ............................................................................................................................. 63
Methods of assessments ................................................................................................................. 64
1-Regulations ............................................................................................................................. 64
2-Structure of the examination 64

Intensive Care Medicine Egyptian Fellowship
4

Intensive Care Medicine Egyptian Fellowship
5
Introduction The goal of the Fellowship in intensive care medicine ICM is to provide trainees with background
knowledge necessary for the care of critically ill patients and an appreciation of management
issues unique to this patient population.
Intensive care medicine is a multidisciplinary field concerned with patients who have sustained, or
are at risk of sustaining, life threatening, single or multiple organ system failure due to disease or
injury. Intensive care medicine seeks to provide for the needs of these patients through immediate
and continuous observation and intervention so as to restore health and prevent complications.
A Fellow will become competent in all aspects of recognizing and managing acutely ill adult
patients with single or multiple organ system failure requiring ongoing monitoring and support.
Dedicated faculty provides a comprehensive, state of the art approach to patient care in a complex
environment. The breadth of clinical experiences in this multidisciplinary fellow training program
provides equal learning opportunities for critical care fellows.
The educational program for this fellowship will include lectures, clinical cases, procedures,
skills, and other scientific activities

Intensive Care Medicine Egyptian Fellowship
6
Intensive Care Medicine Egyptian Fellowship
7
Structure of the training program for the
Egyptian Fellowship of Intensive care medicine The Egyptian Fellowship Board is a 5 years supervised on job training program that includes 2
year of structured general medicine training, followed by 3 years of Intensive Care Training (ICT).
Both general medicine and ICT must be conducted in accredited hospitals before sitting for the
final examination. A list of hospitals will be accredited yearly by the scientific council.
FIRST TWO YEARS OF TRAINING (Y1& Y2)
The trainees will spend these two years in a rotation program as it appears below in the table to
cover all the related subspecialties. These 2 years should be spent in certain accredited hospitals
After spending 18 months of these two years of training, the trainees are legible to site for the 1st
part exam of the Egyptian Fellowship of Intensive Care Medicine.
Important Notice: Trainees must pass successfully all the foundation courses (evidence based
medicine, communication skills, research methodology and medical ethics) before being
promoted to Y3 (CCT1) of their training. Full information about foundation courses is
available at the Egyptian Fellowship website and administration office.
THIRD YEAR OF TRAINING (Y3, ICT1)
The trainees will spend this year in Intensive Care practice basics in accredited training hospitals.
FOURTH AND FIFTH YEAR OF TRAINING (Y4, ICT2 AND Y5, ICT3)
The trainees will spend these two years in accredited hospitals where they will have rotations in
coronary care units, neurology ICU units, cardiothoracic surgical ICU units, nephrology dialysis
units, liver transplantation and renal transplantation units , Pulmonology units, neurosurgery post
operative care units, general postoperative care units, pediatric ICU, and intensive care units as it
appears in the table below
By the end of the 5th year, trainees will be legible to site for the 2nd part and 3rd part exams of the
Egyptian Fellowship of Intensive Care.
The following table illustrates the job rotational plan for the Intensive Care Fellowship over the
five year training program;
Internal medicine Y1& Y2 Training duration
Months
Diabetes & metabolism
Endocrinal
Rheumatology
3
Year Training
Y1& Y2 (GM) General Medicine
Y3 (ICT1) Intensive Care Training 1
Y4 (ICT2) Intensive Care Training 2
Y5 (ICT3) Intensive Care Training 3
Intensive Care Medicine Egyptian Fellowship
8
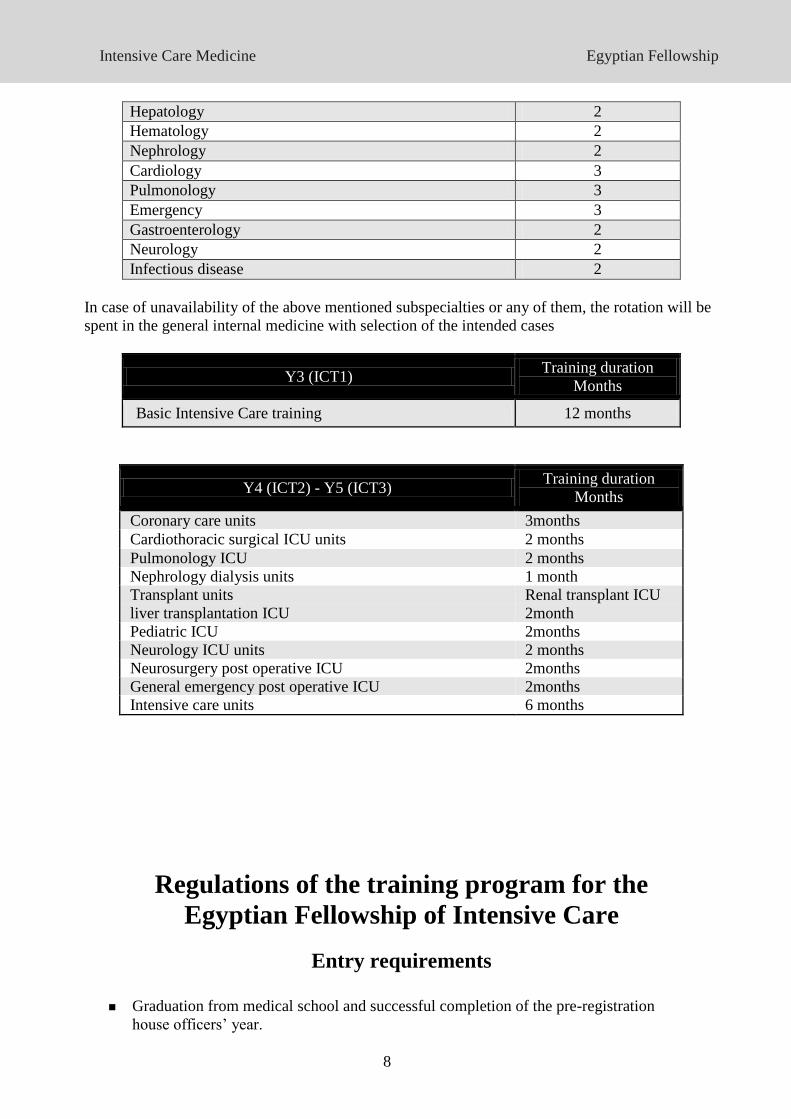
Hepatology 2
Hematology 2
Nephrology 2
Cardiology 3
Pulmonology 3
Emergency 3
Gastroenterology 2
Neurology 2
Infectious disease 2
In case of unavailability of the above mentioned subspecialties or any of them, the rotation will be
spent in the general internal medicine with selection of the intended cases
Y3 (ICT1) Training duration
Months
Basic Intensive Care training 12 months
Y4 (ICT2) - Y5 (ICT3) Training duration
Months
Coronary care units 3months
Cardiothoracic surgical ICU units 2 months
Pulmonology ICU 2 months
Nephrology dialysis units 1 month
Transplant units
liver transplantation ICU
Renal transplant ICU
2month
Pediatric ICU 2months
Neurology ICU units 2 months
Neurosurgery post operative ICU 2months
General emergency post operative ICU 2months
Intensive care units 6 months
Regulations of the training program for the
Egyptian Fellowship of Intensive Care
Entry requirements
Graduation from medical school and successful completion of the pre-registration
house officers’ year.
Intensive Care Medicine Egyptian Fellowship
9
Trainees who are enrolled in the Ministry of Health and Population (MOHP) residency
program as Intensive Care trainees: will start the program from Y1.
Trainees who have had their masters’ degree in general medicine, cardiology,
pulmonology, anesthesia or ICU: will join the program from Y3 (CCT1). These
trainees will be exempted from Y1& Y2 and the 1st part exam of the Egyptian
Fellowship of Intensive Care.
General Rules and Regulations
Trainees should pass a local TOEFL exam with a minimum score of 500 and should
pass a computer course in word processing, Internet and power point in order to be
eligible for the 1st part exam
Trainees should pass successfully the 1st part exam of the Egyptian Fellowship of
Intensive Care before being promoted to Y3 (ICT1) (including exam of basic science)
Trainees must pass successfully all the obligatory foundation courses (evidence based
medicine, communication skills, research methodology and medical ethics) before
being promoted to Y3 (ICT1) of their training. Full information about foundation
courses is available at the EF website and administration office.
After completing the whole training period, completing all logbook requirements and
completing their research project, trainees are allowed to sit for the 2nd part exam.
Only candidates who pass successfully the 2nd part exam are allowed to sit for the 3rd
part.
Trainees’ General Duties and Obligations during the
Training Period of the Intensive Care Fellowship Program
Trainees must attend at least 75% of the lectures designed for each module.
Trainees must attend at least 75% of the practical sessions designed for certain
modules.
All trainees will work as trainees (dedicated full time) in the accredited hospital and
they must fulfill all trainees’ jobs defined by supervisors and trainers.
The trainees should be responsible under supervision for inpatient routine work
The trainees should be actively involved and fully responsible for patient care
including sharing in making decisions about diagnosis and management under
supervision of consultants.
They must take supervised shifts (on call duties) according to hospital requirements
and regulation.
Trainees’ Specific Duties and Obligations during GM
During their rotations in General Medicine, trainees will act as junior trainees and will share the
same responsibilities of corresponding trainees in these specialties. These include full obligations
towards admitted patients, in the inpatient and outpatient clinics, mandatory clinical and academic
activities and record these activities as required in the log book.
Trainees’ Specific Duties and Obligations during ICT
Intensive Care Medicine Egyptian Fellowship
10
Obligations in the Intensive Care units The trainees should attend the Intensive Care rounds and become actively involved in
history taking, examination and management of these critically ill patients under
supervision from their trainers.
The trainees should also perform regularly under supervision certain diagnostic and
therapeutic procedures.
The trainees in the Intensive Care rotations will be responsible for supervised admission of
patients. In such cases, the trainees will write the admission form for the patient with a
written plan of management after consultation and approval from consultants or
supervisors.
During their Intensive Care rotations, trainees should attend and participate in at least 75%
of the total number of clinical rounds and journal club meetings within the rotation period.
Obligations towards admitted patients
The trainees in the inpatient rotations will be responsible for reporting the progress of the
patient in stuff rounds.
The trainees will be responsible for the following:
Completing history and examination forms.
Writing investigations requests and ordering necessary diagnostic procedure.
Writing medication sheet according to the management plan approved by the
supervisors.
Writing daily progress notes.
Reporting results of investigations.
Discussing the case in weekly inpatient rounds with consultants and supervisors.
Writing discharge summaries and follow up cards
Writing sick leaves and medical reports for inpatients
Logbook The trainees must keep and update the Logbook where they record all activities and skills
performed and learned during the training program whether being performed independently or as
assistant or observer. Each activity registered in the Logbook should be countersigned by the
trainer and finally by the educational supervisor. The trainer and educational supervisor shall sign
the completed logbook at the end of the training program.
Research project The trainees should undertake one research project during their training program under guidance
and supervision of their trainers. After passing the 1st part exam of the Egyptian Fellowship of
Intensive Care, each candidate will be given a topic chosen by the scientific council. The review
article should be presented to an educational committee before the trainee is accepted for
admission to the 2nd
part exam of the Egyptian Fellowship of Intensive Care
Evaluation Procedures 1st, 2nd and 3rd parts of the Intensive Care Fellowship Exam.
Performance of the trainees will be evaluated on regular and continuous basis and the evaluation
process should involve all aspects of the training including theoretical, clinical, investigative
procedures, skills as well as attendance and participation.
