Integrating Multidisciplinary Health Promotion ... · Informal discussions with the population...
11
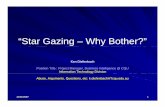
Ankur Sharma. Multidisciplinary Health Promotion Additional Material 1 Session II: Improving Outcomes through Community Engagement Integrating Multidisciplinary Health Promotion Interventions with Dental Education for Community Health Activation Dr. Ankur Sharma Lecturer, Department of Public Health Dentistry ManavRachna Dental College, Faridabad. India. Email: [email protected] Mob. +91 9560299027 1 The Problem People tend to ignore their healthcare needs for chronic disease until acute exacerbations. This leads to underutilization of chronic disease care services except in emergency. In spite of a high prevalence of dental disease in our region, people visited our hospital mainly for advanced diseases. This led to excessive load for particular procedures while many services still remained underutilized. Situation analysis: Looking for causes Situation analysis showed that the patients do not visit till their disease takes an acute form. Our Community Dental Health Program had covered a diverse population including people of various ages, lifestyles and socioeconomic groups. We had an attendance rate of 4% of the population at our camps, while, studies show a prevalence rate of more than 85% for periodontal disease in Indian population . Hence, majority of population was left unattended. Informal discussions with the population revealed that people do not bother about chronic disease until it takes an acute stage due to lack of self-efficacy. Solution: Standardized & Integrated Health Education “Integrated Health Promotion Program” (IHPP). A program that uses both informative and transformative health education approaches based on evidence from an extensive review of literature. In this program, we standardized health education intervention, tailored a training protocol and devised as well as validated tools for assessing its effectiveness. Figure 1.Multifaceted Integration
Transcript of Integrating Multidisciplinary Health Promotion ... · Informal discussions with the population...

Ankur Sharma. Multidisciplinary Health Promotion Additional Material
1
Session II: Improving Outcomes through Community Engagement
Integrating Multidisciplinary Health Promotion Interventions with Dental Education for
Community Health Activation
Dr. Ankur Sharma
Lecturer, Department of Public Health Dentistry
ManavRachna Dental College, Faridabad. India.
Email: [email protected]
Mob. +91 9560299027
1
The Problem
People tend to ignore their healthcare needs for chronic disease until acute exacerbations. This leads to
underutilization of chronic disease care services except in emergency. In spite of a high prevalence of dental disease
in our region, people visited our hospital mainly for advanced diseases. This led to excessive load for particular
procedures while many services still remained underutilized.
Situation analysis: Looking for causes
Situation analysis showed that the patients do not visit till their disease takes an acute form.
Our Community Dental Health Program had covered a diverse population including people of various ages,
lifestyles and socioeconomic groups.
We had an attendance rate of 4% of the population at our camps, while, studies show a prevalence rate of
more than 85% for periodontal disease in Indian population.
Hence, majority of population was left
unattended.
Informal discussions with the population revealed that people do not bother about chronic disease until it
takes an acute stage due to lack of self-efficacy.
Solution: Standardized & Integrated Health Education
“Integrated Health Promotion Program” (IHPP).
A program that uses both informative and transformative health education approaches based on evidence
from an extensive review of literature.
In this program, we standardized health education intervention, tailored a training protocol and devised as
well as validated tools for assessing its effectiveness.
Figure 1.Multifaceted Integration

Ankur Sharma. Multidisciplinary Health Promotion Additional Material
2
We integrated service provision through various providers like dentists, physicians, nutritionists and social
care professionals who facilitated and trained the dental students to provide a multidisciplinary health
education intervention.
We initially used the Trans-theoretical Model of Health Behavior Change, however, we soon switched over
to the Health Action Process Approach (HAPA) model, on which we could form a more firm basis of our
interventions and evaluations.
It is worth mentioning here that we retained our initial thought of name of one of our evaluation tools as
Trans-theoretical Questionnaire, thus recognizing the contribution of the model in building our thought
process.
Figure 2. The IHPP Model showing components and multifaceted integration.