The trainers who are required to write confidential reports of the performance of each trainee
should evaluate the trainee periodically. The trainee should not be allowed to proceed in the
training program and move to the next rotation unless he/she attains a satisfactory level of
Intensive Care Medicine Egyptian Fellowship
11
performance acceptable to the responsible trainer and educational supervisor.
Holidays According to the Ministry of Health regulations
Interruption of Training It is not permissible to interrupt such a structured training program except in major unavoidable
circumstances. Such circumstances should be convincing and approved by the Secretary General.
The interruption once approved should not be for more than one year. Interruption of the training
program for more than one year shall result in dismissal from the program and cancellation of the
preceding training period
Rational Statement The purpose of this curriculum is to describe the knowledge, skills and attitudes that must be
gained by trainees in Intensive Care in order to practice independently and safely. The curriculum
also describes teaching, learning and assessment methods that will be used to ensure that the
trainees have attained the required competencies. We derived the content of the curriculum
through consultation and revision of the European and the American Board curricula.. Therefore,
we ensured that the curriculum is up to the international accepted standards of practice in Intensive
Care training. In the meantime the curriculum addresses national needs for Intensive Care practice
and the availability of training resources
Aims
The aim of the program is to provide the community with skilled independent intensivist
who:
1. Have essential knowledge about the pathophysiology, clinical presentation and
management of critical illnesses.
2. Have skills necessary to diagnose and manage common and important life threatening
emergencies.
3. Have achieved certain level of competency in Intensive Care procedures and management
of specific Intensive Care subspecialties including cardiac, organ transplant and
neurological cases.
4. Have communication skills that result in effective information exchange and teaming with
patients, their families, and professional associates.
5. Are capable of applying national and international standards of patient care using the
principles of evidence based medicine competently in practice.
6. Keep ethical attitudes and respond to the changing health needs of the community.
7. Keep their medical standards through encouraging the concept of continuing medical
education.
Intensive Care Medicine Egyptian Fellowship
12
Program Intended Learning Outcomes
Knowledge & Understanding
By the end of the program, Intensive Care fellowship trainees will gain knowledge and
systematic understanding of:
1. The basic scientific knowledge related to critical illness in its different aspects.
2. The etiology, clinical features, natural history and prognosis of critical illness in different age
groups
3. The basic concepts of important diagnostic and therapeutic procedures, their indications,
limitations and complications.
4. The management of certain subdivisions in critical illness including cardiac, neurological and
transplanted patients.
5. The differential diagnosis of various critical illness presentations.
6. The principles of health education, disease prevention, amelioration of suffering and disability
and rehabilitation where relevant.
Skills
I. Intellectual skills:
By the end of the training years, trainees will be able to:
1. Interpret, integrate and document the history and physical examination findings with
histopathology to arrive to an appropriate provisional diagnosis and differential diagnosis.
2. Select the most appropriate and cost effective investigations and diagnostic procedure and
interpret the results of investigations.
3. Combine the clinical and investigational knowledge, with evidence-based knowledge to reach
proficiency in clinical problem solving.
4. Plan management and design rational therapeutic strategies with the appropriate involvement of
the patient and family.
5. Recognize when a clinical problem exceeds their capacity to deal with it safely and efficiently
and when to request support and expert advice from colleagues and seniors.
6. Make decisions in different aspects of delivering intensive care.
7. Interpret and criticize medical evidence logically and scientifically.
8. Analyze common clinical practice, management, and education roles used by intensivist.
9. Corroborate the advances in knowledge which will occur in his work over his entire career.
II. Professional and Practical skills
By the end of the training years, trainees will be able to:
1. Take a tactful, accurate, organized and problem-focused medical history and relate this to the
Intensive Care Medicine Egyptian Fellowship
13
general medical condition of the patient.
2. Perform a reliable focused and appropriate examination in addition to relevant general physical
examination.
3. Choose from the repertoire of clinical skills, those which are appropriate and practical in a given
situation.
4. Competently carry out different therapeutic modalities as detailed in their specific modules.
5. Recognize patients with serious/life-threatening conditions requiring Intensive Care and outline
an initial course of management.
6. Apply sterile, safe techniques and infection control guidelines according to international
principles.
7. Monitor the efficacy of therapy by assessing the patient's response according to the relevant
clinical and investigative parameters and re-evaluate management plan accordingly.
8. Communicate opinion in oral and written form.
III. Skills related to health promotion and disease prevention:
By the end of the training years, trainees will be able to:
1. Provide health promotion and quality of life advices for patients with critical illness
2. Provide health education sessions for the prevention and management of infectious problems in
the ICU
IV. Skills related to delivery of quality health care services
By the end of the training years, trainees will be able to:
1. Practice cost effective health care through proper resource allocation that does not compromise
quality of care.
2. Work with health care managers and health care providers to assess, coordinate, and improve
patient care.
3. Acknowledge medical errors and help in the development of systems to prevent them.
V. Generic and Transferable skills:
By the end of the training years, trainees will be able to:
1-Communicate effectively with patients, in the form of:
Demonstrate respect to all patients irrespective of their socio-cultural or religious status.
Conduct patient interview with patience, attentive listening and respect.
Adequately and clearly explain to the patient and/or his relatives the nature of the illness,
diagnostic and therapeutic plans, possible complications and outcomes.
Provide information in a manner which ensures that patients and families are adequately
informed when being advised of their diagnosis and/or consenting to any procedures or
treatment.
Handle appropriately difficult situations such as conveying bad news or dealing with
patients' anger.
Discuss the progression of the patient's condition, therapeutic outcomes and professional
Intensive Care Medicine Egyptian Fellowship
14
mistakes (if any), openly in a way that promotes patient trust and confidence.
2-Communicate effectively with health care providers, in the form of:
Willingness to work effectively and respect contribution in a team with other colleagues,
seniors, coworkers and other health care providers, and to behave honorably towards them
and to acknowledge and respect their opinions.
Seeking formal and informal consultations from colleagues.
Document correct patient’s medical records (admission sheet, progress notes, discharge
sheet, consultation request, investigations, informed consent and drug prescription).
Mange time effectively.
Analyze his own practical experience to recognize his/her strengths, deficiencies, and
limits in knowledge and expertise.
Use evaluations of performance provided by peers, patients, superiors, and subordinates to
improve practice.
Use information technology to optimize patient care and enhance his/her lifelong learning
skills.
Locate, appraise, and summarize evidence from scientific studies related to health
problems of his patients.
PROFESSIONALISM:
1. Accept responsibility for patient care including those who are not able to pay or from different
social or religious background
2. Demonstrate integrity, honesty, compassion, and empathy in his role as a physician
3. Respect the patient’s privacy and autonomy and maintaining appropriate professional
boundaries
4. Demonstrate accountability and commitment

Intensive Care Medicine Egyptian Fellowship
15
Intensive Care Medicine Egyptian Fellowship
16
The core curriculum for training in adult ICM is categorized in domains, each of
which is presented as Knowledge, Skills, Attitudes and behavior, lectures,
procedures, workshops, and different scientific activities targeting competence and
professionalism, in addition to basic sciences.
The curriculum refers only to adult practice except for those items listed in the
pediatric section.
Syllabus
Intensive Care Medicine Egyptian Fellowship
17
Intensive care procedures
GENERAL DESCRIPTION of the training including educational purpose, rationale or value:
The training program requires certification of clinical competency in specified diagnostic and
therapeutic procedures.
Trainees receive both didactic and various practice sessions, life videos, and simulator training in
all procedures prior to performing them on patients, as an observer, then active participant, and
finally independent operator. All trainees must be supervised by a certified trainee and document
the procedure in their procedure logbook.
TRAINEE RESPONSIBILITIES:
The trainee is responsible for attending the designated lectures to learn specific
Techniques and demonstrate initiative in completing the requisite number of procedures.
EDUCATIONAL OBJECTIVES:
During this training, the trainee will:
1. List the indications, methods, alternatives and complications for each procedure.
2. Discuss the principles of informed consent and ensure that this is obtained on all
Patients.
3. Become certified in all required procedures prior to completing the training program.
4. Be supervised by a certified individual for procedures until he/she is certified.
5. Document all completed procedure in the Procedure Log Book.
6. Discuss results of bodily fluids obtained, e.g., ascites, pleural fluid, & synovial
fluid.
7. Document procedure in the patient’s record clearly and appropriately
THE SPECIFIC PROCEDURES REQUIRED for determination of clinical competency are:
1- Tracheal intubation 11- Lumbar puncture
2- Tracheotomy 12- NG tube placement
3- Intercostal intubation 13- Cardiac pacing
4- Thoracocentesis 14- Pericardiocentesis
5- Abdominal lavage 15- Cardio version
6- Cut down 16- Urinary catheterization
7- Abdominal paracentesis 17- FAST
8- Arterial line placement
9- Arterial puncture for ABG
10- Central line placement
a- Internal jugular
b- Subclavian
c- Femoral
These procedures will be implemented over the five years training program in a synchronized way
with the nature and type of the educational program for each year.
Year 1 &2 will get the following training procedures competency
1. Thoracocentesis
Intensive Care Medicine Egyptian Fellowship
18
2. Pericardiocentesis
3. Abdominocentesis
4. Urinary catheterization
5. NG tube placement
6. Arterial puncture for ABG
Year 3 will get the following training procedures competency
1. Tracheal intubation
2. Tracheotomy
3. Intercostal intubation
4. Central line placement
a. Internal jugular
b. Subclavian
c. Femoral
5. Lumbar puncture
6. Arterial line placement
7. Cut down
8. Cardio version
Year 4 and 5 will get the following training procedures competency
1. Abdominal lavage
2. FAST
3. Cardiac pacing

Intensive Care Medicine Egyptian Fellowship
19
Y1 & Y2 1- General Medicine (GM)
(Internal medicine)
The following part of the curriculum describes the requested learning outcomes, topics and clinical
conditions that the candidate must achieve study or encounter during the whole internal medicine
program. The candidate should master management of chronic illness through rotation training
program in different medical subspecialties. This will prepare the candidate to face in the
following training years, patients with acute exacerbation of chronic illness or acute illness in a
chronically ill patient. So it is mandatory for the candidate to master and be competent in internal
medicine subspecialties before going through intensive care subspecialty
INTENDED LEARNING OUTCOMES
General internal medicine trainees must achieve the following intended learning
outcomes for the subsequently mentioned clinical conditions.
1. Define the etiology & describe the epidemiology & pathophysiology of the condition.
2. Recognize various clinical presentations through adequate history & full clinical
examination.
3. Have high index of suspicion & screen for important preventable or controllable
medical conditions like diabetes mellitus.
4. Order appropriate investigations to confirm the diagnosis & establish a differential
diagnosis.
5. Write & apply a comprehensive management plan based on patient's risk, & associated
co morbidities. The plan should include:
a. Initial & ongoing medical treatment.
b. Counseling & life style change.
c. Treatment of disease complications if present.
d. Prevention of specific risk (if relevant to the condition).
e. Referral for surgical or other specialty care if indicated.
f. Follow up options & settings.
6. Communicate appropriately with different subspecialties & refer for colleagues
& senior opinion in indicated cases.
THEORETICAL TOPICS
By the end of these two years, Intensive Care fellowship trainees will gain knowledge and
systematic understanding of the following:
Intensive Care Medicine Egyptian Fellowship
20
Cardiovascular system (problems & diseases)
1. Coronary artery diseases.
2. Congestive heart failure.
3. Rheumatic heart diseases & rheumatic activity.
4. Infective endocarditic.
5. Cardiomyopathies.
6. Hypertension.
7. Arrhythmias & dysrhythmias.
8. Aortic dissection.
9. Syncope.
10. Dyslipidemia.
Respiratory system (problems & diseases) 1. Bronchial asthma
2. Chronic obstructive airway disease
3. Upper & lower respiratory tract infections
4. Obstructive sleep apnea
5. Suppurative lung disease & bronchiectasis
6. Pleural effusion
7. Pneumothorax
8. Interstitial lung disease
9. Mediastinal syndrome
10. Tumors of the lung & pleura
11. Pulmonary embolism & DVT
12. Pulmonary hypertension
13. Respiratory failure and mechanical ventilation
Infections (problems & diseases) 1. Fever of unknown origin
2. Sepsis, shock ,DIC,ARDS
3. Community acquired infections
4. CNS infections
5. Travelers fever
6. HIV & AIDS
7. Infections in immune-compromised host
8. Tuberculosis
9. Salmonellosis
10. Hepatitis
11. Brucellosis
12. Common genitor-urinary infections
Nutritional problems 1. Cachexia
2. Metabolic syndrome
3. Obesity
4. Osteoporosis
5. Vitamin deficiency
6. Enteral & Parenteral nutrition.
Gastroenterology (problems & conditions)
Intensive Care Medicine Egyptian Fellowship
21
1. Peptic Ulceration & Gastritis.
2. GI malignancy (esophagus, gastric, hepatic, pancreatic, & colonic).
3. Inflammatory bowel disease.
4. Gastrointestinal bleeding.
5. Functional disease: irritable bowel syndrome, non-ulcer dyspepsia.
6. Celiac disease.
7. Acute liver injury: jaundice, ascites, encephalopathy.
8. Liver cirrhosis.
9. Gastro-esophageal reflux disease.
10. Gallstones.
11. Autoimmune liver disease.
Neurology (problems & conditions)
1. Transient ischemic attacks.
2. Hemiplegia.
3. Paraplegia.
4. Cranial nerve palsy.
5. Ataxias.
6. Extra pyramidal syndromes.
7. Peripheral neuropathies.
8. Myopathies & other muscle diseases.
9. Myasthenia gravis.
10. Degenerative brain diseases.
11. Brain tumors.
12. Migraine & other headaches.
13. CNS infections.
14. Language problems.
15. Multiple sclerosis.
16. Seizures.
Hematology (problems & conditions)
1. Bone marrow failure & myelodysplastic syndromes.
2. Bleeding disorders (hemophilia & purpura).
3. Thrombophilias (acquired & congenital).
4. Transfusion reactions.
5. Anemia & Haemolytica disease.
6. Leukemia.
7. Lymphoma.
8. Myeloma.
9. Myeloproliferative disease.
10. Amyloid diseases.
11. Care of Bone Marrow Transplantation recipient.
Rheumatology & musculoskeletal conditions
1. Gout
2. Systemic lupus erythematosus & other vasculitides.
3. Rheumatoid arthritis.
4. Osteoarthritis.
5. Tendinitis.
6. Fasciitis & myositis.
Intensive Care Medicine Egyptian Fellowship
22
7. Dermatomyositis.
8. Osteomalacia & osteoporosis.
9. Chronic fatigue syndrome.
10. Polymyalgia & temporal arteritis.
11. Septic arthritis.
Endocrine & metabolic conditions
Diabetes Problems 1. Diabetes and Diabetic ketoacidosis.
2. Non-acidotic hyperosmolar coma.
3. Uncontrolled diabetes (type 1 & type 2).
4. Hypoglycemia.
5. Peri-operative diabetes care.
6. Gestational diabetes.
Other Endocrine Problems
1. Hyper/Hypocalcaemia.
2. Adrenocortical insufficiency.
3. Hyper/Hyponatremia.
4. Thyroid dysfunction.
Renal problems & conditions
1. Acute renal failure
2. Chronic renal failure.
3. Glomerulonephritis and acute nephritic syndrome.
4. Nephrotic syndrome.
5. Urinary tract infection.
6. Renal calculi.
7. End stage renal disease.
8. Care of patients on renal replacement therapy.
9. Electrolyte imbalance in renal patients.
Dermatological problems in medical practice
The trainee is requested to recognize the condition, initiate management & timely involve
dermatology specialists
1. Hyperpigmented lesions.
2. Cellulitis.
3. Diabetic ulcers.
4. Erythematous skin lesions.
5. Cutaneous drug eruptions, urticaria & angioedema.
6. Eczema.
7. Vasculitis.
8. Psoriasis.
9. Vitiligo.
10. Herpes zoster & herpes simplex.
11. Lymphedema.
Occupational diseases
The trainee is requested to screen for or suspect the following conditions during routine practice
settings & timely refer to appropriate specialty
1. Lead poisoning.
2. Asbestosis.

Intensive Care Medicine Egyptian Fellowship
23
3. Occupational lung diseases.
Traveler’s diseases
The trainee is requested to suspect & initiate investigations and treatment for the
following conditions in high-risk groups.
1. Malaria.
2. Avian flu.
3. Swine flu
4. SARS
Genetic disorder
For The following genetic conditions, the trainee would be able to diagnose the case and
consult appropriately.
1. Down’s syndrome.
2. Turner’s syndrome.
3. Huntington’s disease.
4. Hemochromatosis.
5. Marfan’s syndrome.
6. Klinefelter’s syndrome.
7. Familial cancer syndromes.
8. Familial cardiovascular disorders.
CLINICAL CASES
By the end of these two years, trainees will be able to manage competently the following cases:
Cardiac Cases 1. Acute coronary syndrome
2. Cardiac arrest
3. Syncope
4. Right sided heart failure
5. Left sided heart failure (rheumatic, ischemic, cardiomyopathic)
6. Cardiogenic shock
7. Atrial arrhythmia
8. Ventricular arrhythmia
9. Pericarditis
10. Artificial valve dysfunction
Hypertension
Respiratory Cases 1. Adult respiratory distress syndrome (ARDS)
2. Respiratory failure (COPD)
3. Respiratory failure (status asthmaticus)
4. Respiratory failure (pneumonia)
5. Severe community acquired pneumonia (CAP)
6. Ventilator associated pneumonia (VAP)
7. Aspiration pneumonia
8. Pulmonary embolism
9. Pneumothorax
Intensive Care Medicine Egyptian Fellowship
24
10. Respiratory failure in special situations ( e.g. pregnancy)
11. Hemoptysis
Hematological cases 1. Leukemia
2. Lymphoma
3. Coagulation disorders
4. TTP
ITP
Nephrology cases 1. Nephrotic syndrome
2. Acute nephritis
3. Acute renal failure
4. Chronic renal failure
5. Hypertension
6. Urinary tract infection
7. Tubular disorders
8. Hematuria for differential diagnosis
9. Proteinuria for differential diagnosis
Endocrinal disorders 1. Thyroid diseases
2. Suprarenal diseases
3. Pituitary diseases
Neurological and neuromuscular cases 1. Epilepsy
2. Cerebro vascular stroke
3. Spinal cord injuries (traumatic, vascular…)
4. Guillain Barré syndrome
5. Myasthenia gravis
6. coma
7. Vegetative state
8. Myopathy
9. Neuropathy
Rheumatology cases 1. SLE
2. Rheumatoid arthritis
3. Vasculitis
4. Connective tissue diseases
Diabetes & metabolism Cases 1. Diabetic cases
2. Electrolyte disturbances
Internal medicine emergency Cases 1. CNS
2. Cardiac
3. Respiratory
4. Abdominal
5. Hepatic
6. Renal
7. Vascular
8. Hematological
Intensive Care Medicine Egyptian Fellowship
25
9. Mixed
Gastroenterology Cases 1. Crohns disease
2. Ulcerative colitis
3. Hematemesis
4. Melena
5. Pancreatic diseases
Hepatology Cases 1. Hepatitis
2. HCC
3. Ascites
4. Liver cell failure, hepatic coma
5. Portal hypertension and GIT bleeding
6. Jaundice
Dermatological problems in medical practice 1. Hyperpigmented lesions.
2. Cellulitis.
3. Diabetic ulcers.
4. Erythematous skin lesions.
5. Cutaneous drug eruptions, urticaria & angioedema.
6. Eczema.
7. Vasculitis.
8. Psoriasis.
9. Vitiligo.
10. Herpes zoster & herpes simplex.
11. Lymphedema.
Infectious cases
1. Malaria.
2. Avian flu.
3. Swine flu
4. SARS
5. Meningitis
6. Encephalitis
7. Tetanus
PROCEDURES AND SKILLS
Upon completion of this Y1& Y2 the candidate should be able to discuss the indications
contraindications and complications of every procedure. He should be able to discuss the risk
benefit of each procedure. He should be able to master all these procedures with high competency.
These procedures are;
1. Arterial puncture for ABG
2. Thoracocentesis
3. Abdominocentesis
4. Pericardiocentesis
5. NGT settlement
6. Urethral catheter settlement
Intensive Care Medicine Egyptian Fellowship
26
WORKSHOPS (All to be attended through this Y1&Y2 training program)
1. AIRWAY
2. BLS
3. ACLS
4. ECG
5. LAB.INTERPRETATION
6. ECHOCARIOGRAM TRANSTHORACIC
Y1 &Y2 2- Basic sciences
1. Physiology
2. Pathology
3. Pharmacology
4. Clinical pathology
5. Radiology
6. Immunology & bacteriology
INTENDED LEARNING OUTCOMES
Knowledge : By the end of the first two years of training, trainees should have adequate knowledge about:
The normal function of the human body (cell tissues and organs).
The nature of agents and mechanisms that produce alterations in Structure and function of
the body.
The nature and course of alterations in function produced by Etiological agents and
mechanisms (Pathophysiology) of the body.
The nature and course of alterations in structure produced by Ttiological agents and
mechanisms (Pathological Anatomy) of the body.
The appropriate use of laboratory techniques in identifying diseases or health problems.
The action, metabolism, and toxic effects of drugs.
The therapeutic use of drugs.
The principles and concepts underlying normal behavior and mental illness.
The definition ,classifications, and types of immunological reactions
Bacterial classifications, normal flora, pathogenesis of infection, lab. diagnosis, and best to
treat
Skills: The ability to perform a satisfactory physical exam.
The ability to take a satisfactory medical history including psychosocial, nutritional,
occupational and sexual dimensions.
The ability to utilize data from the history, physical exam and laboratory
evaluations to identify the health problem.
The ability to formulate an appropriate differential diagnosis.
Intensive Care Medicine Egyptian Fellowship
27
The ability to formulate effective management plans (diagnostic, treatment, and
prevention strategies) for diseases and other health problems.
The ability to monitor the course of illnesses and to appropriately revise the
management plan.
The ability to perform routine technical procedures specific to the medical
specialty.
The ability to document the clinical encounter.
The ability to apply the therapeutic use of drugs in patient care.
The ability to recognize the relationship between health and illness, the patient and
the patient's environment.
The ability to apply preventive and health maintenance principles and techniques in
the delivery of health care.
The ability to apply the appropriate use of laboratory methods in identifying
diseases or health problems.
The ability to recognize patients with immediately life threatening conditions.
The ability to manage pain and ameliorate the suffering of patients.
The ability to apply Evidence Based Medicine principles to clinical decision
making.
The ability to Produce radiologic comments that are accurate, concise, and
grammatically correct
The ability to diagnose immunological diseases
The ability to tackle infection through diagnose, management, and prevention
Attitude and behavior: The ability to apply humanistic values in the delivery of health care.