Ankur Sharma. Multidisciplinary Health Promotion Additional Material
3
The Program
Table 2.Evaluation Tools

Ankur Sharma. Multidisciplinary Health Promotion Additional Material
4
Table.2 Evaluation tools
Tool Aim Description Theoretical Basis Validity
Trans-theoretical Questionnaire
To evaluate participant's self -management attitude and self-efficacy thereby determining readiness to bring about healthy changes in lifestyle
- The questionnaire consists of 10 questions to be answered on a 5 point Likert scale. - Scores ranged from 0 to 40.
1. Health Related Self-efficacy 2. HAPA Model 3. Trans-theoretical Model
Detailed Validity established according to COSMIN criteria.
One-dimensional Measure of Self Efficacy
High reliability values(chronbach’s alpha = 0.822; ICC = 0.854)
No floor or ceiling effects.
Wellness Analogue Scale (WAS)
To evaluate participant's perception of wellness.
Visual Analogue Scale with pictographic illustration of various wellness stages of on a scale of 0 to 100 in intervals of 10.
Determinants of Physical, Psychological and Social Wellness.
Face, content and criterion validity established
Oral Health Related Knowledge and Attitude Questionnaire
To evaluate Oral Health related knowledge and attitudes attained after the program.
- A 14 question instrument to be answered on a dichotomous scale (yes/ no). - Number of correct answers determined the score.
Adapted from Oral Health KAP questionnaires used previously in India and China.
Pretested questionnaires were used and tested on 15 lay persons for simplicity.
Motivational Interview
Motivational and Evaluation tool to assess effectiveness through participation, ability of the participants to answer and make collective decisions.
- A 23 question instrument. - The interview dealt with three topics: cost of health and disease, responsibility for health care and importance of balanced diet.
- Shared decision making through motivational interviewing
Tested for ease of understanding in a group of 5 dental students and 10 community members. Tested for construct by a specialist group consisting of a public health dentist, primary care physician, Health Promotion Perspectives nutritionist and a social worker.
Group Discussion
Motivational and Evaluation tool to assess effectiveness through participant's change in belief and understanding about personal hygiene
Undergraduate student moderated discussion along with comments and explanations by the moderator.
Determinants of personal, household and oral hygiene
Personal Hygiene Demonstration (PHD)Test
To assess the personal hygiene skills learnt by the participants.
Evaluated through undergraduate students
Determinants of personal, household and oral hygiene
Number of participants utilizing healthcare services
Daily foot-fall for 8 times/2 months on patient feeders after screening programs after0, 2 months, 4 months and 6 months. Comparisons with control sites.

Ankur Sharma. Multidisciplinary Health Promotion Additional Material
5
4
Testing of Program
The program was evaluated and tested in house wives of two underprivileged communities in Faridabad in families
selected by an NGO. Two neighboring communities were taken as controls.
Table 3.Population Characteristics
NGO's criteria for inclusion into Family Support Program:
The family was selected by the NGO if it lacked access to at least five of the following assets:
Television
Refrigerator
Washing machine
Motorcycle
Toilet
Safe drinking water
Own house
Agricultural Land.
Total No. of Participants = 55
Response Rate = 61.1%
Total Number of families = 90
Target Population (Underpreviliged)
Intervention Sites
Ismailpur Tilpat
Control Sites
Agwanpur Palla

Ankur Sharma. Multidisciplinary Health Promotion Additional Material
6
Geographical location
Results:
TtQ (Pre-Post)(Both intervention sites N= 55)
t-Test
Pre- Post-
Mean 25.47272727 32.5454545
P(T<=t) two-tail 0.0000000918 (Highly Significant)
ISMAILPUR

Ankur Sharma. Multidisciplinary Health Promotion Additional Material
7
WAS (Pre-Post)(Both intervention sites N=55)
t-Test
Pre- Post-
Mean 51.8181818 70.36364
P(T<=t) two-tail 0.00000164 (Highly Significant)
Service Utilization Ismailpur (intervention) Vs Agwanpur (control) (all six months) over 32 visits for number of
persons utilizing the services per visit
t-test
Ismailpur (Intervention) Agwanpur (Control)
Arithmetic mean 25.8750 6.8750
Mean difference -19.0000
Two-tailed probability P < 0.0001 (Highly Significant)
Service Utilization Tilpat (intervention) Vs Palla(control) (all six months) over 32 visits for number of persons
utilizing the services per visit
t-test
Tilpat (Intervention) Palla (Control)
Arithmetic mean 23.1250 7.6875
Mean difference -15.4375
Two-tailed probability P < 0.0001 (Highly Significant)
Oral Health Knowledge & Attitude (Both intervention sites N=55)
Knowledge Level
Low Average High
4 (7.3%) 27 (49.1%) 24 (43.6%)
Attitude Level
Poor Fair Good
7 (12.7%) 26 (47.3%) 22 (40%)
PHD Test (Both intervention sites N=55)
Correct = 50
Wrong = 5