The ability to work cooperatively with other health care workers in the delivery of
health care.
The ability to respect the patients’ dignity, privacy, and confidentiality in the
delivery of health care.
The ability to effectively interact with patients, peers and other healthcare workers
from diverse cultural backgrounds.
THEORETICAL TOPICS RELEVANT TO BASIC SCIENCES
By the end of these two years, Intensive Care fellowship trainees will gain knowledge and
systematic understanding of the following:
Physiology 1. Mechanics of the heart
2. Blood pressure regulation
3. Blood volume regulation
4. Systemic versus pulmonary circulation
5. Coronary and cerebral circulation
6. Renal perfusion and function
Intensive Care Medicine Egyptian Fellowship
28
7. Oxygen cascades
8. Lung mechanics
9. Body temperature regulation
10. Hemostasis
11. Body response to trauma
Pathology
1. Inflammation and sepsis
2. Cell injury
3. Cell adaptation
4. Acute respiratory distress syndrome(ARDS)
5. Bronchial asthma
6. Renal failure acute and chronic
7. Vasculitis
8. Basic immunologic reactions
9. Pancreatitis
10. Liver failure
11. Rejection reactions
Pharmacology 1. Pharmacodynamics and kinetics
2. Volume of distribution
3. Vasoactive drugs
4. Antihypertensive drugs
5. Antiarrhythmic drugs
6. Anticoagulants
7. Fibrinolytics
8. Sedatives
9. Muscle relaxants
10. Hypnotics
11. Anticonvulsants
12. IHD drugs
13. Bronchodilator drugs
Clinical pathology 1. CBC interpretation
2. Urinalysis
3. Exudates versus transudates
4. Cardiac enzymes
5. Lipids and lipid profile
6. Tumor markers
7. Coagulopathy
8. Atherothrombotic
9. Ascitic fluid
10. Pleural fluid
11. Broncho-alveolar lavage
Radiology
1. Chest X ray
2. CT chest
3. CT brain
Intensive Care Medicine Egyptian Fellowship
29
4. MRI brain
5. CT spine
6. MRI spine
7. Ultra sound abdomen
Immunology & bacteriology 1. Immunology
a. Definitions
b. Classifications
c. Types of reactions
d. AIDS
2. Bacteriology
a) Classifications
b) Normal flora
c) Pathogenesis of infections
d) Lab. diagnosis
e) Bacterial resistance
Intensive Care Medicine Egyptian Fellowship
30
Y3 (ICM1)
1- Basic intensive care medicine
By the end of this year, Intensive Care fellowship trainees will gain knowledge and systematic
understanding of the following items:
1. Criteria for admission and discharge to ICU
2. Oxygen cascades
3. Carbon dioxide cascades
4. Acid base disturbances
5. Transport of critically ill patients
6. Pre and post operative care
7. Comfort care
8. Sepsis and infection control
9. End of life care
CRITERIA FOR ADMISSION AND DISCHARGE TO ICU
Candidates should be able to:
Select patients who are likely to benefit from ICU care
Utilize prioritization, diagnosis, and objective parameters models.
Prioritization Model Candidate should be able to utilize prioritization system for admission of patients
This system defines those that will benefit most from the ICU (Priority 1) to those that will not
benefit at from ICU admission.
Priority 1: These are critically ill, unstable patients in need of intensive treatment and monitoring
that cannot be provided outside of the ICU.
Priority 2: These patients requirpe intensive monitoring and may potentially need immediate
intervention. No therapeutic limits are generally stipulated for these patients.
Priority 3: These unstable patients are critically ill but have a reduced likelihood of recovery
because of underlying disease or nature of their acute illness.
Priority 4: These are patients who are generally not appropriate for ICU admission. Admission of
these patients should be on an individual basis, under unusual circumstances and at the discretion
of the ICU Director
Diagnosis Model Candidate should be able to define and diagnose the life threatening cases from, cardiovascular
system, pulmonary system, neurological system, drug ingestion and drug over dose,
gastrointestinal system, endocrinal system, surgical problems, and mixed cases
Intensive Care Medicine Egyptian Fellowship
31
Objective Parameters Model Candidate should be able to build up the criteria for admission on specific vital signs, laboratory
data, radiological data, and ECG data.
Discharge Criteria The status of patients admitted to an ICU should be revised continuously to identify patients who
may no longer need ICU care.
A. When a patient's physiologic status has stabilized and the need for ICU monitoring and care is
no longer necessary
B. When a patient's physiological status has deteriorated and active interventions are no longer
planned, discharge to a lower level of care is appropriate
Skills Good assessment of critically ill patient
Prioritization
Admission and discharge according to prescribed guidelines
Attitude Communicate effectively with intended medical staff and patient family
Good explanation for either admission or discharge
Oxygen cascades
Knowledge
Trainees should have adequate knowledge and deep understanding of:
Pressure oxygen in air, alveoli, arterial and venous blood, and at mitochondrial level
Oxygen dissociation curve and factors affecting it
Oxygen delivery, extraction and extraction fraction ratio
Hypoxia, causes, and pathogenesis and its management
Oxygen supply, indications, contraindications, and different ways of its supply
Central oxygen and peripheral oxygen stores
Apnea ventilation and how to utilize it
Oxygen behavior at alveoli and tissue
Skills Trainees will be able to:
Calculate oxygen pressure in alveoli
Recognize Alveoarterial gradient, its values, and its importance
Calculate oxygen delivery, and extraction fraction
Read oxygen in ABG
Utilize oxygen dissociation curve for patient diagnosis and management
Improve patient oxygenation through face mask or ventilation
Use appropriately pulse oximeter, and blood gases machine
Attitude
Intensive Care Medicine Egyptian Fellowship
32
Be determined to provide the best care possible to all admitted case and based on
appropriate guidelines
Follow-up patients through good and competent monitoring.
Has good communication and relationships with ward staff.
Good handling and utilization of ICU machines
Carbon dioxide cascades
Knowledge Trainees should have adequate knowledge and deep understanding of:
The pressure of carbon dioxide in air, alveoli, arterial and venous blood, and at cellular
level
The hypo and hypercarbia, causes, and pathogenesis and its management
Ventilatory support, indications, and management
The central and peripheral carbon dioxide stores
Apnea ventilation and how to utilize it
The use of capnogram
Skills Trainees will be able to:
Use capnogram appropriately for the diagnosis management and outcome detection of
their patients
Adjust carbon dioxide in a ventilated patient
Read carbon dioxide in ABG
Operate appropriately capnogram, and blood gases machine
Knowledge Trainees should be able to:
Define anion gab, its value normal or abnormal and discuss how to use it in diagnosis
and management
Define the normal value of ABG and recall the definition of each item
Discuss the classifications causes, diagnose, and management of acidosis
Discuss the classification, causes, diagnosis, and management of alkalosis
Discuss pH and Henderson Hassel Bach equation
Discuss the rules used for calculation and compensation
Discuss base deficit and how to correct
Differentiate between Alfa versus pH state
Describe ABG sampling techniques and pitfalls
Acid base disturbances
Intensive Care Medicine Egyptian Fellowship
33
Skills Trainees will be able to:
Interpret ABG
Take ABG sample
Use appropriate calculation methods for diagnosis and replacement therapy
Timely make appropriate decisions in the diagnosis and management after ABG
reading
Knowledge Trainees should be able to:
Discuss the principles of safe transfer of patients.
Describe various portable monitoring systems
Skills Trainees should:
Perform Intra-hospital transfer of patients requiring ventilatory support alone.
Perform Inter hospital transfer of patients with single or multiple organ failure.
Attitude and behavior Insist on stabilization before transfer.
Pre transfer checking of kit and personnel.
Anticipate and prevent problems during transfer.
Communicate with referring and receiving institutions and teams.
Insist on adequate support from senior / more experienced colleagues.
Knowledge
By the end of training, trainees will have adequate knowledge and deep understanding of:
Factors which predispose patients to critical illness, including poor nutrition.
Early warning signs of impending critical illness.
Methods of optimizing high risk surgical patients.
Criteria for admission to & discharge from intensive & high dependency (HDU) care
units.
Risk factors for ICU readmission following discharge to the ward.
Tracheostomy care outside the ICU or HDU.
Post-ICU mortality rate, and common reasons for death following discharge
Common symptomatology following critical illness .
Rehabilitation: physical and psychological .
Long-term or home ventilation .
Persistent vegetative state .
5-Transport of the critically ill patients
Pre- and post-ICU care
Intensive Care Medicine Egyptian Fellowship
34
Skills
By the end of training, trainees will able to:
Perform Resuscitation and initial stabilization (see domain 1).
Recognize and manage risk factors associated with critical illness.
Manage Optimization of high-risk surgical patients before surgery
Liaison with ward staff to ensure optimal communication & continuing care after ICU
discharge.
Perform Timely discussion of ‘do not resuscitate’ orders and treatment limitation
decisions.
Identify complications associated with critical illness (e.g.: nerve palsies) and appropriate
referral.
Attitudes and behavior Be determined to provide best care possible regardless of environment.
Follow-up of patients following discharge to the ward.
Have Good communication and relationships with ward staff.
Knowledge
By the end of training, trainees will have adequate knowledge and deep understanding of:
Causes of, and methods of minimizing distress to patients
Bereavement: anticipating and responding to grief
Methods of communicating with intubated patients
Methods of measuring depth of sedation
Stress responses
Causes and management of acute confusional states
Sleep deprivation and its consequences
Acute pain management
Patient-controlled analgesia
Indications, contra-indications and complications of commonly used analgesic, hypnotic,
and neuromuscular blocking drugs
Comfort care
Intensive Care Medicine Egyptian Fellowship
35
Pharmacokinetics and dynamics of commonly used analgesic and hypnotic agents, and
neuromuscular blocking drugs in-patients with normal and abnormal organ system
function.
Indications, contra-indications, methods and complications of regional analgesia in critical
illness
Importance of mouth care
Skills
By the end of training, trainees will able to:
Identify and treat causes of distress
Safely use analgesic, hypnotic and neuromuscular blocking drugs
Manage appropriately established epidural analgesia
Minimize complications associated with opioid and non-opioid analgesics
Attitude and behavior Minimize patient distress
Work with nurses and relatives to minimize patient distress
Communicate with and support next-of-kin
Knowledge
By the end of training, trainees will have adequate knowledge and deep understanding of:
Universal precautions and good working practices (hand washing, gloves etc) .
Proper handling of medical devices including intravascular devices .
Cross infection: modes of transfer and common agents.
Autogenous infection: routes and methods of prevention.
Emergence of resistant strains.
Antibiotic policies in a hospital.
Activity of commonly used antibiotics.
Common surgical infections: antibiotic choice and prophylaxis.
Infections from contaminated blood.
Hepatitis and HIV infections: modes of infection: natural history: at risk groups.
Immunization policy.
Sterilization of equipment.
Strategy if contaminated .
Skills Trainees will be able to:
Recognize specific risk groups including immunocompromised patients .
Sepsis and infection control
Intensive Care Medicine Egyptian Fellowship
36
Recognize the risk associated with administration of IV antibiotics: e.g. risk of allergy
and anaphylaxis etc.
Use appropriate aseptic techniques .
Use disposable filters and breathing systems .
Use protective clothing/gloves/masks etc .
Apply appropriate methods for preventing autogenous infection (e.g.: posture, mouth
hygiene) .
Attitude and behavior Appreciate that every patient is entitled to the best care available
Prevent self-infection
Appreciate that prevention of cross infection is their responsibility
Knowledge
Trainees should have adequate knowledge and deep understanding of:
Causes of, and methods of minimizing distress to patients
Bereavement: anticipating and responding to grief
Methods of communicating with intubated patients
Methods of measuring depth of sedation
Stress responses
Causes and management of acute confusional states
Sleep deprivation and its consequences
Acute pain management
Patient-controlled analgesia
Indications, contra-indications and complications of commonly used analgesic, hypnotic,
and neuromuscular blocking drugs
Pharmacokinetics and dynamics of commonly used analgesic and hypnotic agents, and
neuromuscular blocking drugs in-patients with normal and abnormal organ system
function.
Indications, contra-indications, methods and complications of regional analgesia in critical
illness
Importance of mouth care
Skills Trainees will be able to:
Identify and treat causes of distress
End of life care
Intensive Care Medicine Egyptian Fellowship
37
Safely use analgesic, hypnotic and neuromuscular blocking drugs
Manage established epidural analgesia
Minimize complications associated with opioid and non-opioid analgesics
Attitude and behavior be sincere towards minimization of patient distress
Work collaboratively with nurses and relatives to minimize patient distress
Aim to communicate with and support next-of-kin
Y3 (ICM1)
In this year the candidate will gain most of his knowledge, skills, and experiences managing all the
multidisciplinary critically ill case in such ICU. It the working place for the intensive care fellow.
Resuscitation, stabilization, clinical assessment, monitoring, investigation, performing required
and indicated procedures, discussing differential diagnosis, management, and discharge plane, all
should be mastered with competence though this year
INTENDED LEARNING OUTCOMES
a- Resuscitation and initial stabilization
Knowledge
By the end of training, trainees should have adequate knowledge and deep understanding of:
The patient at risk of critical illness including cardiopulmonary arrest.
The management of common medical emergencies (acute asthma, COPD, hypertension,
myocardial infarction, ventricular failure, hypotension and shock, hemorrhage).
The common causes for admission to intensive and high dependency care.
Triage and management of competing priorities.
Methods of maintaining a clear airway.
Indications for and methods of tracheal intubation.
The use of drugs to facilitate airway control.
Criteria for Selection of tube type (oral, nasal, armoured etc), diameter and length.
The Management of difficult intubation and failed intubation.
Methods of confirming correct placement of the endotracheal tube.
The methods for Insertion and use of oral airways face masks and laryngeal mask airway.
Causes of regurgitation and vomiting; prevention and management of pulmonary
2- Adult Intensive care medicine
Intensive care of general
medical conditions
Intensive Care Medicine Egyptian Fellowship
38
aspiration.
Cricoid pressure.
Airway management in special circumstances, (head injury, full stomach, upper airway
obstruction, shock).
Indications for and methods of ventilatory support.
the recognition and Emergency treatment of life-threatening disorders of cardiac rhythm.
External cardiac massage.
Drugs: pharmacology and dosages of hypnotics, analgesics and relaxants.
Side effects of drugs used and their interactions.
Approaches to Monitoring during sedation/induction of anesthesia for endotracheal
intubation.
The Recognition and management of anaphylactic and anaphylactoid reactions.
the Recognition and management of inadvertent intra-arterial injection of harmful
substances.
Problems of the obese or immobilized patient.
Methods of securing adequate vascular access rapidly.
Skills
Trainees should appropriately perform the following skills:
Life support skills to ALS provider level.
Airway assessment and optimizing the patient’s position for airway management.
Airway management with mask and oral/nasal airways.
Support of ventilation using bag and mask.
Introduction and checking correct placement of laryngeal mask airway.
Appropriate choice and passage of oral endotracheal tubes.
Orotracheal intubation: (up to grade II Cormack-Lehane for SHOs).
Use of gum elastic bougie and stiletto.
9. Identifying correct/incorrect placement of tube (oesophagus, R main bronchus).
Interpretation of capnograph trace.
Failed intubation drill.
Rapid sequence induction/cricoid pressure.
External cardiac massage.
Percutaneous pericardial aspiration (emergency).
Obtaining vascular access sufficient to manage acute hemorrhage.
Fluid resuscitation and initial management of shock, including use of drugs.
Use of emergency monitoring equipment.
Safety checking of resuscitation equipment (see equipment section).
Management and avoidance of cardiovascular and respiratory changes during and after
intubation.
Attitudes and behavior Stick to the principles of Safety first and knowing limitations.
Intensive Care Medicine Egyptian Fellowship
39
Always knowing the location of senior assistance.
Being clear in explanations to patient and staff.
Being reassuring to patients and relatives.
Consideration of ethical issues: e.g. patient autonomy, appropriateness of ICU
admission.
b- Clinical assessment
Knowledge
Trainees should have adequate knowledge and deep understanding of:
The Importance of clinical history in making diagnosis.
The Relevance of prior health status in determining risk of critical illness and outcomes.
the impact of drug therapy on organ-system function.
Physical signs associated with critical illness.
The inflammatory response in relation to organ-system dysfunction.
Infection and its relation to the inflammatory response.
Methods of obtaining clinical information.
Relative importance and interpretation of clinical signs.
Pathogenesis of multiple organ dysfunctions.
Principles of prevention of multiple organ failure.
Skills Candidates should be able to:
Obtain an accurate history of the current condition, comorbidities and previous health
status using appropriate sources of information.
Elicit and interpret symptoms and signs on clinical examination.
Perform Examination and care of the unconscious or confused patient.
Obtain and interpret information from case records, charts and ICU chart.
Document information in the case record in a structured and accessible manner.
Link clinical with laboratory information to form a diagnosis.
Establish a management plan.
Timely recognize impending organ system dysfunction.
Attitudes and behavior Manage patients in a compassionate and considerate manner.
Communicate effectively with other health care professionals to obtain accurate
information and plan care
Intensive Care Medicine Egyptian Fellowship
40
c- Investigation, data interpretation and diagnosis
Knowledge By the end of training, trainees should have adequate knowledge and deep understanding of:
The use of laboratory tests to confirm or refute a clinical diagnosis.
Advantages and disadvantages of laboratory tests.
Indications for, and basic interpretation of:
Electrocardiographs of common dysrhythmias, infarction, pulmonary
hypertension/embolism, pericarditis, LVH.
Echocardiography.
Ultrasound examination.
Cardiovascular physiological variables.
Fluid balance charts.
Blood gas measurement.
Respiratory function tests.
Chest radiographs: collapse, consolidation, infiltrates (including ALI/ARDS),
pneumothorax, pleural effusion, pericardial effusion, position of cannulae, tubes or foreign
bodies, airway compression, cardiac silhouette, mediastinal masses.
X-rays of long bone, skull, vertebral and rib fractures.
CT and MRI scans of head demonstrating fractures/ hemorrhage.
Neck and thoracic inlet films.
X-rays of abdominal fluid levels / free air.
Microbiology: types of organisms; colonization vs infection; appropriate antibiotics use.
Hematology (including coagulation and sickle tests).
Blood grouping and X-matching.
Urea, creatinine, electrolytes (Na, K, Ca, Mg).
Liver function tests.
Drug levels in blood or plasma.
Endocrine function: diabetes, thyroid disorders, adrenal failure.
Skills
Bronchoscopic broncho-alveolar lavage in an intubated patient.
Diagnostic bronchoscopy in a non-intubated awake patient.
Lumbar puncture and CSF sampling.
Link clinical with laboratory information to form a diagnosis.
Establish a management plan based on clinical and laboratory information.
Document results of laboratory tests
Attitudes and behavior Communicate and collaborate effectively with all laboratory staff.
Avoid unnecessary tests
d- Organ system support and related practical procedures
Knowledge Trainees should have adequate knowledge and deep understanding of:
Intensive Care Medicine Egyptian Fellowship
41
Respiratory system
Indications for and methods of tracheal intubation.
Appropriate use of drugs to facilitate airway control.
Tube types (oral, nasal, tracheostomy etc), diameter and length.
Management of difficult intubation and failed intubation.
Methods of confirming correct placement of the endotracheal tube.
Methods for Insertion and use of oral airways face masks and laryngeal mask airway.
Indications and contraindications to tracheostomy and minitracheostomy.
Management of and complications associated with tracheostomy tubes.
Causes of regurgitation and vomiting; prevention and management of pulmonary
aspiration.
Cricoid pressure: indications and safe provision.
Airway management in special circumstances, (head injury, full stomach, upper airway
obstruction, shock, cervical spine injury).
Indications for and methods of mechanical ventilation.
Ventilatory modes: CMV, IRV, PRVC, SIMV, PS, CPAP, BiPAP, Non-invasive
ventilation.
Principles of extra-corporeal membrane oxygenation (ECMO).
Detection and management of complications of mechanical ventilation.
Detection and management of pneumothorax (simple and tension).
Insertion and safe management of chest drains.
Indications and methods of bronchoscopy via an endotracheal tube.
Indications and methods of bronchoscopy in a conscious non-intubated patient.
Principles of weaning from mechanical ventilation.
Cardiovascular system
Cardiopulmonary resuscitation to ALS provider level.
Peripheral and central venous cannulation.
Arterial catheterization.
Pulmonary arterial catheterization, oesophageal Doppler, transesophageal echo.
Principles of transvenous cardiac pacing.
Use of inotropic, chronotropic, vasodilator and vasoconstrictor drugs.
Use of intravenous fluids: crystalloids, colloids, blood and blood products.
Principles of intra-aortic counterpulsation balloon pump.
Renal system
Safe urinary catheterization.
Methods of preventing renal failure.
Investigation of impaired renal function.
Knowledge of nephrotoxic drugs.
Adjustment of drug doses in renal impairment/failure.
Renal replacement therapies.
Intensive Care Medicine Egyptian Fellowship
42
Gastrointestinal system and nutrition
Principles of adequate nutrition in the critically ill patient, including vitamins, trace
elements, immuno nutrition.
Assessment of nutritional status (e.g.: skin-fold thickness, muscle wasting).
Selection of enteral or parenteral routes for nutrition.
Nasogastric cannulation.
Nasojejunal and percutaneous feeding tube insertion.
Sengstaken tube insertion.
Principles of support for the failing liver.
Prevention of stress ulceration.
Techniques for preventing microbial translocation.
Nervous system
Principles of management of closed head injury.
Principles of management of raised intracranial pressure.
Principles of management of vasospasm.
Indications for and use of information from intracranial pressure monitoring devices.
Musculoskeletal system
Prevention of pressure sores.
Principles of management of fluid losses following burns.
Short-term complications of fractures.
Consequences of muscle wasting.
Sepsis and infection:
Requirements for microbiological surveillance and clinical sampling.
Relation between lab results and patient's condition.
Appropriate use of antibiotics.
Proper handling of invasive medical devices.
Skills
Trainees should be able to perform the following:
Maintenance of a clear airway using bag and mask.
Orotracheal intubation.
Naso-tracheal intubation.
Percutaneous tracheostomy.
Minitracheostomy or needle cricothyoidotomy.
Changing an orotracheal tube.
Changing a tracheostomy tube electively.
Manual bagging and tracheal suction.
Institution and maintenance of controlled mechanical ventilation in a critically ill
patient.
Confirmation of adequate oxygenation and control of PaCO2 and pH.
Aseptic insertion of a pleural chest drains and connects to a one-way seal device.
Establish peripheral venous access sufficient to manage major hemorrhage.
Aseptic insertion of central venous, pulmonary arterial and arterial catheters.
Aseptic insertion of tunneled central venous catheter for parenteral nutrition.
Appropriate use of intravenous fluids.