Ankur Sharma. Multidisciplinary Health Promotion Additional Material
8
Motivational Interview
The groups were able to understand and discuss the importance of diet in their lives and questioned the nutritionist
freely. They were also able to take collective decisions about their health. All the groups agreed that they could take
care of their family's health only when they themselves were healthy.
Group Discussion
The group discussion was based on personal hygiene. Most of the individuals considered personal hygiene
important and had a strong sense of personal cleanliness based on social and ritual importance of cleanliness in the
society. Most of the women, however, did not know about the right way to wash their hand and clean their teeth. They
were also unaware of diseases caused by preparing food with unclean hands or eating food with unwashed hands.
The group moderators taught them the right way to clean hands and teeth at the end of the discussion and gave them
personal hygiene instructions. After the discussion, the groups were able to correlate personal hygiene with health
and developed a positive outlook toward personal hygiene.
Conclusion
Integrated Health Promotion Program (IHPP) was successful in bringing about a positive change in health related behavior and self efficacy of participants resulting in improved healthcare resource utilization. Its success could be attributed to its strong design, theoretical basis of construction, integration of various healthcare needs and methods of health promotion. The program was successful in integrating health promotion in primary health care with dental education. It also established that dental students could be involved successfully in community health promotion. Varied healthcare student population should be involved for health promotion activities .In the future, a structured program such as this will prove beneficial to the society as well as health care fraternity in developing world.
Practice implications
Healthcare student population may be used in developing countries to bring about attitude change and improvement of health related self-efficacy in underprivileged population through an integrated health promotion program.
Integrating dental education with primary health care for health promotion has been successful as shown by the present program. Such a program will be able to address capital and manpower shortage in primary health care which is a major barrier for health promotion in developing countries.
Health promotion among masses will help in reducing the disease burden in developing nations and reducing the loss of time and money due to diseases. The present program did not incur a huge cost and used basic health education techniques to activate the participants.
Similar programs can prove beneficial in providing cost effective solutions to many a healthcare woes in the developing world. The program provides a win -win situation for the community, students as well as the future policy makers.
Future researches can be aimed at the effectiveness of the program involving various other student populations such as Medical, Homeopathic, Aurvedic, Unani, Nursing, Social work and Physical education students for whom health education is a part of the curriculum.

Ankur Sharma. Multidisciplinary Health Promotion Additional Material
9
Evaluating the long term results of the program in different geographical and cultural areas in India, SAARC
nations and other developing countries worldwide can be another endeavour. Suitable changes may be made to the program according to the cultural and health care requirements of the country.
Finally, the program brings forth concepts that may be used by the healthcare service industry to improve healthcare service utilization for various chronic diseases.

Ankur Sharma. Multidisciplinary Health Promotion Additional Material
10
Some Program Photographs
Registeration & Initial Briefing Group Discussion
Interaction with Nutritionist PHD test
Evaluating the program A learning experience

Ankur Sharma. Multidisciplinary Health Promotion Additional Material
11
Project Team: Dr. Ankur Sharma, Department of Public Health Dentistry, Manav Rachna Dental College, Faridabad. Dr. Meena Jain, Department of Public Health Dentistry, Manav Rachna Dental College, Faridabad. Dr. Shilpi Singh, Department of Public Health Dentistry, Institute of Dental Studies & Technology, Modinagar Dr. Gurjeet Kaur Chawla, Department of Nutrition & Dietetics, Manav Rachna International University,
Faridabad. Dr. Poornima Sharma, Department of Public Health Dentistry, Manav Rachna Dental College, Faridabad. Dr. Puneet Gupta, Department of Public Health Dentistry, IDS, Bareilly Mr. Nalin Maurya, SOS Childrens’ Villages of India, Faridabad. Mr. Shadab Khan, Assistant Project Manager, Radio Manav Rachna 107.8 FM, community radio station,
Faridabad. Advisory Team:
Maj Gen(Retd) (Dr.) PN Awasthi, Dr. AK Kapoor, Dr. Arudeep Singh, Dr. CP Sharma, Dr. Karim Virjee, Dr. Nagesh L, Dr Sridhar Kanan, Dr Nisha Yadav Participants:
Dr Shefali Bhola, Dr. Shivngini, Dr. Saurabh Sharma, Dr. Shreya Bhargava, Dr. Sushant Dhalla, Dr.Vijay Karan Sandhu, Dr. Meenu, Dr. Manish Gaur, Dr. Manish Panwar, Dr. Kanwaljeet, Dr. Karishma, Dr. Harris Bhandari, Dr. Farah Bano, Dr Surabhi, Dr. Kiran Banga, Dr. Nishant Bhushan Sharma, Dr. Nitish Khanna, Dr. Prarthana.