Intensive Care Medicine Egyptian Fellowship
43
Appropriate use of infused vasoactive drugs.
Measurement of cardiac output using pulmonary artery catheter or oesophageal
Doppler.
Identification and avoidance of factors contributing to impaired renal function.
Urinary catheterization: male and female.
Nasogastric tube placement.
Management of cardiorespiratory physiology to minimize rises in intracranial
pressure.
Recognition and temporary stabilization of unstable cervical spine.
Attitudes and behavior Appreciate the importance of ensuring physiological safety as a primary aim..
Recognize the difference between organ system support and specific treatment.
Appreciate the importance of timely institution of organ-system support.
Call for senior/more experienced help when experiencing difficulties.
Consider patient comfort in performance of practical procedures.
e- Monitoring and clinical measurement 1-Knowledge Trainees should have adequate knowledge and deep understanding of:
The role of clinical assessment in monitoring.
Physical principles underlying use of monitoring devices (see physics and measurement).
Indications for and contraindications to the use of monitoring devices.
Interpretation of information from monitoring devices, and identification of common
causes of error.
Principles of 'minimal monitoring'.
Complications associated with monitoring and monitoring devices.
Methods for measuring temperature.
Methods for assessing pain and sedation.
One general method for measuring severity of illness (severity scoring systems).
Methods for severity scoring or case mix adjustment for trauma, burns, therapeutic
intensity or costs.
Glasgow Coma Scale.
2-Skills Safe use of and interpretation of data from:
Pulse oximetry.
ECG (3- and 12-lead).
Non-invasive arterial blood pressure measurement.
Invasive arterial blood pressure measurement.
Central venous pressure measurement.
Pulmonary artery catheters or oesophageal Doppler.
Jugular bulb catheters and SjO2 monitoring.
Arterial blood gas sample handling.
Inspired and expired gas monitoring for O2, CO2, and NOi.
Spirometry and peak flow measurement.
Intensive Care Medicine Egyptian Fellowship
44
Ventilator alarms.
Intracranial pressure monitoring.
Nerve stimulator to measure therapeutic neuromuscular block.
Clinical assessment of pain.
Scoring or scaling systems to assess degree of sedation.
Collection of data for one general method for severity scoring or case mix adjustment.
3-Attitudes and behavior
Ensure safe use of monitoring equipment in an appropriate environment.
Minimize patient discomfort in relation to monitoring devices.
Support other staff in the correct use of devices.
Review regularly the need for continued monitoring.
f- Safe use of equipment
1- Knowledge Trainees should have adequate knowledge and deep understanding of:
Airways, tracheal tubes, tracheostomy tubes, emergency airways, laryngeal masks, fixed
and variable.
Performance oxygen therapy equipment, self-inflating bags.
Humidification and nebulizing devices.
Modes of ventilation and method of operation of at least one positive pressure ventilator,
one non-invasive ventilator, and a constant positive airway pressure (CPAP) device.
Principles of use of pressure regulators, flowmeters, vaporizers, breathing systems.
Principles of disconnection monitors.
Manufacture, storage and safe use of oxygen, nitric oxide (NOi), compressed air and
helium.
Pipeline and suction systems, gas cylinders.
Non-invasive monitoring devices.
Methods for checking ventilator, breathing systems and monitoring apparatus.
Environmental control of temperature, humidity, air changes and scavenging systems for
waste gases and vapors.
Sterilization and cleaning of equipment.
Electrical safety.
Characteristics and safe use of vascular access cannulae, spinal needles, epidural catheters,
chest drains.
Function and use of defibrillator and other resuscitation equipment, transfusion devices.
Function and use of continuous haemodiafiltration devices
2-Skills Trainees should be able to perform the following:
Checking and setting the ventilator.
Checking pipelines, checking and changing cylinders.
Connecting and checking breathing systems.
Intensive Care Medicine Egyptian Fellowship
45
Setting alarm limits for monitoring equipment.
Identifying and correcting ventilator miss-assembly and disconnections.
Collecting data from monitors.
Record keeping.
Checking, assembling resuscitation equipment.
Safe defibrillation.
Preparing equipment for:
Difficult and failed intubation.
Pediatric intubation set.
Aseptic vascular access.
Intravascular pressure monitoring.
Choosing appropriate fluid balances using renal replacement therapies.
3-Attitudes and behavior Shared responsibility for equipment with nursing and technical staff.
Determination to maximize safety.
Rapid response to acute changes in monitored variables.
THEORETICAL TOPICS
By the end of this year the candidate should have gained a vast and updated date and knowledge
about the following topics
1. Acid base disturbances
2. Water and electrolyte disturbances
3. Scoring system
4. Respiratory failure
5. Statue asthmaticus
6. Smoke inhalation and aspiration syndrome
7. Oxygen therapy
8. Pulmonary mechanics and gas exchange
9. Pathophysiology of mechanical ventilation
10. Conventional modes of mechanical ventilation
11. New modes of mechanical ventilation
12. Indications and complications of mechanical ventilation
13. Weaning of mechanical ventilation
14. Non invasive mechanical ventilation
15. Massive hemoptysis
16. Pulmonary embolism
17. Ventilator associated pneumonia(VAP)
18. Hemodynamic monitoring
19. Acute coronary syndrome
Intensive Care Medicine Egyptian Fellowship
46
20. Arrhythmias
21. Heart failure- pulmonary edema
22. Hypertensive emergencies
23. Shock
24. Vasoactive drugs in critically ill
25. Aortic dissection
26. Neuro- monitoring
27. Cerebro-vascular stroke
28. Convulsions in ICU
29. Coma
30. Neuromuscular disorders in critically ill
31. Delirium in ICU, acute psychosis, neuroleptic malignant syndrome
32. GIT hemorrhage
33. Hepatic failure
34. Acute pancreatitis
35. Abdominal compartmental syndrome
36. Ileus and motility disorders
37. Acute renal failure
38. Renal replacement therapy
39. Sepsis syndrome
40. Multiple organ dysfunction syndrome(MODS)
41. Anemia in critically ill
42. Blood and blood product transfusion
43. Bleeding and coagulation disorders
44. Diabetic emergency
45. Adrenal crisis
46. Thyroid storm and Myxedema coma
47. Microangiopathy hemolytic anemia’s(TTP HELLP--),
48. Near drowning and electric burn
49. Eclampsia
50. Total parental nutrition(TPN)
CLINICAL CASES
By the end of this training, candidate should have gained experience in the evaluation and
management of the diverse systems encountered in intensive care units that include the following
areas:
1. Management of acute respiratory failure
2. Traumatology cases
3. Metabolic &electrolyte disturbances
4. Sepsis & infection control
5. Acute coronary syndrome, dysrhythmias & cardiac pacing
6. Neurology& C.V. strokes
7. Nephrology& acute renal failure
8. Nutrition (Enteral & parenteral)
PROCEDURES By the end of this year the candidate should be handle the following procedures with high
competence and performance.
Intensive Care Medicine Egyptian Fellowship
47
1. Central venous line placement
2. Endotracheal Intubation
3. Arterial line placement
4. Mechanical ventilation
5. Intercostal tube Insertion
6. Tracheotomy
7. Cardiac pacing
8. Venous cut down
9. Pulmonary artery catheter
WORKSHOPS By the end of this year the candidate should have attended and passed successfully the following
workshops
1. Mechanical ventilation
2. Acid base
3. Nutrition
Y4 &Y5 (ICM3&ICM4)
INTENDED LEARNING OUTCOMES
Knowledge By the end of training, trainees should have adequate knowledge and deep understanding of:
The signs and symptoms that suggest life threatening or critical illnesses in neonates,
infants and children.
2. Management of cardiopulmonary arrest including basic and advanced life support.
The etiology, pathophysiology, clinical presentation and management of different types of
shock.
The etiology and clinical presentation of different types of coma in infants and children.
Causes and clinical presentation of childhood poisoning.
Initial management of burns, drowning and traumatized children.
The etiology, clinical presentation and management of acid base disturbances and
electrolyte imbalance.
Types and indications for mechanical ventilation.
The causes and management of childhood pain.
Ethical issues related to pediatric Intensive Care like withholding or withdrawal of life
support.
Intellectual and professional skills Trainees will be able to:
1. Recognize neonates, infants and children with critical or life threatening presentation
related to any body organ/system.
Take focused history and performs timely appropriate clinical examination for children in
the ER and in pediatric ICU.
3. Assess infants and children for fluid needs and manage different degrees of
1- Pediatric intensive care medicine
Intensive Care Medicine Egyptian Fellowship
48
dehydration.
Differentiate between types of electrolyte disturbances and manage appropriately.
5. Differentiate between various types of acid base disturbances and manage
appropriately.
Perform cardiopulmonary resuscitation in the field and in the ICU.
Assess and manage different types of shock.
8. Recognize , assess and initiate management for infants and children with different
organ/ system failure
Assess and manage different types of pain in infants and children system failure.
Initiate management and refer appropriately infants and children presenting with burns,
multiple traumas and pediatric surgical emergencies.
Recognize and initiate management for infants and children presenting with uncommon
emergencies like drowning, cold injury, and electric injury, psychiatric and gynecological
emergencies.
Initiate mechanical ventilation.
Communicate effectively with parents and children in critical situations like the need to
withdraw life support or when delivering bad news.
advise parents about prevention of childhood injuries.
THEORETICAL TOPICS
By the end of this training period the candidate should have gained an updated date and knowledge
about the following topics
1. The critically ill infant and child.
2. Respiratory emergencies.
3. Cardiac emergencies.
4. Renal emergencies.
5. Neurological emergencies.
6. Metabolic emergencies.
7. Hepatic failure.
8. Hematological emergencies.
9. Fluid replacement therapy.
10. Acid- base disturbances
11. Shock.
12. Mechanical ventilation.
CLINICAL CASES
By the end of this training period candidate should be able to diagnose and manage with high
perfection the life threatening aspect of the following cases:
1. Respiratory emergencies
i. Upper airway diseases 1. Stridor.
2. Foreign body inhalation
ii. Lower airway diseases
1. Wheezy infants and bronchial asthma
2. Pneumonia , effusion and pneumothorax
iii. Respiratory failure due to various causes
2. Cardiac vascular emergencies i. Heart failure
ii. Arrhythmias
Intensive Care Medicine Egyptian Fellowship
49
iii. Hypertension
iv. shock
3. Neurological emergencies v. Coma
vi. Convulsions
4. Metabolic emergencies: Diabetic ketoacidosis
5. Hematological emergencies
vii. Anemia
viii. DIC
6. Child abuse
PROCEDURES
1. PACLS
2. Mechanical ventilation
3. Intravascular access
a. Peripheral
b. Central
c. Intraosseous
4. Chest tube
5. Ascites tap
6. Urinary catheter
7. Nasogastric tube
8. Oropharyngeal suction
9. Blood products
10. Total parenteral nutrition
Y4 &Y5
INTENDED LEARNING OUTCOMES
Upon completion of training, Y4 & Y5 the fellow should be able to:
Patient Care
Demonstrate competency in the initial assessment, triage, and resuscitation of injured
patients
Demonstrate competency in airway assessment and management, including rapid sequence
intubation (RSI) and cricothyroidotomy
Demonstrate competency in recognizing and managing thoracic injury, including simple
and tension pneumothorax, [massive] hemothorax, rib fractures and flail chest, pulmonary
contusion, and great vessel injury
Demonstrate familiarity with such procedures as needle chest decompression and tube
thoracostomy
Demonstrate competency in appropriate performance of emergency thoracotomy
Demonstrate appropriate use of crystalloids and blood products for resuscitation
Demonstrate competency in implementing massive transfusion protocol
2-Trauma and burns
Intensive Care Medicine Egyptian Fellowship
50
Cite the advantages and disadvantages of endpoints of resuscitation, including vital signs
and other physical examination findings, base deficit, lactate levels, and global oxygen
delivery and consumption variables
Demonstrate familiarity with the type and placement of vascular access and the use of
massive transfusion devices
Demonstrate competency in diagnosing intra-abdominal injury, including the use of
focused assessment with sonography in trauma (FAST) examination and diagnostic
peritoneal lavage
Demonstrate competency in recognizing and managing abdominal compartment syndrome
and temporary abdominal closure techniques
Demonstrate competency in the diagnosis and management of pelvic fractures, including
recognition of associated injuries
Demonstrate competency in the management of patients with traumatic brain injury, spinal
cord injury, and blunt cerebrovascular injury, including the selection and use of intracranial
pressure monitoring devices and other brain monitoring devices
Demonstrate competency in appropriate timing and selection of radiographic studies in the
evaluation of the injured patient
Demonstrate the ability to interpret radiologic and laboratory data to develop
comprehensive management plans
Demonstrate comprehensive knowledge relevant to specific trauma patient populations
(e.g., pediatric, geriatric, and obstetric) including:
Methods of preventing the 'second insult' to the brain.
Management of cervical spine injuries.
Soft tissue injury related to fractures.
Crush injury and compartment syndromes.
Calculation of area burned.
Prevention of infection in the burned patient.
Detection and management of smoke inhalation or airway compromise.
Fluid resuscitation in the burned patient.
Medical Knowledge
Explain the significance of mechanism of injury in the care of the injured patient
Differentiate between blunt and penetrating mechanisms of injury
Explain the specific concerns in the care of the injured pediatric, geriatric, or obstetric
patient
Cite the principles of initial trauma evaluation and management
Describe the different types of thoracic injury and appropriate management strategies for
each, including initial and subsequent interventions
Cite the principles and practice of nonoperative management of solid abdominal organ
injury, including injury grading scales
Describe the causes and pathophysiology of elevated intra-abdominal pressure and
abdominal compartment syndrome, as well as principles and complications of temporary
abdominal closure
Describe the pathophysiology of various types of traumatic brain injury (including
epidural, subdural, intraparenchymal hemorrhage, diffuse axonal injury), and explain
techniques for preventing secondary brain injury
Describe the pathophysiology of intracranial hypertension and its management, including
the use of ICP monitoring devices, extraventricular drains, and operative intervention
Intensive Care Medicine Egyptian Fellowship
51
Cite key considerations in the management of patients with CNS injury, including fluid
selection, nutrition, management of coagulopathy, DVT prophylaxis, and such
complications as diabetes insipidus, cerebral salt wasting, and the syndrome of
inappropriate antidiuretic hormone release.
Describe the mechanisms and clinical signs and symptoms of blunt cerebrovascular injury,
and explain potential treatment strategies for these patients
Explain the pathophysiology of spinal cord and spinal column injury and its clinical
presentation, and describe management considerations (including complications) for these
patients
Describe clinical issues associated with spinal cord injury (e.g., cardiovascular and
ventilator considerations, tracheostomy, DVT prophylaxis, skin integrity, and contracture)
Demonstrate competency in managing extremity fractures, including optimal timing of
fracture fixation, recognition of associated vascular and neurologic injuries, and
recognition and prevention of compartment syndrome
Cite the complications associated with extremity injuries, including rhabdomyolysis, fat
embolism syndrome, and compartment syndrome
Explain key considerations in evaluating and managing the patient with a mangled
extremity, including the use of appropriate scores and adjunctive measures
Explain the significance of different types of pelvic fractures, and demonstrate competency
in management of associated injuries (e.g., urethral trauma and open fractures)
Cite the indications for and complications of blood component therapy and application of
massive transfusion principles
Practice-Based Learning
Describe measures and techniques for improving trauma system performance, including
review of specific indicators (e.g., delay to operative intervention)
Review published information critically to understand current evidence-based information
to optimize resuscitation (e.g., fluid selection, blood pressure control), select appropriate
radiographic imaging, and tailor care to specific problems (e.g., thoracic aortic injuries or
prevention of secondary brain injury)
Interpersonal and Communication Skills
Demonstrate effective communication with emergency medicine colleagues, nurses,
respiratory therapists, and consulting services for collaborative management of the injured
patient
Demonstrate effective communication with patients and family members, both listening
and conveying information with appropriate degree of complexity
Develop collaborative relationships with consulting services for optimizing the timing of
interventional procedures
Professionalism
Demonstrate respect, compassion, integrity and responsiveness to the needs of the patients
and their families
Approach discussions of ethical issues (including advanced directive and end-of-life issues)
with sensitivity
Demonstrate accurate self-assessment, knowledge of professional limits, and an ongoing
desire for self-improvement
Intensive Care Medicine Egyptian Fellowship
52
Systems-Based Practice
Demonstrate an understanding of the impact of a trauma system on regionalization of
trauma care
Demonstrate understanding of cost-effective patient care in a tertiary care hospital setting
Participate actively in triage decision-making in the setting of multiple casualties
Serve as an advocate for quality patient care with due attention to costs and resources
Partner appropriately with other health care providers, including consulting physicians,
nurses, pharmacists, respiratory therapists, and physical and speech therapists
Demonstrate understanding of the role of discharge planning and selection of appropriate
discharge venue (rehabilitation facility vs skilled nursing facility vs home)
Skills Assessment and immediate stabilization of the trauma patient: primary survey.
Assessment and immediate stabilization of the trauma patient: primary & secondary
survey.
Calculation and documentation of Glasgow coma scale.
Recognition of need for appropriate investigations (Hb, cross-match, chest X-ray, CT scan
etc).
Assessment, prediction and management of circulatory shock.
Emergency airway management, oxygen therapy and ventilation.
Chest drains insertion & management: emergency relief of tension Pneumothorax.
Cannulation of major vessels for resuscitation and monitoring.
Care and immobilization of cervical spine.
Analgesia for the trauma patient.
Urinary catheterization in pelvic trauma.
Differentiate & manage tension Pneumothorax, cardiac tamponade, and pulmonary
embolus.
THEORETICAL TOPICS
This course will cover the following lectures in addition to the rotation in the intended mono
disciplinary intensive care in year 4 and 5
Surgical management of head injury
Intensive care management of head injury
Surgical management of chest injury
Intensive care management of chest injury
Management of abdominal trauma
Management of spinal cord trauma
Management of face trauma
Management of wound
Surgical management of burns
Intensive care management of burn
Antibiotic therapy in burn, elective surgery and trauma patient
CLINICAL CASES All cases of trauma admitted to the surgical causality intensive care whether mono or poly trauma
should be managed and in collaboration with the intended subspecialty
Y4&Y5
3- Surgical post operative intensive care
Intensive Care Medicine Egyptian Fellowship
53
INTENDED LEARNING OUTCOMES
Knowledge Trainees should have adequate knowledge and deep understanding of:
A. General factors:
Importance of preoperative health status on postoperative outcomes.
Factors determining perioperative risk, and methods of optimizing high-risk patients.
Implications for postoperative care of type of surgery.
Implications for postoperative care of type of anesthesia.
Anesthetic risk factors complicating recovery: suxamethonium apnea, anaphylaxis,
malignant hyperpyrexia, difficult airway.
Dangers of emergency anesthesia.
The interpretation of relevant preoperative investigations.
Effect of gastric contents, smoking, and dehydration on perioperative risk.
Implications for postoperative care of common medical conditions (see section on
general medical conditions).
Implications of current drug therapy.
Need for and methods of perioperative anti-thrombotic treatment.
Assessment of post-operative analgesic needs.
Management of cyanosis, hypo- and hypertension, shivering and stridor.
Assessment of pain and methods of pain management.
Methods of treating of postoperative nausea and vomiting.
Causes and management of post-operative confusion.
Assessment of appropriate level of postoperative care: ICU, HDU, post-anesthesia
recovery.
The importance of consent and the issues surrounding it.
B. Respiratory:
Interpretation of symptoms and signs of respiratory insufficiency in the surgical patient; the
unprotected airway; upper and lower airway obstruction including epiglottitis; pneumonia,
collapse or consolidation, pulmonary infiltrates including acute lung injury (ALI) and the acute
respiratory distress syndrome (ARDS) and their causative factors; pulmonary edema; pleural
effusion, pneumothorax (simple and tension); use of chest drains; factors affecting patients
following thoracotomy, lung resection, oesophagectomy, cardiac surgery and thymectomy.
C. Cardiovascular:
Interpretation of symptoms and signs of cardiovascular insufficiency in the surgical patient;
operative risk factors in patients with ischemic heart disease; pulmonary embolus; cardiac
tamponade; management of patients following cardiac surgery (coronary grafting, valve
replacement) and aortic surgery (thoracic descending, abdominal); heart and heart-lung
transplantation.
D. Renal:
Causes of perioperative oliguria and anuria; prevention and management of acute renal failure;
consequences of nephrectomy, ileal conduits.
E. Gastrointestinal:
Intensive Care Medicine Egyptian Fellowship
54
Interpretation of abdominal pain and distension; peptic ulceration and upper GI hemorrhage;
diarrhea, vomiting and ileus; peritonitis; intestinal ischemia, abdominal tamponade; pancreatitis;
jaundice; management of the post-liver transplant patient; perioperative nutrition.
F. Neurological:
Surgical causes of confusion, coma and raised intracranial pressure; determinants of cerebral
perfusion and oxygenation; prevention of secondary brain injury; perioperative management of
patients with neuropathies and myopathies (e.g.: thymectomy); intracranial pressure monitoring;
intracerebral hemorrhage; spinal cord and brachial plexus injury.
G. Sepsis and infection:
Pyrexia and hypothermia; wound infections; necrotizing fasciitis; prophylactic antibiotics; risk
of infection in patients with indwelling medical devices including intravascular and urethral
catheters and heart valves; peritonitis; intestinal ischemia.
H. Hematology and oncology:
Care of the immunosuppressed or immunoincompetent patient; management of severe acute
hemorrhage and blood transfusion; coagulation disorders and hemoglobinopathies
I. Metabolic and hormonal:
Perioperative management of patients with diabetes; hypo- and hyperadrenalism, surgery to
thyroid, adrenal and pituitary glands; perioperative electrolyte disorders.
J. Musculo-skeletal:
Trauma patients (see trauma section); pressure area care; compartment syndromes; paralyzed
patients.
Skills Obtain information from sources other than the patient.
Identify airway or intubation difficulties, preoperative health status and intercurrent
disease, medications, allergies, nature of anesthetic and surgery.
Assess conscious level, status of airway and cervical spine, and conduct careful systems
review.
Determine adequacy and route of administration of analgesia.
Document, monitor and manage fluid balance, circulating volume, drains, systemic
oxygen supply.
Identify life-threatening cardio respiratory complications, and manage hypovolemia.
Differentiate and manage tension Pneumothorax, cardiac tamponade, and pulmonary
embolus.
Attitudes and behavior Establish a plan for postoperative management.
Ensure the necessary resources are available for safe postoperative care.
Communicate effectively to establish care plan with anesthetist, surgeon, nursing staff
and other professionals, and with relatives and patient where appropriate.
THEORETICAL TOPICS Organ transplantation:
Indications for transplantation of heart, kidney, and liver
Immunosuppression
Intensive Care Medicine Egyptian Fellowship
55
Infections in the immunocompromised patient
Organ rejection early and late
Organ donation
Bone marrow transplantation complications
Post operative management of brain and spinal cord surgery
Post operative management of open heart surgery
Post operative management of liver transplantation
Post operative management of renal transplantation
Post operative of major abdominal surgery
CLINICAL CASES
Intensive Care Post Operative Liver Transplantation (2 M)
1. Post operative cases
2. I.C.U Post transplantation complication cases
Intensive Care Neurosurgery Cases (2M)
1. Brain
2. Spinal cord
Intensive Care Post Operative Open Heart (2M)
1. CABG
2. Valve replacement
3. Open heart operations
Post Operative General Intensive Care (2M)
Different cases
Y4 & Y5
INTENDED LEARNING OUTCOMES
Knowledge By the end of training, trainees should have adequate knowledge and deep understanding of:
The recognition, evaluation and management of critically ill patients as part of an
intensivist-led multidisciplinary team.
Assessment and management of common ICU problems/syndromes/diseases will be
emphasized.
The management of the ventilator for common conditions, including asthma, COPD,
pneumonia, CHF, and ARDS.
The management of acute coronary syndrome, heart failure, arrhythmias, and
conduction defects
The management of cases with peritoneal dialysis, hemodialysis, and ultra filtration.
4-Medical intensive care
Intensive Care Medicine Egyptian Fellowship
56
The management of CVS, convulsions, Myopathies, and neuropathies
The scientific evidence behind treatment of common critical care conditions.
The indications and contraindications for common critical care procedures, including
central line placement, pulmonary artery catheterization, dialysis, arterial line
placement, thoracentesis, intubation, and non-invasive ventilation
Skills
Obtain information from sources other than the patient.
Identify airway or intubation difficulties, and discuss ventilation data and
complications
Assess conscious level, neurological status, and plan for the management of the case
and the anticipated complications
Determine adequacy and route of administration of analgesia. and other drugs and
discuss its actions and interactions
Document, monitor and manage fluid balance, circulating volume, drains, and
systemic oxygen supply.
Identify life-threatening complications in every patient according to his
pathological status
Access and critically evaluate current medical information and scientific evidence.
Attitudes and behavior Develop a good working relationship and rapport with other physicians, health
Professionals, patients, and families.
Communicate effectively, including presenting cases precisely and efficiently
Maintain comprehensive, timely and legible medical records.
Participate in daily sign-out rounds
Demonstrate interest in learning, and apply and open-minded and analytical approach
to acquiring knowledge.
THEORETICAL TOPICS
1. Microcirculatory failure in critically ill
2. Gastro-enteropathy in critically ill
3. Immunological response in critically ill
4. Immuno – inflammatory crosstalk in critically ill
5. Coagulopathy in critically ill
6. Coagulation – inflammation crosstalk in critically ill
7. Protective lung strategies in ventilated, COPD, ARDS, & Bronchial asthma
8. Regional perfusion pressure in critically ill
9. Priorities in resuscitation
10. Antibiotic therapy guidelines in critically ill
11. Impact of mechanical ventilation on cardiac function
12. Lung mechanics and its impact on ventilator adjustment variables
13. Protective brain strategies in critically ill
14. Protective renal strategies in critically ill
15. Post arrest syndrome
16. Calcium homeostasis in critically ill
17. Rejection and organ transplant
18. Waveform analysis of ventilated patient
CLINICAL CASES
Intensive Care Medicine Egyptian Fellowship
57
Intensive Care Cardiology (3M) 1. Acute coronary syndrome
2. Cardiac arrest
3. Right sided heart failure
4. Left sided heart failure (rheumatic, ischemic, cardiomyopathic)
5. Cardiogenic shock
6. Atrial arrhythmia
7. Ventricular arrhythmia
8. Pericarditis
9. Artificial valve dysfunction
10. Hypertension
Intensive Care Pulmonology Cases (2M) 1. Adult respiratory distress syndrome (ARDS)
2. Respiratory failure (COPD)
3. Respiratory failure (status asthmaticus)
4. Respiratory failure (pneumonia)
5. Severe community acquired pneumonia (CAP)
6. Ventilator associated pneumonia (VAP)
7. Aspiration pneumonia
8. Pulmonary embolism
9. Pneumothorax
10. Respiratory failure in special situations ( e.g. pregnancy)
11. Hemoptysis
Nephrology (Dialysis) (1M) 1. Hemodialysis
2. Ultra filtration
3. Peritoneal dialysis
Intensive Care Neurological and neuromuscular cases (2M) 1. Epilepsy
2. Cerebro vascular stroke
3. Spinal cord injuries (traumatic, vascular…)
4. Guillain Barré syndrome
5. Myasthenia gravis
6. Coma
7. Vegetative state
8. Myopathy
9. Neuropathy
Critical Care Training (6M) 1. Management of acute respiratory failure
2. Trauma cases
3. Metabolic & electrolyte disturbances cases
4. Sepsis& Infection control
5. Acute coronary syndrome, Dysrhythmias& Cardiac pacing
6. Neurology & C.V. Strokes
7. Nephrology& Acute renal failure
8. Toxicology
9. Nutrition
Intensive Care Medicine Egyptian Fellowship
58
PROCEDURES & SKILLS
As a part of the ICU experience is the performance of the multiple procedures needed for the
evaluation, monitoring, and care of patients. After being competent in performing a lot of
procedures along the previous training years , Candidate will be instructed and supervised in the
planning and performance of the following procedures,
1. Abdominal lavage
2. FAST
3. Cardiac pacing
WORKSHOPS
By the end of these training years Y4and Y5 the candidate should have finished the following
workshops
1. ATLS
2. PACLS
3. Echocardiogram (trans-esophageal)
5- Toxicology
Knowledge 1. Explain The epidemiology of poisoning in Egypt and define the common types of
ingestions in adults.
2. Describe The clinical features of common poisons and the principle of their
management (e.g. salicylate poisoning, Paracetamol, antidepressants, etc).
3. Highlight The medicolegal aspects of poisoning and what physicians should do to
protect their patients.
4. Describe The role of gastric lavage, activated charcoal, alkalinization and antidote
in the management of poisoning.
5. List The common types of environmental emergencies seen by internist and
outline their clinical manifestations and methods of treatment.
Skills 1. Recognize the symptoms and signs suggestive of poisoning, stabilize the patients
and call for help through immediate contact with poisoning centers.
2. Carefully obtain drug history from patient and relatives to identify the causative
agent.
3. Perform gastric lavage only when indicated.
4. Recognize cases suggestive of drug abuse stabilize and consult or refer to
toxicology centers, in the mean time the physician should involve appropriate
authorities.
5. Stabilize and resuscitate patients using The ABCDE approach.
6. Provide specific treatment if available or ensure safe referral.
7. Identify associated complications if present.
8. In case of scorpion or snake bite, he should be able to recognize the bite &
initiate treatment through the immediate provision of passive immunization.
Lectures
Intensive Care Medicine Egyptian Fellowship
59
1. General principles of management of acute poisoning
2. Corrosives
3. Animal poisoning
4. Food poisoning
5. Toxic gases exposure
6. Pesticides
7. Sedatives and hypnotic poisoning
8. Analgesic poisoning
9. Digitalis poisoning
10. Antipyretic poisoning
11. Antipsychotic poisoning
12. Antidepressant poisoning
13. Narcotic poisoning
METHODS OF ASSESSMENTS
REGULATIONS
The general rules and regulations of assessment approved by the Egyptian fellowship board and
published at the training handbook and also the board web site applies for the intensive care
specialty. In addition to the successful completion of the training program, all candidates must
successfully pass three exams in order to get the fellowship certificate.
First part Exam: The first part exam is a written exam. Trainees are allowed to sit for the first
part exam after 18 months of training. Each candidate has three chances to pass the exam and one
more additional chance may be granted in some special circumstances approved by the secretary
general of the higher committee of medical specialties. It is to be noted that after 18 months of
training each time the candidate will choose not to enter the exam will be calculated as one of
his three attempts.
Second part exam: The second part exam is a written exam. Trainees are allowed to sit for the
second part exam after passing successfully the first part and after completion of the training
period (five years). In addition, each candidate must submit his log book for final assessment. The
log book requirements must all be completed and signed by the trainer and educational supervisor.
Each candidate has three chances to pass the exam and one more additional chance may be granted
in special approved circumstances.
Clinical Exam (third part): The third part exam is a clinical and oral exam. Candidates who pass
successfully the second part are allowed to sit for the third part. Again each candidate has three
chances to pass the clinical exam and an additional fourth chance may be granted in special
approved circumstances.
Pre‐ requisites for entering the first part exam
Trainees should pass the following courses in order to be eligible for the first part exam 1. Local TOEFEL with a score of at least 500
2. Computer courses in word processing, spread sheets, internet and power point
Intensive Care Medicine Egyptian Fellowship
60
STRUCTURE OF THE EXAMINATION
The first part exam aims to test trainee's knowledge in basic science and different subspecialties of
internal medicine as it is mentioned in this curriculum.
The structure of the first part exam: PART I examination consists of two papers:
1- Paper I (2 hours): Multiple choice questions with a single best answer format. This paper will
cover applied basic sciences mentioned in the curriculum.
2- Paper II (2 hours): short answer and /or problem solving questions and this paper test trainees'
knowledge in the basics of internal medicine subspecialties that must be covered during the first
two years of training. The second part exam aims to test trainees' knowledge and skills in internal medicine. In this exam all
the internal medicine curriculum will be covered.
The structure of the second part exam: Part II examination consists of four papers:
1. Two MCQ papers each two hours in duration. They are covering all intensive care specialties. In
both papers, facts, problem solving and management skills are going to be assessed. You will
choose one best answer in each question 2. Two short assay papers each two hours in duration. They cover all intensive care subspecialties.
Questions will assess Trainees' knowledge about various diseases and their management. In addition, it
will test students' problem solving skills.
The structure of the third part exam: part III exam is a clinical and oral exam and is composed of
the following components:
1. Clinical exam
The clinical exam remains the most important part of the examination as the long case evaluate the
potential performance of the candidate in clinical practice while short cases assess clinical
examination skills in various system. Passing this component of the exam independently is
essential for certification.
1.1. Long Clinical Case : the candidate is observed in silence for the first part of the
examination by two examiners where he/she is taking the history from the relatives or the
patient and performing a physical examination and then the examiner asks the candidate to
present the finding, in history , examination and discuss the management of the case .
Marks are given according to a predetermined weighting of the components of the exam.
1.2. Clinical OSCE (Objective Structured Clinical Examination) this has replaced the
traditional short cases. Each candidate examines four or five patients. The examiners
evaluate his abilities to correctly elicit and interpret physical signs. An agreed marking
system is used to ensure objectivity and fairness of the exam.
1.3. OSPE is a multiple station examination including ECG/ X-ray / CT Scans/ laboratory
data results / skin photographs / karyotypes etc set as 10-20 OSCE stations. The candidate
rotates from station to station where he / she are tested on a specific element that measures
his data interpretation skills.
1.4. VIVA: The oral exam which tests the candidates’ ability to manage patients and
explores his/her knowledge of making an accurate diagnosis and whether he/she
understands the essentials of therapeutics. It also assesses his attitudes and interpersonal
communication skills. It is based on a set of topics with opening and supplementary
questions. The questions cards are prepared in advance together with the expected ideal
answer and allocated marks. This allows a good objective basis for marking.

Intensive Care Medicine Egyptian Fellowship
61

Intensive Care Medicine Egyptian Fellowship
62


















